
Associations between Consumption of Dietary Fibers and the Risk of Type 2 Diabetes, Hypertension, Obesity, Cardiovascular Diseases, and Mortality in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
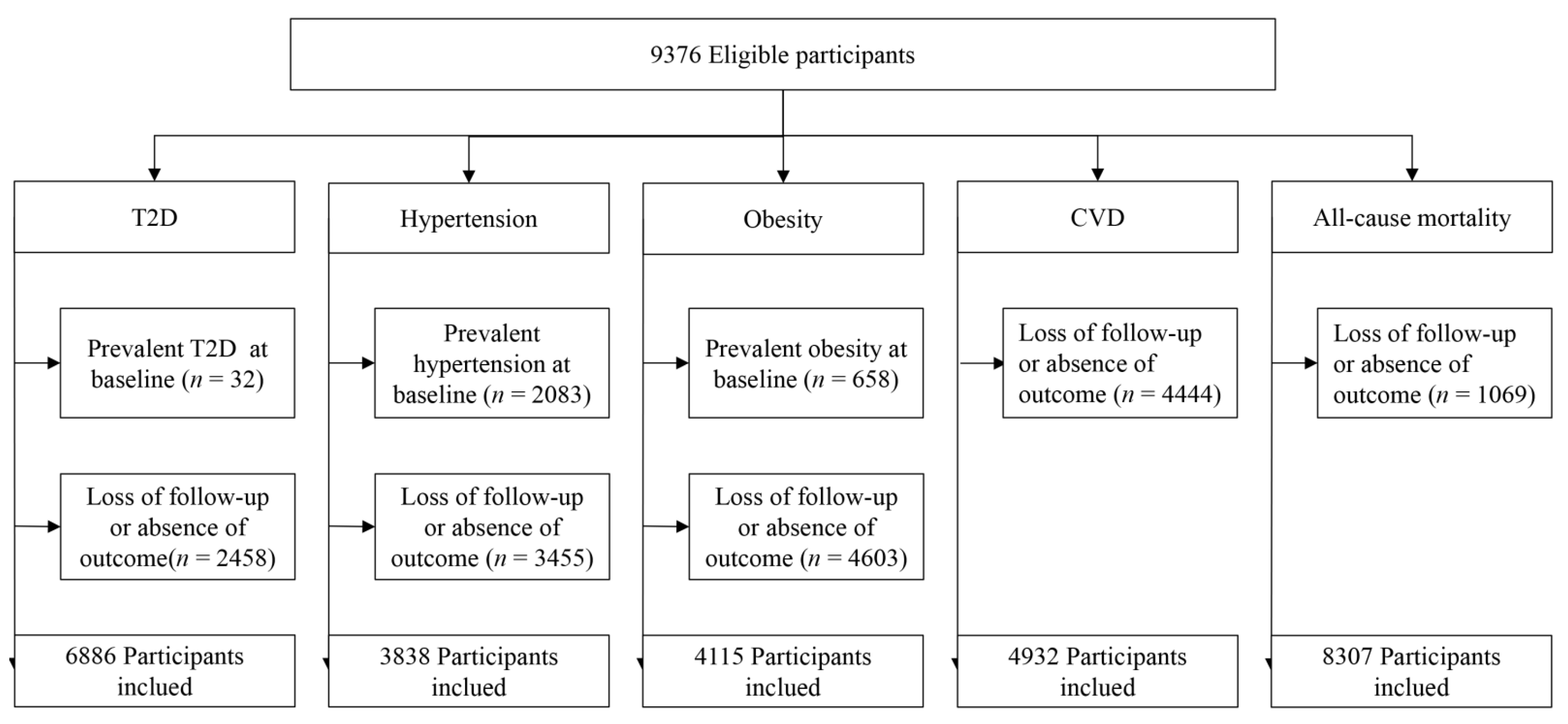
2.1. Study Design and Participants
2.2. Dietary Assessment
2.3. Measurement
2.4. Case Ascertainment
2.5. Statistical Analysis
3. Results
3.1. Description of the Study Population
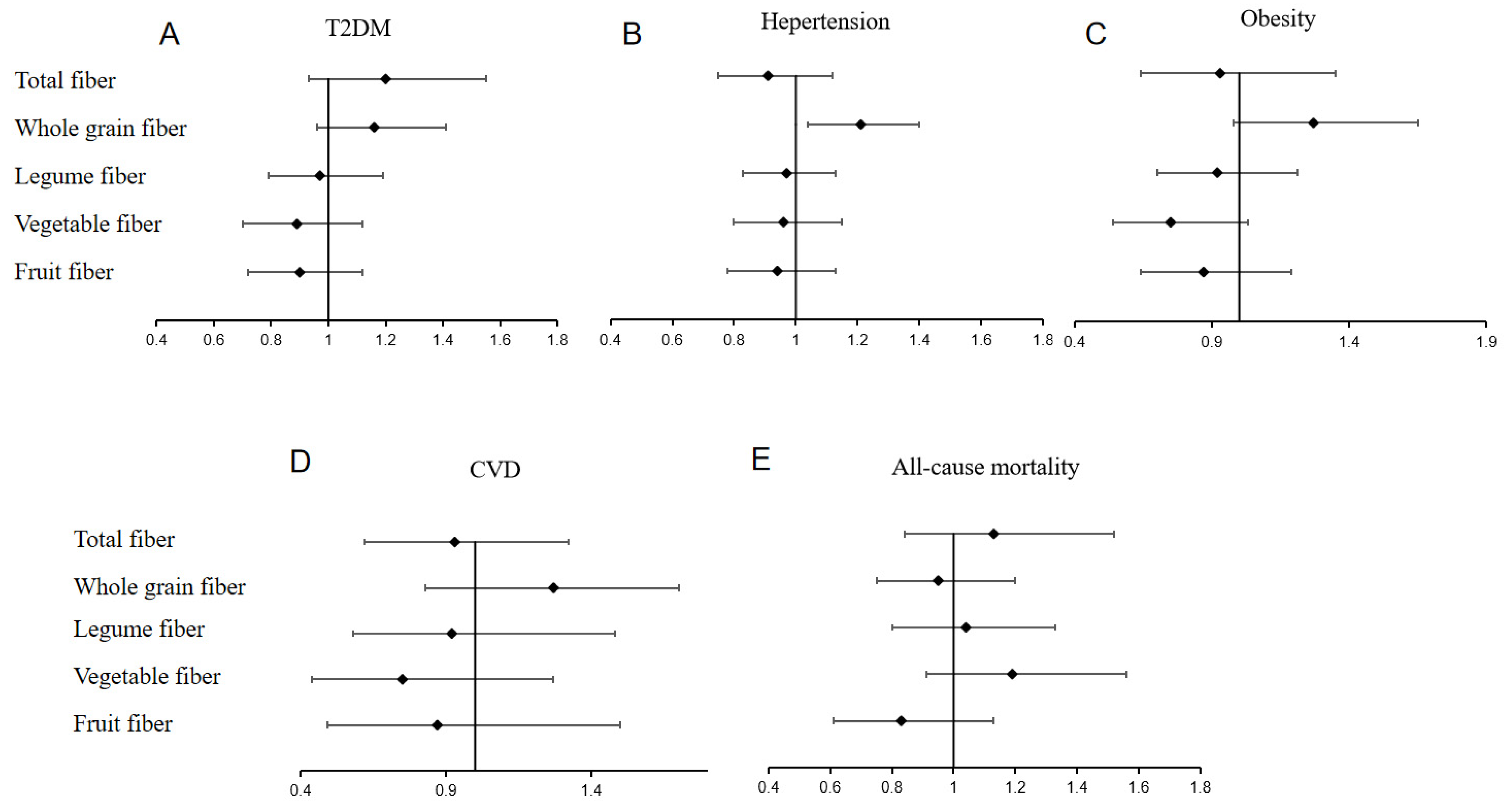
3.2. Associations between Total Dietary Fiber Intake and T2D, Hypertension, Obesity, CVD, and All-Cause Mortality
3.3. Associations between Whole-Grain Fiber Intake and T2D, Hypertension, Obesity, CVD, and All-Cause Mortality
3.4. Associations between Legume Fiber Intake and T2D, Hypertension, Obesity, CVD, and All-Cause Mortality
3.5. Associations between Vegetable Fiber Intake and T2D, Hypertension, Obesity, CVD, and All-Cause Mortality
3.6. Associations between Fruit Fiber Intake and T2D, Hypertension, Obesity, CVD, and All-Cause Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Salpea, P.; Karuranga, S.; Petersohn, I.; Malanda, B.; Gregg, E.W.; Unwin, N.; Wild, S.H.; Williams, R. Mortality attributable to diabetes in 20–79 years old adults, 2019 estimates: Results from the international diabetes federation diabetes atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108086. [Google Scholar] [CrossRef] [Green Version]
- Watkins, D.A.; Johnson, C.O.; Colquhoun, S.M.; Karthikeyan, G.; Beaton, A.; Bukhman, G.; Forouzanfar, M.H.; Longenecker, C.T.; Mayosi, B.M.; Mensah, G.A.; et al. Global, regional, and national burden of rheumatic heart disease, 1990–2015. N. Engl. J. Med. 2017, 377, 713–722. [Google Scholar] [CrossRef]
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Mills, K.T.; Bundy, J.D.; Kelly, T.N.; Reed, J.E.; Kearney, P.M.; Reynolds, K.; Chen, J.; He, J. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 countries. Circulation 2016, 134, 441–450. [Google Scholar] [CrossRef]
- InterAct Consortium. Dietary fibre and incidence of type 2 diabetes in eight European countries: The EPIC-InterAct Study and a meta-analysis of prospective studies. Diabetologia 2015, 58, 1394–1408. [Google Scholar] [CrossRef] [Green Version]
- Lairon, D.; Arnault, N.; Bertrais, S.; Planells, R.; Clero, E.; Hercberg, S.; Boutron-Ruault, M.C. Dietary fiber intake and risk factors for cardiovascular disease in French adults. Am. J. Clin. Nutr. 2005, 82, 1185–1194. [Google Scholar] [CrossRef] [Green Version]
- Mirmiran, P.; Bahadoran, Z.; Khalili Moghadam, S.; Zadeh Vakili, A.; Azizi, F. A Prospective study of different types of dietary fiber and risk of cardiovascular disease: Tehran lipid and glucose study. Nutrients 2016, 8, 686. [Google Scholar] [CrossRef] [Green Version]
- Du, H.; van der A, D.L.; Boshuizen, H.C.; Forouhi, N.G.; Wareham, N.J.; Halkjaer, J.; Tjønneland, A.; Overvad, K.; Jakobsen, M.U.; Boeing, H.; et al. Dietary fiber and subsequent changes in body weight and waist circumference in European men and women. Am. J. Clin. Nutr. 2010, 91, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Buil-Cosiales, P.; Zazpe, I.; Toledo, E.; Corella, D.; Salas-Salvadó, J.; Diez-Espino, J.; Ros, E.; Navajas, J.F.-N.; Santos-Lozano, J.M.; Arós, F.; et al. Fiber intake and all-cause mortality in the Prevención con Dieta Mediterránea (PREDIMED) study. Am. J. Clin. Nutr. 2014, 100, 1498–1507. [Google Scholar] [CrossRef]
- Xu, H.; Huang, X.; Risérus, U.; Krishnamurthy, V.M.; Cederholm, T.; Arnlöv, J.; Lindholm, B.; Sjögren, P.; Carrero, J.J. Dietary fiber, kidney function, inflammation, and mortality risk. Clin. J. Am. Soc. Nephrol. 2014, 9, 2104–2110. [Google Scholar] [CrossRef]
- Miller, S.J.; Batra, A.K.; Shearrer, G.E.; House, B.T.; Cook, L.T.; Pont, S.J.; Goran, M.I.; Davis, J.N. Dietary fibre linked to decreased inflammation in overweight minority youth. Pediatr. Obes. 2016, 11, 33–39. [Google Scholar] [CrossRef]
- Erkkilä, A.T.; Lichtenstein, A.H. Fiber and cardiovascular disease risk: How strong is the evidence? J. Cardiovasc. Nurs. 2006, 21, 3–8. [Google Scholar] [CrossRef]
- Partula, V.; Deschasaux, M.; Druesne-Pecollo, N.; Latino-Martel, P.; Desmetz, E.; Chazelas, E.; Kesse-Guyot, E.; Julia, C.; Fezeu, L.K.; Galan, P.; et al. Associations between consumption of dietary fibers and the risk of cardiovascular diseases, cancers, type 2 diabetes, and mortality in the prospective NutriNet-Santé cohort. Am. J. Clin. Nutr. 2020, 112, 195–207. [Google Scholar] [CrossRef]
- Threapleton, D.E.; Greenwood, D.C.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Cade, J.E.; Gale, C.P.; Burley, V.J. Dietary fibre intake and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2013, 347, f6879. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Zhao, L.G.; Wu, Q.J.; Ma, X.; Xiang, Y.B. Association between dietary fiber and lower risk of all-cause mortality: A meta-analysis of cohort studies. Am. J. Epidemiol. 2015, 181, 83–91. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Bes-Rastrollo, M.; Toledo, E.; Gea, A.; Fresán, U.; Barbagallo, M.; Martínez-González, M.A. Dietary fiber intake and mortality in a Mediterranean population: The “Seguimiento Universidad de Navarra” (SUN) project. Eur. J. Nutr. 2019, 58, 3009–3022. [Google Scholar] [CrossRef]
- Katagiri, R.; Goto, A.; Sawada, N.; Yamaji, T.; Iwasaki, M.; Noda, M.; Iso, H.; Tsugane, S. Dietary fiber intake and total and cause-specific mortality: The Japan Public Health Center-based prospective study. Am. J. Clin. Nutr. 2020, 111, 1027–1035. [Google Scholar] [CrossRef]
- Steffen, L.M.; Jacobs, D.R., Jr.; Stevens, J.; Shahar, E.; Carithers, T.; Folsom, A.R. Associations of whole-grain, refined-grain, and fruit and vegetable consumption with risks of all-cause mortality and incident coronary artery disease and ischemic stroke: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Clin. Nutr. 2003, 78, 383–390. [Google Scholar] [CrossRef]
- Popkin, B.M.; Du, S.; Zhai, F.; Zhang, B. Cohort profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2010, 39, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Zhai, F.Y.; Du, S.F.; Popkin, B.M. The China Health and Nutrition Survey, 1989–2011. Obes. Rev. 2014, 15, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Zhai, F.Y.; Du, S.F.; Wang, Z.H.; Zhang, J.G.; Du, W.W.; Popkin, B.M. Dynamics of the Chinese diet and the role of urbanicity, 1991–2011. Obes. Rev. 2014, 15, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.; Lee, K.; Rebholz, C.M.; Kim, J. Plant-based diets and incident metabolic syndrome: Results from a South Korean prospective cohort study. PLoS Med. 2020, 17, e1003371. [Google Scholar] [CrossRef]
- Yuan, X.; Liu, T.; Wu, L.; Zou, Z.Y.; Li, C. Validity of self-reported diabetes among middle-aged and older Chinese adults: The China health and retirement longitudinal study. BMJ Open 2015, 5, e006633. [Google Scholar] [CrossRef] [Green Version]
- China Nutrition Association. The Chinese Dietary Guidline 2022. Available online: http://dg.cnsoc.org/ (accessed on 23 April 2022).
- Kimura, Y.; Yoshida, D.; Hirakawa, Y.; Hata, J.; Honda, T.; Shibata, M.; Sakata, S.; Uchida, K.; Kitazono, T.; Ninomiya, T. Dietary fiber intake and risk of type 2 diabetes in a general Japanese population: The Hisayama Study. J. Diabetes Investig. 2021, 12, 527–536. [Google Scholar] [CrossRef]
- Witteman, J.C.; Willett, W.C.; Stampfer, M.J.; Colditz, G.A.; Sacks, F.M.; Speizer, F.E.; Rosner, B.; Hennekens, C.H. A prospective study of nutritional factors and hypertension among US women. Circulation 1989, 80, 1320–1327. [Google Scholar] [CrossRef] [Green Version]
- Ascherio, A.; Rimm, E.B.; Giovannucci, E.L.; Colditz, G.A.; Rosner, B.; Willett, W.C.; Sacks, F.; Stampfer, M.J. A prospective study of nutritional factors and hypertension among US men. Circulation 1992, 86, 1475–1484. [Google Scholar] [CrossRef] [Green Version]
- Du, P.; Luo, K.; Wang, Y.; Xiao, Q.; Xiao, J.; Li, Y.; Zhang, X. Intake of dietary fiber from grains and the risk of hypertension in late midlife women: Results from the SWAN study. Front. Nutr. 2021, 8, 730205. [Google Scholar] [CrossRef]
- Zhang, S.; Tian, J.; Lei, M.; Zhong, C.; Zhang, Y. Association between dietary fiber intake and atherosclerotic cardiovascular disease risk in adults: A cross-sectional study of 14,947 population based on the National Health and Nutrition Examination Surveys. BMC Public Health 2022, 22, 1076. [Google Scholar] [CrossRef]
- Liu, L.; Wang, S.; Liu, J. Fiber consumption and all-cause, cardiovascular, and cancer mortalities: A systematic review and meta-analysis of cohort studies. Mol. Nutr. Food Res. 2015, 59, 139–146. [Google Scholar] [CrossRef]
- Khan, K.; Jovanovski, E.; Ho, H.; Marques, A.; Zurbau, A.; Mejia, S.B.; Sievenpiper, J.L.; Vuksan, V. The effect of viscous soluble fiber on blood pressure: A systematic review and meta-analysis of randomized controlled trials. Nutr. Metab. Cardiovasc. Dis. NMCD. 2018, 28, 3–13. [Google Scholar] [CrossRef]
- Yao, B.; Fang, H.; Xu, W.; Yan, Y.; Xu, H.; Liu, Y.; Mo, M.; Zhang, H.; Zhao, Y. Dietary fiber intake and risk of type 2 diabetes: A dose-response analysis of prospective studies. Eur. J. Epidemiol. 2014, 29, 79–88. [Google Scholar] [CrossRef] [PubMed]
- Salmerón, J.; Ascherio, A.; Rimm, E.B.; Colditz, G.A.; Spiegelman, D.; Jenkins, D.J.; Stampfer, M.J.; Wing, A.L.; Willett, W.C. Dietary fiber, glycemic load, and risk of NIDDM in men. Diabetes Care 1997, 20, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Schulze, M.B.; Liu, S.; Rimm, E.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Glycemic index, glycemic load, and dietary fiber intake and incidence of type 2 diabetes in younger and middle-aged women. Am. J. Clin. Nutr. 2004, 80, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Koh-Banerjee, P.; Franz, M.; Sampson, L.; Liu, S.; Jacobs, D.R., Jr.; Spiegelman, D.; Willett, W.; Rimm, E. Changes in whole-grain, bran, and cereal fiber consumption in relation to 8-y weight gain among men. Am. J. Clin. Nutr. 2004, 80, 1237–1245. [Google Scholar] [CrossRef] [Green Version]
- Bakker, S.J.; Hoogeveen, E.K.; Nijpels, G.; Kostense, P.J.; Dekker, J.M.; Gans, R.O.; Heine, R.J. The association of dietary fibres with glucose tolerance is partly explained by concomitant intake of thiamine: The hoorn study. Diabetologia 1998, 41, 1168–1175. [Google Scholar] [CrossRef] [Green Version]
- Sun, B.; Shi, X.; Wang, T.; Zhang, D. Exploration of the association between dietary fiber intake and hypertension among U.S. adults using 2017 american college of cardiology/american heart association blood pressure guidelines: NHANES 2007–2014. Nutrients 2018, 10, 1091. [Google Scholar] [CrossRef] [Green Version]
- Kochar, J.; Gaziano, J.M.; Djoussé, L. Breakfast cereals and risk of hypertension in the Physicians’ Health Study I. Clin. Nutr. 2012, 31, 89–92. [Google Scholar] [CrossRef] [Green Version]
- Borgi, L.; Muraki, I.; Satija, A.; Willett, W.C.; Rimm, E.B.; Forman, J.P. Fruit and vegetable consumption and the incidence of hypertension in three prospective cohort studies. Hypertension 2016, 67, 288–293. [Google Scholar] [CrossRef] [Green Version]
- Masala, G.; Bendinelli, B.; Versari, D.; Saieva, C.; Ceroti, M.; Santagiuliana, F.; Caini, S.; Salvini, S.; Sera, F.; Taddei, S.; et al. Anthropometric and dietary determinants of blood pressure in over 7000 Mediterranean women: The European prospective investigation into cancer and nutrition-florence cohort. J. Hypertens. 2008, 26, 2112–2120. [Google Scholar] [CrossRef]
- Davy, B.M.; Melby, C.L.; Beske, S.D.; Ho, R.C.; Davrath, L.R.; Davy, K.P. Oat consumption does not affect resting casual and ambulatory 24-h arterial blood pressure in men with high-normal blood pressure to stage I hypertension. J. Nutr. 2002, 132, 394–398. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.W.; Tietyen-Clark, J. Dietary fiber: Hyperlipidemia, hypertension, and coronary heart disease. Am. J. Gastroenterol. 1986, 81, 907–919. [Google Scholar] [PubMed]
- Anderson, J.W.; Chen, W.J. Plant fiber. Carbohydrate and lipid metabolism. Am. J. Clin. Nutr. 1979, 32, 346–363. [Google Scholar] [CrossRef] [PubMed]
- Hamaker, B.R.; Tuncil, Y.E. A perspective on the complexity of dietary fiber structures and their potential effect on the gut microbiota. J. Mol. Biol. 2014, 426, 3838–3850. [Google Scholar] [CrossRef]
- Parnell, J.A.; Reimer, R.A. Prebiotic fiber modulation of the gut microbiota improves risk factors for obesity and the metabolic syndrome. Gut Microbes. 2012, 3, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, S.M. The interplay between fiber and the intestinal microbiome in the inflammatory response. Adv. Nutr. 2013, 4, 16–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, S.C.; Norat, T.; Murphy, N.; Olsen, A.; Tjønneland, A.; Overvad, K.; Boutron-Ruault, M.C.; Perquier, F.; Dartois, L.; Kaaks, R.; et al. Fiber intake and total and cause-specific mortality in the European Prospective Investigation into Cancer and Nutrition cohort. Am. J. Clin. Nutr. 2012, 96, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Ark, Y.; Subar, A.F.; Hollenbeck, A.; Schatzkin, A. Dietary fiber intake and mortality in the NIH-AARP diet and health study. Arch. Intern. Med. 2011, 171, 1061–1068. [Google Scholar]
- Jin, F.; Zhang, J.; Shu, L.; Han, W. Association of dietary fiber intake with newly-diagnosed type 2 diabetes mellitus in middle-aged Chinese population. Nutr. J. 2021, 20, 81. [Google Scholar] [CrossRef]
- Zhang, S.; Meng, G.; Zhang, Q.; Liu, L.; Yao, Z.; Wu, H.; Gu, Y.; Wang, Y.; Zhang, T.; Wang, X.; et al. Dietary fiber intake and risk of prediabetes in China: Results from the TCLSIH Cohort Study. Br. J. Nutr. 2021, 1–20. [Google Scholar] [CrossRef]
- Kim, H.; Rebholz, C.M.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Caulfield, L.E. Operational differences in plant-based diet indices affect the ability to detect associations with incident hypertension in middle-aged US adults. J. Nutr. 2020, 150, 842–850. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Fiber Intake (g/d) | p | |||
|---|---|---|---|---|---|
| Quartile 1 (<6.21) | Quartile 2 (6.21–8.81) | Quartile 3 (8.81–13.50) | Quartile 4 (>13.50) | ||
| Number | 1611 | 1718 | 1799 | 1778 | |
| Age (years) | 47.62 ± 14.89 | 46.93 ± 13.71 | 47.44 ± 13.41 | 47.77 ± 13.34 | 0.307 |
| Male, n (%) | 667 (42.14) | 797 (46.69) | 865 (49.01) | 931 (52.57) | <0.001 |
| BMI (kg/m2) | 22.97 ± 3.33 | 23.04 ± 3.41 | 23.25 ± 3.28 | 23.10 ± 3.29 | 0.097 |
| Waist circumference (cm) | 80.04 ± 9.98 | 80.44 ± 9.85 | 81.34 ± 9.78 | 81.32 ± 9.58 | 0.001 |
| Systolic blood pressure (mmHg) | 122.46 ± 17.89 | 121.43 ± 17.35 | 121.97 ± 18.70 | 121.04 ± 17.29 | 0.136 |
| Diastolic blood pressure (mmHg) | 79.24 ± 10.79 | 78.58 ± 10.47 | 78.57 ± 11.94 | 78.11 ± 10.92 | 0.048 |
| Physical activity (MET-MIN/day) | 274.28 (0.00–1531.29) | 978.96 (0.00–1992.86) | 993.01 (0.00–2090.14) | 1079.04 (0.00–2220.01) | <0.001 |
| Smoking, n (%) | |||||
| Yes | 461 (29.21) | 555 (32.44) | 613 (34.61) | 628 (35.44) | 0.006 |
| No | 1117 (70.79) | 1156 (67.56) | 1158 (65.39) | 1144 (64.56) | |
| Alcohol drinking, n (%) | |||||
| Yes | 444 (28.14) | 555 (32.44) | 638 (36.09) | 649 (36.60) | <0.001 |
| No | 1134 (71.86 | 1156 (67.56) | 1130 (63.91) | 1124 (63.40) | |
| Educational level, n (%) | 0.004 | ||||
| Primary school or below | 699 (44.16) | 768 (44.99) | 835 (47.34) | 916 (51.72) | |
| Junior high school | 497 (31.40) | 558 (32.69) | 571 (32.37) | 515 (29.08) | |
| Senior high school | 237 (14.97) | 229 (13.42) | 214 (12.13) | 211 (11.91) | |
| College and above | 150 (9.48) | 152 (8.90) | 144 (8.16) | 129 (7.28) | |
| Regions, n (%) | |||||
| Urban | 600 (37.24) | 535 (31.14) | 531 (29.85) | 444 (24.97) | <0.001 |
| Rural | 1011 (62.76) | 1183 (68.86) | 1248 (70.15) | 1334 (75.03) | |
| Total energy intake (kcal/day) | 1869.11 ± 547.14 | 2115.88 ± 550.74 | 2280.64 ± 576.40 | 2479.94 ± 598.07 | <0.001 |
| Total carbohydrate intake (g/d) | 263.19 ± 79.91 | 311.06 ± 85.94 | 338.77 ± 100.03 | 378.01 ± 108.77 | <0.001 |
| Total protein intake (g/d) | 55.26 ± 18.97 | 62.11 ± 19.08 | 69.03 ± 20.59 | 76.46 ± 25.01 | <0.001 |
| Total fatty intake (g/d) | 63.99 ± 35.09 | 66.95 ± 35.87 | 68.67 ± 35.74 | 70.90 ± 37.45 | <0.001 |
| Na intake (mg/d) | 60.91 (14.41–485.21) | 52.81 (16.20–829.61) | 60.60 (16.63–1130.85) | 49.61 (16.74–850.52) | <0.001 |
| Whole-grain fiber intake (g/d) | 0.37 ± 0.79 | 0.72 ± 1.26 | 1.18 ± 1.99 | 2.58 ± 5.49 | <0.001 |
| Legume fiber intake (g/d) | 0.11 ± 0.32 | 0.33 ± 0.74 | 0.76 ± 1.53 | 2.56 ± 5.52 | <0.001 |
| Vegetable fiber intake (g/d) | 2.01 ± 0.96 | 3.37 ± 1.32 | 4.82 ± 2.36 | 10.86 ± 9.53 | <0.001 |
| Fruit fiber intake (g/d) | 0.10 ± 0.33 | 0.21 ± 0.59 | 0.37 ± 0.93 | 0.48 ± 1.37 | <0.001 |
| Total Fiber Intake | |||||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Trend | |
| T2D | |||||
| Number of cases | 132 | 166 | 174 | 178 | |
| Person-years | 16,902 | 17,888 | 18,545 | 18,515 | |
| Incidence density (1000 person-years) | 7.81 | 9.28 | 9.38 | 9.61 | |
| T2D a | 1.0 | 1.18 (0.94, 1.48) | 1.19 (0.95, 1.50) | 1.22 (0.97, 1.53) | 0.12 |
| T2D b | 1.0 | 1.12 (0.88, 1.43) | 1.13 (0.88, 1.44) | 1.20 (0.93, 1.55) | 0.08 |
| Hypertension | |||||
| Number of cases | 270 | 297 | 307 | 304 | |
| Person-years | 9241 | 10,116 | 10,667 | 10,552 | |
| Incidence density (1000 person-years) | 29.21 | 29.35 | 28.78 | 28.81 | |
| Hypertension a | 1.0 | 1.01 (0.86, 1.19) | 0.99 (0.84, 1.17) | 0.99 (0.84, 1.17) | 0.63 |
| Hypertension c | 1.0 | 0.98 (0.82, 1.18) | 0.86 (0.71, 1.04) | 0.91 (0.75, 1.12) | 0.25 |
| Obesity | |||||
| Number of cases | 75 | 98 | 109 | 97 | |
| Person-years | 10,087 | 11,308 | 12,089 | 11,781 | |
| Incidence density (1000 person-years) | 7.43 | 8.67 | 9.01 | 8.23 | |
| Obesity a | 1.0 | 1.17 (0.86, 1.57) | 1.21 (0.90, 1.63) | 1.11 (0.82, 1.50) | 0.14 |
| Obesity c | 1.0 | 1.09 (0.78, 1.52) | 1.02 (0.73, 1.44) | 0.93 (0.64, 1.35) | 0.40 |
| CVD | |||||
| Number of cases | 22 | 38 | 35 | 32 | |
| Person-years | 12,276 | 15,363 | 14,124 | 14,289 | |
| Incidence density (1000 person-years) | 1.79 | 2.47 | 2.48 | 2.23 | |
| CVD a | 1.0 | 1.56 (0.93, 2.64) | 1.38 (0.81, 2.36) | 1.25 (0.73, 2.15) | 0.34 |
| CVD c | 1.0 | 1.56 (0.90, 2.70) | 1.24 (0.70, 2.23) | 1.13 (0.60, 2.12) | 0.07 |
| All-cause mortality | |||||
| Number of cases | 133 | 105 | 101 | 129 | |
| Person-years | 21,571 | 22,398 | 22,663 | 22,543 | |
| Incidence density (1000 person-year) | 6.16 | 4.68 | 4.45 | 5.72 | |
| All-cause mortality a | 1.0 | 0.76 (0.59, 0.98) | 0.72 (0.56, 0.94) | 0.93 (0.73, 1.18) | 0.11 |
| All-cause mortality c | 1.0 | 1.05 (0.79, 1.38) | 0.95 (0.70, 1.27) | 1.13 (0.84, 1.52) | 0.14 |
| Whole-Grain Fiber | ||||
|---|---|---|---|---|
| Tercile 1 | Tercile 2 | Tercile 3 | p-Trend | |
| T2D a | 1.00 | 1.33 (1.11, 1.62) | 1.31 (1.09, 1.57) | 0.06 |
| T2D b1 | 1.00 | 1.16 (0.94, 1.43) | 1.16 (0.96, 1.41) | 0.12 |
| Hypertension a | 1.00 | 1.13 (0.96, 1.31) | 1.29 (1.13, 1.47) | 0.04 |
| Hypertension c1 | 1.00 | 1.05 (0.88, 1.25) | 1.21 (1.04, 1.40) | 0.03 |
| Obesity a | 1.00 | 1.67 (1.29, 2.15) | 1.62 (1.28, 2.05) | 0.73 |
| Obesity c1 | 1.00 | 1.23 (0.91, 1.65) | 1.27 (0.98, 1.65) | 0.55 |
| CVD a | 1.00 | 1.04 (0.64, 1.70) | 1.43 (0.97, 2.12) | 0.16 |
| CVD c1 | 1.00 | 0.94 (0.56, 1.59) | 1.29 (0.85, 1.96) | 0.52 |
| All-cause mortality a | 1.00 | 0.83 (0.65, 1.06) | 0.87 (0.69, 1.08) | 0.14 |
| All-cause mortality c1 | 1.00 | 0.98 (0.75, 1.28) | 0.95 (0.75, 1.20) | 0.09 |
| Legume Fiber | ||||
|---|---|---|---|---|
| Tercile 1 | Tercile 2 | Tercile 3 | p-Trend | |
| T2D a | 1.00 | 1.15 (0.92, 1.43) | 1.12 (0.93, 1.33) | 0.43 |
| T2D b2 | 1.00 | 1.09 (0.87, 1.38) | 0.97 (0.79, 1.19) | 0.24 |
| Hypertension a | 1.00 | 0.95 (0.79, 1.15) | 1.07 (0.94, 1.22) | 0.37 |
| Hypertension c2 | 1.00 | 1.01 (0.82, 1.24) | 0.97 (0.83, 1.13) | 0.16 |
| Obesity a | 1.00 | 0.84 (0.59, 1.20) | 1.06 (0.84, 1.33) | 0.20 |
| Obesity c2 | 1.00 | 0.84 (0.57, 1.25) | 0.92 (0.70, 1.21) | 0.08 |
| CVD a | 1.00 | 1.06 (0.63, 1.76) | 1.06 (0.70, 1.60) | 0.12 |
| CVD c2 | 1.00 | 1.09 (0.64, 1.85) | 0.90 (0.56, 1.46) | 0.67 |
| All-cause mortality a | 1.00 | 0.91 (0.70, 1.20) | 0.86 (0.69, 1.07) | 0.19 |
| All-cause mortality c2 | 1.00 | 1.07 (0.81, 1.42) | 1.04 (0.80, 1.33) | 0.46 |
| Vegetable Fiber | |||||
|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | p-Trend | |
| T2D a | 1.00 | 0.85 (0.68, 1.06) | 0.97 (0.79, 1.20) | 0.85 (0.68, 1.06) | 0.24 |
| T2D b3 | 1.00 | 0.83 (0.66, 1.05) | 0.97 (0.77, 1.21) | 0.89 (0.70, 1.12) | 0.34 |
| Hypertension a | 1.00 | 0.93 (0.79, 1.09) | 0.92 (0.78, 1.08) | 0.90 (0.77, 1.06) | 0.18 |
| Hypertension c3 | 1.00 | 1.01 (0.85, 1.20) | 0.96 (0.81, 1.15) | 0.96 (0.80, 1.15) | 0.12 |
| Obesity a | 1.00 | 0.72 (0.54, 0.96) | 0.84 (0.64, 1.10) | 0.72 (0.54, 0.96) | 0.46 |
| Obesity c3 | 1.00 | 0.78 (0.57, 1.08) | 0.87 (0.64, 1.19) | 0.75 (0.54, 1.03) | 0.71 |
| CVD a | 1.00 | 0.72 (0.43, 1.18) | 0.83 (0.51, 1.33) | 0.85 (0.53, 1.36) | 0.19 |
| CVD c3 | 1.00 | 0.70 (0.41, 1.18) | 0.75 (0.45, 1.26) | 0.77 (0.46, 1.29) | 0.83 |
| All-cause mortality a | 1.00 | 0.97 (0.75, 1.25) | 0.88 (0.67, 1.14) | 1.14 (0.89, 1.46) | 0.16 |
| All-cause mortality c3 | 1.00 | 1.01 (0.77, 1.34) | 1.14 (0.85, 1.51) | 1.19 (0.91, 1.56) | 0.47 |
| Fruit Fiber | ||
|---|---|---|
| No Intake Group | Intake Group | |
| T2D a | 1.00 | 0.98 (0.80, 1.20) |
| T2D b4 | 1.00 | 0.90 (0.72, 1.12) |
| Hypertension a | 1.00 | 0.86 (0.73, 1.02) |
| Hypertension c4 | 1.00 | 0.94 (0.78, 1.13) |
| Obesity a | 1.00 | 1.01 (0.77, 1.33) |
| Obesity c4 | 1.00 | 0.87 (0.64, 1.19) |
| CVD a | 1.00 | 0.89 (0.55, 1.46) |
| CVD c4 | 1.00 | 0.91 (0.53, 1.54) |
| All-cause mortality a | 1.00 | 0.58 (0.44, 0.77) |
| All-cause mortality c4 | 1.00 | 0.83 (0.61, 1.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Chen, B.; Zeng, J.; Fan, M.; Xu, W.; Li, X.; Xing, Y.; Xu, S. Associations between Consumption of Dietary Fibers and the Risk of Type 2 Diabetes, Hypertension, Obesity, Cardiovascular Diseases, and Mortality in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey. Nutrients 2022, 14, 2650. https://doi.org/10.3390/nu14132650
Zhang Z, Chen B, Zeng J, Fan M, Xu W, Li X, Xing Y, Xu S. Associations between Consumption of Dietary Fibers and the Risk of Type 2 Diabetes, Hypertension, Obesity, Cardiovascular Diseases, and Mortality in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey. Nutrients. 2022; 14(13):2650. https://doi.org/10.3390/nu14132650
Chicago/Turabian StyleZhang, Zhaoxia, Bo Chen, Jingjing Zeng, Menglin Fan, Wenlei Xu, Xiaying Li, Ying Xing, and Shaoyong Xu. 2022. "Associations between Consumption of Dietary Fibers and the Risk of Type 2 Diabetes, Hypertension, Obesity, Cardiovascular Diseases, and Mortality in Chinese Adults: Longitudinal Analyses from the China Health and Nutrition Survey" Nutrients 14, no. 13: 2650. https://doi.org/10.3390/nu14132650