
Disturbed Ratios between Essential and Toxic Trace Elements as Potential Biomarkers of Acute Ischemic Stroke
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Blood Sample Collection and Analysis
2.2. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Landrigan, P.J.; Fuller, R.; Acosta, N.J.R.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.B.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.I.; et al. The Lancet Commission on pollution and health. Lancet 2017, 391, 462–512. [Google Scholar] [CrossRef] [Green Version]
- Breathett, K.; Sims, M.; Gross, M.; Jackson, E.A.; Jones, E.J.; Navas-Acien, A.; Taylor, H.; Thomas, K.L.; Howard, B.V.; on behalf of the American Heart Association Council on Epidemiology and Prevention; et al. Cardiovascular Health in American Indians and Alaska Natives: A Scientific Statement From the American Heart Association. Circulation 2020, 141, e948–e959. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Brainin, M.; Norrving, B.; Martins, S.; Sacco, R.L.; Hacke, W.; Fisher, M.; Pandian, J.; Lindsay, P. World Stroke Organization (WSO): Global Stroke Fact Sheet 2022. Int. J. Stroke 2022, 17, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Long, P.; Liu, K.; Xiao, Y.; He, S.; Li, J.; Mo, T.; Liu, Y.; Yu, Y.; Wang, H.; et al. Multiple plasma metals, genetic risk and serum C-reactive protein: A metal-metal and gene-metal interaction study. Redox Biol. 2020, 29, 101404. [Google Scholar] [CrossRef] [PubMed]
- Bao, Q.J.; Zhao, K.; Guo, Y.; Wu, X.T.; Yang, J.C.; Yang, M.F. Environmental toxic metal contaminants and risk of stroke: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2022, 29, 32545–32565. [Google Scholar] [CrossRef]
- Kuźma, Ł.; Kurasz, A.; Dąbrowski, E.J.; Dobrzycki, S.; Bachórzewska-Gajewska, H. Short-Term Effects of “Polish Smog” on Cardiovascular Mortality in the Green Lungs of Poland: A Case-Crossover Study with 4,500,000 Person-Years (PL-PARTICLES Study). Atmosphere 2021, 12, 1270. [Google Scholar] [CrossRef]
- Omeljaniuk, W.J.; Socha, K.; Soroczynska, J.; Charkiewicz, A.E.; Laudanski, T.; Kulikowski, M.; Kobylec, E.; Borawska, M.H. Cadmium and lead in women who miscarried. Clin. Lab. 2018, 164, 59–67. [Google Scholar] [CrossRef]
- Socha, K.; Mielcarek, K.; Soroczyńska, J.; Puścion-Jakubik, A.; Karpińska, E.; Borawska, M.H. Content of cadmium and lead in freshwater smoked fish from Warmia and Masuria region. Probl. Hig. Epidemiol. 2018, 99, 79–81. (In Polish) [Google Scholar]
- Charkiewicz, A.E.; Backstrand, J.R. Lead Toxicity and Pollution in Poland. Int. J. Environ. Res. Public Health 2020, 18, 4385. [Google Scholar] [CrossRef]
- Mielcarek, K.; Nowakowski, P.; Puścion-Jakubik, A.; Gromkowska-Kępka, K.J.; Soroczyńska, J.; Markiewicz-Żukowska, R.; Naliwajko, S.K.; Grabia, M.; Bielecka, J.; Żmudzińska, A.; et al. Arsenic, cadmium, lead and mercury content and health risk assessment of consuming freshwater fish with elements of chemometric analysis. Food Chem. 2022, 379, 132167. [Google Scholar] [CrossRef]
- Lin, C.H.; Hsu, Y.T.; Yen, C.C.; Chen, H.H.; Tseng, C.J.; Lo, Y.K.; Chan, J.Y.H. Association between heavy metal levels and acute ischemic stroke. J. Biomed. Sci. 2018, 25, 49. [Google Scholar] [CrossRef]
- Li, Z.; Liu, Q.; Xu, Z.; Guo, X.; Wu, S. Association between short-term exposure to ambient particulate air pollution and biomarkers of oxidative stress: A meta-analysis. Environ. Res. 2020, 191, 110105. [Google Scholar] [CrossRef] [PubMed]
- Sall, M.L.; Diaw, A.K.D.; Gningue-Sall, D.; Efremova; Aaron, S.; Aaron, J.J. Toxic heavy metals: Impact on the environment and human health, and treatment with conducting organic polymers, a review. Environ. Sci. Pollut. Res. Int. 2020, 27, 29927–29942. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.; Huang, S.; Zhang, Y.; Zhang, H.; Zhou, L.; Li, D.; Xie, C.; Lv, Z.; Guo, Y.; Ke, Y.; et al. Associations of multiple plasma metals with the risk of ischemic stroke: A case-control study. Environ. Int. 2019, 125, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.C.; Chen, H.H.; Hsu, Y.T.; Tseng, C.J.; Lin, C.H. Effects of heavy metals in acute ischemic stroke patients: A cross-sectional study. Medicine 2022, 101, e28973. [Google Scholar] [CrossRef] [PubMed]
- Balali-Mood, M.; Naseri, K.; Tahergorabi, Z.; Khazdair, M.R.; Sadeghi, M. Toxic Mechanisms of Five Heavy Metals: Mercury, Lead, Chromium, Cadmium, and Arsenic. Front. Pharm. 2021, 12, 643972. [Google Scholar] [CrossRef]
- Liu, F.; Chen, X.; Liu, Y.; Niu, Z.; Tang, H.; Mao, S.; Li, N.; Chen, G.; Xiang, H. Serum cardiovascular-related metabolites disturbance exposed to different heavy metal exposure scenarios. J. Hazard. Mater. 2021, 415, 125590. [Google Scholar] [CrossRef]
- Patwa, J.; Flora, S.J.S. Heavy Metal-Induced Cerebral Small Vessel Disease: Insights into Molecular Mechanisms and Possible Reversal Strategies. Int. J. Mol. Sci. 2020, 21, 3862. [Google Scholar] [CrossRef]
- Renu, K.; Chakraborty, R.; Myakala, H.; Koti, R.; Ademola, C.; Famurewa, A.C.; Madhyastha, H.; Vellingiri, B.; George, A.; Gopalakrishnan, A.V. Molecular mechanism of heavy metals (Lead, Chromium, Arsenic, Mercury, Nickel and Cadmium)—induced hepatotoxicity—A review. Chemosphere 2021, 271, 129735. [Google Scholar] [CrossRef]
- Witkowska, D.; Słowik, J.; Chilicka, K. Heavy metals and human health: Possible exposure pathways and the competition for protein binding sites. Molecules 2021, 26, 6060. [Google Scholar] [CrossRef]
- Guo, X.; Su, W.; Li, N.; Song, Q.; Wang, H.; Liang, Q.; Li, Y.; Lowe, S.; Bentley, R.; Zhou, Z.; et al. Association of urinary or blood heavy metals and mortality from all causes, cardiovascular disease, and cancer in the general population: A systematic review and meta-analysis of cohort studies. Environ. Sci. Pollut. Res. Int. 2022, 29, 67483–67503. [Google Scholar] [CrossRef] [PubMed]
- Ruczaj, A.; Brzóska, M.M. Environmental exposure of the general population to cadmium as a risk factor of the damage to the nervous system: A critical review of current data. J. Appl. Toxicol. 2023, 43, 66–88. [Google Scholar] [CrossRef] [PubMed]
- Fagerberg, B.; Barregard, L. Review of cadmium exposure and smoking-independent effects on atherosclerotic cardiovascular disease in the general population. J. Intern. Med. 2021, 290, 1153–1179. [Google Scholar] [CrossRef] [PubMed]
- Borné, Y.; Fagerberg, B.; Sallsten, G.; Hedblad, B.; Persson, M.; Melander, O.; Nilsson, J.; Orho-Melander, M.; Barregard, L.; Engström, G. Biomarkers of blood cadmium and incidence of cardiovascular events in non-smokers: Results from a population-based proteomics study. Clin. Proteom. 2019, 16, 21. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, A.H.; Sears, C.G.; Harrington, J.; Howe, C.J.; James, K.A.; Roswall, N.; Overvad, K.; Tjønneland, A.; Wellenius, G.A.; Meliker, J.; et al. Urinary cadmium and stroke—A case-cohort study in Danish never-smokers. Environ. Res. 2021, 200, 111394. [Google Scholar] [CrossRef]
- Hecht, E.M.; Arheart, K.; Lee, D.J.; Hennekens, C.H.; Hlaing, W.M. A cross-sectional survey of cadmium biomarkers and cigarette smoking. Biomarkers 2016, 21, 429–435. [Google Scholar] [CrossRef]
- Bergström, G.; Fagerberg, B.; Sallsten, G.; Lundh, T.; Barregard, L. Is cadmium exposure associated with the burden, vulnerability and rupture of human atherosclerotic plaques? PLoS ONE 2015, 10, e0121240. [Google Scholar] [CrossRef] [Green Version]
- Wan, Y.; Mo, L.; Huang, H.; Mo, L.; Zhu, W.; Li, W.; Yang, G.; Chen, L.; Wu, Y.; Song, J.; et al. Cadmium contributes to atherosclerosis by affecting macrophage polarization. Food Chem. Toxicol. 2023, 173, 113603. [Google Scholar] [CrossRef]
- Oliveira, T.F.; Batista, P.R.; Leal, M.A.; Campagnaro, B.P.; Nogueira, B.V.; Vassallo, D.V.; Meyrelles, S.S.; Padilha, A.S. Chronic cadmium exposure accelerates the development of atherosclerosis and induces vascular dysfunction in the aorta of ApoE−/− Mice. Biol. Trace Elem. Res. 2019, 187, 163–171. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Filippini, T.; Ajsuvakova, O.P.; Skalnaya, M.G.; Aaseth, J.; Bjørklund, G.; Gatiatulina, E.R.; Popova, E.V.; Nemereshina, O.N.; Huang, P.T.; et al. Cadmium and atherosclerosis: A review of toxicological mechanisms and a meta-analysis of epidemiologic studies. Environ. Res. 2018, 162, 240–260. [Google Scholar] [CrossRef]
- Fagerberg, B.; Barregard, L.; Sallsten, G.; Forsgard, N.; Ostling, G.; Persson, M.; Borné, Y.; Engström, G.; Hedblad, B. Cadmium exposure and atherosclerotic carotid plaques--results from the Malmö diet and Cancer study. Environ. Res 2015, 136, 67–74. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Ramond, A.; O’Keeffe, L.M.; Shahzad, S.; Kunutsor, S.K.; Muka, T.; Gregson, J.; Willeit, P.; Warnakula, S.; Khan, H.; et al. Environmental toxic metal contaminants and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ Open 2018, 362, 14–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.D.; Oh, H.; Hoang, N.H.M.; Kim, M.S. Association between heavy metals, high-sensitivity C-reaction protein and 10-year risk of cardiovascular diseases among adult Korean population. Sci. Rep. 2021, 11, 14664. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Relloso, A.; Grau-Perez, M.; Briongos-Figuero, L.; Gomez-Ariza, J.L.; Garcia-Barrera, T.; Dueñas-Laita, A.; Bobb, J.F.; Chaves, F.J.; Kioumourtzoglou, M.-A.; Navas-Acien, A.; et al. The Association of Urine Metals and Metal Mixtures with Cardiovascular Incidence in an Adult Population from Spain: The Hortega Follow-Up Study. Int. J. Epidemiol. 2019, 48, 1839–1849. [Google Scholar] [CrossRef] [PubMed]
- Borne, Y.; Fagerberg, B.; Persson, M.; Ostling, G.; Söderholm, M.; Hedblad, B.; Sallsten, G.; Barregard, L.; Engström, G. Cadmium, carotid atherosclerosis, and incidence of ischemic stroke. J. Am. Heart Assoc. 2017, 6, e006415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tellez-Plaza, M.; Guallar, E.; Navas-Acien, A. Environmental metals and cardiovascular disease. BMJ 2018, 362, k3435. [Google Scholar] [CrossRef]
- Tellez-Plaza, M.; Guallar, E.; Howard, B.V.; Umans, J.G.; Francesconi, K.A.; Goessler, W.; Silbergeld, E.K.; Devereux, R.B.; Navas-Acien, A. Cadmium exposure and incident cardiovascular disease. Epidemiology 2013, 24, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Soderholm, M.; Borne, Y.; Hedblad, B.; Persson, M.; Barregard, L.; Engstrom, G. Blood cadmium concentration and risk of subarachnoid haemorrhage. Environ. Res. 2020, 180, 108826. [Google Scholar] [CrossRef]
- Xu, L.; Liu, Y.; Zhao, Q.; Du, H.; Gao, Y.; Bai, M.; Lv, J.; Guo, Y.; Li, L.; Sun, L.; et al. Urinary element profiles and associations with cardiometabolic diseases: A cross-sectional study across ten areas in China. Environ. Res. 2022, 205, 112535. [Google Scholar] [CrossRef]
- Ma, S.; Zhang, J.; Xu, C.; Da, M.; Xu, Y.; Chen, Y.; Mo, X. Increased serum levels of cadmium are associated with an elevated risk of cardiovascular disease in adults. Environ. Sci. Pollut. Res. Int. 2022, 29, 1836–1844. [Google Scholar] [CrossRef]
- Chen, C.; Xun, P.; Tsinovoi, C.; McClure, L.A.; Brockman, J.; MacDonald, L.; Cushman, M.; Cai, J.; Kamendulis, L.; Mackey, J.; et al. Urinary cadmium concentration and the risk of ischemic stroke. Neurology 2018, 91, e382–e391. [Google Scholar] [CrossRef] [Green Version]
- Jeong, J.; Yun, S.M.; Kim, M.; Koh, Y.H. Association of blood cadmium with cardiovascular disease in Korea: From the Korea National Health and Nutrition Examination Survey 2008–2013 and 2016. Int. J. Environ. Res. Public Health 2020, 17, 6288. [Google Scholar] [CrossRef] [PubMed]
- Nahan, K.S.; Walsh, K.B.; Adeoye, O.; Landero-Figueroa, J.A. The metal and metalloprotein profile of human plasma as biomarkers for stroke diagnosis. J. Trace Elem Med. Biol. 2017, 42, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Oliver-Williams, C.; Howard, A.G.; Navas-Acien, A.; Howard, B.V.; Tellez-Plaza, M.; Franceschini, N. Cadmium body burden, hypertension, and changes in blood pressure over time: Results from a prospective cohort study in american indians. J. Am. Soc. Hypertens 2018, 12, 426–437.e429. [Google Scholar] [CrossRef] [PubMed]
- Martins, A.C.; Santos, A.A.D.; Lopes, A.C.B.A.; Skalny, A.V.; Aschner, M.; Tinkov, A.A.; Paoliello, M.M.B. Endothelial Dysfunction Induced by Cadmium and Mercury and its Relationship to Hypertension. Curr. Hypertens. Rev. 2021, 17, 14–26. [Google Scholar] [CrossRef]
- Aramjoo, H.; Arab-Zozani, M.; Feyzi, A.; Naghizadeh, A.; Aschner, M.; Naimabadi, A.; Farkhondeh, T.; Samarghandian, S. The association between environmental cadmium exposure, blood pressure, and hypertension: A systematic review and meta-analysis. Environ. Sci. Pollut. Res. Int. 2022, 29, 35682–35706. [Google Scholar] [CrossRef]
- Ujueta, F.; Arenas, I.A.; Diaz, D.; Yates, T.; Beasley, R.; Navas-Acien, A.; Lamas, G.A. Cadmium level and severity of peripheral artery disease in patients with coronary artery disease. Eur. J. Prev. Cardiol. 2019, 26, 1456–1458. [Google Scholar] [CrossRef] [PubMed]
- Sears, C.G.; Poulsen, A.H.; Eliot, M.; Howe, C.J.; James, K.A.; Harrington, J.M.; Roswall, N.; Overvad, K.; Tjønneland, A.; Raaschou-Nielsen, O.; et al. Urine cadmium and acute myocardial infarction among never smokers in the Danish Diet, Cancer and Health cohort. Environ. Int. 2021, 150, 106428. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Chou, S.H.; Fan, P.C.; Zhu, Z.; Pan, J.; Li, J.; Chang, C.H.; Wu, V.C.; Chen, S.W.; Chu, P.H. The association between Day-1 urine cadmium excretion and 30-day mortality in patients with acute myocardial infarction: A multi-institutional cohort study. Int. J. Cardiol. 2023, 371, 397–401. [Google Scholar] [CrossRef]
- Wang, Z.; Sun, Y.; Yao, W.; Ba, Q.; Wang, H. Effects of Cadmium Exposure on the Immune System and Immunoregulation. Front. Immunol. 2021, 12, 695484. [Google Scholar] [CrossRef]
- Fagerberg, B.; Borne, Y.; Barregard, L.; Sallsten, G.; Forsgard, N.; Hedblad, B.; Persson, M.; Engstrom, G. Cadmium exposure is associated with soluble urokinase plasminogen activator receptor, a circulating marker of inflammation and future cardiovascular disease. Environ. Res. 2017, 152, 185–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinkov, A.A.; Filippini, T.; Ajsuvakova, O.; Aaseth, J.; Gluhcheva, Y.G.; Ivanova, J.; Bjørklund, G.; Skalnaya, M.; Gatiatulina, E.; Popova, E.V.; et al. The role of cadmium in obesity and diabetes. Sci. Total Environ. 2017, 601–602, 741–755. [Google Scholar] [CrossRef]
- Tinkov, A.A.; Aschner, M.; Ke, T.; Ferrer, B.; Zhou, J.-C.; Chang, J.-S.; Santamaría, A.; Chao, J.C.-J.; Aaseth, J.; Skalny, A.V. Adipotropic effects of heavy metals and their potential role in obesity. Fac. Rev. 2021, 10, 32. [Google Scholar] [CrossRef]
- Kim, M.; Yun, S.M.; Jeong, J.; Jo, C.; Koh, Y.H. Association between blood lead level and risk of stroke in Korean adults: A cross-sectional study in the Korea National Health and Nutrition Examination Survey 2008–2013. BMJ Open 2020, 10, e035725. [Google Scholar] [CrossRef] [PubMed]
- Lamas, G.A.; Ujueta, F.; Navas-Acien, A. Lead and Cadmium as Cardiovascular Risk Factors: The burden of proof has been met. J. Am. Heart Assoc. 2021, 10, e018692. [Google Scholar] [CrossRef]
- Zheng, X.; Huo, X.; Zhang, Y.; Wang, Q.; Zhang, Y.; Xu, X. Cardiovascular endothelial inflammation by chronic coexposure to lead (Pb) and polycyclic aromatic hydrocarbons from preschool children in an e-waste recycling area. Environ. Pollut. 2019, 246, 587–596. [Google Scholar] [CrossRef]
- Chen, Z.; Huo, X.; Chen, G.; Luo, X.; Xu, X. Lead (Pb) exposure and heart failure risk. Environ. Sci. Pollut. Res. 2021, 28, 28833–28847. [Google Scholar] [CrossRef] [PubMed]
- Byun, G.; Kim, S.; Kim, S.Y.; Park, D.; Shin, M.J.; Oh, H.; Lee, J.T. Blood lead concentrations and mortality in Korean adults: The Korea National Health and Nutrition examination survey with mortality follow-up. Int. J. Environ. Res. Public Health 2020, 17, 6898. [Google Scholar] [CrossRef]
- Mirończuk, A.; Kapica-Topczewska, K.; Socha, K.; Soroczyńska, J.; Jamiołkowski, J.; Kułakowska, A.; Kochanowicz, J. Selenium, Copper, Zinc Concentrations and Cu/Zn, Cu/Se Molar Ratios in the Serum of Patients with Acute Ischemic Stroke in Northeastern Poland-A New Insight into Stroke Pathophysiology. Nutrients 2021, 13, 2139. [Google Scholar] [CrossRef]
- Chung, J.W.; Park, S.H.; Kim, N.; Kim, W.J.; Park, J.H.; Ko, Y.; Yang, M.H.; Jang, M.S.; Han, M.K.; Jung, C.; et al. Trial of ORG 10172 in acute stroke treatment (TOAST) classification and vascular territory of ischemic stroke lesions diagnosed by diffusion-weighted imaging. J. Am. Heart Assoc. 2014, 3, e001119. [Google Scholar] [CrossRef] [Green Version]
- Yamal, J.M.; Grotta, J.C. National Institutes of Health Stroke Scale as an Outcome Measure for Acute Stroke Trials. Stroke 2021, 52, 142–143. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef]
- Dembińska-Kieć, A.; Solnica, B.; Naskalski, J. Diagnostyka Laboratoryjna z Elementami Biochemii Klinicznej, 4th ed.; Edra Urban & Partner: Wrocław, Poland, 2017; p. 23. (In Polish) [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, version 26.0, Released 2019; IBM Corp: Armonk, NY, USA, 2019.
- Barregard, L.; Sallsten, G.; Fagerberg, B.; Borné, Y.; Persson, M.; Hedblad, B.; Engström, G. Blood cadmium levels and incident cardiovascular events during follow-up in a population-based cohort of Swedish adults: The Malmo diet and cancer study. Environ. Health Perspect. 2016, 124, 594–600. [Google Scholar] [CrossRef]
- Dev, P.; Gupta, P.; Mahapatra, A.; Cyriac, M.; Kumar, A.; Singh, V.K.; Mishra, V.N.; Pathak, A. Systematic Review and Meta-analysis of Environmental Toxic Metal Contaminants and the Risk of Ischemic Stroke. Ann. Indian Acad. Neurol. 2022, 25, 1159–1166. [Google Scholar]
- Shi, L.; Yuan, Y.; Xiao, Y.; Long, P.; Li, W.; Yu, Y.; Liu, Y.; Liu, K.; Wang, H.; Zhou, L.; et al. Associations of plasma metal concentrations with the risks of all-cause and cardiovascular disease mortality in Chinese adults. Environ. Int. 2021, 157, 106808. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Yuan, Y.; Liu, Y.; Yu, Y.; Jia, N.; Zhou, L.; Wang, H.; Huang, S.; Zhang, Y.; Yang, H.; et al. Circulating Multiple Metals and Incident Stroke in Chinese Adults. Stroke 2019, 50, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Yim, G.; Wang, Y.; Howe, C.G.; Romano, M.E. Exposure to Metal Mixtures in Association with Cardiovascular Risk Factors and Outcomes: A Scoping Review. Toxics 2022, 10, 116. [Google Scholar] [CrossRef]
- Mukherjee, A.G.; Renu, K.; Gopalakrishnan, A.V.; Veeraraghavan, V.P.; Vinayagam, S.; Paz-Montelongo, S.; Dey, A.; Vellingiri, B.; George, A.; Madhyastha, H.; et al. Heavy Metal and Metalloid Contamination in Food and Emerging Technologies for Its Detection. Sustainability 2023, 15, 1195. [Google Scholar] [CrossRef]
- Messner, B.; Knoflach, M.; Seubert, A.; Ritsch, A.; Pfaller, K.; Henderson, B.; Shen, Y.H.; Zeller, I.; Willeit, J.; Laufer, G.; et al. Cadmium is a novel and independent risk factor for early atherosclerosis mechanisms and in vivo relevance. Arter. Thromb. Vasc. Biol. 2009, 29, 1392–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messner, B.; Bernhard, D. Smoking and cardiovascular disease: Mechanisms of endothelial dysfunction and early atherogenesis. Arter. Thromb. Vasc. Biol. 2014, 34, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Fagerberg, B.; Borné, Y.; Sallsten, G.; Smith, J.G.; Acosta, S.; Persson, M.; Melander, O.; Forsgard, N.; Gottsäter, A.; Hedblad, B.; et al. Circulating cadmium concentration and risk of aortic aneurysms: A nested casecontrol study within the Malmö Diet and Cancer cohort. Atherosclerosis 2017, 261, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Mao, Y.; Liu, Z.; Li, Y.; Li, Z.; Sun, Y.; Ding, Y.; Liu, X.; Hong, J.; Xu, D.; et al. Association of Blood Heavy Metal Exposure with Atherosclerotic Cardiovascular Disease (ASCVD) Among White Adults: Evidence from NHANES 1999-2018. Biol. Trace Elem. Res 2022. [Google Scholar] [CrossRef] [PubMed]
- Borné, Y.; Barregard, L.; Persson, M.; Hedblad, B.; Fagerberg, B.; Engström, G. Cadmium exposure and incidence of heart failure and atrial fibrillation: A population-based prospective cohort study. BMJ Open 2015, 5, e007366. [Google Scholar] [CrossRef] [PubMed]
- Lind, P.M.; Olsén, L.; Lind, L. Circulating levels of metals are related to carotid atherosclerosis in elderly. Sci. Total Environ. 2012, 416, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Melough, M.M.; Vance, T.M.; Kim, D.; Noh, H.; Koo, S.I.; Chun, O.K. The relationship between zinc intake and cadmium burden is influenced by smoking status. Food Chem. Toxicol. 2019, 125, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Hecht, E.M.; Landy, D.C.; Ahn, S.; Hlaing, W.M.; Hennekens, C.H. Hypothesis: Cadmium explains, in part, why smoking increases the risk of cardiovascular disease. J. Cardiovasc. Pharm. 2013, 18, 550–554. [Google Scholar] [CrossRef]
- Martins, A.C.; Urbano, M.R.; Almeida Lopes, A.C.B.; Carvalho, M.F.H.; Buzzo, M.L.; Docea, A.O.; Mesas, A.E.; Aschner, M.; Silva, A.M.R.; Silbergeld, E.K.; et al. Blood cadmium levels and sources of exposure in an adult urban population in southern Brazil. Environ. Res. 2020, 187, 109618. [Google Scholar] [CrossRef]
- Li, C.; Sun, H.; Arrick, D.M.; Mayhan, W.G. Chronic nicotine exposure exacerbates transient focal cerebral ischemia-induced brain injury. J. Appl. Physiol. 2016, 120, 328–333. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Colditz, G.A.; Stampfer, M.J. Smoking cessation and decreased risk of stroke in women. JAMA 1993, 269, 232–236. [Google Scholar] [CrossRef]
- Jiang, C.Q.; Xu, L.; Lam, T.H.; Lin, J.M.; Cheng, K.K.; Thomas, G.N. Smoking cessation and carotid atherosclerosis: The Guangzhou Biobank Cohort Study–CVD. J. Epidemiol. Commun. Health 2010, 64, 1004–1009. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Xu, Y.; Huang, Z.; Wei, Y.; Hou, J.; Long, T.; Wang, F.; Cheng, X.; Duan, Y.; Chen, X.; et al. Association of Multiple Metals with Lipid Markers against Different Exposure Profiles: A Population-Based Cross-Sectional Study in China. Chemosphere 2021, 264, 128505. [Google Scholar] [CrossRef]
- Zhong, Q.; Wu, H.; Niu, Q.; Jia, P.P.; Qin, Q.R.; Wang, X.D.; He, J.L.; Yang, W.J.; Huang, F. Exposure to Multiple Metals and the Risk of Hypertension in Adults: A Prospective Cohort Study in a Local Area on the Yangtze River, China. Environ. Int. 2021, 153, 106538. [Google Scholar] [CrossRef]
- Yang, A.M.; Lo, K.; Zheng, T.Z.; Yang, J.L.; Bai, Y.N.; Feng, Y.Q.; Cheng, N.; Liu, S.M. Environmental heavy metals and cardiovascular diseases: Status and future direction. Chronic Dis. Transl. Med. 2020, 6, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Zhen, J.; Leng, J.; Cai, L.; Ji, H.L.; Keller, B.B. Zinc as a Countermeasure for Cadmium Toxicity. Acta Pharmacol. Sin. 2021, 42, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Q.; Narbad, A.; Chen, W. Dietary strategies for the treatment of cadmium and lead toxicity. Nutrients 2015, 7, 552–571. [Google Scholar] [CrossRef] [Green Version]
- Obeng-Gyasi, E. Chronic cadmium exposure and cardiovascular disease in adults. J. Environ. Sci. Health Part A 2020, 55, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Noor, N.; Zong, G.; Seely, E.W.; Weisskopf, M.; James-Todd, T. Urinary cadmium concentrations and metabolic syndrome in U.S. adults: The National Health and Nutrition Examination Survey 2001–2014. Environ. Int. 2018, 121, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Weng, Z.; Zhang, L.; Xu, J.; Dahal, M.; Basnet, T.B.; Gu, A. HDL cholesterol: A potential mediator of the association between urinary cadmium concentration and cardiovascular disease risk. Ecotoxicol. Environ. Saf. 2021, 208, 111433. [Google Scholar] [CrossRef]
- Zhu, X.; Fan, Y.; Sheng, J.; Gu, L.; Tao, Q.; Huang, R.; Liu, K.; Yang, L.; Chen, G.; Cao, H.; et al. Association between blood heavy metal concentrations and dyslipidemia in the elderly. Biol. Trace Elem. Res. 2021, 199, 1280–1290. [Google Scholar] [CrossRef]
- Jiang, Q.; Xiao, Y.; Long, P.; Li, W.; Yu, Y.; Liu, Y.; Liu, K.; Zhou, L.; Wang, H.; Yang, H.; et al. Associations of plasma metal concentrations with incident dyslipidemia: Prospective findings from the Dongfeng-Tongji cohort. Chemosphere 2021, 285, 131497. [Google Scholar] [CrossRef]
- Zhao, M.; Yin, G.; Xu, J.; Ge, X.; Li, A.; Mei, Y.; Wu, J.; Liu, X.; Wei, L.; Xu, Q. Independent, combine and interactive effects of heavy metal exposure on dyslipidemia biomarkers: A cross-sectional study in northeastern China. Ecotoxicol. Environ. Saf. 2023, 250, 114494. [Google Scholar] [CrossRef]
- Xu, H.; Mao, Y.; Xu, B.; Hu, Y. Low-level environmental lead and cadmium exposures and dyslipidemia in adults: Findings from the NHANES 2005-2016. J. Trace Elem. Med. Biol. 2021, 63, 126651. [Google Scholar] [CrossRef]
- Xu, C.; Shu, Y.; Fu, Z.; Hu, Y.; Mo, X. Associations between lead concentrations and cardiovascular risk factors in US adolescents. Sci. Rep. 2017, 7, 9121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skalny, A.V.; Klimenko, L.L.; Turna, A.A.; Budanova, M.N.; Baskakov, I.S.; Savostina, M.S.; Mazilina, A.N.; Deyev, A.I.; Skalnaya, M.G.; Tinkov, A.A. Serum trace elements are associated with hemostasis, lipid spectrum and inflammatory markers. in men suffering from acute ischemic stroke. Metab. Brain Dis. 2017, 32, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Mousavi-Mirzaei, S.M.; Khorasani, E.Y.; Amirabadizadeh, A.; Nakhaee, S.; Baharshahi, A.; Rajabpour-Sanati, A.; Talebi, A.; Lamarine, R.J.; Mehrpour, M.; Mehrpour, O. Comparison of blood lead concentrations in patients with acute ischemic stroke and healthy subjects. J. Trace Elem. Med. Biol. 2020, 61, 126532. [Google Scholar] [CrossRef] [PubMed]
- Rogalska, J.; Brzóska, M.M.; Roszczenko, A.; Moniuszko-Jakoniuk, J. Enhanced zinc consumption prevents cadmium-induced alterations in lipid metabolism in male rats. Chem. Biol. Interact 2009, 177, 142–152. [Google Scholar] [CrossRef]
- Xiao, L.; Zhou, Y.; Ma, J.; Cao, L.; Zhu, C.; Li, W.; Wang, D.; Fan, L.; Ye, Z.; Chen, W. Roles of C-reactive protein on the association between urinary cadmium and type 2 diabetes. Environ. Pollut. 2019, 255, 113341. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Yang, S.K.; Kim, J.; Lee, D.-C. Association between C-reactive protein and metabolic syndrome in Korean adults. Korean J. Fam. Med. 2019, 40, 116. [Google Scholar] [CrossRef] [Green Version]
- Asgary, S.; Movahedian, A.; Keshvari, M.; Taleghani, M.; Sahebkar, A.; Sarrafzadegan, N. Serum levels of lead, mercury and cadmium in relation to coronary artery disease in the elderly: A cross-sectional study. Chemosphere 2017, 180, 540–544. [Google Scholar] [CrossRef]
- Skalny, A.V.; Kopylov, P.Y.; Paoliello, M.M.B.; Chang, J.S.; Aschner, M.; Bobrovnitsky, I.P.; Chao, J.C.; Aaseth, J.; Chebotarev, S.N.; Tinkov, A.A. Hair Lead, Aluminum, and Other Toxic Metals in Normal-Weight and Obese Patients with Coronary Heart Disease. Int. J. Environ. Res. Public Health 2021, 18, 8195. [Google Scholar] [CrossRef]
- Wang, X.; Mukherjee, B.; Park, S.K. Associations of cumulative exposure to heavy metal mixtures with obesity and its comorbidities among U.S. adults in NHANES 2003–2014. Environ. Int. 2018, 121, 683–694. [Google Scholar] [CrossRef]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.C.; Liu, C.C.; Lin, Y.C.; Hsu, C.W. Epigallocatechin Gallate Modulates Essential Elements, Zn/Cu Ratio, Hazardous Metal, Lipid Peroxidation, and Antioxidant Activity in the Brain Cortex during Cerebral Ischemia. Antioxidants 2022, 11, 396. [Google Scholar] [CrossRef] [PubMed]
- Ro, J.H.; Liu, C.C.; Lin, M.C. Resveratrol Mitigates Cerebral Ischemic Injury by Altering Levels of Trace Elements, Toxic Metal, Lipid Peroxidation, and Antioxidant Activity. Biol. Trace Elem. Res. 2021, 199, 3718–3727. [Google Scholar] [CrossRef]
- Zhang, T.; Yin, X.; Zhang, Y.; Chen, H.; Man, J.; Li, Y.; Chen, J.; Yang, X.; Lu, M. Global Trends in Mortality and Burden of Stroke Attributable to Lead Exposure From 1990 to 2019. Front. Cardiovasc. Med. 2022, 9, 870747. [Google Scholar] [CrossRef]
- Chen, C.; Li, Q.; Nie, X.; Han, B.; Chen, Y.; Xia, F.; Zhai, H.; Wang, N.; Lu, Y. Association of lead exposure with cardiovascular risk factors and diseases in Chinese adults. Environ. Sci. Pollut. Res. Int. 2017, 24, 22275–22283. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.-Y.; Staessen, J.A. Letter to editor: Blood pressure, hypertension and lead exposure. Environ. Health 2018, 17, 16. [Google Scholar] [CrossRef] [Green Version]
- Steenland, K.; Barry, V.; Anttila, A.; Sallmén, M.; McElvenny, D.; Todd, A.C.; Straif, K. A cohort mortality study of lead-exposed workers in the USA, Finland and the UK. Occup. Environ. Med. 2017, 74, 785–791. [Google Scholar] [CrossRef] [Green Version]
- Klimenko, L.L.; Skalny, A.V.; Turna, A.A.; Tinkov, A.A.; Budanova, M.N.; Baskakov, I.S.; Savostina, M.S.; Mazilina, A.N.; Deev, A.I.; Nikonorov, A.A. Serum Trace Element Profiles, Prolactin, and Cortisol in Transient Ischemic Attack Patients. Biol. Trace Elem. Res. 2016, 172, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Hernandez, A.; Navas-Acien, A.; Pastor-Barriuso, R.; Crainiceanu, C.M.; Redon, J.; Guallar, E.; Tellez-Plaza, M. Declining exposures to lead and cadmium contribute to explaining the reduction of cardiovascular mortality in the US population, 1988–2004. Int. J. Epidemiol. 2017, 46, 1903–1912. [Google Scholar] [CrossRef] [Green Version]
- Medina-Estévez, F.; Zumbado, M.; Luzardo, O.P.; Rodríguez-Hernández, Á.; Boada, L.D.; Fernández-Fuertes, F.; Santandreu-Jimenez, M.E.; Henríquez-Hernández, L.A. Association between Heavy Metals and Rare Earth Elements with Acute Ischemic Stroke: A Case-Control Study Conducted in the Canary Islands (Spain). Toxics 2020, 8, 66. [Google Scholar] [CrossRef] [PubMed]
- Nigra, A.E.; Ruiz-Hernandez, A.; Redon, J.; Navas-Acien, A.; Tellez-Plaza, M. Environmental Metals and Cardiovascular Disease in Adults: A Systematic Review Beyond Lead and Cadmium. Curr. Environ. Health Rep. 2016, 3, 416–433. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinical Parameters | AIS Patients (n = 187) | Controls (n = 94) | p * |
|---|---|---|---|
| Gender (M n (%)/F n (%)) | 96 (51.3%)/91 (48.7%) | 37 (39.4%)/57 (60.6%) | 0.058 |
| Age (years) median (Q1–Q3) | 69 (63;76) | 56.5 (40;65) | <0.05 |
| BMI (Kg/M2) median (Q1–Q3) | 27 (24.6; 30.4) | 25.2 (22.9; 27.8) | <0.05 |
| Total cholesterol (TC) (mg/dL) median (Q1–Q3) | 185.5 (150;219.3) | ** | ** |
| Triglyceride (TG) (mg/dL) median (Q1–Q3) | 106 (79;137.8) | ** | ** |
| Low-density lipoprotein cholesterol (LDL-C) (mg/dL) median (Q1–Q3) | 122 (92,156.3) | ** | ** |
| High-density lipoprotein cholesterol (HDL-C) (mg/dL) median (Q1–Q3) | 47 (38;56) | ** | ** |
| Hypertension n (%) | 166 (88.8%) | ** | ** |
| Diabetes mellitus n (%) | 65 (34.8%) | ** | ** |
| Smokers n (%) | 83 (44.4%) | ** | ** |
| Obese n (%) BMI ≥ 25 | 133 (71%) | 51 (54.3%) | ** |
| C-reactive protein (CRP) (mg/L) median (Q1–Q3) | 3.1 (1.5;6.2) | ** | ** |
| Brain lesion size (mm2) median (Q1–Q3) | 440 (169;1225) | ** | ** |
| Lesion location (R n(%)/L n(%) hemisphere) | 80 (42.8%)/93 (49.7%), both 14 (7.5%) | ** | ** |
| NIHSS on admission median (Q1–Q3) | 8 (6;12) | ** | ** |
| NIHSS at discharge median (Q1–Q3) | 3 (1;5) | ** | ** |
| MRS scale median (Q1–Q3) | 2 (0;6) | ** | ** |
| HbA1c (%) median (Q1–Q3) | 5.9 (5.6;6.3) | ** | ** |
| Creatinine (mg/dL) median (Q1–Q3) | 0.85 (0.73;1) | ** | ** |
| Highly sensitive troponin (ng/L) median (Q1–Q3) | 10 (10;12.2) | ** | ** |
| Fibrinogen (mg/dL) median (Q1–Q3) | 370 (320;437) | ** | ** |
| D-dimer (µg/mL) median (Q1–Q3) | 0.8 (0.4;1.5) | ** | ** |
| Uric acid (mg/dL) median (Q1–Q3) | 5.3 (4.2;6.9) | ** | ** |
| Hemoglobin (g/dL) median (Q1–Q3) | 13.7 (12.8;14.8) | ** | ** |
| Homocysteine (µmol/L) median (Q1–Q3) | 11 (8.9;14.7) | ** | ** |
| Intervention treatment (T ± MT) n (%) | 85 (45.5%) | ** | ** |
| Trombolysis (T) n (%) | 73 (39%) | ** | ** |
| Mechanical thrombectomy (MT) n (%) | 32 (17.1%) | ** | ** |
| Hyperlipidemia n (%) | 146 (78.5%) | ** | ** |
| Atrial fibrillation n (%) | 62 (33.2%) | ** | ** |
| Carotid atherosclerosis | 148 (79.1%) | ** | ** |
| >30% stenosis n (%) | 47 (25.2%) | ** | ** |
| TOAST classification | 187 (100%) | ** | ** |
| LAA n (%) | 69 (36.9%) | ** | ** |
| SVO n (%) | 42 (22.5%) | ** | ** |
| CE n (%) | 76 (40.6%) | ** | ** |
| AIS Patients | Controls | p * | ||
|---|---|---|---|---|
| Cd [μg/L] [63] | Total | 1.8 (1.1–2.5) | 1.2 (0.8–1.9) | <0.001 |
| Males | 1.9 (1.2–2.5) | 1.2 (0.7–2) | ||
| Females | 1.7 (1–2.4) | 1.2 (0.9–1.6) | ||
| p ** | 0.128 | 0.786 | ||
| Pb [μg/L] [63] | Total | 26.2 (16.8–42.3) | 31.3 (19.6–46.3) | 0.223 |
| Males | 27.4 (18.2–41.1) | 36.8 (23.7–48.1) | ||
| Females | 25.1 (14.4–43) | 27.2 (17.7–43.2) | ||
| p ** | 0.274 | 0.064 | ||
| Cd/Zn molar ratio *** | Total | 0.0016 (0.0010–0.0024) | 0.0009 (0.0005–0.0014) | <0.001 |
| Males | 0.0016 (0.0011–0.0027) | 0.0010 (0.0005–0.0015) | ||
| Females | 0.0014 (0.0010–0.0023) | 0.0008 (0.0006–0.0013) | ||
| p ** | 0.329 | 0.911 | ||
| Cu/Cd molar ratio *** | Total | 968.6 (621–1447.2) | 1680 (829.7–2376.4) | <0.001 |
| Males | 909.3 (553–1396) | 1247.1 (829.7–2376.4) | ||
| Females | 1073.1 (704.5–1660.2) | 1836.3 (1050–2413.4) | ||
| p ** | 0.033 | 0.217 | ||
| Se/Cd molar ratio *** | Total | 44.6 (30–75.3) | 88.1 (55.1–141.1) | <0.001 |
| Males | 42.7 (26.5–70.1) | 78.9 (54.8–182.3) | ||
| Females | 49.1 (30.8–85.8) | 92.6 (57.1–132.8) | ||
| p ** | 0.189 | 0.911 | ||
| Cd/Pb molar ratio *** | Total | 0.12 (0.07–0.19) | 0.08 (0.05–0.13) | 0.001 |
| Males | 0.12 (0.07–0.18) | 0.07 (0.04–0.12) | ||
| Females | 0.11 (0.07–0.20) | 0.08 (0.05–0.14) | ||
| p ** | 0.802 | 0.056 | ||
| Se/Pb molar ratio *** | Total | 5.7 (3.2–9) | 6.5 (4.6–10.4) | <0.001 |
| Males | 5.2 (3–8.6) | 6.2 (4.2–8.4) | ||
| Females | 6.2 (3.4–9.2) | 6.7 (4.8–12.4) | ||
| p ** | 0.236 | 0.108 | ||
| Zn/Pb molar ratio *** | Total | 71.4 (45.6–126.8) | 87 (53.4–146.2) | 0.059 |
| Males | 76.9 (39.7–112.9) | 73.1 (52.6–99.2) | ||
| Females | 68 (47.6–134.7) | 97.1 (54–164.5) | ||
| p ** | 0.467 | 0.08 | ||
| Cu/Pb molar ratio *** | Total | 120.9 (62.3–201) | 103.8 (70.9–211.1) | 0.898 |
| Males | 105.1 (57.5–176) | 85.5 (57.7–130.0) | ||
| Females | 128.2 (69.8–254.7) | 134.4 (86.2–241.6) | ||
| p ** | 0.107 | 0.001 | ||
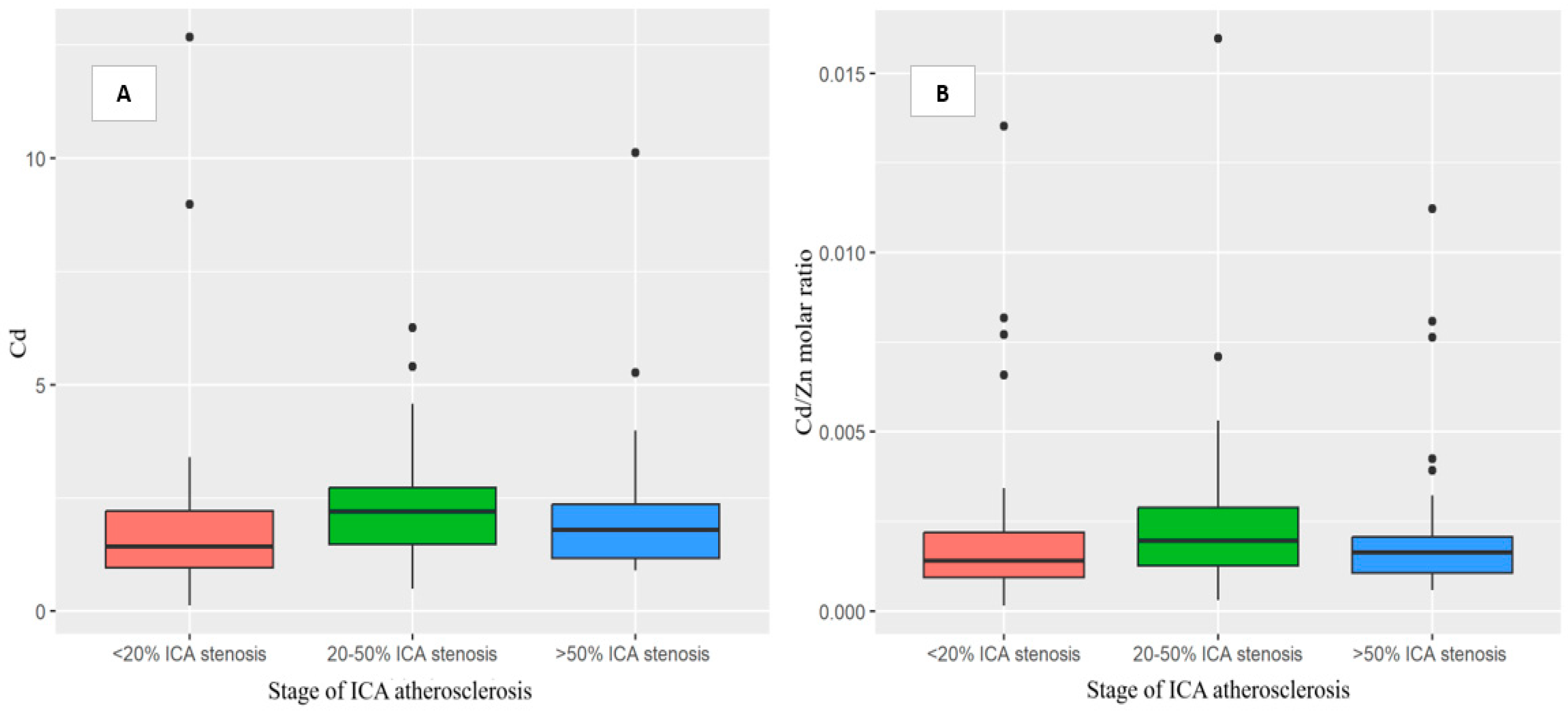
| Stage of ICA Atherosclerosis | ||||||
|---|---|---|---|---|---|---|
| Total | Smokers | Never-Smokers | ||||
| r | p | r | p | r | p | |
| Cd | 0.24 | * 0.001 | 0.08 | 0.457 | 0.16 | 0.095 |
| Pb | 0.06 | 0.423 | 0.05 | 0.679 | 0.05 | 0.617 |
| Zn | 0.11 | 0.152 | 0.01 | 0.920 | 0.23 | * 0.02 |
| Cu | 0.02 | 0.768 | 0.00 | 0.999 | 0.08 | 0.430 |
| Se | −0.04 | 0.628 | −0.12 | 0.292 | 0.06 | 0.567 |
| Cu/Cd molar ratio | −0.18 | * 0.014 | −0.10 | 0.363 | −0.06 | 0.565 |
| Se/Cd molar ratio | −0.23 | * 0.002 | −0.15 | 0.168 | −0.12 | 0.218 |
| Cd/Pb molar ratio | 0.11 | 0.150 | 0.04 | 0.746 | 0.03 | 0.734 |
| Se/Pb molar ratio | −0.08 | 0.296 | −0.09 | 0.435 | −0.04 | 0.668 |
| Zn/Pb molar ratio | −0.05 | 0.532 | −0.08 | 0.489 | 0.02 | 0.862 |
| Cd/Zn molar ratio | 0.15 | * 0.037 | 0.04 | 0.720 | 0.02 | 0.822 |
| Cu/Zn molar ratio | −0.03 | 0.723 | 0.00 | 1.000 | −0.11 | 0.278 |
| Cu/Pb molar ratio | −0.04 | 0.567 | −0.04 | 0.688 | −0.02 | 0.831 |
| Cadmium (A) | ||||
|---|---|---|---|---|
| Variable | B | 95% C.I. | p | |
| SEX M (vs. F) | 0.037 | −0.478 | 0.552 | 0.889 |
| Treatment conservative (vs. intervention) | 0.060 | −0.385 | 0.505 | 0.792 |
| Smoking status | 1.240 | 0.784 | 1.695 | * 0.000 |
| Stage of ICA atherosclerosis: >50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 0.376 | −0.212 | 0.964 | 0.210 |
| Stage of ICA atherosclerosis: 20–50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 0.228 | −0.254 | 0.710 | 0.354 |
| Diabetes mellitus type 2 | 0.037 | −0.438 | 0.512 | 0.879 |
| Atrial fibrillation | 0.653 | 0.162 | 1.144 | * 0.009 |
| Age | 0.021 | 0.001 | 0.041 | * 0.038 |
| Brain lesion size (mm2) | 0.000 | 0.000 | 0.000 | 0.617 |
| NIHSS on admission | −0.067 | −0.125 | −0.008 | * 0.025 |
| BMI index | −0.057 | −0.114 | 0.000 | 0.050 |
| HDL-C | −0.001 | −0.018 | 0.017 | 0.931 |
| LDL-C | −0.002 | −0.007 | 0.002 | 0.276 |
| TG | −0.002 | −0.004 | 0.001 | 0.142 |
| CRP | −0.045 | −0.120 | 0.031 | 0.249 |
| Hemoglobin | 0.086 | −0.073 | 0.245 | 0.292 |
| Creatinine | −0.022 | −0.811 | 0.768 | 0.957 |
| D-dimer | 0.016 | −0.058 | 0.091 | 0.667 |
| Fibrinogen | 0.001 | −0.002 | 0.003 | 0.695 |
| Lead (B) | ||||
| Variable | B | 95% C.I. | p | |
| SEX M (vs. F) | −2.760 | −18.990 | 13.470 | 0.739 |
| Treatment conservative (vs. intervention) | 16.920 | 2.887 | 30.953 | * 0.018 |
| Smoking status | −9.728 | −24.092 | 4.636 | 0.184 |
| Stage of ICA atherosclerosis: >50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 25.007 | 6.480 | 43.535 | * 0.008 |
| Stage of ICA atherosclerosis: 20–50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 8.593 | −6.603 | 23.788 | 0.268 |
| Diabetes mellitus type 2 | 6.990 | −7.990 | 21.969 | 0.360 |
| Atrial fibrillation | 5.503 | −9.963 | 20.969 | 0.486 |
| Age | −0.257 | −0.882 | 0.368 | 0.420 |
| Brain lesion size | −0.001 | −0.012 | 0.009 | 0.791 |
| NIHSS on admission | −0.683 | −2.524 | 1.158 | 0.467 |
| BMI index | −0.341 | −2.137 | 1.455 | 0.710 |
| HDL-C | 0.325 | −0.231 | 0.882 | 0.252 |
| LDL-C | 0.006 | −0.132 | 0.143 | 0.937 |
| TG | −0.053 | −0.120 | 0.014 | 0.121 |
| CRP | −0.107 | −2.497 | 2.284 | 0.930 |
| Hemoglobin | 5.946 | 0.932 | 10.961 | * 0.020 |
| Creatinine | 17.904 | −6.976 | 42.784 | 0.158 |
| D-dimer | −1.486 | −3.847 | 0.875 | 0.217 |
| Fibrinogen | 0.026 | −0.055 | 0.106 | 0.533 |
| Cd/Zn molar ratio (C) | ||||
| Variable | B | 95% C.I. | p | |
| SEX M (vs. F) | −0.00016 | −0.00091 | 0.00059 | 0.680 |
| Treatment conservative (vs. intervention) | 0.00029 | −0.00036 | 0.00093 | 0.388 |
| Smoking status | 0.00158 | 0.00092 | 0.00224 | * 0.000 |
| Stage of ICA atherosclerosis: >50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 0.00010 | −0.00076 | 0.00095 | 0.823 |
| Stage of ICA atherosclerosis: 20–50% ICA atherosclerosis (vs. <20% ICA atherosclerosis) | 0.00033 | −0.00037 | 0.00103 | 0.354 |
| Diabetes mellitus type 2 | 0.00019 | −0.00050 | 0.00088 | 0.595 |
| Atrial fibrillation | 0.00055 | −0.00016 | 0.00126 | 0.131 |
| Age | 0.00003 | 0.00000 | 0.00006 | * 0.032 |
| Brain lesion size (mm2) | 0.00000 | 0.00000 | 0.00000 | 0.817 |
| NIHSS on admission | −0.00003 | −0.00012 | 0.00005 | 0.443 |
| BMI index | −0.00011 | −0.00019 | −0.00003 | * 0.010 |
| HDL-C | 0.00000 | −0.00002 | 0.00003 | 0.769 |
| LDL-C | 0.00000 | −0.00001 | 0.00000 | 0.169 |
| TG | 0.00000 | 0.00000 | 0.00000 | 0.368 |
| CRP | −0.00008 | −0.00019 | 0.00003 | 0.172 |
| Hemoglobin | 0.00022 | −0.00001 | 0.00045 | 0.062 |
| Creatinine | 0.00036 | −0.00078 | 0.00151 | 0.535 |
| D-dimer | −0.00001 | −0.00012 | 0.00010 | 0.854 |
| Fibrinogen | 0.00000 | 0.00000 | 0.00000 | 0.814 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirończuk, A.; Kapica-Topczewska, K.; Socha, K.; Soroczyńska, J.; Jamiołkowski, J.; Chorąży, M.; Czarnowska, A.; Mitrosz, A.; Kułakowska, A.; Kochanowicz, J. Disturbed Ratios between Essential and Toxic Trace Elements as Potential Biomarkers of Acute Ischemic Stroke. Nutrients 2023, 15, 1434. https://doi.org/10.3390/nu15061434
Mirończuk A, Kapica-Topczewska K, Socha K, Soroczyńska J, Jamiołkowski J, Chorąży M, Czarnowska A, Mitrosz A, Kułakowska A, Kochanowicz J. Disturbed Ratios between Essential and Toxic Trace Elements as Potential Biomarkers of Acute Ischemic Stroke. Nutrients. 2023; 15(6):1434. https://doi.org/10.3390/nu15061434
Chicago/Turabian StyleMirończuk, Anna, Katarzyna Kapica-Topczewska, Katarzyna Socha, Jolanta Soroczyńska, Jacek Jamiołkowski, Monika Chorąży, Agata Czarnowska, Agnieszka Mitrosz, Alina Kułakowska, and Jan Kochanowicz. 2023. "Disturbed Ratios between Essential and Toxic Trace Elements as Potential Biomarkers of Acute Ischemic Stroke" Nutrients 15, no. 6: 1434. https://doi.org/10.3390/nu15061434