

Comparing Prognostic Factors of Cancers Identified by Artificial Intelligence (AI) and Human Readers in Breast Cancer Screening
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
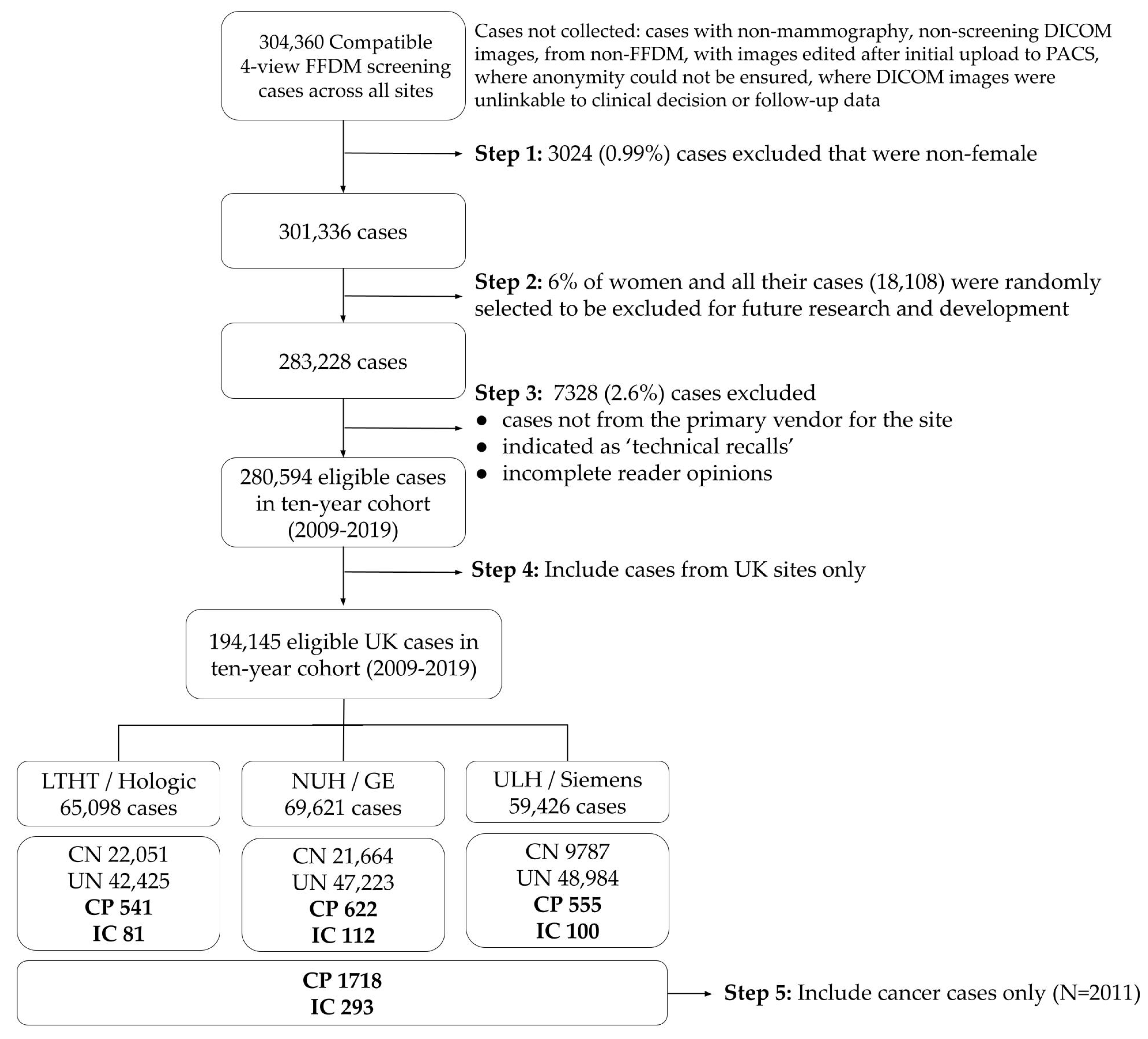
2.1. Study Populations and Samples
2.2. AI System
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
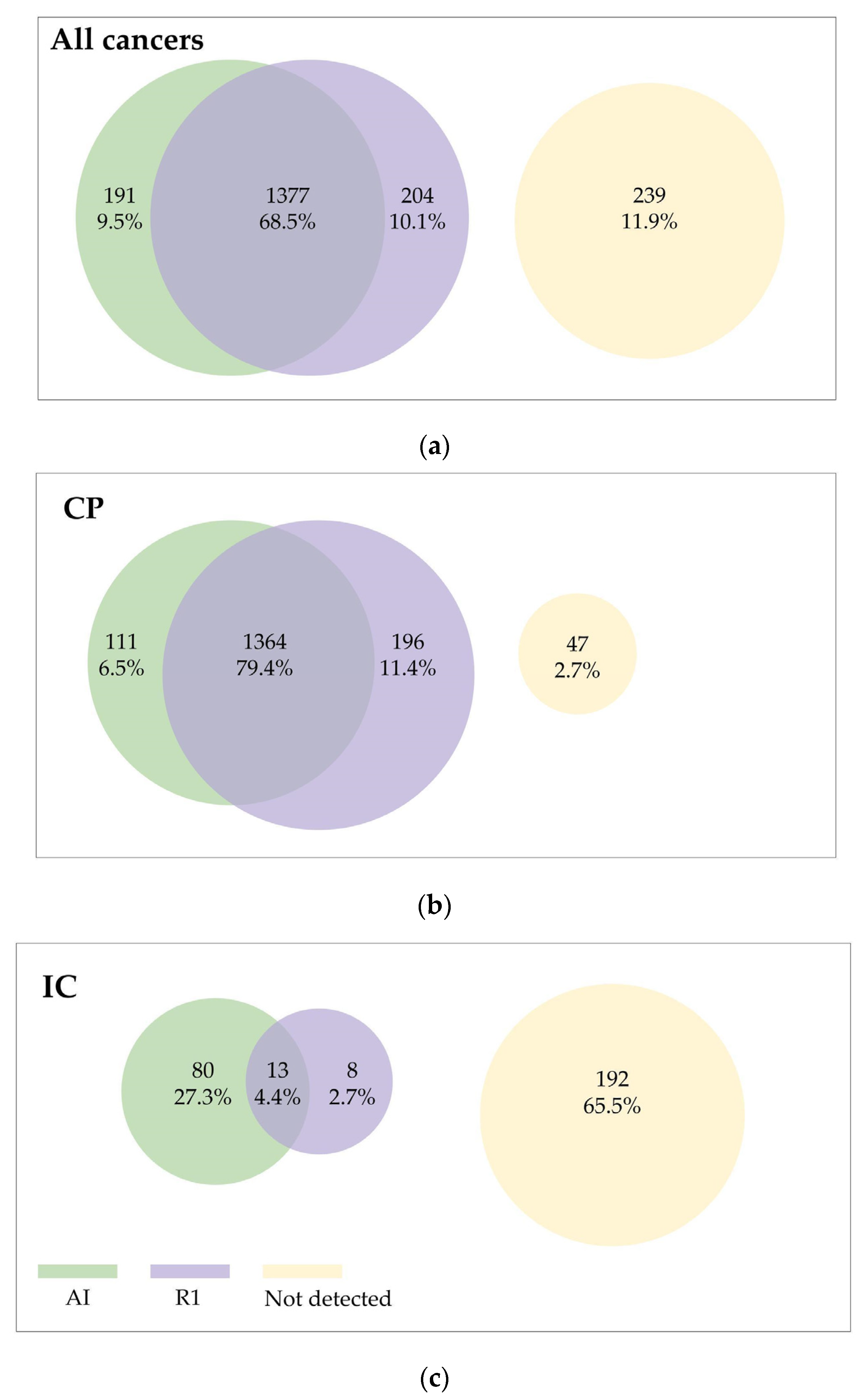
3.2. General Performance Metrics
3.3. Distribution of Tumour Characteristics
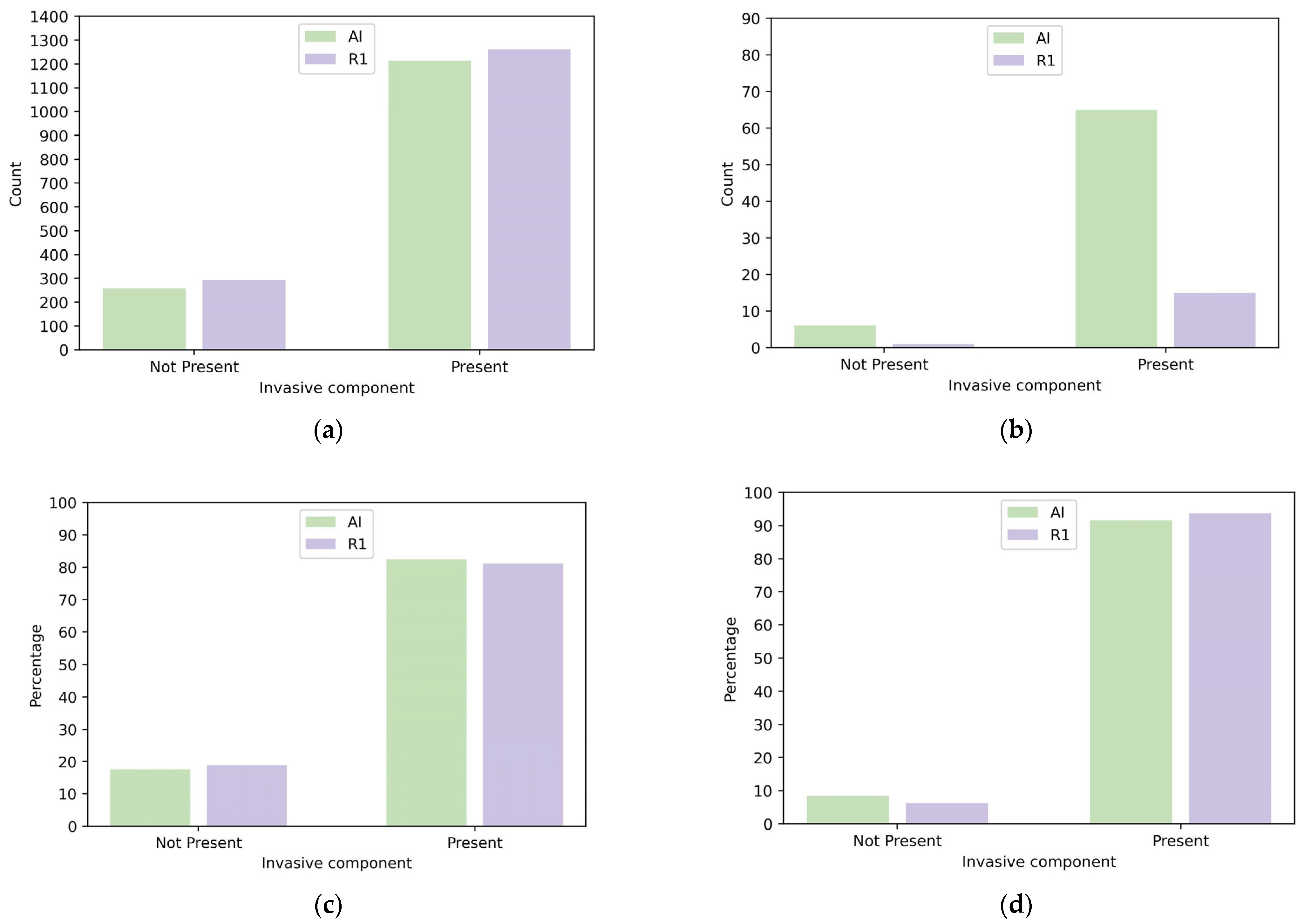
3.3.1. Invasive Cancer Detection
3.3.2. Histological Grade
3.3.3. Tumour Size
3.3.4. Lymph Node Stage
3.4. Sensitivity and Relative Sensitivity per Prognostic Subgroup of R1 and AI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- de Munck, L.; Siesling, S.; Fracheboud, J.; den Heeten, G.J.; Broeders, M.J.M.; de Bock, G.H. Impact of Mammographic Screening and Advanced Cancer Definition on the Percentage of Advanced-Stage Cancers in a Steady-State Breast Screening Programme in the Netherlands. Br. J. Cancer 2020, 123, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.W.; Tabár, L.; Yen, A.M.-F.; Dean, P.B.; Smith, R.A.; Jonsson, H.; Törnberg, S.; Chen, S.L.-S.; Chiu, S.Y.-H.; Fann, J.C.-Y.; et al. Mammography Screening Reduces Rates of Advanced and Fatal Breast Cancers: Results in 549,091 Women. Cancer 2020, 126, 2971–2979. [Google Scholar] [CrossRef] [PubMed]
- Blanks, R.G.; Wallis, M.G.; Alison, R.J.; Given-Wilson, R.M. An Analysis of Screen-Detected Invasive Cancers by Grade in the English Breast Cancer Screening Programme: Are We Failing to Detect Sufficient Small Grade 3 Cancers? Eur. Radiol. 2021, 31, 2548–2558. [Google Scholar] [CrossRef] [PubMed]
- Sechopoulos, I.; Teuwen, J.; Mann, R. Artificial Intelligence for Breast Cancer Detection in Mammography and Digital Breast Tomosynthesis: State of the Art. Semin. Cancer Biol. 2021, 72, 214–225. [Google Scholar] [CrossRef]
- Larsen, M.; Aglen, C.F.; Hoff, S.R.; Lund-Hanssen, H.; Hofvind, S. Possible Strategies for Use of Artificial Intelligence in Screen-Reading of Mammograms, Based on Retrospective Data from 122,969 Screening Examinations. Eur. Radiol. 2022, 32, 8238–8246. [Google Scholar] [CrossRef]
- Ng, A.Y.; Glocker, B.; Oberije, C.; Fox, G.; Sharma, N.; James, J.J.; Ambrózay, É.; Nash, J.; Karpati, E.; Kerruish, S.; et al. Artificial Intelligence as Supporting Reader in Breast Screening: A Novel Workflow to Preserve Quality and Reduce Workload. J. Breast Imaging 2023, 5, 267–276. [Google Scholar] [CrossRef]
- Riveira-Martin, M.; Rodríguez-Ruiz, A.; Martí, R.; Chevalier, M. Multi-Vendor Robustness Analysis of a Commercial Artificial Intelligence System for Breast Cancer Detection. J. Med. Imaging 2023, 10, 051807. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.W.; Larsen, M.; Bartsch, H.; Kurz, K.D.; Hofvind, S. Artificial Intelligence in BreastScreen Norway: A Retrospective Analysis of a Cancer-Enriched Sample Including 1254 Breast Cancer Cases. Eur. Radiol. 2023, 5, 3735–3743. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Phillips, S.; Seedat, F.; Kijauskaite, G.; Marshall, J.; Halligan, S.; Hyde, C.; Given-Wilson, R.; Wilkinson, L.; Denniston, A.K.; Glocker, B.; et al. UK National Screening Committee’s Approach to Reviewing Evidence on Artificial Intelligence in Breast Cancer Screening. Lancet Digit Health 2022, 4, e558–e565. [Google Scholar] [CrossRef]
- Tabar, L.; Chen, T.H.-H.; Yen, A.M.-F.; Chen, S.L.-S.; Fann, J.C.-Y.; Chiu, S.Y.-H.; Ku, M.M.S.; Wu, W.Y.-Y.; Hsu, C.-Y.; Chen, Y.-Y.; et al. Effect of Mammography Screening on Mortality by Histological Grade. Cancer Epidemiol. Biomark. Prev. 2018, 27, 154–157. [Google Scholar] [CrossRef] [Green Version]
- Duffy, S.W.; Dibden, A.; Michalopoulos, D.; Offman, J.; Parmar, D.; Jenkins, J.; Collins, B.; Robson, T.; Scorfield, S.; Green, K.; et al. Screen Detection of Ductal Carcinoma in Situ and Subsequent Incidence of Invasive Interval Breast Cancers: A Retrospective Population-Based Study. Lancet Oncol. 2016, 17, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.E.; Han, K.; Yoon, J.H.; Youk, J.H.; Kim, E.-K. Depiction of Breast Cancers on Digital Mammograms by Artificial Intelligence-Based Computer-Assisted Diagnosis according to Cancer Characteristics. Eur. Radiol. 2022, 32, 7400–7408. [Google Scholar] [CrossRef] [PubMed]
- McKinney, S.M.; Sieniek, M.; Godbole, V.; Godwin, J.; Antropova, N.; Ashrafian, H.; Back, T.; Chesus, M.; Corrado, G.S.; Darzi, A.; et al. International Evaluation of an AI System for Breast Cancer Screening. Nature 2020, 577, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.; Kim, M.J. Introduction of a New Staging System of Breast Cancer for Radiologists: An Emphasis on the Prognostic Stage. Korean J. Radiol. 2019, 20, 69–82. [Google Scholar] [CrossRef] [Green Version]
- Sunderland, M.C.; McGuire, W.L. Prognostic Indicators in Invasive Breast Cancer. Surg. Clin. N. Am. 1990, 70, 989–1004. [Google Scholar] [CrossRef]
- Donegan, W.L. Tumor-Related Prognostic Factors for Breast Cancer. CA Cancer J. Clin. 1997, 47, 28–51. [Google Scholar] [CrossRef]
- Sharma, N.; Ng, A.Y.; James, J.J.; Khara, G.; Ambrózay, É.; Austin, C.C.; Forrai, G.; Fox, G.; Glocker, B.; Heindl, A.; et al. Multi-Vendor Evaluation of Artificial Intelligence as an Independent Reader for Double Reading in Breast Cancer Screening on 275,900 Mammograms. BMC Cancer 2023, 23, 460. [Google Scholar] [CrossRef]
- Wilson, E.B. Probable Inference, the Law of Succession, and Statistical Inference. J. Am. Stat. Assoc. 1927, 22, 209–212. [Google Scholar] [CrossRef]
- Newcombe, R.G. Two-Sided Confidence Intervals for the Single Proportion: Comparison of Seven Methods. Stat. Med. 1998, 17, 857–872. [Google Scholar] [CrossRef]
- McNemar, Q. Note on the Sampling Error of the Difference between Correlated Proportions or Percentages. Psychometrika 1947, 12, 153–157. [Google Scholar] [CrossRef]
- Van Rossum, G.; Drake, F.L. Python 3 Reference Manual; CreateSpace: Scotts Valley, CA, USA, 2009; ISBN 9781441412690. [Google Scholar]
- Leibig, C.; Brehmer, M.; Bunk, S.; Byng, D.; Pinker, K.; Umutlu, L. Combining the Strengths of Radiologists and AI for Breast Cancer Screening: A Retrospective Analysis. Lancet Digit Health 2022, 4, e507–e519. [Google Scholar] [CrossRef] [PubMed]
- Hofvind, S.; Sagstad, S.; Sebuødegård, S.; Chen, Y.; Roman, M.; Lee, C.I. Interval Breast Cancer Rates and Histopathologic Tumor Characteristics after False-Positive Findings at Mammography in a Population-Based Screening Program. Radiology 2018, 287, 58–67. [Google Scholar] [CrossRef]
- O’Rourke, K. Breast Cancer Overdiagnosis through Mammograms Is Lower than Previous Estimates. Cancer 2022, 128, 2398–2399. [Google Scholar] [CrossRef] [PubMed]
- Chaltiel, D.; Hill, C. Estimations of Overdiagnosis in Breast Cancer Screening Vary between 0% and over 50%: Why? BMJ Open 2021, 11, e046353. [Google Scholar] [CrossRef]
- Independent UK Panel on Breast Cancer Screening the Benefits and Harms of Breast Cancer Screening: An Independent Review. Lancet 2012, 380, 1778–1786. [CrossRef] [PubMed]
- Duffy, S.W. The Benefits and Harms of Breast Cancer Screening. Lancet 2013, 381, 802. [Google Scholar] [CrossRef] [PubMed]
- Nagendran, M.; Chen, Y.; Lovejoy, C.A.; Gordon, A.C.; Komorowski, M.; Harvey, H.; Topol, E.J.; Ioannidis, J.P.A.; Collins, G.S.; Maruthappu, M. Artificial Intelligence versus Clinicians: Systematic Review of Design, Reporting Standards, and Claims of Deep Learning Studies. BMJ 2020, 368, m689. [Google Scholar] [CrossRef] [Green Version]
- Voets, M.M.; Veltman, J.; Slump, C.H.; Siesling, S.; Koffijberg, H. Systematic Review of Health Economic Evaluations Focused on Artificial Intelligence in Healthcare: The Tortoise and the Cheetah. Value Health 2022, 25, 340–349. [Google Scholar] [CrossRef]
- Chang, Y.-W.; An, J.K.; Choi, N.; Ko, K.H.; Kim, K.H.; Han, K.; Ryu, J.K. Artificial Intelligence for Breast Cancer Screening in Mammography (AI-STREAM): A Prospective Multicenter Study Design in Korea Using AI-Based CADe/x. J. Breast Cancer 2022, 25, 57–68. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Screen Detected Cancers | ||||||||
| Detected by R1 | Detected By AI | Total | ||||||
| N = 1560 | % | 95% CI | N = 1475 | % | 95% CI | N = 1718 | p * | |
| Invasive component | ||||||||
| present | 1261 | 81.1% | 79.1–83.0% | 1213 | 82.5% | 80.4–84.3% | 1385 | 0.374 |
| not present | 293 | 18.9% | 17.0–20.9% | 258 | 17.5% | 15.7–19.6% | 326 | |
| missing | 6 | 4 | 7 | |||||
| Interval Cancers | ||||||||
| Detected by R1 | Detected by AI | Total | ||||||
| N = 21 | % | 95% CI | N = 93 | % | 95% CI | N = 293 | p ** | |
| Invasive component | ||||||||
| present | 15 | 93.8% | 71.7–98.9% | 65 | 91.5% | 82.8–96.1% | 222 | 0.999 |
| not present | 1 | 6.3% | 1.1–28.3% | 6 | 8.5% | 3.9–17.2% | 15 | |
| missing | 5 | 22 | 56 | |||||
| Detected by R1 | Detected by AI | |||||||
|---|---|---|---|---|---|---|---|---|
| N = 1261 | % | 95% CI | N = 1213 | % | 95% CI | p * | ||
| Histological grade | 1 | 329 | 27.1% | 24.7–29.7% | 313 | 26.9% | 24.4–29.5% | 0.981 |
| 2 | 673 | 55.5% | 52.7–58.3% | 651 | 55.9% | 53.1–58.8% | ||
| 3 | 210 | 17.3% | 15.3–19.6% | 200 | 17.2% | 15.1–19.5% | ||
| Missing | 49 | 97 | ||||||
| Whole tumour size | ≤20 mm | 742 | 66.1% | 63.3–68.8% | 723 | 66.9% | 64.1–69.7% | 0.720 |
| >20 mm | 380 | 33.9% | 31.2–36.7% | 357 | 33.1% | 30.3–35.9% | ||
| Missing | 139 | 181 | ||||||
| Invasive tumour size | ≤20 mm | 941 | 83.1% | 80.8–85.1% | 907 | 83.1% | 80.8–85.2% | 0.995 |
| >20 mm | 192 | 16.9% | 14.9–19.2% | 184 | 16.9% | 14.8–19.2% | ||
| Missing | 128 | 170 | ||||||
| Lymph node status | Negative | 912 | 79.9% | 77.4–82.1% | 878 | 80.0% | 77.6–82.3% | 0.959 |
| Positive | 230 | 20.1% | 17.9–22.6% | 219 | 20.0% | 17.7–22.4% | ||
| Missing | 119 | 164 | ||||||
| Detected by R1 | Detected by AI | |||||||
|---|---|---|---|---|---|---|---|---|
| N = 15 | % | 95% CI | N = 65 | % | 95% CI | p * | ||
| Histological grade | 1 | 3 | 20.0% | 7.0–45.2% | 16 | 25.0% | 16.0–36.8% | 0.999 |
| 2 | 7 | 46.7% | 24.8–69.9% | 25 | 39.1% | 28.1–51.3% | ||
| 3 | 5 | 33.3% | 15.2–58.3% | 23 | 35.9% | 25.3–48.2% | ||
| Missing | 0 | 1 | ||||||
| Whole tumour size | ≤20 mm | 3 | 37.5% | 13.7–69.4% | 19 | 44.2% | 30.4–58.9% | 0.999 |
| >20 mm | 5 | 62.5% | 30.6–86.3% | 24 | 55.8% | 41.1–69.6% | ||
| Missing | 7 | 22 | ||||||
| Invasive tumour size | ≤20 mm | 9 | 64.3% | 38.8–83.7% | 34 | 56.7% | 44.1–68.4% | 0.766 |
| >20 mm | 5 | 35.7% | 16.3–61.2% | 26 | 43.3% | 31.6–55.9% | ||
| Missing | 1 | 5 | ||||||
| Lymph node status | Negative | 6 | 60.0% | 31.3–83.2% | 28 | 63.6% | 48.9–76.2% | 0.999 |
| Positive | 4 | 40.0% | 16.8–68.7% | 16 | 36.4% | 23.8–51.1% | ||
| Missing | 5 | 21 | ||||||
| Variable | N | Detected AI | SEN AI | 95% CI | Detected R1 | SEN R1 | 95% CI | p | |
|---|---|---|---|---|---|---|---|---|---|
| Invasive Component | not present | 341 | 264 | 77.4% | 72.9–81.8% | 294 | 86.2% | 82.5–89.9% | <0.001 |
| present | 1607 | 1278 | 79.5% | 77.6–81.5% | 1276 | 79.4% | 77.4–81.4% | 0.954 | |
| missing | 63 | ||||||||
| Tumour grade | grade 1 | 401 | 329 | 82.0% | 78.3–85.6% | 332 | 82.8% | 78.9–86.5% | 0.836 |
| grade 2 | 845 | 676 | 80.0% | 77.2–82.6% | 680 | 80.5% | 77.7–83.0% | 0.805 | |
| grade 3 | 307 | 223 | 72.6% | 67.6–77.5% | 215 | 70.0% | 64.9–75.3% | 0.322 | |
| missing | 54 | ||||||||
| Whole tumour size | ≤20 mm | 911 | 742 | 81.4% | 78.9–83.9% | 745 | 81.8% | 79.2–84.2% | 0.880 |
| >20 mm | 492 | 381 | 77.4% | 73.7–81.1% | 385 | 78.3% | 74.6–81.9% | 0.752 | |
| missing | 204 | ||||||||
| Invasive tumour size | ≤20 mm | 1168 | 941 | 80.6% | 78.3–82.7% | 950 | 81.3% | 79.1–83.5% | 0.594 |
| >20 mm | 289 | 210 | 72.7% | 67.5–77.8% | 197 | 68.2% | 62.8–73.5% | 0.092 | |
| missing | 150 | ||||||||
| Lymph node status | negative | 1110 | 906 | 81.6% | 79.3–83.8% | 918 | 82.7% | 80.4–84.9% | 0.460 |
| positive | 298 | 235 | 78.9% | 74.2–83.6% | 234 | 78.5% | 73.7–83.1% | 0.999 | |
| missing | 199 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oberije, C.J.G.; Sharma, N.; James, J.J.; Ng, A.Y.; Nash, J.; Kecskemethy, P.D. Comparing Prognostic Factors of Cancers Identified by Artificial Intelligence (AI) and Human Readers in Breast Cancer Screening. Cancers 2023, 15, 3069. https://doi.org/10.3390/cancers15123069
Oberije CJG, Sharma N, James JJ, Ng AY, Nash J, Kecskemethy PD. Comparing Prognostic Factors of Cancers Identified by Artificial Intelligence (AI) and Human Readers in Breast Cancer Screening. Cancers. 2023; 15(12):3069. https://doi.org/10.3390/cancers15123069
Chicago/Turabian StyleOberije, Cary J. G., Nisha Sharma, Jonathan J. James, Annie Y. Ng, Jonathan Nash, and Peter D. Kecskemethy. 2023. "Comparing Prognostic Factors of Cancers Identified by Artificial Intelligence (AI) and Human Readers in Breast Cancer Screening" Cancers 15, no. 12: 3069. https://doi.org/10.3390/cancers15123069