
Sarcopenic Obesity Is a Risk Factor for Worse Oncological Long-Term Outcome in Locally Advanced Rectal Cancer Patients: A Retrospective Single-Center Cohort Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Eligibility
2.2. Tumor Assessment
2.3. Baseline Variables
2.4. Treatment Strategy
2.5. Histopathological Examination
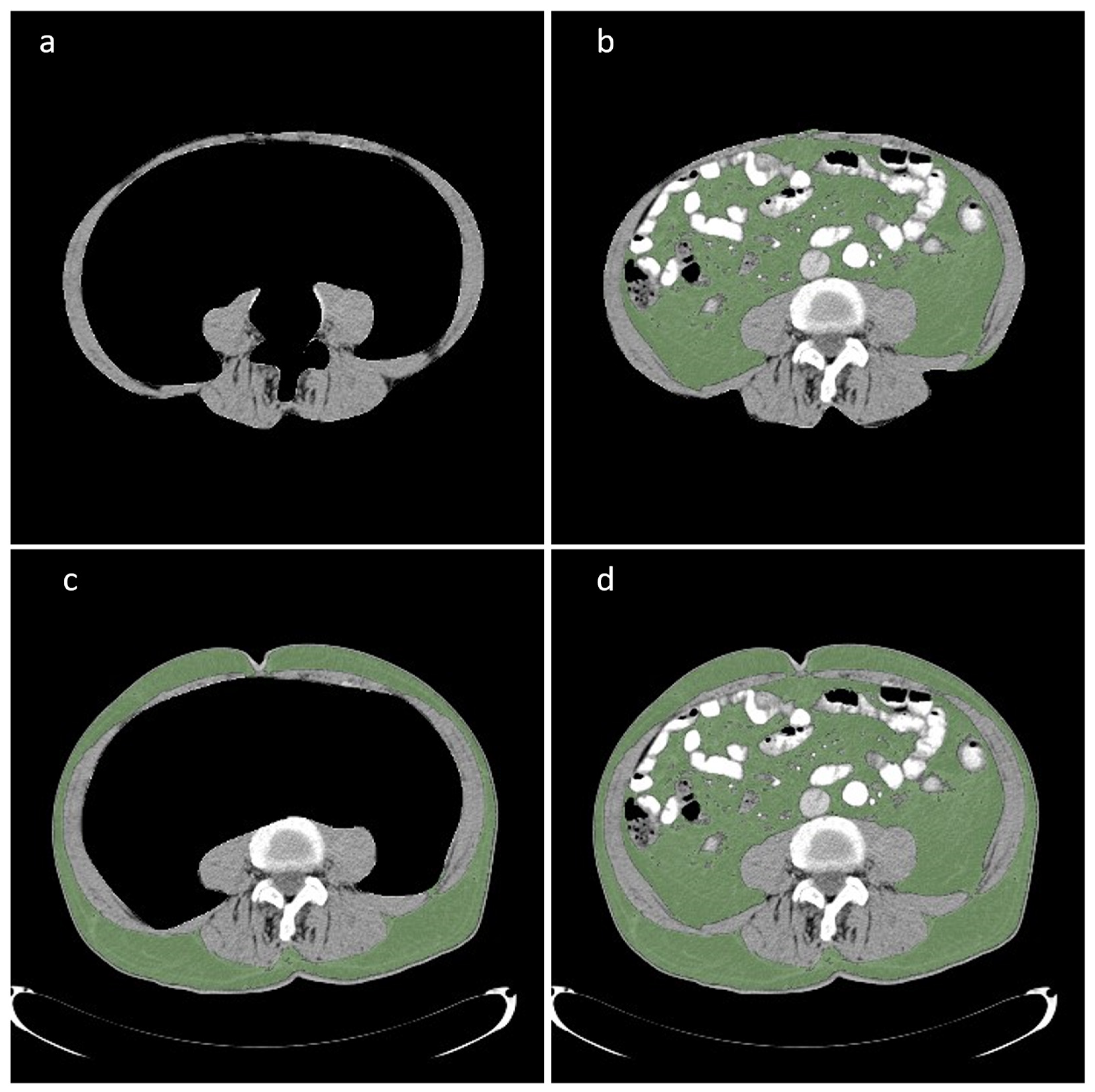
2.6. CT Evaluation
2.7. Statistical Analysis
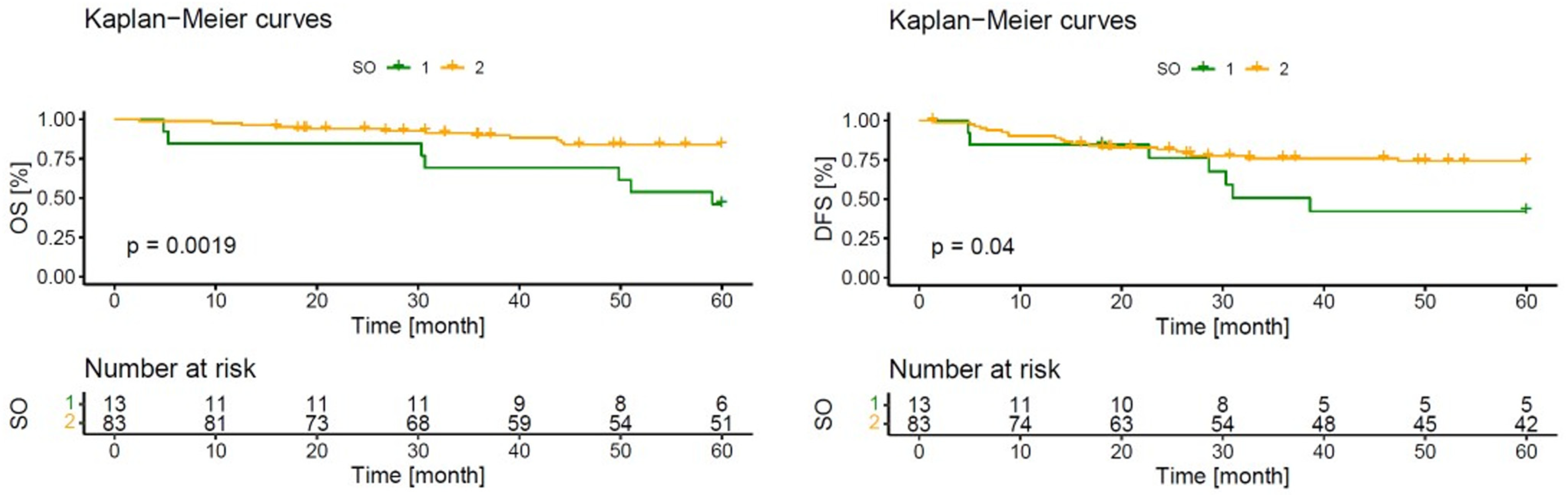
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRC | Colorectal cancer |
| LAR | Low anterior resection |
| AL | Anastomotic leakage |
| BMI | Body mass index |
| CT | Computer tomography |
| MRI | Magnetic resonance imaging |
| ASA | American Society of Anesthesiologists |
| UICC | Union for International Cancer Control |
| DFS | Disease-free survival |
| OS | Overall survival |
| HU | Hounsfield units |
| TFA | Total fat area |
| VFA | Visceral fat area |
| SFA | Subcutaneous fat area |
| SMA | Skeletal muscle area |
| SMI | Skeletal muscle index |
| TME | Total mesorectal excision |
| CCI | Charlson Comorbidity Index |
References
- Bocca, G.; Mastoridis, S.; Yeung, T.; James, D.R.C.; Cunningham, C. Visceral-to-subcutaneous fat ratio exhibits strongest association with early post-operative outcomes in patients undergoing surgery for advanced rectal cancer. Int. J. Colorectal Dis. 2022, 37, 1893–1900. [Google Scholar] [CrossRef]
- Rawla, P.; Sunkara, T.; Barsouk, A. Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Prz. Gastroenterol. 2019, 14, 89–103. [Google Scholar] [CrossRef]
- Hossain, M.S.; Karuniawati, H.; Jairoun, A.A.; Urbi, Z.; Ooi, D.J.; John, A.; Lim, Y.C.; Kibria, K.M.K.; Mohiuddin, A.K.M.; Ming, L.C.; et al. Colorectal Cancer: A Review of Carcinogenesis, Global Epidemiology, Current Challenges, Risk Factors, Preventive and Treatment Strategies. Cancers 2022, 14, 1732. [Google Scholar] [CrossRef]
- Tschann, P.; Weigl, M.P.; Szeverinski, P.; Lechner, D.; Brock, T.; Rauch, S.; Rossner, J.; Eiter, H.; Girotti, P.N.C.; Jäger, T.; et al. Are risk factors for anastomotic leakage influencing long-term oncological outcomes after low anterior resection of locally advanced rectal cancer with neoadjuvant therapy? A single-centre cohort study. Langenbecks. Arch. Surg. 2022, 407, 2945–2957. [Google Scholar] [CrossRef]
- Harris, L.J.; Phillips, B.R.; Maxwell, P.J.; Isenberg, G.A.; Goldstein, S.D. Outcomes of low anterior resection anastomotic leak after preoperative chemoradiation therapy for rectal cancer. Am. Surg. 2010, 76, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, H.; Matsuda, T.; Arimoto, A.; Yamashita, K.; Nishi, M.; Takase, N.; Hosono, M.; Nakamura, T.; Suzuki, S.; Kakeji, Y. Does anastomotic leakage after rectal cancer resection worsen long-term oncologic outcome? Int. J. Colorectal Dis. 2020, 35, 1243–1253. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.C.; Lim, S.-B.; Lee, J.L.; Kim, C.W.; Yoon, Y.S.; Park, I.J.; Yu, C.S.; Kim, J.C. Defunctioning Protective Stoma Can Reduce the Rate of Anastomotic Leakage after Low Anterior Resection in Rectal Cancer Patients. Ann. Coloproctol. 2020, 36, 192–197. [Google Scholar] [CrossRef]
- Wang, F.-G.; Yan, W.-M.; Yan, M.; Song, M.-M. Comparison of anastomotic leakage rate and reoperation rate between transanal tube placement and defunctioning stoma after anterior resection: A network meta-analysis of clinical data. Eur. J. Surg. Oncol. 2019, 45, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Zhang, L.; Gao, F.; Wu, M.; Zheng, J.; Bai, L.; Li, F.; Liu, B.; Pan, Z.; Liu, J.; et al. Transanal Drainage Tube Use for Preventing Anastomotic Leakage After Laparoscopic Low Anterior Resection in Patients With Rectal Cancer: A Randomized Clinical Trial. JAMA Surg. 2021, 156, 1151–1158. [Google Scholar] [CrossRef]
- Du, P.; Burke, J.P.; Khoury, W.; Lavery, I.C.; Kiran, R.P.; Remzi, F.H.; Dietz, D.W. Factors associated with the location of local rectal cancer recurrence and predictors of survival. Int. J. Colorectal Dis. 2016, 31, 825–832. [Google Scholar] [CrossRef]
- Jäger, T.; Nawara, C.; Neureiter, D.; Holzinger, J.; Öfner-Velano, D.; Dinnewitzer, A. Einfluss der Anastomoseninsuffizienz auf das Langzeitüberleben beim tiefen Rektumkarzinom. Chirurg 2015, 86, 1072–1082. [Google Scholar] [CrossRef]
- van Rees, J.M.; Visser, E.; van Vugt, J.L.A.; Rothbarth, J.; Verhoef, C.; van Verschuer, V.M.T. Impact of nutritional status and body composition on postoperative outcomes after pelvic exenteration for locally advanced and locally recurrent rectal cancer. BJS Open 2021, 5, zrab096. [Google Scholar] [CrossRef] [PubMed]
- van Vugt, J.L.A.; Braam, H.J.; van Oudheusden, T.R.; Vestering, A.; Bollen, T.L.; Wiezer, M.J.; de Hingh, I.H.J.T.; van Ramshorst, B.; Boerma, D. Skeletal Muscle Depletion is Associated with Severe Postoperative Complications in Patients Undergoing Cytoreductive Surgery with Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis of Colorectal Cancer. Ann. Surg. Oncol. 2015, 22, 3625–3631. [Google Scholar] [CrossRef]
- Martin, L.; Birdsell, L.; Macdonald, N.; Reiman, T.; Clandinin, M.T.; McCargar, L.J.; Murphy, R.; Ghosh, S.; Sawyer, M.B.; Baracos, V.E. Cancer cachexia in the age of obesity: Skeletal muscle depletion is a powerful prognostic factor, independent of body mass index. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 1539–1547. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Horwich, T.B.; Oreopoulos, A.; Kovesdy, C.P.; Younessi, H.; Anker, S.D.; Morley, J.E. Risk factor paradox in wasting diseases. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, L.; Bonne, A.; Trilling, B.; Foote, A.; Laverrière, M.-H.; Roth, G.; Fournier, J.; Girard, E.; Faucheron, J.-L. Impact of obesity on morbidity and oncologic outcomes after total mesorectal excision for mid and low rectal cancer. Tech. Coloproctol. 2022, 27, 407–418. [Google Scholar] [CrossRef]
- Tschann, P.; Lechner, D.; Girotti, P.N.C.; Adler, S.; Rauch, S.; Presl, J.; Jäger, T.; Schredl, P.; Mittermair, C.; Szeverinski, P.; et al. Incidence and risk factors for umbilical incisional hernia after reduced port colorectal surgery (SIL + 1 additional port)-is an umbilical midline approach really a problem? Langenbecks. Arch. Surg. 2022, 407, 1241–1249. [Google Scholar] [CrossRef]
- Kang, J.; Baek, S.-E.; Kim, T.; Hur, H.; Min, B.S.; Lim, J.S.; Kim, N.K.; Lee, K.Y. Impact of fat obesity on laparoscopic total mesorectal excision: More reliable indicator than body mass index. Int. J. Colorectal Dis. 2012, 27, 497–505. [Google Scholar] [CrossRef]
- Bao, Q.R.; Crimì, F.; Valotto, G.; Chiminazzo, V.; Bergamo, F.; Prete, A.A.; Galuppo, S.; El Khouzai, B.; Quaia, E.; Pucciarelli, S.; et al. Obesity may not be related to pathologic response in locally advanced rectal cancer following neoadjuvant chemoradiotherapy. Front. Oncol. 2022, 12, 994444. [Google Scholar] [CrossRef]
- Doyle, D.J.; Goyal, A.; Garmon, E.H. StatPearls: American Society of Anesthesiologists Classification; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Brierley, J.D. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA; Incorporated: Chicester, UK, 2017; ISBN 9781119263562. [Google Scholar]
- Deutsche Krebsgesellschaft, D.K. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF): S3-Leitlinie Kolorektales Karzinom, Langversion 2.1, 2019, AWMF Registrierungsnummer: 021/007OL. Available online: https://www.leitlinienprogramm-onkologie.de/leitlinien/kolorektales-karzinom/ (accessed on 16 March 2023).
- Quirke, P.; Durdey, P.; Dixon, M.F.; Williams, N.S. Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet 1986, 2, 996–999. [Google Scholar] [CrossRef]
- Fleming, C.A.; O’Connell, E.P.; Kavanagh, R.G.; O’Leary, D.P.; Twomey, M.; Corrigan, M.A.; Wang, J.H.; Maher, M.M.; O’Connor, O.J.; Redmond, H.P. Body Composition, Inflammation, and 5-Year Outcomes in Colon Cancer. JAMA Netw. Open 2021, 4, e2115274. [Google Scholar] [CrossRef]
- van der Werf, A.; Langius, J.A.E.; de van der Schueren, M.A.E.; Nurmohamed, S.A.; van der Pant, K.A.M.I.; Blauwhoff-Buskermolen, S.; Wierdsma, N.J. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur. J. Clin. Nutr. 2018, 72, 288–296. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samples). Biometrika 1965, 52, 591. [Google Scholar] [CrossRef]
- Barret, M.; Malka, D.; Aparicio, T.; Dalban, C.; Locher, C.; Sabate, J.-M.; Louafi, S.; Mansourbakht, T.; Bonnetain, F.; Attar, A.; et al. Nutritional status affects treatment tolerability and survival in metastatic colorectal cancer patients: Results of an AGEO prospective multicenter study. Oncology 2011, 81, 395–402. [Google Scholar] [CrossRef]
- Giani, A.; Famularo, S.; Riva, L.; Tamini, N.; Ippolito, D.; Nespoli, L.; Conconi, P.; Sironi, S.; Braga, M.; Gianotti, L. Association between specific presurgical anthropometric indexes and morbidity in patients undergoing rectal cancer resection. Nutrition 2020, 75–76, 110779. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyamoto, Y.; Baba, Y.; Sakamoto, Y.; Ohuchi, M.; Tokunaga, R.; Kurashige, J.; Hiyoshi, Y.; Iwagami, S.; Yoshida, N.; Yoshida, M.; et al. Sarcopenia is a Negative Prognostic Factor After Curative Resection of Colorectal Cancer. Ann. Surg. Oncol. 2015, 22, 2663–2668. [Google Scholar] [CrossRef] [PubMed]
- Lieffers, J.R.; Bathe, O.F.; Fassbender, K.; Winget, M.; Baracos, V.E. Sarcopenia is associated with postoperative infection and delayed recovery from colorectal cancer resection surgery. Br. J. Cancer 2012, 107, 931–936. [Google Scholar] [CrossRef] [Green Version]
- Gortan Cappellari, G.; Guillet, C.; Poggiogalle, E.; Ballesteros Pomar, M.D.; Batsis, J.A.; Boirie, Y.; Breton, I.; Frara, S.; Genton, L.; Gepner, Y.; et al. Sarcopenic obesity research perspectives outlined by the sarcopenic obesity global leadership initiative (SOGLI)-Proceedings from the SOGLI consortium meeting in rome November 2022. Clin. Nutr. 2023, 42, 687–699. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Kritchevsky, S.B.; Goodpaster, B.H.; Newman, A.B.; Nevitt, M.; Stamm, E.; Harris, T.B. Leg muscle mass and composition in relation to lower extremity performance in men and women aged 70 to 79: The health, aging and body composition study. J. Am. Geriatr. Soc. 2002, 50, 897–904. [Google Scholar] [CrossRef]
- Feliciano, E.M.C.; Kroenke, C.H.; Meyerhardt, J.A.; Prado, C.M.; Bradshaw, P.T.; Kwan, M.L.; Xiao, J.; Alexeeff, S.; Corley, D.; Weltzien, E.; et al. Association of Systemic Inflammation and Sarcopenia With Survival in Nonmetastatic Colorectal Cancer: Results From the C SCANS Study. JAMA Oncol. 2017, 3, e172319. [Google Scholar] [CrossRef] [PubMed]
- Chua, W.; Charles, K.A.; Baracos, V.E.; Clarke, S.J. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br. J. Cancer 2011, 104, 1288–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, J.S.; Ryu, H.; Park, I.J.; Kim, K.W.; Shin, Y.; Kim, S.O.; Lim, S.-B.; Kim, C.W.; Yoon, Y.S.; Lee, J.L.; et al. Association of Body Composition with Long-Term Survival in Non-metastatic Rectal Cancer Patients. Cancer Res. Treat. 2020, 52, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Malietzis, G.; Johns, N.; Al-Hassi, H.O.; Knight, S.C.; Kennedy, R.H.; Fearon, K.C.H.; Aziz, O.; Jenkins, J.T. Low Muscularity and Myosteatosis Is Related to the Host Systemic Inflammatory Response in Patients Undergoing Surgery for Colorectal Cancer. Ann. Surg. 2016, 263, 320–325. [Google Scholar] [CrossRef] [PubMed]
- Giani, A.; Famularo, S.; Fogliati, A.; Riva, L.; Tamini, N.; Ippolito, D.; Nespoli, L.; Braga, M.; Gianotti, L. Skeletal muscle wasting and long-term prognosis in patients undergoing rectal cancer surgery without neoadjuvant therapy. World J. Surg. Oncol. 2022, 20, 51. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients’ Characteristics | Total (n = 96) |
|---|---|
| Sex, Male/Female, n (%) | 64 (66.7%)/32 (33.3%) |
| Age (year), mean ± std | 64.0 ± 11.0 |
| BMI (kg/m2), mean ± std | 26.7 ± 4.2 |
| ASA Classification, n (%) | |
| I | 14 (14.6%) |
| II | 49 (51.0%) |
| III | 30 (31.3%) |
| IV | 1 (1.0%) |
| V | 0 (0.0%) |
| Tumor localization (in cm from the anal verge), mean ± std | 7.5 ± 3.7 |
| CEA level preoperative (µg/l), mean ± std | 3.8 ± 4.4 |
| Comorbidities, n (%) | 49 (51.0%) |
| Charlson Comorbidity Index | 5.4 ± 2.5 |
| Preoperative therapy, n (%) | |
| Combined long-term chemo-radiation | 80 (83.3%) |
| Short-term radiation (5 × 5 Gy) | 16 (16.7%) |
| Type of Anastomosis, n (%) (n = 97) | |
| Stapled E-E | 62 (64.6%) |
| Stapled S-E | 24 (25.0%) |
| Hand sewn colo-anal anastomosis | 10 (10.4%) |
| Operative technique, n (%) | |
| open | 56 (58.3%) |
| laparoscopic | 40 (41.8%) |
| Operation time (min), mean ± std: | 207.9 ± 64.6 |
| Complications, n (%) | 36 (37.5%) |
| Anastomotic leakage | 20 (20.8%) |
| Superficial SSI | 1 (1.0%) |
| Bleeding | 2 (2.1%) |
| Bowel obstruction | 5 (5.2%) |
| Renal failure | 1 (1.0%) |
| Stoma obstruction | 1 (1.0%) |
| Parastomal hernia | 2 (2.1%) |
| Others | 3 (3.1%) |
| Clavien-Dindo Classificatio, n (%) | |
| I | 2 (2.1%) |
| II | 4 (4.2%) |
| III | 28 (29.2%) |
| IV | 0 (0.0%) |
| V | 1 (1.0%) |
| Duration of hospital stay (d), mean ± std | 20.0 ± 14.2 |
| TME quality, n (%) | |
| Grade 1 (good) | 67 (69.8%) |
| Grade 2 (moderate) | 21 (21.9%) |
| Grade 3 (poor) | 8 (8.3%) |
| Pathological yT stages, n (%) | |
| 0 | 13 (13.5%) |
| Tis | 2 (2.1%) |
| T1 | 3 (3.1%) |
| T2 | 33 (34.4%) |
| T3 | 43 (44.8%) |
| T4 | 2 (2.1%) |
| Pathological yN Stage, n (%) | |
| N0 | 64 (66.7%) |
| N1 | 19 (19.8%) |
| N2 | 13 (13.5%) |
| Postoperative UICC-Stage, n (%) | |
| 0 | 14 (14.6%) |
| I | 28 (29.2%) |
| II | 22 (22.9%) |
| III | 32 (33.3%) |
| Residual Tumor (R1), n (%) | 4 (4.2%) |
| Adjuvant chemotherapy, n (%) | 47 (49.0%) |
| Follow-up: | |
| Follow-up time (months), mean ± std | 69.0 ± 46.5 |
| Local recurrence, n (%) | 6 (6.3%) |
| Distant metastasis, n (%) | 22 (22.9%) |
| Normal | Underweight | Overweight | p-Value | ||
|---|---|---|---|---|---|
| Subcutaneous adiposity | <0.01 | ||||
| No | 23 (76.7%) | 4 (100.0%) | 24 (38.7%) | ||
| Yes | 7 (23.3%) | 0 (0.0%) | 38 (61.3%) | ||
| Visceral adiposity | <0.01 | ||||
| No | 15 (50.0%) | 4 (100.0%) | 13 (21.0%) | ||
| Yes | 15 (50.0) | 0 (0.0%) | 49 (79.0%) | ||
| Visceral to total fat ratio | 0.058 | ||||
| No | 14 (46.7%) | 2 (50.0%) | 16 (25.8%) | ||
| Yes | 16 (53.3%) | 2 (50.0%) | 46 (74.2%) | ||
| Sarcopenic obesety | 0.771 | ||||
| No | 3 (10.0%) | 0 (0.0%) | 7 (11.3%) | ||
| Yes | 27 (90.0%) | 4 (100.0%) | 55 (88.7%) | ||
| Skelettal muscle index | 0.138 | ||||
| No | 5 (16.7%) | 2 (50.0%) | 8 (12.9%) | ||
| Yes | 25 (83.3%) | 2 (50.0%) | 54 (87.1%) | ||
| Subcutaneous to total fat ratio | 0.06 | ||||
| No | 12 (40.0%) | 4 (100.0%) | 34 (54.8%) | ||
| Yes | 18 (60.0%) | 0 (0.0%) | 28 (45.2%) | ||
| Skelettal muscle area | 0.157 | ||||
| No | 7 (23.3%) | 2 (50.0%) | 9 (14.5%) | ||
| Yes | 23 (76.7%) | 2 (50.0%) | 53 (85.5%) | ||
| Total fat | 0.001 | ||||
| No | 27 (90.0%) | 4 (100.0%) | 33 (53.2%) | ||
| Yes | 3 (10.0%) | 0 (0.0%) | 29 (46.8%) | ||
| Variable | Overall Morbidity | Anastomotic Leakage | Disease Free Survival | Local Recurrency | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| yes | no | p-value | yes | no | p-value | yes | no | p-value | yes | no | p-value | |
| Age | 69.0 ± 10.0 | 62.0 ± 11.0 | 0.004 | 68.0 ± 10.0 | 64.0 ± 12.0 | 0.151 | 65.0 ± 11.0 | 64.0 ± 12.0 | 0.829 | 71.0 ± 12.0 | 64.0 ± 11.0 | 0.178 |
| Sex (Male/Female) | 23 (65.7%)/12 (34.3%) | 41 (67.2%)/20 (32.8%) | 1 | 16 (69.6%) /7 (30.4%) | 48 (65.8%)/25 (34.3%) | 0.933 | 47 (64.4%)/26 (35.6%) | 17 (73.9%)/6 (26.1%) | 0.554 | 4 (66.7%) /2 (33.3%) | 60 (66.7%)/30 (33.3%) | 1 |
| CCI | 6.6 ± 2.5 | 4.66 ± 2.2 | <0.01 | 6.6 ± 2.5 | 5.0 ± 2.4 | 0.006 | 5.4 ± 2.5 | 5.39 ± 2.5 | 0.89 | 4.8 ± 0.9 | 5.4 ± 2.6 | 0.909 |
| Type of neoadjuvant therapy | 0.129 | 0.285 | 0.134 | 0.572 | ||||||||
| long-term | 26 (74.3%) | 54 (88.5%) | 17 (73.9%) | 63 (86.3%) | 58 (79.5%) | 22 (95.7%) | 6 (100.0%) | 74 (82.2%) | ||||
| short-term | 9 (25.7%) | 7 (11.5%) | 6 (26.1%) | 10 (13.7%) | 15 (20.5%) | 1 (4.3%) | 0 (0.0%) | 16 (17.8%) | ||||
| Type of surgery | 0.971 | 0.968 | 0.968 | 1 | ||||||||
| open | 21 (60.0%) | 35 (57.4%) | 14 (60.9%) | 42 (57.5%) | 42 (57.5%) | 14 (60.9%) | 4 (66.7%) | 52 (57.8%) | ||||
| laparoscopic | 14 (40.0%) | 26 (42.6%) | 9 (39.1%) | 31 (42.5%) | 31 (42.5%) | 9 (39.1%) | 2 (33.3%) | 38 (42.2%) | ||||
| TME-Quality | 0.695 | 0.997 | 0.639 | 0.733 | ||||||||
| 1 (good) | 26 (74.3%) | 41 (67.2%) | 16 (69.6%) | 51 (69.9%) | 52 (71.2%) | 15 (65.3%) | 4 (66.7%) | 63 (70.0%) | ||||
| 2 (moderate) | 6 (17.1%) | 15 (24.6%) | 5 (21.7%) | 16 (21.9%) | 16 (21.9%) | 5 (21.7%) | 1 (16.7%) | 20 (22.2%) | ||||
| 3 (worse) | 3 (8.6%) | 5 (8.2%) | 2 (8.7%) | 6 (8.2%) | 5 (6.9%) | 3 (13.0%) | 1 (16.7%) | 7 (7.8%) | ||||
| BMI | 0.72 | 0.635 | 0.995 | 0.591 | ||||||||
| Normal | 12 (34.3%) | 18 (29.5%) | 9 (39.1%) | 21 (28.8%) | 23 (31.5%) | 7 (30.4%) | 1 (16.7%) | 29 (32.2%) | ||||
| Underweight | 2 (5.7%) | 2 (3.3%) | 1 (4.4%) | 3 (4.1%) | 3 (4.1%) | 1 (4.4%) | 0 (0.0%) | 4 (4.4%) | ||||
| Overweight | 21 (60.0%) | 41 (67.2%) | 13 (56.5%) | 49 (67.1%) | 47 (64.4%) | 15 (65.2%) | 5 (83.3%) | 57 (63.3%) | ||||
| Subcutaneous adiposity | 250.4 ± 97.2 | 225.3 ± 103.1 | 0.146 | 254.6 ± 85.4 | 228.2 ± 105.5 | 0.141 | 244.3 ± 101.7 | 203.4 ± 95.1 | 0.108 | 232.8 ± 66.0 | 234.6 ± 103.6 | 0.862 |
| Visceral adiposity | 165.0 ± 71.4 | 177.0 ± 91.7 | 0.787 | 171.0 ± 56.8 | 173.2 ± 92.2 | 0.874 | 175.0 ± 86.0 | 165.2 ± 81.6 | 0.631 | 206.3 ± 85.1 | 170.4 ± 84.6 | 0.454 |
| Skelettal muscle index | 45.1 ± 15.9 | 51.4 ± 13.5 | 0.053 | 45.6 ± 12.2 | 50.2 ± 15.3 | 0.135 | 49.4 ± 14.3 | 48.2 ± 16.0 | 0.874 | 43.3 ± 13.9 | 49.5 ± 14.7 | 0.329 |
| Subcutaneous to total fat ratio | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.096 | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.363 | 0.6 ± 0.1 | 0.6 ± 0.1 | 0.178 | 0.5 ± 0.1 | 0.6 ± 0.1 | 0.345 |
| Skelettal muscle area | 129.4 ± 47.6 | 151.0 ± 46.3 | 0.045 | 131.6 ± 38.2 | 146.8 ± 50.1 | 0.152 | 145.0 ± 48.3 | 137.1 ± 46.3 | 0.609 | 122.5 ± 42.7 | 144.5 ± 48.0 | 0.217 |
| Total fat | 412.6 ± 149.6 | 402.4 ± 161.3 | 0.615 | 421.3 ± 123.5 | 401.3 ± 166.2 | 0.474 | 417.9 ± 155.1 | 368.6 ± 158.3 | 0.142 | 439.2 ± 142.4 | 403.9 ± 157.9 | 0.7 |
| Visceral to total fat ratio | 0.4 ± 0.1 | 0.4 ± 0.1 | 0.204 | 0.42 ± 0.13 | 0.4 ± 0.1 | 0.699 | 0.4 ± 0.1 | 0.5 ± 0.1 | 0.243 | 0.5 ± 0.1 | 0.4 ± 0.1 | 0.393 |
| Sarcopenic obesity | 8 (22.9%) | 3 (4.9%) | 0.02 | 3 (13.0%) | 8 (11.0%) | 1 | 9 (12.3%) | 3 (13.0%) | 1 | 0 (0.0%) | 11 (12.2%) | 0.804 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tschann, P.; Weigl, M.P.; Clemens, P.; Szeverinski, P.; Attenberger, C.; Kowatsch, M.; Jäger, T.; Emmanuel, K.; Brock, T.; Königsrainer, I. Sarcopenic Obesity Is a Risk Factor for Worse Oncological Long-Term Outcome in Locally Advanced Rectal Cancer Patients: A Retrospective Single-Center Cohort Study. Nutrients 2023, 15, 2632. https://doi.org/10.3390/nu15112632
Tschann P, Weigl MP, Clemens P, Szeverinski P, Attenberger C, Kowatsch M, Jäger T, Emmanuel K, Brock T, Königsrainer I. Sarcopenic Obesity Is a Risk Factor for Worse Oncological Long-Term Outcome in Locally Advanced Rectal Cancer Patients: A Retrospective Single-Center Cohort Study. Nutrients. 2023; 15(11):2632. https://doi.org/10.3390/nu15112632
Chicago/Turabian StyleTschann, Peter, Markus P. Weigl, Patrick Clemens, Philipp Szeverinski, Christian Attenberger, Matthias Kowatsch, Tarkan Jäger, Klaus Emmanuel, Thomas Brock, and Ingmar Königsrainer. 2023. "Sarcopenic Obesity Is a Risk Factor for Worse Oncological Long-Term Outcome in Locally Advanced Rectal Cancer Patients: A Retrospective Single-Center Cohort Study" Nutrients 15, no. 11: 2632. https://doi.org/10.3390/nu15112632