
Co-Creation of Breast Cancer Risk Communication Tools and an Assessment of Risk Factor Awareness: A Qualitative Study of Patients and the Public in India
 , ,
, ,  , ,
, ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Development of BC and Risk Factor Awareness Tools
2.2. Analysis
3. Results
3.1. Varying Awareness Levels of BC and Its Diagnosis
3.2. Varying Awareness Levels and Some Misconceptions of Breast Cancer Risk Factors
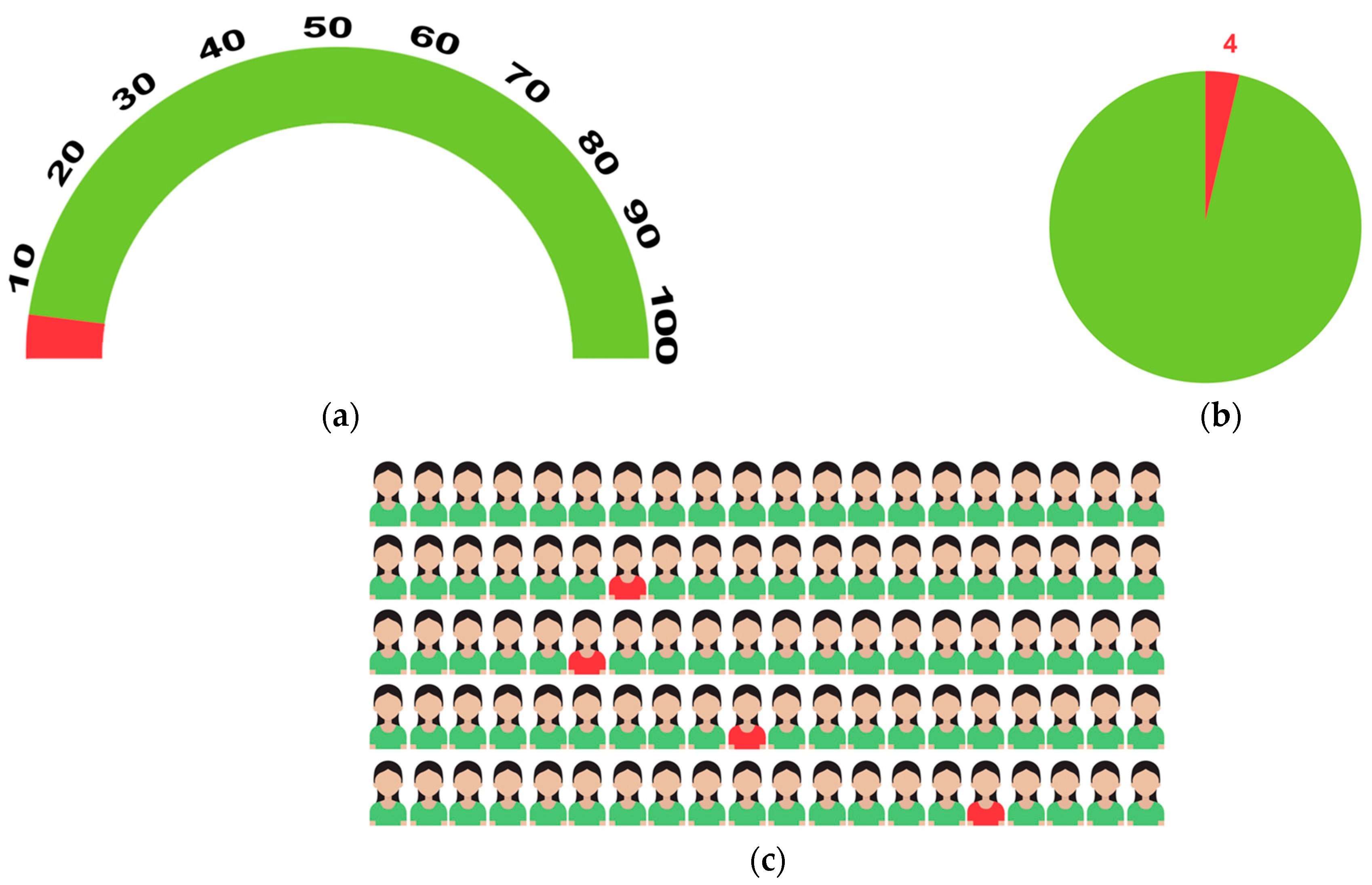
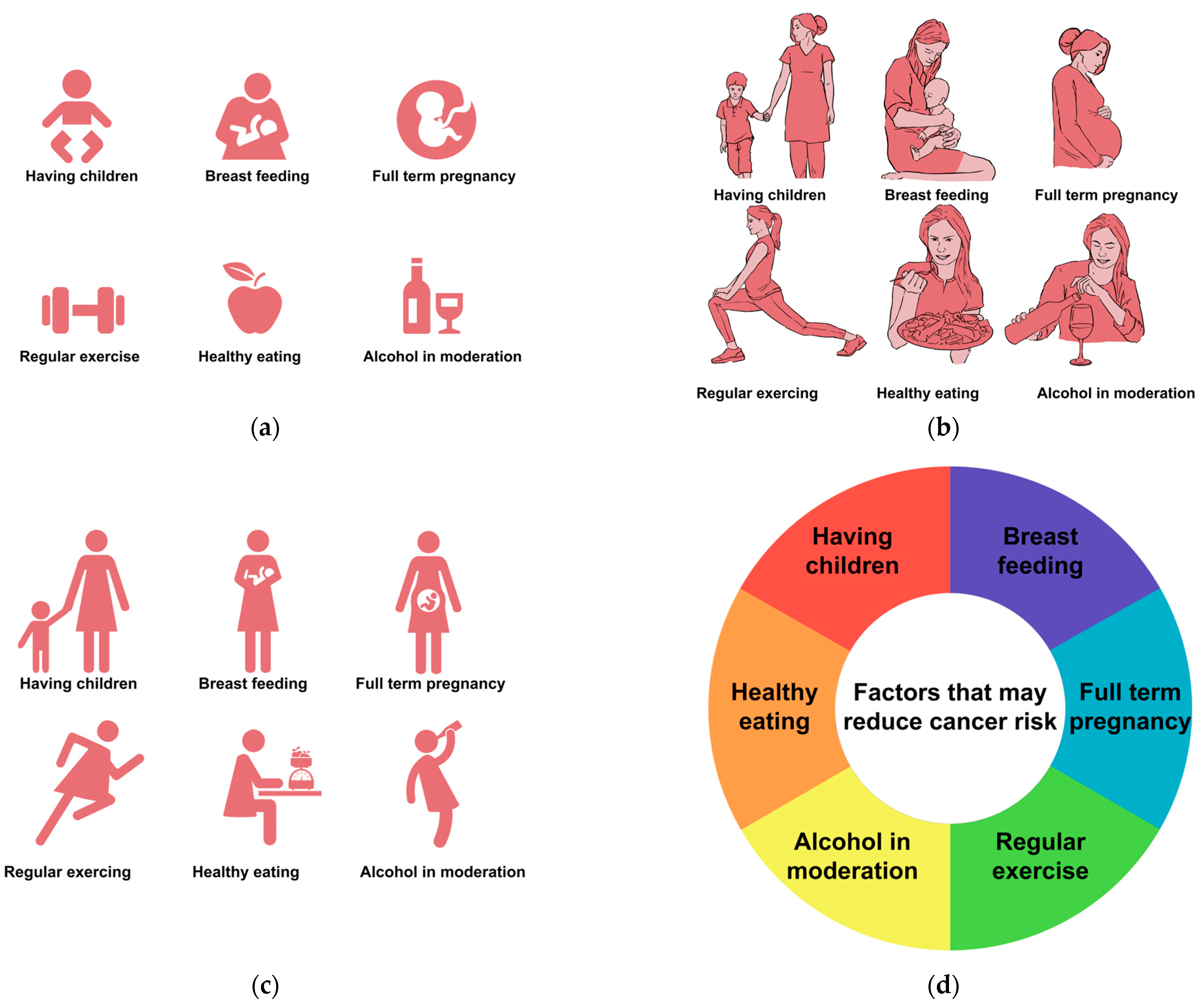
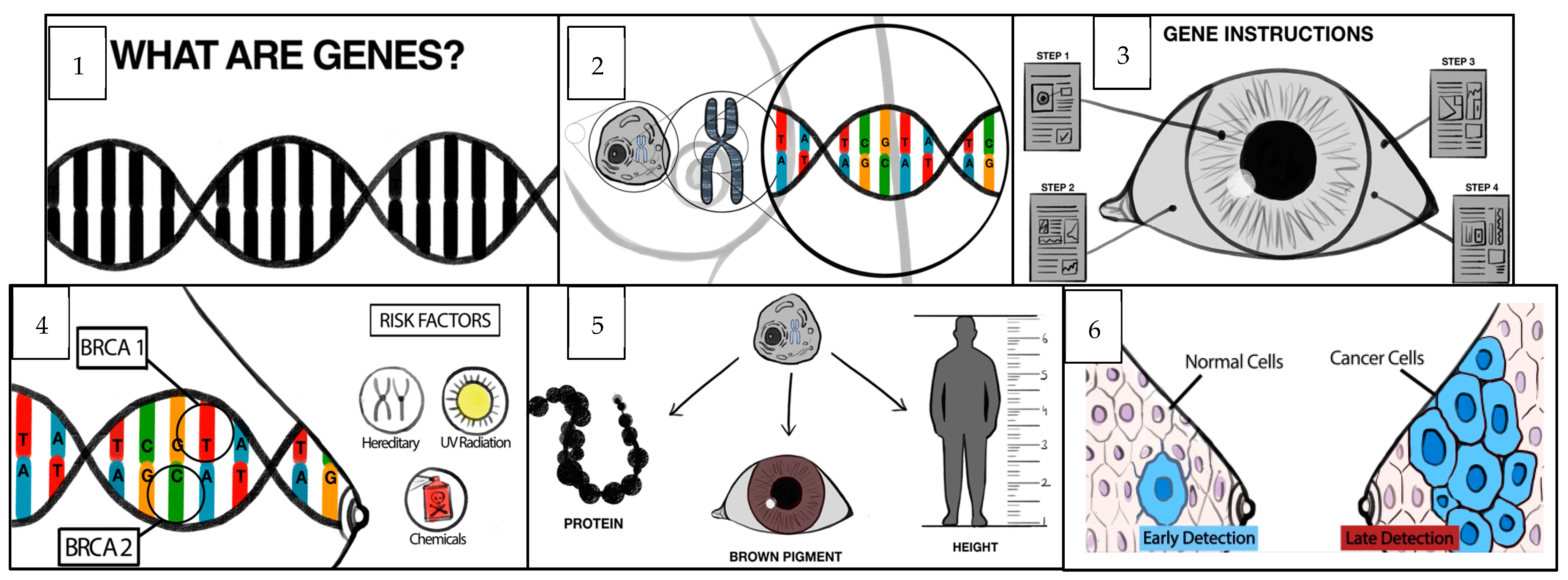
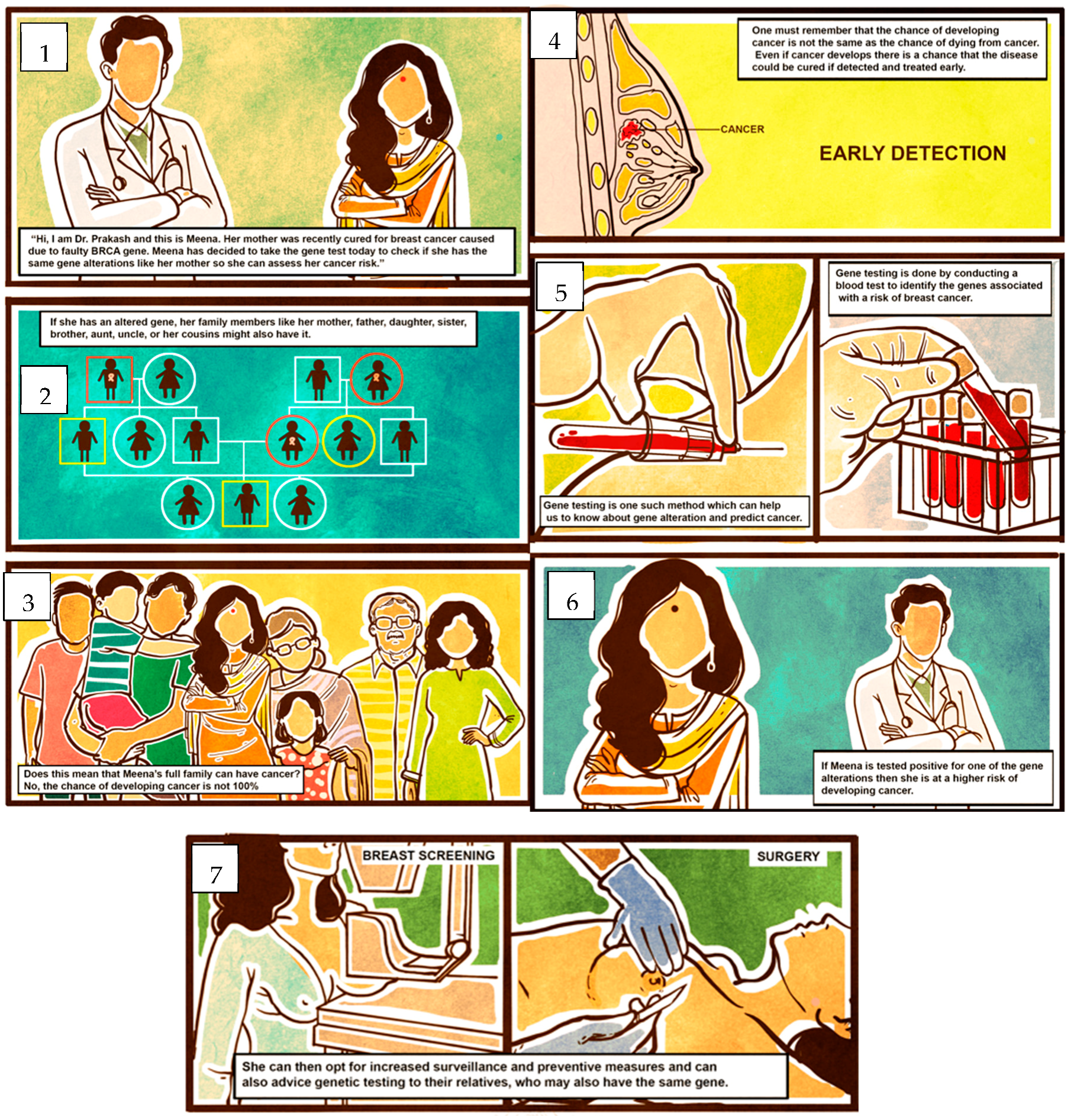
3.3. Preference for Risk Communication Prototypes
3.4. Other Suggestions
4. Discussion
4.1. Main Findings
4.2. In the Context of Other Literature
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. Breast Cancer in Young Women. 2021. Available online: https://www.cdc.gov/cancer/breast/young_women/bringyourbrave/breast_cancer_young_women/index.html (accessed on 2 August 2021).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Lima, S.M.; Kehm, R.D.; Terry, M.B. Global breast cancer incidence and mortality trends by region, age-groups, and fertility patterns. Eclinicalmedicine 2021, 38, 100985. [Google Scholar] [CrossRef]
- National Cancer Registry Programme. Trends over Time for All Sites and on Selected Sites of Cancer and Projection of Burden of Cancer. In Three-Year Report of Population Based Cancer Registries: 2012–2014; Chapter 10; Indian Council of Medical Research: New Delhi, India. Available online: https://main.icmr.nic.in/sites/default/files/reports/Preliminary_Pages_Printed1.pdf (accessed on 2 August 2021).
- Cancer Research UK (CRUK, 2020). Risk Factors. Available online: https://www.cancerresearchuk.org/about-cancer/breast-cancer/risks-causes/risk-factors (accessed on 25 July 2020).
- Feng, Y.; Spezia, M.; Huang, S.; Yuan, C.; Zeng, Z.; Zhang, L.; Ji, X.; Liu, W.; Huang, B.; Luo, W.; et al. Breast cancer development and progression: Risk factors, cancer stem cells, signaling pathways, genomics, and molecular pathogenesis. Genes Dis. 2018, 5, 77–106. [Google Scholar] [CrossRef]
- Chen, J.; Bae, E.; Zhang, L.; Hughes, K.; Parmigiani, G.; Braun, D.; Rebbeck, T.R. Penetrance of Breast and Ovarian Cancer in Women Who Carry a BRCA1/2 Mutation and Do Not Use Risk-Reducing Salpingo-Oophorectomy: An Updated Meta-Analysis. JNCI Cancer Spectr. 2020, 4, pkaa029. [Google Scholar] [CrossRef]
- Kuchenbaecker, K.B.; Hopper, J.L.; Barnes, D.R.; Phillips, K.A.; Mooij, T.M.; Roos-Blom, M.J.; BRCA1 and BRCA2 Cohort Consortium. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 2017, 317, 2402–2416. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. New Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef]
- Breast Cancer Association Consortium (BCAC). Breast cancer risk genes—Association analysis in more than 113,000 women. New Engl. J. Med. 2021, 384, 428–439. [Google Scholar] [CrossRef]
- Rivera- Franco, M.M.; Leon-Rodriguez, E. Delays in Breast Cancer Detection and Treatment in Developing Countries. Breast Cancer Basic Clin. Res. 2018, 12, 1178223417752677. [Google Scholar] [CrossRef] [PubMed]
- Malvia, S.; Bagadi, S.A.; Dubey, U.S.; Saxena, S. Epidemiology of breast cancer in Indian women. Asia-Pacific J. Clin. Oncol. 2017, 13, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Gupta, S.; Mehrotra, R.; Sodhani, P. Risk factors of breast cancer and breast self-examination in early detection: Systematic review of awareness among Indian women in community and health care professionals. J. Public Health 2020, 42, 118–131. [Google Scholar] [CrossRef]
- Sathwara, J.A.; Balasubramaniam, G.; Bobdey, S.C.; Jain, A.; Saoba, S. Sociodemographic factors and late-stage diagnosis of breast cancer in India: A hospital-based study. Indian J. Med. Paediatr. Oncol. 2017, 38, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Krishnamurthy, A.; Soundara, V.; Ramshankar, V. Preventive and Risk Reduction Strategies for Women at High Risk of Developing Breast Cancer: A Review. Asian Pac. J. Cancer Prev. 2016, 17, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Sivell, S.; Elwyn, G.; Gaff, C.L.; Clarke, A.J.; Iredale, R.; Shaw, C.; Dundon, J.; Thornton, H.; Edwards, A. How Risk is Perceived, Constructed and Interpreted by Clients in Clinical Genetics, and the Effects on Decision Making: Systematic Review. J. Genet. Couns. 2007, 17, 30–63. [Google Scholar] [CrossRef] [PubMed]
- Julian-Reynier, C.; Welkenhuysen, M.; Hagoel, L.; Decruyenaere, M.; Hopwood, P. Risk communication strategies: State of the art and effectiveness in the context of cancer genetic services. Eur. J. Hum. Genet. 2003, 11, 725–736. [Google Scholar] [CrossRef]
- Naik, G.; Ahmed, H.; Edwards, A.G. Communicating risk to patients and the public. Br. J. Gen. Pr. 2012, 62, 213–216. [Google Scholar] [CrossRef]
- Reyna, V.F.; Nelson, W.L.; Han, P.K.; Dieckmann, N.F. How numeracy influences risk comprehension and medical decision making. Psychol. Bull. 2009, 135, 943–973. [Google Scholar] [CrossRef]
- Hawley, S.T.; Zikmund-Fisher, B.; Ubel, P.; Jancovic, A.; Lucas, T.; Fagerlin, A. The impact of the format of graphical presentation on health-related knowledge and treatment choices. Patient Educ. Couns. 2008, 73, 448–455. [Google Scholar] [CrossRef]
- Fischhoff, B. Communicating Risks and Benefits: An Evidence Based User’s Guide; Government Printing Office: Washington, DC, USA, 2012.
- Chopra, B.; Kaur, V.; Singh, K. Age shift: Breast cancer is occurring in younger age groups-Is it true? Clin. Cancer Investig. J. 2014, 3, 526. [Google Scholar] [CrossRef]
- Sandhu, D.S.; Karwasra, R.K.; Marwah, S. Profile of breast cancer patients at a tertiary care hospital in north India. Indian J. Cancer 2010, 47, 16–22. [Google Scholar] [CrossRef]
- Saleem, S.M.; Jan, S.S. Modified Kuppuswamy socioeconomic scale updated for the year 2021. Indian J. Forensic Community Med. 2019, 8, 1–3. [Google Scholar] [CrossRef]
- Farmer, G.D.; Pearson, M.; Skylark, W.J.; Freeman, A.L.; Spiegelhalter, D.J. Redevelopment of the Predict: Breast Cancer website and recommendations for developing interfaces to support decision-making. Cancer Med. 2021, 10, 5141–5153. [Google Scholar] [CrossRef]
- Schapira, M.M.; Nattinger, A.B.; McAuliffe, T.L. The influence of graphic format on breast cancer risk communication. J. Health Commun. 2006, 11, 569–582. [Google Scholar] [CrossRef] [PubMed]
- Schapira, M.M.; Nattinger, A.B.; McHorney, C.A. Frequency or probability? A qualitative study of risk communication formats used in health care. Med. Decis. Mak. 2001, 21, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, K.; Crawford, B.J.; Pruthi, S.; I Williams, C.; Neal, L.; Sandhu, N.P.; Johnson, E.R.; Wahner-Roedler, D.; Britain, M.K.; Cha, S.S.; et al. Frequency format diagram and probability chart for breast cancer risk communication: A prospective, randomized trial. BMC Womens Health 2008, 8, 18. [Google Scholar] [CrossRef]
- Machida, M.; Murakami, M.; Goto, A. Differences in Data Trustworthiness and Risk Perception between Bar Graphs and Pictograms. Int. J. Environ. Res. Public Health 2022, 19, 4690. [Google Scholar] [CrossRef] [PubMed]
- Waldron, C.-A.; van der Weijden, T.; Ludt, S.; Gallacher, J.; Elwyn, G. What are effective strategies to communicate cardiovascular risk information to patients? A systematic review. Patient Educ. Couns. 2011, 82, 169–181. [Google Scholar] [CrossRef]
- Occa, A.; Suggs, L.S. Communicating Breast Cancer Screening with Young Women: An Experimental Test of Didactic and Narrative Messages Using Video and Infographics. J. Health Commun. 2016, 21, 1–11. [Google Scholar] [CrossRef]
- Tan, M.L.; Lee, K.H.; Yong, W.S.; Rodgers, C. The effects of a video-based education in women with newly diagnosed breast cancer in Singapore. Support. Care Cancer 2018, 26, 3891–3897. [Google Scholar] [CrossRef]
- Blastland, M.; Freeman, A.L.; van der Linden, S.; Marteau, T.M.; Spiegelhalter, D. Five rules for evidence communication. Nature 2020, 587, 362–364. [Google Scholar] [CrossRef]
- Dey, S.; Mishra, A.; Govil, J.; Dhillon, P.K. Breast Cancer Awareness at the Community Level among Women in Delhi, India. Asian Pac. J. Cancer Prev. 2015, 16, 5243–5251. [Google Scholar] [CrossRef]
- Gupta, A.; Shridhar, K.; Dhillon, P. A review of breast cancer awareness among women in India: Cancer literate or awareness deficit? Eur. J. Cancer 2015, 51, 2058–2066. [Google Scholar] [CrossRef]
- Sayed, S.; Ngugi, A.K.; Mahoney, M.R.; Kurji, J.; Talib, Z.M.; Macfarlane, S.B.; Wynn, T.A.; Saleh, M.; Lakhani, A.; Nderitu, E.; et al. Breast Cancer knowledge, perceptions and practices in a rural Community in Coastal Kenya. BMC Public Health 2019, 19, 180. [Google Scholar] [CrossRef] [PubMed]
- Abdou, A.; Van Hal, G.; Dille, I. Awareness, attitudes and practices of women in relation to breast cancer in Niger. Heliyon 2020, 6, e04316. [Google Scholar] [CrossRef] [PubMed]
- Ullah, Z.; Khan, M.N.; Din, Z.U.; Afaq, S. Breast Cancer Awareness and Associated Factors Amongst Women in Peshawar, Pakistan: A Cross-Sectional Study. Breast Cancer: Basic Clin. Res. 2021, 15, 11782234211025346. [Google Scholar] [CrossRef] [PubMed]
- Solikhah, S.; Promthet, S.; Hurst, C. Awareness Level about Breast Cancer Risk Factors, Barriers, Attitude and Breast Cancer Screening among Indonesian Women. Asian Pac. J. Cancer Prev. 2019, 20, 877–884. [Google Scholar] [CrossRef]
- Hassan, E.E.; Seedhom, A.E.; Mahfouz, E.M. Awareness about Breast Cancer and Its Screening among Rural Egyptian Women, Minia District: A Population-Based Study. Asian Pac. J. Cancer Prev. 2017, 18, 1623–1628. [Google Scholar] [CrossRef]
- Moodley, J.; Constant, D.; Mwaka, A.D.; Scott, S.E.; Walter, F.M. Mapping awareness of breast and cervical cancer risk factors, symptoms and lay beliefs in Uganda and South Africa. PLoS ONE 2020, 15, e0240788. [Google Scholar] [CrossRef]
- Wang, Y.-J.; Wang, F.; Yu, L.-X.; Xiang, Y.-J.; Zhou, F.; Huang, S.-Y.; Zheng, C.; Fu, Q.-Y.; Li, L.; Gao, D.-Z.; et al. Worldwide review with meta-analysis of women’s awareness about breast cancer. Patient Educ. Couns. 2021, 105, 1818–1827. [Google Scholar] [CrossRef]
- Morère, J.-F.; Viguier, J.; Couraud, S.; Brignoli-Guibaudet, L.; Lhomel, C.; Pivot, X.B.; Eisinger, F. Awareness and Misconceptions of Breast Cancer Risk Factors Among Laypersons and Physicians. Curr. Oncol. Rep. 2018, 20 (Suppl. S1), 15. [Google Scholar] [CrossRef]
- Liu, L.; Wang, Y.-J.; Wang, F.; Yu, L.-X.; Xiang, Y.-J.; Zhou, F.; Li, L.; Zhang, Q.; Fu, Q.-Y.; Ma, Z.-B.; et al. Factors associated with insufficient awareness of breast cancer among women in Northern and Eastern China: A case–control study. BMJ Open 2018, 8, e018523. [Google Scholar] [CrossRef]
- Karayurt, Ö.; Özmen, D.; Çetinkaya, A.Ç. Awareness of breast cancer risk factors and practice of breast self exam-ination among high school students in Turkey. BMC Public Health 2008, 8, 359. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.-Y.; Wang, F.; Yu, L.-X.; Ma, Z.-B.; Zhang, Q.; Gao, D.-Z.; Li, Y.-Y.; Li, L.; Zhao, Z.-T.; Yu, Z.-G. Breast cancer awareness among women in Eastern China: A cross-sectional study. BMC Public Health 2014, 14, 1004. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Shrivastava, J.P.; Dwivedi, A. Breast cancer screening existence in India: A nonexisting reality. Oncol. Off. J. Indian Soc. Med. Paediatr. Oncol. 2015, 36, 207–209. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| S. No. | Participant Category | Age | Gender | Qualification | Employment | Marital Status | Monthly Household Income | Kuppuswamy Score |
|---|---|---|---|---|---|---|---|---|
| 1. | BC Patient 1 | 40 | Female | Graduate | Not employed | Married | 75,000 | Lower middle (III) |
| 2. | BC Patient 2 | 37 | Female | Postgraduate | Teacher | Married | 75,000 | Upper middle (II) |
| 3. | BC Patient 3 | 41 | Female | Postgraduate | Employed | Single | 150,000 | Upper (I) |
| 4. | BC Patient 4 | 41 | Female | Postgraduate | Employed | Married | 100,000 | Upper (I) |
| 5. | BC Patient 5 | 50 | Female | Postgraduate | Chartered accountant | Married | 300,000 | Upper (I) |
| 6. | BC Patient 6 | 50 | Female | Intermediate (12) | Not employed | Married | 15,000 | Upper lower (IV) |
| 7. | BC Patient 7 | 31 | Female | High school (9) | Not employed | Widow | 0 | Upper lower (IV) |
| 8. | Relative to BC 1 | 25 | Female | Postgraduate | Student | Single | 25,000 | Upper lower (IV) |
| 9. | Relative to BC 2 | 77 | Male | Postgraduate | Retired | Married | 15,000 | Lower middle (III) |
| 10. | Relative to BC 3 | 34 | Male | High school (10) | Driver | Married | 15,000 | Lower middle (III) |
| 11. | Relative to BC 4 | 27 | Male | High school (10) | Textile shop worker | Single | 4000 | Upper lower (IV) |
| 12. | Relative to BC 5 | 44 | Male | Postgraduate | Architecture | Married | 180,000 | Upper (I) |
| 13. | Relative to BC 6 | 55 | Male | Postgraduate | Chartered accountant | Married | 300,000 | Upper (I) |
| 14. | Lay public 1 | 30 | Female | Postgraduate | Public policy researcher | Single | 300,000 | Upper (I) |
| 15. | Lay public 2 | 21 | Female | No Formal Education | House help | Single | 13,000 | Upper lower (IV) |
| 16. | Lay public 3 | 44 | Female | Postgraduate | Not employed | Married | 100,000 | Upper middle (II) |
| 17. | Lay public 4 | 49 | Female | Graduate | Coordinator | Married | 40,000 | Upper middle (II) |
| 18. | Lay public 5 | 42 | Female | Middle School | Social worker | Married | 10,000 | Lower middle (III) |
| 19. | Lay public 6 | 21 | Female | Postgraduate | Student | Single | 120,000 | Upper middle (II) |
| 20. | Health Provider 1 | 32 | Female | Graduate | Nurse | Married | 130,000 | Upper middle (II) |
| 21. | Health Provider 2 | 34 | Female | Graduate | Nurse | Single | 80,000 | Upper middle (II) |
| 22. | Health Provider 3 | 22 | Female | Graduate | Physician assistant | Single | 20,000 | Upper middle (II) |
| 23. | Health Provider 4 | 34 | Female | Graduate | Nursing assistant | Married | 50,000 | Upper middle (II) |
| 24. | Health Provider 5 | 48 | Male | Postgraduate | Radiologist | Single | 100,000 | Upper (I) |
| 25. | Health Provider 6 | 46 | Female | Postgraduate | Pathologist | Married | 250,000 | Upper (I) |
| Participant Category | No. of Participants | Median Age (Min.–Max) | Median Income (Min.–Max) | Kuppuswamy Socio-Economic Status Scale 2020 | |||
|---|---|---|---|---|---|---|---|
| Upper (I) | Upper Middle (II) | Lower Middle (III) | Upper Lower (IV) | ||||
| BC patients | 7 | 41 (31–50) | 75,000 (0–300,000) | 43 | 14 | 14 | 29 |
| Relatives | 6 | 44 (25–77) | 20,000 (4000–300,000) | 33 | 0 | 33 | 33 |
| General public | 6 | 35 (21–49) | 70,000 (10,000–300,000) | 17 | 50 | 17 | 17 |
| Health professionals | 6 | 36 (22–48) | 90,000 (20,000–300,000) | 33 | 50 | 17 | 0 |
| Breast cancer and its diagnosis—varying levels of awareness | Lack of awareness of symptoms |
| Limited awareness of BC among the general public | |
| Poor knowledge among older women | |
| Misconceptions associated with diagnosis | |
| Limited awareness of patients and relatives of BC before the diagnosis | |
| Breast cancer risk factors —varying levels of awareness and some misconceptions | Limited understanding and knowledge of BC risk factors |
| Misconception that BC was a disease affecting women only | |
| Awareness that age was associated with increasing BC risk | |
| Some awareness about the hereditary nature of BC but no in-depth knowledge of genetic abnormalities/ BRCA pathogenic variants | |
| Higher awareness levels among graduates and younger generations | |
| Awareness that smoking and alcohol consumption were risk factors for lung and liver cancers but not breast cancer | |
| Misconception that BC was a communicable disease |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pillai, D.; Narayan, J.; Gentry-Maharaj, A.; Deo, S.; Vijaykumar, D.K.; Mukherjee, P.; Wadhwa, N.; Bhasin, A.; Mishra, A.; Rajanbabu, A.; et al. Co-Creation of Breast Cancer Risk Communication Tools and an Assessment of Risk Factor Awareness: A Qualitative Study of Patients and the Public in India. Cancers 2023, 15, 2973. https://doi.org/10.3390/cancers15112973
Pillai D, Narayan J, Gentry-Maharaj A, Deo S, Vijaykumar DK, Mukherjee P, Wadhwa N, Bhasin A, Mishra A, Rajanbabu A, et al. Co-Creation of Breast Cancer Risk Communication Tools and an Assessment of Risk Factor Awareness: A Qualitative Study of Patients and the Public in India. Cancers. 2023; 15(11):2973. https://doi.org/10.3390/cancers15112973
Chicago/Turabian StylePillai, Divya, Jyoti Narayan, Aleksandra Gentry-Maharaj, Suryanarayana Deo, Dehannathparambil Kottarathil Vijaykumar, Poulome Mukherjee, Nitya Wadhwa, Aparajita Bhasin, Ashutosh Mishra, Anupama Rajanbabu, and et al. 2023. "Co-Creation of Breast Cancer Risk Communication Tools and an Assessment of Risk Factor Awareness: A Qualitative Study of Patients and the Public in India" Cancers 15, no. 11: 2973. https://doi.org/10.3390/cancers15112973