
Selenium in Infants and Preschool Children Nutrition: A Literature Review

Abstract
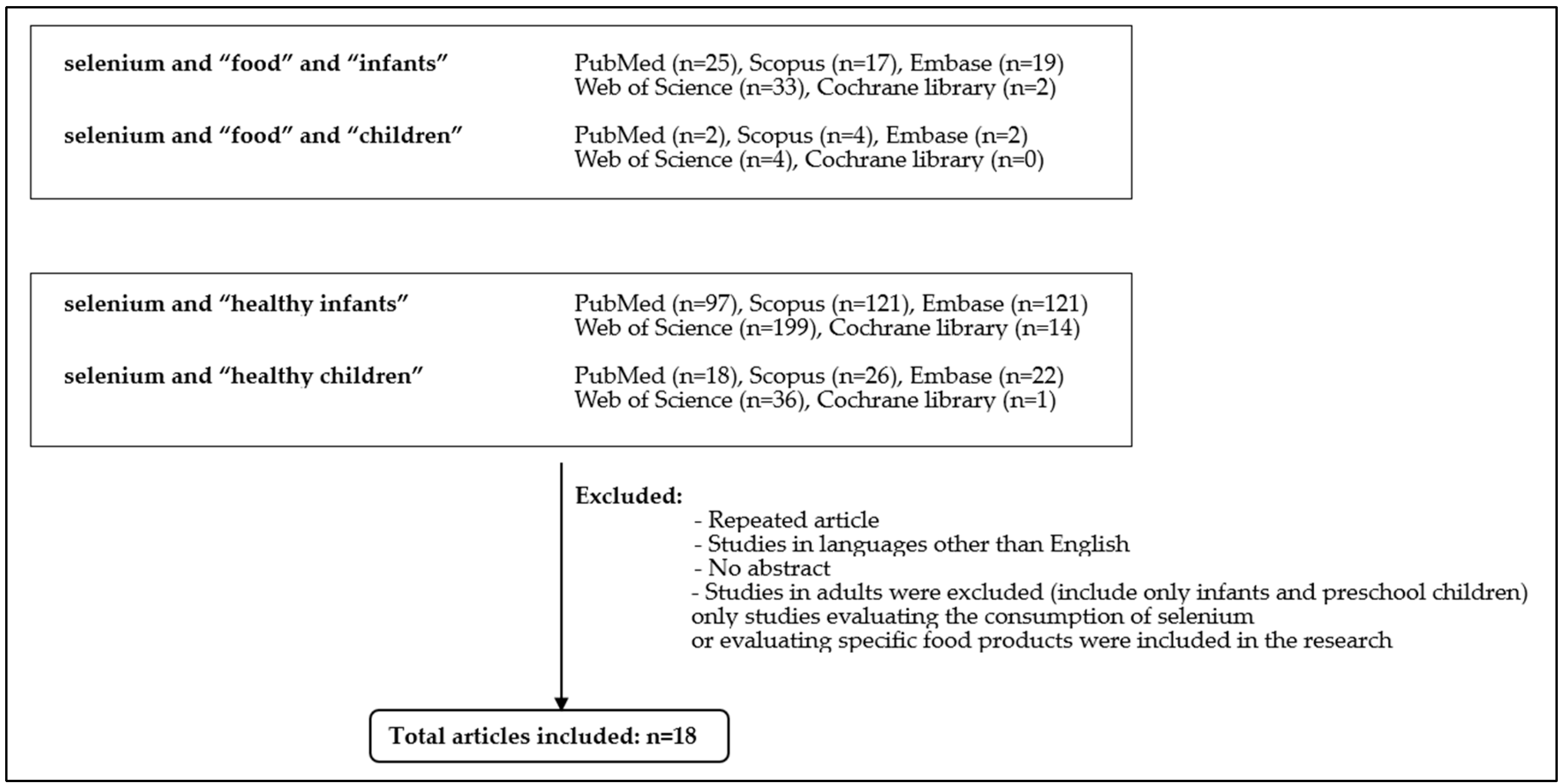
:1. Introduction
Methodology
2. Selenium in the Human Body
2.1. Main Function of Selenium in the Human Body
2.2. Symptoms of Selenium Deficiency and Excess
2.3. Selenium Dietary Requirement in Infants and Preschool Children
3. Main Dietary Selenium Sources in Infants and Preschool Children
3.1. Selenium in Dietary Products
3.2. Breast Milk and Infant Formula

{kind=link}
| Food Source | Average Content | Comments |
|---|---|---|
| Breast milk | 2.2–3.0 μg/100 kcal * | Se content depends on the maternal diet |
| Infant formula | 3.0–8.6 μg/100 kcal | According to the Delegated Regulation (EU) |
| 2.0–7.0 μg/100 kcal | According to the FDA |
3.3. Main Dietary Selenium Sources after Weaning in Children
3.3.1. Fish Products
3.3.2. Meat, Eggs and Milk Products
3.3.3. Frutis and Vegetables
3.3.4. Brazil Nut
3.3.5. Cereals and Yeast
4. Bioavailability of Selenium
5. Selenium Intake in Elimination Diets
6. Selenium Dietary Intake in Infant and Preschool Children—Overview of Available Studies
7. Serum Selenium Concentration in Infant and Preschool Children—Overview of Available Studies
| Study | Country | Patients | Observations |
|---|---|---|---|
| Zyambo et al., 2022 [170] | Zambia | 269 children: with severe acute malnutrition (n = 19), with stunting (n = 164), and children without stunting (n = 86), received Se supplementation Age: 15 (4–23) months Sex: both | The median Se levels were 32.37 μg/L (21.32–62.38) among unstunted children, 45.01 μg/L (41.85–64.74) among stunted children, and 71.85 μg/L (47.37–89.22) among severely malnourished children Se deficiency is widespread in Lusaka province and could in part be related to socio-economic status, therefore supplementation or agronomic biofortification is needed |
| Martens et al., 2015 [18] | Brazil | 129 children: 41 receiving 15–30 g of brazil nuts 3d/w and 88 that did not receive nuts age: 4.7 ± 0.9 (3.1–6.3) years old in the study group; 4.5 ± 1.2 (2.1–6.6) in control sex: both | Plasma Se concentration in supplemented children: 107.29 ± 27.15 (73–172) μg/L Plasma Se concentration in controls: 83.56 ± 23.32 (47–142) μg/L Plasma Se levels of supplemented children were significantly higher than in the control group but the Se concentration was higher than the accepted cutoff (>84–100 μg/L) for both groups Se supplementation of Brazilian children is not necessary and could even lead to Se poisoning |
| Darlow et al., 1995 [49] | New Zealand | 15 children age: 0–5 days sex: both | Plasma Se concentration: 39.69 ± 3.16 μg/L After 1 month of feeding with standard formula: 21.32 ± 0.79 μg/L After 3 months of feeding with standard formula: 31.58 ± 3.16 μg/L There was a significant drop in plasma Se levels between birth and the first month of life but compared to a group of infants supplemented with Se 17 μg/L to resemble breast milk composition, there were no differences in growth parameters or thyroid function |
| Perez-Plazola et al., 2023 [169] | Malawi | 387 children age: 7 (1.2) months sex: both | Plasma Se at baseline was 47.41 (28.48) μg/L and 50.59 (28.58) μg/L The children had inadequate plasma Se concentrations given the minimal cutoff of 70 μg/L for optimal body functioning The provision of one additional egg per day for 6 months did not increase plasma Se levels, which is thought to happen because of high rates of stunting and underweight status in those children |
| Flax et al., 2014 [168] | Malawi | 526 children of HIV-infected mothers age: 2–6 weeks old sex: both | Plasma Se: 55.6 ± 16.3 μg/L at 2–6 weeks and 61.0 ± 15.4 μg/L at 24 weeks The children did not have adequate plasma Se levels at any time The Se concentrations correlated with baseline tertile, being the lowest (40.1 ± 9.3) for low tertile, medium (57.0 ± 3.9) for middle tertile, and the highest (73.9 ± 7.5) for high tertile Maternal plasma Se levels and breast milk Se concentrations correlated with infant plasma Se |
| Olmez et al., 2004 [176] | Turkey | 131 children: 88 with acute gastroenteritis, 43 healthy age: 2–24 months sex: both | Control group: 74.36 ± 10.65 μg/L Study group: 62.41 ± 13.06 μg/L on admission and 81.73 ± 17.10 μg/L 7–10 days after the end of symptoms Children suffering from gastroenteritis had significantly lower plasma Se levels on admission than healthy children but higher after the end of symptoms Se levels did not correlate with the severity of the symptoms |
| Gibson et al., 2011 [177] | Zambia | 476 children age: 6 months sex: both | Baseline serum Se concentrations: 48.95 (47.37, 50.53) μg/L, and 49.75 (47.37, 52.11) μg/L Plasma Se levels were defined as below adequate for maximal activity of plasma GPx and selenoprotein P (~78.96–94.75 μg/L) Children with higher baseline plasma Se showed a better response to Se fortification, probably because of the decreased expression of selenoproteins in children with low Baseline plasma Se |
| Daniles et al., 1996 [174] | Australia | 38 preterm infants fed parenterally with or without Se supplementation age: <7 days sex: both | Baseline plasma Se: 28(3) μg/L and 27(3) μg/L Baseline plasma Se levels were inadequate Se supplementation with 3 µg/kg/day prevented health deterioration but did not achieve levels similar to breastfed infants |
| Christodoulides et al., 2011 [178] | United Kingdom | 44 children with intractable epilepsy divided into 2 age groups (2–3 and 4–6) age: 2–6 years sex: both | Baseline mean plasma Se levels: 2–3-year-old group 75.80 (15.00) μg/L 4–6-year-old group 77.38 (20.53) μg/L (further divided into male and female groups with concentrations of 64.74 (45.80–89.22) μg/L and 63.96 (45.01–82.90) μg/L, respectively) Plasma Se levels were within the range of GOSH reference (39.48–102.65 μg/L for 2–4-year-olds and 55.28–134.23 μg/L for 4–17-year-olds) The children were either on a classical ketogenic diet or MCT ketogenic (the main fat source is MCT fatty acids) and there were no significant differences in plasma Se levels between these two groups |
| Bogye et al., 1998 [171] | Hungary | 36 preterm infants (mean gestational age 27 weeks) age: one day sex: both | Baseline serum concentration in the control group: 34.4 (20.4) μg/L Serum concentration after 14 days: 26.1 (16.6) μg/L Baseline serum concentration in the study group: 36.1 (12.8) μg/L Serum concentration after 14 days of supplementation (4.8 mg yeast–Se containing 5 μg Se daily with nasogastric drip): 43.5 (7.9) μg/L Se concentration in the control group decreased during the first 14 days of life and increased significantly in the supplemented study group There were no side effects and the intervention was considered safe |
| Linday et al., 2002 [179] | USA | 39 children undergoing placement of tympanostomy tube for frequent ear infections and/or persistent middle ear effusion | Serum Se concentration: 110.54 ± 16.58 μg/L There was no difference in plasma Se concentrations from published values Cod liver oil and multivitamins containing Se were proposed as antioxidants to prevent free radical-induced lipid peroxidation that could lead to otitis media The intervention improved the time of antibiotic therapy and symptom re-occurrence |
| Strauss et al., 2010 [175] | USA | 15 children with maple syrup urine disease age: 0–36 months sex: both | Baseline Se concentration: 56.7 (10.9) μg/L Baseline plasma Se in studied children was inadequate Supplementation of 4–9 μg/kg/day raised plasma Se levels, but they remained lower than in the healthy population (83.4 (11.0) μg/L vs. 110–160 μg/L normal) |
| Li et al., 1999 [172] | Austria, Slovenia | 25 neonates—5 Austrian, 20 Slovenian age: 0 (umbilical cord blood at the time of delivery) sex: both | Austrian neonates: 42 ± 6 μg/L Slovenian neonates: 34 ± 7 μg/L All infants had plasma Se levels lower than their mothers, which is consistent with previous findings |
| Age | Serum Se Concentrations (µg/L) |
|---|---|
| <1 month | 15–107 |
| 1–2 months | 15–100 |
| 2–4 months | 10–93 |
| 4–12 months | 13–116 |
| 1–5 years | 34–129 |
8. Concluding Remarks—Nutritional Recommendation for Infants and Preschool Children Regarding Selenium Intake
9. Summary
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Muntau, A.C.; Streiter, M.; Kappler, M.; Röschinger, W.; Schmid, I.; Rehnert, A.; Schramel, P.; Roscher, A.A. Age-Related Reference Values for Serum Selenium Concentrations in Infants and Children. Clin. Chem. 2002, 48, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Fordyce, F.M. Selenium Deficiency and Toxicity in the Environment. In Essentials of Medical Geology; Revised Edition; Selinus, O., Ed.; Springer: Dordrecht, The Netherlands, 2013; pp. 375–416. [Google Scholar]
- Belay, A.; Joy, E.J.M.; Chagumaira, C.; Zerfu, D.; Ander, E.L.; Young, S.D.; Bailey, E.H.; Lark, R.M.; Broadley, M.R.; Gashu, D. Selenium Deficiency Is Widespread and Spatially Dependent in Ethiopia. Nutrients 2020, 12, 1565. [Google Scholar] [CrossRef] [PubMed]
- Bogye, G.; Fehér, J.; Georg, A.; Antti, A. Complex study of selenium levels in healthy subjects in Hungary. Orv. Hetil. 1993, 134, 2585–2588. [Google Scholar]
- Ning, Y.; Hu, M.; Chen, S.; Zhang, F.; Yang, X.; Zhang, Q.; Gong, Y.; Huang, R.; Liu, Y.; Chen, F.; et al. Investigation of Selenium Nutritional Status and Dietary Pattern among Children in Kashin-Beck Disease Endemic Areas in Shaanxi Province, China Using Duplicate Portion Sampling Method. Environ. Int. 2022, 164, 107255. [Google Scholar] [CrossRef]
- Chen, Z.; Li, H.; Yang, L.; Wang, W.; Li, Y.; Gong, H.; Guo, M.; Nima, C.; Zhao, S.; Wang, J.; et al. Hair Selenium Levels of School Children in Kashin–Beck Disease Endemic Areas in Tibet, China. Biol. Trace Elem. Res. 2015, 168, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Joy, E.J.M.; Ander, E.L.; Young, S.D.; Black, C.R.; Watts, M.J.; Chilimba, A.D.C.; Chilima, B.; Siyame, E.W.P.; Kalimbira, A.A.; Hurst, R.; et al. Dietary Mineral Supplies in Africa. Physiol. Plant. 2014, 151, 208–229. [Google Scholar] [CrossRef]
- Phiri, F.P.; Ander, E.L.; Bailey, E.H.; Chilima, B.; Chilimba, A.D.C.; Gondwe, J.; Joy, E.J.M.; Kalimbira, A.A.; Kumssa, D.B.; Lark, R.M.; et al. The Risk of Selenium Deficiency in Malawi Is Large and Varies over Multiple Spatial Scales. Sci. Rep. 2019, 9, 6566. [Google Scholar] [CrossRef]
- Sempértegui; Estrella; Vallejo; Tapia; Herrera; Moscoso; Cerón; Griffiths; Hamer. Selenium Serum Concentrations in Malnourished Ecuadorian Children: A Case-Control Study. Int. J. Vitam. Nutr. Res. 2003, 73, 181–186. [Google Scholar] [CrossRef]
- Berger, M.M. Trace element issues in Switzerland and Europe. Rev. Med. Suisse 2012, 8, 2078–2082, 2084. [Google Scholar]
- Jablonska, E.; Gromadzinska, J.; Klos, A.; Bertrandt, J.; Skibniewska, K.; Darago, A.; Wasowicz, W. Selenium, Zinc and Copper in the Polish Diet. J. Food Compos. Anal. 2013, 31, 259–265. [Google Scholar] [CrossRef]
- Aro, A.; Kumpulainen, J.; Alfthan, G.; Voshchenko, A.V.; Ivanov, V.N. Factors Affecting the Selenium Intake of People in Transbaikalian Russia. Biol. Trace Elem. Res. 1994, 40, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Kawai, M. For Debate: When is Selenium Deficiency Suspected and When is Its Measurement Indicated? Pediatr. Endocrinol. Rev. 2019, 16, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Shreenath, A.P.; Ameer, M.A.; Dooley, J. Selenium Deficiency. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Peroni, D.G.; Bonomo, B.; Casarotto, S.; Boner, A.L.; Piacentini, G.L. How Changes in Nutrition Have Influenced the Development of Allergic Diseases in Childhood. Ital. J. Pediatr. 2012, 38, 22. [Google Scholar] [CrossRef] [PubMed]
- Vega, C.M.; Godoy, J.M.; Barrocas, P.R.G.; Gonçalves, R.A.; De Oliveira, B.F.A.; Jacobson, L.V.; Mourão, D.S.; Hacon, S.S. Selenium Levels in the Whole Blood of Children and Teenagers from Two Riparian Communities at the Madeira River Basin in the Western Brazilian Amazon. Biol. Trace Elem. Res. 2017, 175, 87–97. [Google Scholar] [CrossRef] [PubMed]
- Leroux, I.N.; Ferreira, A.P.S.D.S.; Paniz, F.P.; Silva, F.F.D.; Luz, M.S.; Batista, B.L.; Marchioni, D.M.; Olympio, K.P.K. Brazilian Preschool Children Attending Day Care Centers Show an Inadequate Micronutrient Intake through 24-h Duplicate Diet. J. Trace Elem. Med. Biol. 2019, 54, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Martens, I.B.G.; Cardoso, B.R.; Hare, D.J.; Niedzwiecki, M.M.; Lajolo, F.M.; Martens, A.; Cozzolino, S.M.F. Selenium Status in Preschool Children Receiving a Brazil Nut–Enriched Diet. Nutrition 2015, 31, 1339–1343. [Google Scholar] [CrossRef]
- EFSA Panel on Nutrition, Novel Foods and Food Allergens (NDA); Turck, D.; Bohn, T.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; et al. Scientific Opinion on the Tolerable Upper Intake Level for Selenium. EFSA J. 2023, 21, e07704. [Google Scholar] [CrossRef]
- Minich, W.B. Selenium Metabolism and Biosynthesis of Selenoproteins in the Human Body. Biochem. Mosc. 2022, 87, S168–S177. [Google Scholar] [CrossRef]
- Mehdi, Y.; Hornick, J.-L.; Istasse, L.; Dufrasne, I. Selenium in the Environment, Metabolism and Involvement in Body Functions. Molecules 2013, 18, 3292–3311. [Google Scholar] [CrossRef]
- Fairweather-Tait, S.J.; Bao, Y.; Broadley, M.R.; Collings, R.; Ford, D.; Hesketh, J.E.; Hurst, R. Selenium in Human Health and Disease. Antioxid. Redox Signal. 2011, 14, 1337–1383. [Google Scholar] [CrossRef]
- Tinggi, U. Selenium: Its Role as Antioxidant in Human Health. Environ. Health Prev. Med. 2008, 13, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Yamanoshita, O.; Ichihara, S.; Hama, H.; Ichihara, G.; Chiba, M.; Kamijima, M.; Takeda, I.; Nakajima, T. Chemopreventive Effect of Selenium-Enriched Japanese Radish Sprout against Breast Cancer Induced by 7,12-Dimethylbenz[a]Anthracene in Rats. Tohoku J. Exp. Med. 2007, 212, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Kuršvietienė, L.; Mongirdienė, A.; Bernatonienė, J.; Šulinskienė, J.; Stanevičienė, I. Selenium Anticancer Properties and Impact on Cellular Redox Status. Antioxidants 2020, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Broughton Pipkin, F.; Redman, C.W.G.; Poston, L. Selenium in Reproductive Health. Am. J. Obstet. Gynecol. 2012, 206, 21–30. [Google Scholar] [CrossRef]
- Rahman, M.M.; Asiri, A.M.; Khan, A.; Inamuddin. Importance of Selenium in the Environment and Human Health; IntechOpen: Rijeka, Croatia, 2020; ISBN 978-1-78985-868-6. [Google Scholar]
- Schwarz, K.; Foltz, C.M. Selenium as an Integral Part of Factor 3 against Dietary Necrotic Liver Degeneration. Nutrition 1957, 15, 255. [Google Scholar]
- Fordyce, F.M. Selenium Deficiency and Toxicity in the Environment. In Essentials of Medical Geology; Elsevier: London, UK, 2005. [Google Scholar]
- Ge, K.; Xue, A.; Bai, J.; Wang, S. Keshan Disease-an Endemic Cardiomyopathy in China. Vichows Archiv A Pathol. Anat. 1983, 401, 1–15. [Google Scholar] [CrossRef]
- Rayman, M.P. The Importance of Selenium to Human Health. Lancet 2000, 356, 233–241. [Google Scholar] [CrossRef]
- Institute of Medicine, Food and Nutrition Board. Dietary Reference Intakes: Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academy Press: Washington, DC, USA, 2000. [Google Scholar]
- Schepman, K.; Engelbert, R.H.H.; Visser, M.M.; Yu, C.; De Vos, R. Kashin Beck Disease: More than Just Osteoarthrosis: A Cross-Sectional Study Regarding the Influence of Body Function-Structures and Activities on Level of Participation. Int. Orthop. 2011, 35, 767–776. [Google Scholar] [CrossRef]
- Cao, J.; Li, S.; Shi, Z.; Yue, Y.; Sun, J.; Chen, J.; Fu, Q.; Hughes, C.E.; Caterson, B. Articular Cartilage Metabolism in Patients with Kashin–Beck Disease: An Endemic Osteoarthropathy in China. Osteoarthr. Cartil. 2008, 16, 680–688. [Google Scholar] [CrossRef]
- Yao, Y.; Pei, F.; Kang, P. Selenium, Iodine, and the Relation with Kashin-Beck Disease. Nutrition 2011, 27, 1095–1100. [Google Scholar] [CrossRef]
- Toulis, K.A.; Anastasilakis, A.D.; Tzellos, T.G.; Goulis, D.G.; Kouvelas, D. Selenium Supplementation in the Treatment of Hashimoto’s Thyroiditis: A Systematic Review and a Meta-Analysis. Thyroid 2010, 20, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Bartalena, L.; Kahaly, G.J.; Baldeschi, L.; Dayan, C.M.; Eckstein, A.; Marcocci, C.; Marinò, M.; Vaidya, B.; Wiersinga, W.M.; EUGOGO. The 2021 European Group on Graves’ Orbitopathy (EUGOGO) Clinical Practice Guidelines for the Medical Management of Graves’ Orbitopathy. Eur. J. Endocrinol. 2021, 185, G43–G67. [Google Scholar] [CrossRef] [PubMed]
- Pelewicz, K.; Miśkiewicz, P. Iodinated Contrast Media-Induced Hyperthyroidism. J. Med. Sci. 2020, 89, e439. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Kitts, D.; Giovannucci, E.L.; Sahye-Pudaruth, S.; Paquette, M.; Blanco Mejia, S.; Patel, D.; Kavanagh, M.; Tsirakis, T.; Kendall, C.W.; et al. Selenium, Antioxidants, Cardiovascular Disease, and All-Cause Mortality: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Am. J. Clin. Nutr. 2020, 112, 1642–1652. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.; Arthur, J. Selenium, Selenoproteins and Human Health: A Review. Public. Health Nutr. 2001, 4, 593–599. [Google Scholar] [CrossRef]
- Pieczyńska, J.; Grajeta, H. The Role of Selenium in Human Conception and Pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 31–38. [Google Scholar] [CrossRef]
- Lima, L.G.; Santos, A.A.M.D.; Gueiber, T.D.; Gomes, R.Z.; Martins, C.M.; Chaikoski, A.C. Relation between Selenium and Female Fertility: A Systematic Review. Rev. Bras. Ginecol. Obstet. 2022, 44, 701–709. [Google Scholar] [CrossRef]
- Vinton, N.E.; Dahlstrom, K.A.; Strobel, C.T.; Ament, M.E. Macrocytosis and Pseudoalbinism: Manifestations of Selenium Deficiency. J. Pediatr. 1987, 111, 711–717. [Google Scholar] [CrossRef]
- Masumoto, K.; Nagata, K.; Higashi, M.; Nakatsuji, T.; Uesugi, T.; Takahashi, Y.; Nishimoto, Y.; Kitajima, J.; Hikino, S.; Hara, T.; et al. Clinical Features of Selenium Deficiency in Infants Receiving Long-Term Nutritional Support. Nutrition 2007, 23, 782–787. [Google Scholar] [CrossRef]
- Uchoa, K.M.C.B.; Evangelista, N.M.D.A.; Carvalho De Camargo, M.F.; Leite, H.P. Severe Hypothyroidism in a Child Receiving Long-Term Home Parenteral Nutrition Without Selenium. J. Parenter. Enter. Nutr. 2020, 44, 944–947. [Google Scholar] [CrossRef]
- Chanoine, J.-P. Selenium and Thyroid Function in Infants, Children and Adolescents. BioFactors 2003, 19, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Gashu, D.; Stoecker, B.J.; Bougma, K.; Adish, A.; Haki, G.D.; Marquis, G.S. Stunting, Selenium Deficiency and Anemia Are Associated with Poor Cognitive Performance in Preschool Children from Rural Ethiopia. Nutr. J. 2015, 15, 38. [Google Scholar] [CrossRef] [PubMed]
- Wasantwisut, E. Nutrition and Development: Other Micronutrients’ Effect on Growth and Cognition. Southeast Asian J. Trop. Med. Public Health 1997, 28 (Suppl. S2), 78–82. [Google Scholar] [PubMed]
- Darlow, B.A.; Austin, N. Selenium Supplementation to Prevent Short-Term Morbidity in Preterm Neonates. Cochrane Database Syst. Rev. 2003, 4, CD003312. [Google Scholar] [CrossRef] [PubMed]
- Tindell, R.; Tipple, T. Selenium: Implications for Outcomes in Extremely Preterm Infants. J. Perinatol. 2018, 38, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Filipowicz, D.; Szczepanek-Parulska, E.; Kłobus, M.; Szymanowski, K.; Chillon, T.S.; Asaad, S.; Sun, Q.; Mikulska-Sauermann, A.A.; Karaźniewicz-Łada, M.; Główka, F.K.; et al. Selenium Status and Supplementation Effects in Pregnancy—A Study on Mother–Child Pairs from a Single-Center Cohort. Nutrients 2022, 14, 3082. [Google Scholar] [CrossRef]
- Mistry, H.D.; Kurlak, L.O.; Young, S.D.; Briley, A.L.; Broughton Pipkin, F.; Baker, P.N.; Poston, L. Maternal Selenium, Copper and Zinc Concentrations in Pregnancy Associated with Small-for-Gestational-Age Infants: Micronutrient Concentrations, SGA and Adolescence. Matern. Child Nutr. 2014, 10, 327–334. [Google Scholar] [CrossRef]
- Xu, M.; Guo, D.; Gu, H.; Zhang, L.; Lv, S. Selenium and Preeclampsia: A Systematic Review and Meta-Analysis. Biol. Trace Elem. Res. 2016, 171, 283–292. [Google Scholar] [CrossRef]
- Lombeck, I.; Jochum, F.; Terwolbeck, K. Selenium Status in Infants and Children with Phenylketonuria and in Maternal Phenylketonuria. Eur. J. Pediatr. 1996, 155, S140–S144. [Google Scholar] [CrossRef]
- Michalke, B. Selenium Speciation in Human Serum of Cystic Fibrosis Patients Compared to Serum from Healthy Persons. J. Chromatogr. A 2004, 1058, 203–208. [Google Scholar] [CrossRef]
- Cantin, A.M.; White, T.B.; Cross, C.E.; Forman, H.J.; Sokol, R.J.; Borowitz, D. Antioxidants in Cystic fibrosis☆Conclusions from the CF Antioxidant Workshop, Bethesda, Maryland, November 11–12, 2003. Free Radic. Biol. Med. 2007, 42, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Luciak, M. Antioxidants in the Treatment of Patients with Renal Failure. Rocz. Akad. Med. Bialymst. 2004, 49, 157–161. [Google Scholar] [PubMed]
- Sahebari, M.; Rezaieyazdi, Z.; Khodashahi, M. Selenium and Autoimmune Diseases: A Review Article. Curr. Rheumatol. Rev. 2019, 15, 123–134. [Google Scholar] [CrossRef] [PubMed]
- Kieliszek, M.; Błażejak, S. Current Knowledge on the Importance of Selenium in Food for Living Organisms: A Review. Molecules 2016, 21, 609. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Fordyce, F.M.; Rayman, M.P. Symposium on ‘Geographical and Geological Influences on Nutrition’ Factors Controlling the Distribution of Selenium in the Environment and Their Impact on Health and Nutrition: Conference on ‘Over- and Undernutrition: Challenges and Approaches’. Proc. Nutr. Soc. 2010, 69, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.I.; Westfall, B.B. Further Field Studies on the Selenium Problem in Relation to Public Health. Public Health Rep. 1937, 52, 1375. [Google Scholar] [CrossRef]
- World Health Organization. Environmental Health Criterion 58—Selenium; World Health Organization: Geneva, Switzerland, 1987. [Google Scholar]
- Yang, G.; Wang, S.; Zhou, R.; Sun, S. Endemic Selenium Intoxication of Humans in China. Am. J. Clin. Nutr. 1983, 37, 872–881. [Google Scholar] [CrossRef]
- Bleys, J.; Navas-Acien, A.; Guallar, E. Selenium and Diabetes: More Bad News for Supplements. Ann. Intern. Med. 2007, 147, 271. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Selenium. EFSA J. 2014, 12, 3846. [Google Scholar] [CrossRef]
- Levander, O.A. Selenium Requirements as Discussed in the 1996 Joint FAO/IAEA/WHO Expert Consultation on Trace Elements in Human Nutrition. Biomed. Environ. Sci. 1997, 10, 214–219. [Google Scholar]
- Weekley, C.M.; Harris, H.H. Which Form Is That? The Importance of Selenium Speciation and Metabolism in the Prevention and Treatment of Disease. Chem. Soc. Rev. 2013, 42, 8870. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Dharmaraj, S. Selenium and Selenoproteins: It’s Role in Regulation of Inflammation. Inflammopharmacology 2020, 28, 667–695. [Google Scholar] [CrossRef] [PubMed]
- Dobrzyńska, M.; Drzymała-Czyż, S.; Woźniak, D.; Drzymała, S.; Przysławski, J. Natural Sources of Selenium as Functional Food Products for Chemoprevention. Foods 2023, 12, 1247. [Google Scholar] [CrossRef] [PubMed]
- Tóth, R.J.; Csapó, J. The Role of Selenium in Nutrition—A Review. Acta Univ. Sapientiae Aliment. 2018, 11, 128–144. [Google Scholar] [CrossRef]
- Ip, C.; Lisk, D.J.; Stoewsand, G.S. Mammary Cancer Prevention by Regular Garlic and Selenium-enriched Garlic. Nutr. Cancer 1992, 17, 279–286. [Google Scholar] [CrossRef]
- Davis, C.D.; Zeng, H.; Finley, J.W. Selenium-Enriched Broccoli Decreases Intestinal Tumorigenesis in Multiple Intestinal Neoplasia Mice. J. Nutr. 2002, 132, 307–309. [Google Scholar] [CrossRef]
- Hu, Y.; McIntosh, G.H.; Young, G.P. Selenium-Rich Foods: A Promising Approach to Colorectal Cancer Prevention. Curr. Pharm. Biotechnol. 2012, 13, 165–172. [Google Scholar] [CrossRef]
- Kotrebai, M.; Tyson, J.F.; Uden, P.C.; Birringer, M.; Block, E. Selenium Speciation in Enriched and Natural Samples by HPLC-ICP-MS and HPLC-ESI-MS with Perfluorinated Carboxylic Acid Ion-Pairing Agents. Analyst 2000, 125, 71–78. [Google Scholar] [CrossRef]
- Rayman, M.P. Food-Chain Selenium and Human Health: Emphasis on Intake. Br. J. Nutr. 2008, 100, 254–268. [Google Scholar] [CrossRef]
- Sharma, V.K.; Sohn, M.; McDonald, T.J. Remediation of Selenium in Water: A Review. In Advances in Water Purification Techniques; Elsevier: Amsterdam, The Netherlands, 2019; pp. 203–218. ISBN 978-0-12-814790-0. [Google Scholar]
- Sager, M. Selenium in Agriculture, Food, and Nutrition. Pure Appl. Chem. 2006, 78, 111–133. [Google Scholar] [CrossRef]
- Lönnerdal, B.; Vargas-Fernández, E.; Whitacre, M. Selenium Fortification of Infant Formulas: Does Selenium Form Matter? Food Funct. 2017, 8, 3856–3868. [Google Scholar] [CrossRef] [PubMed]
- Dorea, J.G. Selenium and Breast-Feeding. Br. J. Nutr. 2002, 88, 443–461. [Google Scholar] [CrossRef] [PubMed]
- Zachara, B.A.; Pilecki, A. Selenium Concentration in the Milk of Breast-Feeding Mothers and Its Geographic Distribution. Environ. Health Perspect. 2000, 108, 1043–1046. [Google Scholar] [CrossRef] [PubMed]
- Valent, F.; Horvat, M.; Mazej, D.; Stibilj, V.; Barbone, F. Maternal Diet and Selenium Concentration in Human Milk From an Italian Population. J. Epidemiol. 2011, 21, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Miklavčič, A.; Casetta, A.; Snoj Tratnik, J.; Mazej, D.; Krsnik, M.; Mariuz, M.; Sofianou, K.; Špirić, Z.; Barbone, F.; Horvat, M. Mercury, Arsenic and Selenium Exposure Levels in Relation to Fish Consumption in the Mediterranean Area. Environ. Res. 2013, 120, 7–17. [Google Scholar] [CrossRef]
- Krachler, M.; Prohaska, T.; Koellensperger, G.; Rossipal, E.; Stingeder, G. Concentrations of Selected Trace Elements in Human Milk and in Infant Formulas Determined by Magnetic Sector Field Inductively Coupled Plasma-Mass Spectrometry. Biol. Trace Elem. Res. 2000, 76, 97–112. [Google Scholar] [CrossRef]
- (EU) 2016/127; Commission Delegated Regulation (EU) 2016/127 of 25 September 2015 Supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as Regards the Specific Compositional and Information Requirements for Infant Formula and Follow-on Formula and as Regards Requirements on Information Relating to Infant and Young Child Feeding. European Union: Brussels, Belgium, 2015.
- (EU) 2016/128; Commission Delegated Regulation (EU) 2016/128 of 25 September 2015 Supplementing Regulation (EU) No 609/2013 of the European Parliament and of the Council as Regards the Specific Compositional and Information Requirements for Food for Special Medical Purposes. European Union: Brussels, Belgium, 2015.
- Food and Drug Administration, HHS. Infant Formula: The Addition of Minimum and Maximum Levels of Selenium to Infant Formula and Related Labeling Requirements. Final Rule. Fed. Regist. 2015, 80, 35834–35841. [Google Scholar]
- He, M.-J.; Zhang, S.-Q.; Mu, W.; Huang, Z.-W. Selenium in Infant Formula Milk. Asia Pac. J. Clin. Nutr. 2018, 27, 284–292. [Google Scholar] [CrossRef]
- (EU) No 609/2013; Regulation (EU) No 609/2013 of the European Parliament and of the Council of 12 June 2013 on Food Intended for Infants and Young Children, Food for Special Medical Purposes, and Total Diet Replacement for Weight Control and Repealing Council Directive 92/52/EEC, Commission Directives 96/8/EC, 1999/21/EC, 2006/125/EC and 2006/141/EC, Directive 2009/39/EC of the European Parliament and of the Council and Commission Regulations (EC) No 41/2009 and (EC) No 953/2009 Text with EEA Relevance. European Union: Brussels, Belgium, 2015.
- Lin, Y.-H.; Hsu, Y.-C.; Lin, M.-C.; Chen, C.-H.; Wang, T.-M. The Association of Macronutrients in Human Milk with the Growth of Preterm Infants. PLoS ONE 2020, 15, e0230800. [Google Scholar] [CrossRef]
- Litov, R.E.; Combs, G.F. Selenium in Pediatric Nutrition. Pediatrics 1991, 87, 339–351. [Google Scholar] [CrossRef]
- Pilarczyk, B.; Tomza-Marciniak, A.; Pilarczyk, R.; Kuba, J.; Hendzel, D.; Udała, J.; Tarasewicz, Z. Eggs as a Source of Selenium in the Human Diet. J. Food Compos. Anal. 2019, 78, 19–23. [Google Scholar] [CrossRef]
- Xie, M.; Sun, X.; Li, P.; Shen, X.; Fang, Y. Selenium in Cereals: Insight into Species of the Element from Total Amount. Comp. Rev. Food Sci. Food Safe 2021, 20, 2914–2940. [Google Scholar] [CrossRef] [PubMed]
- De Temmerman, L.; Waegeneers, N.; Thiry, C.; Du Laing, G.; Tack, F.; Ruttens, A. Selenium Content of Belgian Cultivated Soils and Its Uptake by Field Crops and Vegetables. Sci. Total Environ. 2014, 468–469, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Pappa, E.C.; Pappas, A.C.; Surai, P.F. Selenium Content in Selected Foods from the Greek Market and Estimation of the Daily Intake. Sci. Total Environ. 2006, 372, 100–108. [Google Scholar] [CrossRef]
- Singhato, A.; Judprasong, K.; Sridonpai, P.; Laitip, N.; Ornthai, N.; Yafa, C.; Chimkerd, C. Effect of Different Cooking Methods on Selenium Content of Fish Commonly Consumed in Thailand. Foods 2022, 11, 1808. [Google Scholar] [CrossRef]
- Navarro-Alarcon, M.; Cabrera-Vique, C. Selenium in Food and the Human Body: A Review. Sci. Total Environ. 2008, 400, 115–141. [Google Scholar] [CrossRef]
- Cappon, C.J.; Smith, J.C. Mercury and Selenium Content and Chemical Form in Fish Muscle. Arch. Environ. Contam. Toxicol. 1981, 10, 305–319. [Google Scholar] [CrossRef]
- Cabañero, A.I.; Carvalho, C.; Madrid, Y.; Batoréu, C.; Cámara, C. Quantification and Speciation of Mercury and Selenium in Fish Samples of High Consumption in Spain and Portugal. Biol. Trace Elem. Res. 2005, 103, 017–036. [Google Scholar] [CrossRef]
- Burger, J.; Gochfeld, M. Mercury and Selenium Levels in 19 Species of Saltwater Fish from New Jersey as a Function of Species, Size, and Season. Sci. Total Environ. 2011, 409, 1418–1429. [Google Scholar] [CrossRef]
- Yamashita, Y.; Yamashita, M.; Iida, H. Selenium Content in Seafood in Japan. Nutrients 2013, 5, 388–395. [Google Scholar] [CrossRef]
- Ganther, H.E.; Goudie, C.; Sunde, M.L.; Kopecky, M.J.; Wagner, P.; Oh, S.-H.; Hoekstra, W.G. Selenium: Relation to Decreased Toxicity of Methylmercury Added to Diets Containing Tuna. Science 1972, 175, 1122–1124. [Google Scholar] [CrossRef] [PubMed]
- Cuvin-Aralar, M.L.A.; Furness, R.W. Mercury and Selenium Interaction: A Review. Ecotoxicol. Environ. Saf. 1991, 21, 348–364. [Google Scholar] [CrossRef] [PubMed]
- Bratakos, M.S.; Zafiropoulos, T.F.; Siskos, P.A.; Ioannou, P.V. Selenium Losses on Cooking Greek Foods. Int. J. Food Sci. Technol. 2007, 23, 585–590. [Google Scholar] [CrossRef]
- Rosnes, J.T.; Skåra, T.; Skipnes, D. Recent Advances in Minimal Heat Processing of Fish: Effects on Microbiological Activity and Safety. Food Bioprocess. Technol. 2011, 4, 833–848. [Google Scholar] [CrossRef]
- Barone, G.; Storelli, A.; Meleleo, D.; Dambrosio, A.; Garofalo, R.; Busco, A.; Storelli, M.M. Levels of Mercury, Methylmercury and Selenium in Fish: Insights into Children Food Safety. Toxics 2021, 9, 39. [Google Scholar] [CrossRef] [PubMed]
- Szajewska, H.; Socha, P.; Horvath, A.; Rybak, A.; Zalewski, B.M.; Nehring-Gugulska, M.; Mojska, H.; Czerwionka-Szaflarska, M.; Gajewska, D.; Helwich, E.; et al. Zasady Żywienia Zdrowych Niemowląt. Stanowisko Polskiego Towarzystwa Gastroenterologii, Hepatologii i Żywienia Dzieci. Pediatria 2021, 11, 321–338. [Google Scholar]
- McNaughton, S.A.; Marks, G.C. Selenium Content of Australian Foods: A Review of Literature Values. J. Food Compos. Anal. 2002, 15, 169–182. [Google Scholar] [CrossRef]
- Díaz-Alarcón, J.P.; Navarro-Alarcón, M.; López-García De La Serrana, H.; López-Martínez, M.C. Determination of Selenium in Meat Products by Hydride Generation Atomic Absorption SpectrometrySelenium Levels in Meat, Organ Meats, and Sausages in Spain. J. Agric. Food Chem. 1996, 44, 1494–1497. [Google Scholar] [CrossRef]
- Klapec, T.; Mandić, M.L.; Grgić, J.; Primorac, L.; Perl, A.; Krstanović, V. Selenium in Selected Foods Grown or Purchased in Eastern Croatia. Food Chem. 2004, 85, 445–452. [Google Scholar] [CrossRef]
- Pan, C.; Zhao, Y.; Liao, S.F.; Chen, F.; Qin, S.; Wu, X.; Zhou, H.; Huang, K. Effect of Selenium-Enriched Probiotics on Laying Performance, Egg Quality, Egg Selenium Content, and Egg Glutathione Peroxidase Activity. J. Agric. Food Chem. 2011, 59, 11424–11431. [Google Scholar] [CrossRef]
- Latshaw, J.D.; Osman, M. A Selenium and Vitamin E Responsive Condition in the Laying Hen. Poult. Sci. 1974, 53, 1704–1708. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S. Selenium Concentration in Egg and Body Tissue as Affected by the Level and Source of Selenium in the Hen Diet. Acta Agric. Scand. 1990, 40, 279–287. [Google Scholar] [CrossRef]
- Bennett, D.C.; Cheng, K.M. Selenium Enrichment of Table Eggs. Poult. Sci. 2010, 89, 2166–2172. [Google Scholar] [CrossRef] [PubMed]
- Yanardag, R.; Orak, H. Selenium Content of Milk and Milk Products of Turkey. II. Biol. Trace Elem. Res. 1999, 68, 79–95. [Google Scholar] [CrossRef] [PubMed]
- White, P.J. Selenium Accumulation by Plants. Ann. Bot. 2015, 117, 217–235. [Google Scholar] [CrossRef] [PubMed]
- Gui, J.; Rao, S.; Gou, Y.; Xu, F.; Cheng, S. Comparative Study of the Effects of Selenium Yeast and Sodium Selenite on Selenium Content and Nutrient Quality in Broccoli Florets (Brassica oleracea L. var. Italica). J. Sci. Food Agric. 2022, 102, 1707–1718. [Google Scholar] [CrossRef]
- Bansal, A.; Sharma, S.; Dhillon, S.K.; Dhillon, K.S. Selenium Accumulation and Biochemical Composition of Brassica Grains Grown in Selenate- or Selenite-Treated Alkaline Sandy Loam Soil. Commun. Soil. Sci. Plant Anal. 2012, 43, 1316–1331. [Google Scholar] [CrossRef]
- Ávila, F.W.; Faquin, V.; Yang, Y.; Ramos, S.J.; Guilherme, L.R.G.; Thannhauser, T.W.; Li, L. Assessment of the Anticancer Compounds Se -Methylselenocysteine and Glucosinolates in Se-Biofortified Broccoli (Brassica oleracea L. var. Italica) Sprouts and Florets. J. Agric. Food Chem. 2013, 61, 6216–6223. [Google Scholar] [CrossRef]
- Barak, P.; Goldman, I.L. Antagonistic Relationship between Selenate and Sulfate Uptake in Onion (Allium cepa): Implications for the Production of Organosulfur and Organoselenium Compounds in Plants. J. Agric. Food Chem. 1997, 45, 1290–1294. [Google Scholar] [CrossRef]
- Larsen, E.H.; Lobinski, R.; Burger-Meÿer, K.; Hansen, M.; Ruzik, R.; Mazurowska, L.; Rasmussen, P.H.; Sloth, J.J.; Scholten, O.; Kik, C. Uptake and Speciation of Selenium in Garlic Cultivated in Soil Amended with Symbiotic Fungi (Mycorrhiza) and Selenate. Anal. Bioanal. Chem. 2006, 385, 1098. [Google Scholar] [CrossRef]
- Singh, V.; Garg, A.N. Availability of Essential Trace Elements in Indian Cereals, Vegetables and Spices Using INAA and the Contribution of Spices to Daily Dietary Intake. Food Chem. 2006, 94, 81–89. [Google Scholar] [CrossRef]
- Pyrzynska, K. Selenium Speciation in Enriched Vegetables. Food Chem. 2009, 114, 1183–1191. [Google Scholar] [CrossRef]
- Wrobel, K.; Kannamkumarath, S.S.; Wrobel, K.; Caruso, J.A. Hydrolysis of Proteins with Methanesulfonic Acid for Improved HPLC-ICP-MS Determination of Seleno-Methionine in Yeast and Nuts. Anal. Bioanal. Chem. 2003, 375, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Tavares, L.; Santos, L.; Zapata Noreña, C.P. Bioactive Compounds of Garlic: A Comprehensive Review of Encapsulation Technologies, Characterization of the Encapsulated Garlic Compounds and Their Industrial Applicability. Trends Food Sci. Technol. 2021, 114, 232–244. [Google Scholar] [CrossRef]
- González, S.; Fernández-Navarro, T.; Arboleya, S.; de los Reyes-Gavilán, C.G.; Salazar, N.; Gueimonde, M. Fermented Dairy Foods: Impact on Intestinal Microbiota and Health-Linked Biomarkers. Front. Microbiol. 2019, 10, 1046. [Google Scholar] [CrossRef]
- Thomson, C.D. Brazil Nuts (Bertholletia Excelsa). In Nuts and Seeds in Health and Disease Prevention; Elsevier: Amsterdam, The Netherlands, 2011; pp. 245–252. ISBN 978-0-12-375688-6. [Google Scholar]
- Lima, L.W.; Stonehouse, G.C.; Walters, C.; Mehdawi, A.F.E.; Fakra, S.C.; Pilon-Smits, E.A.H. Selenium Accumulation, Speciation and Localization in Brazil Nuts (Bertholletia excelsa H.B.K.). Plants 2019, 8, 289. [Google Scholar] [CrossRef]
- Parekh, P.P.; Khan, A.R.; Torres, M.A.; Kitto, M.E. Concentrations of Selenium, Barium, and Radium in Brazil Nuts. J. Food Compos. Anal. 2008, 21, 332–335. [Google Scholar] [CrossRef]
- Chang, J.C.; Gutenmann, W.H.; Reid, C.M.; Lisk, D.J. Selenium Content of Brazil Nuts from Two Geographic Locations in Brazil. Chemosphere 1995, 30, 801–802. [Google Scholar] [CrossRef]
- Broadley, M.R.; White, P.J.; Bryson, R.J.; Meacham, M.C.; Bowen, H.C.; Johnson, S.E.; Hawkesford, M.J.; McGrath, S.P.; Zhao, F.-J.; Breward, N.; et al. Biofortification of UK Food Crops with Selenium. Proc. Nutr. Soc. 2006, 65, 169–181. [Google Scholar] [CrossRef]
- Silva Junior, E.C.; Wadt, L.H.O.; Silva, K.E.; Lima, R.M.B.; Batista, K.D.; Guedes, M.C.; Carvalho, G.S.; Carvalho, T.S.; Reis, A.R.; Lopes, G.; et al. Natural Variation of Selenium in Brazil Nuts and Soils from the Amazon Region. Chemosphere 2017, 188, 650–658. [Google Scholar] [CrossRef]
- Shahidi, F.; Tan, Z. Bioactives and Health Benefits of Brazil Nut. In Tree Nuts; Nutraceutical Science and Technology; Shahidi, F., Alasalvar, C., Eds.; CRC Press: Boca Raton, FL, USA, 2008; Volume 20084476, ISBN 978-0-8493-3735-2. [Google Scholar]
- Cardoso, B.R.; Duarte, G.B.S.; Reis, B.Z.; Cozzolino, S.M.F. Brazil Nuts: Nutritional Composition, Health Benefits and Safety Aspects. Food Res. Int. 2017, 100, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Al Osman, M.; Yang, F.; Massey, I.Y. Exposure Routes and Health Effects of Heavy Metals on Children. Biometals 2019, 32, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Kravchenko, J.; Darrah, T.H.; Miller, R.K.; Lyerly, H.K.; Vengosh, A. A Review of the Health Impacts of Barium from Natural and Anthropogenic Exposure. Environ. Geochem. Health 2014, 36, 797–814. [Google Scholar] [CrossRef] [PubMed]
- McNeill, I.R.; Isoardi, K.Z. Barium Poisoning: An Uncommon Cause of Severe Hypokalemia. Toxicol. Commun. 2019, 3, 88–90. [Google Scholar] [CrossRef]
- Gustafson, D.R.; Bäckman, K.; Scarmeas, N.; Stern, Y.; Manly, J.J.; Mayeux, R.; Gu, Y. Dietary Fatty Acids and Risk of Alzheimer’s Disease and Related Dementias: Observations from the Washington Heights-Hamilton Heights-Inwood Columbia Aging Project (WHICAP). Alzheimer’s Dement. 2020, 16, 1638–1649. [Google Scholar] [CrossRef]
- Adams, M.L.; Lombi, E.; Zhao, F.-J.; McGrath, S.P. Evidence of Low Selenium Concentrations in UK Bread-Making Wheat Grain. J. Sci. Food Agric. 2002, 82, 1160–1165. [Google Scholar] [CrossRef]
- Alfthan, G.; Eurola, M.; Ekholm, P.; Venäläinen, E.-R.; Root, T.; Korkalainen, K.; Hartikainen, H.; Salminen, P.; Hietaniemi, V.; Aspila, P.; et al. Effects of Nationwide Addition of Selenium to Fertilizers on Foods, and Animal and Human Health in Finland: From Deficiency to Optimal Selenium Status of the Population. J. Trace Elem. Med. Biol. 2015, 31, 142–147. [Google Scholar] [CrossRef]
- Wang, W.-C.; Mäkelä, A.-L.; Näntö, V.; Mäkelä, P.; Lagström, H. The Serum Selenium Concentrations in Children and Young Adults: A Long-Term Study during the Finnish Selenium Fertilization Programme. Eur. J. Clin. Nutr. 1998, 52, 529–535. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Selenium-enriched Yeast as Source for Selenium Added for Nutritional Purposes in Foods for Particular Nutritional Uses and Foods (Including Food Supplements) for the General Population—Scientific Opinion of the Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food. EFSA J. 2008, 6, 766. [Google Scholar] [CrossRef]
- Esmaeili, S.; Khosravi, K.; Pourahmad, R.; Komeili, R. An Experimental Design for Production of Selenium-Enriched Yeast. World Appl. Sci. J. 2012, 19, 31–37. [Google Scholar]
- Thomson, C.D. Assessment of Requirements for Selenium and Adequacy of Selenium Status: A Review. Eur. J. Clin. Nutr. 2004, 58, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Panel on Dietary Antioxidants and Related Compounds; Subcommittee on Upper Reference Levels of Nutrients; Subcommittee on Interpretation and Uses of Dietary Reference Intakes; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Food and Nutrition Board; Institute of Medicine. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000; p. 9810. ISBN 978-0-309-06935-9. [Google Scholar]
- Kieliszek, M. Selenium–Fascinating Microelement, Properties and Sources in Food. Molecules 2019, 24, 1298. [Google Scholar] [CrossRef] [PubMed]
- Frączek, A.; Pasternak, K. Selenium in Medicine and Treatment. J. Elem. 2012. [Google Scholar] [CrossRef]
- Thiry, C.; Ruttens, A.; De Temmerman, L.; Schneider, Y.-J.; Pussemier, L. Current Knowledge in Species-Related Bioavailability of Selenium in Food. Food Chem. 2012, 130, 767–784. [Google Scholar] [CrossRef]
- Moreda-Piñeiro, J.; Moreda-Piñeiro, A.; Bermejo-Barrera, P. In Vivo and In Vitro Testing for Selenium and Selenium Compounds Bioavailability Assessment in Foodstuff. Crit. Rev. Food Sci. Nutr. 2017, 57, 805–833. [Google Scholar] [CrossRef] [PubMed]
- Moreda-Piñeiro, J.; Moreda-Piñeiro, A.; Romarís-Hortas, V.; Domínguez-González, R.; Alonso-Rodríguez, E.; López-Mahía, P.; Muniategui-Lorenzo, S.; Prada-Rodríguez, D.; Bermejo-Barrera, P. In Vitro Bioavailability of Total Selenium and Selenium Species from Seafood. Food Chem. 2013, 139, 872–877. [Google Scholar] [CrossRef]
- Yu, Y.-X.; Li, J.-L.; Zhang, X.-Y.; Yu, Z.-Q.; Van De Wiele, T.; Han, S.-Y.; Wu, M.-H.; Sheng, G.-Y.; Fu, J.-M. Assessment of the Bioaccessibility of Polybrominated Diphenyl Ethers in Foods and the Correlations of the Bioaccessibility with Nutrient Contents. J. Agric. Food Chem. 2010, 58, 301–308. [Google Scholar] [CrossRef]
- Moreda-Piñeiro, J.; Moreda-Piñeiro, A.; Romarís-Hortas, V.; Domínguez-González, R.; Alonso-Rodríguez, E.; López-Mahía, P.; Muniategui-Lorenzo, S.; Prada-Rodríguez, D.; Bermejo-Barrera, P. ICP-MS for the Determination of Selenium Bioavailability from Seafood and Effect of Major Food Constituents. Microchem. J. 2013, 108, 174–179. [Google Scholar] [CrossRef]
- Mutanen, M.L.; Mykkänen, H.M. Effect of Dietary Fat on Plasma Glutathione Peroxidase Levels and Intestinal Absorption of 75Se-Labeled Sodium Selenite in Chicks. J. Nutr. 1984, 114, 829–834. [Google Scholar] [CrossRef]
- Bügel, S.; Sandström, B.; Skibsted, L.H. Pork Meat: A Good Source of Selenium? J. Trace Elem. Med. Biol. 2004, 17, 307–311. [Google Scholar] [CrossRef]
- Shen, L.; Dael, P.V.; Luten, L.; Deelstra, H. Estimation of Selenium Bioavailability from Human, Cow’s, Goat and Sheep Milk by an in Vitro Method. Int. J. Food Sci. Nutr. 1996, 47, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ralston, N.V.C.; Raymond, L.J. Dietary Selenium’s Protective Effects against Methylmercury Toxicity. Toxicology 2010, 278, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Reeves, P.G.; Leary, P.D.; Gregoire, B.R.; Finley, J.W.; Lindlauf, J.E.; Johnson, L.K. Selenium Bioavailability from Buckwheat Bran in Rats Fed a Modified AIN-93G Torula Yeast–Based Diet. J. Nutr. 2005, 135, 2627–2633. [Google Scholar] [CrossRef] [PubMed]
- Okano, Y.; Hattori, T.; Fujimoto, H.; Noi, K.; Okamoto, M.; Watanabe, T.; Watanabe, R.; Fujii, R.; Tamaoki, T. Nutritional Status of Patients with Phenylketonuria in Japan. Mol. Genet. Metab. Rep. 2016, 8, 103–110. [Google Scholar] [CrossRef]
- Alves, M.R.A.; Starling, A.L.P.; Kanufre, V.C.; Soares, R.D.L.; Norton, R.d.C.; Aguiar, M.J.B.; Januario, J.N. Selenium Intake and Nutritional Status of Children with Phenylketonuria in Minas Gerais, Brazil. J. Pediatr. 2012, 88, 396–400. [Google Scholar] [CrossRef]
- Demirdas, S.; van Spronsen, F.J.; Hollak, C.E.M.; van der Lee, J.H.; Bisschop, P.H.; Vaz, F.M.; Ter Horst, N.M.; Rubio-Gozalbo, M.E.; Bosch, A.M. Micronutrients, Essential Fatty Acids and Bone Health in Phenylketonuria. Ann. Nutr. Metab. 2017, 70, 111–121. [Google Scholar] [CrossRef]
- Van Bakel, M.M.; Printzen, G.; Wermuth, B.; Wiesmann, U.N. Antioxidant and Thyroid Hormone Status in Selenium-Deficient Phenylketonuric and Hyperphenylalaninemic Patients. Am. J. Clin. Nutr. 2000, 72, 976–981. [Google Scholar] [CrossRef]
- Zhu, K.; Yang, S.; Li, T.; Huang, X.; Dong, Y.; Wang, P.; Huang, J. Advances in the Study of the Mechanism by Which Selenium and Selenoproteins Boost Immunity to Prevent Food Allergies. Nutrients 2022, 14, 3133. [Google Scholar] [CrossRef]
- Matysiak, J. Modern Diagnostics in IgE-Mediated Cow’s Milk Allergy. J. Med. Sci. 2022, 91, e690. [Google Scholar] [CrossRef]
- Kamer, B.; Wąsowicz, W.; Pyziak, K.; Kamer-Bartosińska, A.; Gromadzińska, J.; Pasowska, R. Role of Selenium and Zinc in the Pathogenesis of Food Allergy in Infants and Young Children. Aoms 2012, 6, 1083–1088. [Google Scholar] [CrossRef]
- Zhao, X.; Thijssen, S.; Chen, H.; Garssen, J.; Knippels, L.M.J.; Hogenkamp, A. Selenium Modulates the Allergic Response to Whey Protein in a Mouse Model for Cow’s Milk Allergy. Nutrients 2021, 13, 2479. [Google Scholar] [CrossRef] [PubMed]
- Mak, T.-N.; Angeles-Agdeppa, I.; Tassy, M.; Capanzana, M.V.; Offord, E.A. The Nutritional Impact of Milk Beverages in Reducing Nutrient Inadequacy among Children Aged One to Five Years in the Philippines: A Dietary Modelling Study. Nutrients 2020, 12, 3330. [Google Scholar] [CrossRef] [PubMed]
- Caswell, B.L.; Arnold, C.D.; Lutter, C.K.; Iannotti, L.L.; Chipatala, R.; Werner, E.R.; Maleta, K.M.; Stewart, C.P. Impacts of an Egg Intervention on Nutrient Adequacy among Young Malawian Children. Matern. Child Nutr. 2021, 17, e13196. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Picciano, M.; Milner, J. Selenium Intakes and Status of Human Milk and Formula Fed Infants. Am. J. Clin. Nutr. 1982, 35, 521–526. [Google Scholar] [CrossRef]
- Flax, V.L.; Bentley, M.E.; Combs, G.F.; Chasela, C.S.; Kayira, D.; Tegha, G.; Kamwendo, D.; Daza, E.J.; Fokar, A.; Kourtis, A.P.; et al. Plasma and Breast-Milk Selenium in HIV-Infected Malawian Mothers Are Positively Associated with Infant Selenium Status but Are Not Associated with Maternal Supplementation: Results of the Breastfeeding, Antiretrovirals, and Nutrition Study. Am. J. Clin. Nutr. 2014, 99, 950–956. [Google Scholar] [CrossRef]
- Perez-Plazola, M.; Diaz, J.; Stewart, C.P.; Arnold, C.D.; Caswell, B.L.; Lutter, C.K.; Werner, E.R.; Maleta, K.; Turner, J.; Prathibha, P.; et al. Plasma Mineral Status after a Six-Month Intervention Providing One Egg per Day to Young Malawian Children: A Randomized Controlled Trial. Sci. Rep. 2023, 13, 6698. [Google Scholar] [CrossRef]
- Zyambo, K.; Hodges, P.; Chandwe, K.; Chisenga, C.C.; Mayimbo, S.; Amadi, B.; Kelly, P.; Kayamba, V. Selenium Status in Adults and Children in Urban Zambia: A Cross Sectional Study. SSRN J. 2022. [Google Scholar] [CrossRef]
- Bogye, G.; Alfthan, G.; Machay, T.; Zubovics, L. Enteral Yeast-Selenium Supplementation in Preterm Infants. Arch. Dis. Child. Fetal Neonatal Ed. 1998, 78, F225–F226. [Google Scholar] [CrossRef]
- Li, F.; Rossipal, E.; Micetic-Turk, D. Determination of Selenium in Serum by FI-HG-AAS and Calculation of Dietary Intake. Biol. Trace Elem. Res. Vol. 2000, 73, 201–210. [Google Scholar] [CrossRef]
- Darlow, B.; Inder, T.; Sluis, K.; Nuthall, G.; Mogridge, N.; Winterbourn, C. Selenium Status of New Zealand Infants Fed Either a Selenium Supplemented or a Standard Formula. J. Paediatr. Child Health 1995, 31, 339–344. [Google Scholar] [CrossRef]
- Daniels, L.; Gibson, R.; Simmer, K. Randomised Clinical Trial of Parenteral Selenium Supplementation in Preterm Infants. Arch. Dis. Child. Fetal Neonatal Ed. 1996, 74, F158–F164. [Google Scholar] [CrossRef] [PubMed]
- Strauss, K.A.; Wardley, B.; Robinson, D.; Hendrickson, C.; Rider, N.L.; Puffenberger, E.G.; Shelmer, D.; Moser, A.B.; Morton, D.H. Classical Maple Syrup Urine Disease and Brain Development: Principles of Management and Formula Design. Mol. Genet. Metab. 2010, 99, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Ölmez, A.; Yalcin, S.; Yurdakök, K.; Coskun, T. Serum Selenium Levels in Acute Gastroenteritis of Possible Viral Origin. J. Trop. Pediatr. 2004, 50, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S.; Kafwembe, E.; Mwanza, S.; Gosset, L.; Bailey, K.B.; Mullen, A.; Baisley, K.; Filteau, S. A Micronutrient-Fortified Food Enhances Iron and Selenium Status of Zambian Infants but Has Limited Efficacy on Zinc1–5. J. Nutr. 2011, 141, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Christodoulides, S.S.; Neal, E.G.; Fitzsimmons, G.; Chaffe, H.M.; Jeanes, Y.M.; Aitkenhead, H.; Cross, J.H. The Effect of the Classical and Medium Chain Triglyceride Ketogenic Diet on Vitamin and Mineral Levels: Vitamin and Mineral Levels on Ketogenic Diet. J. Hum. Nutr. Diet. 2012, 25, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Linday, L.A.; Shindledecker, R.D.; Dolitsky, J.N.; Pippenger, C.E. Lemon-Flavored Cod Liver Oil and a Multivitamin-Mineral Supplement for the Secondary Prevention of Otitis Media in Young Children: Pilot Research. Ann. Otol. Rhinol. Laryngol. 2002, 111, 642–652. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategies for Infant and Young Child Feeding; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]

| Age | AI µg/Day | UL µg/Day |
|---|---|---|
| 0–6 months | 12 | 45 * |
| 7–11 months | 15 | 55 |
| 1–3 years | 15 | 70 |
| 4–6 years | 20 | 95 |
| Age Group | Assumed Weight (kg) | Average Normative Requirement of Se (µg/Day) | Recommended Nutrient Intake (RNI) of Se | |
|---|---|---|---|---|
| Per kg Body Weight/Day | Total/Day | |||
| 0–6 months | 6 | 0.85 | 5.1 | 6 |
| 7–12 months | 9 | 0.91 | 8.2 | 10 |
| 1–3 years | 12 | 1.13 | 13.6 | 17 |
| 4–6 years | 19 | 0.92 | 17.5 | 22 |
| Food Source | Average Content µg/g | Average Se Content µg/per Serving (Serving Size) |
|---|---|---|
| Fish [75] | 0.4–4.3 | 20–215 µg [50 g] |
| Meats (mussels) [75] | 0.03–0.45 | 1.5–22.5 µg [50 g] |
| Yolk from egg [91] | 0.12–0.42 | 1.2–4.2 µg [10 g–½ piece] |
| Cereals [92] | 0.01–0.55 | 0.75–41.25 µg [75 g] |
| Broccoli [93] | 0.02 | 1 µg [50 g] |
| Cow’s milk [94] | 0.01–0.02 | 0.5–1 µg [50 mL] |
| Gouda cheese [94] | 0.08 | 1.2 µg [15 g–1 one slice] |
| Yoghurt [94] | 0.02 | 1 µg [50 g] |
| Food Ingredients | Effect on Bioavailability |
|---|---|
| Proteins | ↓ Se bioavailability with increasing protein content in fish and seafood |
| Fats | ↑ Se bioavailability with increase polyunsaturated fatty acid in diet—animal model study ↑ Se bioavailability with reducing the fat content in milk |
| Carbohydrates | ↑ Se bioavailability—analysed in fish and seafood |
| Dietary fibre | ↓ Se bioavailability |
| Vitamins A, D, and E | ↑ Se bioavailability |
| Sulphur | ↓ Se bioavailability sulphur in diet may compete with Se for absorption |
| Study | Type of Study | Country | Patients | Observations |
|---|---|---|---|---|
| Martens et al., 2015 [18] | interventional | Brazil | 129 children: 41 received 15–30 g of Brazil nuts 3 day/w and 88 did not receive nuts age: 4.7 ± 0.9 (3.1–6.3) years old in study group; 4.5 ± 1.2 (2.1–6.6) in control sex: both | Median (range) Se intake in the supplemented group: 155.30 (98.7–195.3) µg/day Median (range) Se intake in the control group: 44.40 (33.9–53.20) µg/day Given the EAR for Se of 17 µg/day for 1–3-year-olds and 23 µg/day for 4–8-year-olds, the children consumed excess Se even without supplementation with nuts Se intake was considered highly probable toxic in the group that received nuts |
| Mak et al., 2020 [165] | interventional | the Philippines | A total of 2642 children in given age groups: 792 children age: 1–2 years sex: both 1136 children age: 3–4 years sex: both 714 children age: 5 years sex: both | mean Se daily intake: 30.2 µg (23% of children had inadequately low Se intake) after supplementing 1 serving (180 g) of powdered milk: 31.2 µg/day after supplementing 1 serving (180 g) of YCM (young children’s milk formula): 35.5 µg/day mean Se daily intake: 45.9 µg (8% of children had inadequately low Se intake) after supplementing 1 serving (180 g) of powdered milk: 46.9 µg/day after supplementing 1 serving (180 g) of PCM (preschool children’s milk): 50.8 µg/day mean Se daily intake: 51.7 µg (4% of children had inadequately low Se intake) after supplementing 1 serving (180 g) of powdered milk: 52.8 µg/day after supplementing 1 serving (180 g) of PCM (preschool children’s milk): 57.1 µg/day In all groups, adding a portion of YCM/PCM significantly improved plasma Se levels; therefore, meeting the guidelines for daily diary recommendations can significantly decrease the number of children with inadequately low Se intake |
| Caswell et al., 2021 [166] | interventional | Malawi | 660 children (8% underweight, 1% wasted) age: 7.4 ± 1.2 months sex: both | Mean (SD) estimated usual intake of Se 19.7 ± 0.2 µg/day Children received 1 additional egg per day Baseline intake was adequate in most children (1% prevalence of inadequacy) but the intervention reduced the prevalence of inadequacy and improved the intake of fat, protein, vitamin A, riboflavin, vitamin B12, and choline |
| Smith et al., 1982 [167] | observational | USA | 28 children age: 3 months sex: both | group I (n = 8) received human milk only group II (n = 20) received formula (Enfamil) mean Se intake in group I: 10.08 ± 2.96 µg/day mean Se intake in group II: 7.22 ± 1.26 µg/day Formula-fed infants had significantly lower daily Se intake than breastfed and did not meet the recommendation of the National Research Council of 10–14 µg Se/day Correlation between intake and plasma levels showed that not only the amount of Se in formula but also its bioavailability should be taken into consideration |
| Flax et al., 2014 [168] | randomized controlled trial | Malawi | 526 children of HIV-infected mothers age: 2–6 weeks old sex: both | mean Se intake at 2nd–6th week of life: 10.1 ± 8.2 µg/day mean Se intake at 24th week of life: 7.7 ± 5.7 µg/day According to the WHO-recommended Se intake, 39% of infants did not achieve sufficient Se intake at 2–6 weeks or 24 weeks postpartum. The mean BMI of mothers was <23 kg/m2 |
| Infants |
|---|
|
|
| Expanding Diet |
|
| Dietary Recommendation from 1 to 3 Years Old |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dobrzyńska, M.; Kaczmarek, K.; Przysławski, J.; Drzymała-Czyż, S. Selenium in Infants and Preschool Children Nutrition: A Literature Review. Nutrients 2023, 15, 4668. https://doi.org/10.3390/nu15214668
Dobrzyńska M, Kaczmarek K, Przysławski J, Drzymała-Czyż S. Selenium in Infants and Preschool Children Nutrition: A Literature Review. Nutrients. 2023; 15(21):4668. https://doi.org/10.3390/nu15214668
Chicago/Turabian StyleDobrzyńska, Małgorzata, Katarzyna Kaczmarek, Juliusz Przysławski, and Sławomira Drzymała-Czyż. 2023. "Selenium in Infants and Preschool Children Nutrition: A Literature Review" Nutrients 15, no. 21: 4668. https://doi.org/10.3390/nu15214668