
Burden of HPV-Related Hospitalization in Germany from 2000 to 2021

Abstract
:1. Introduction
2. Patients and Methods
3. Results
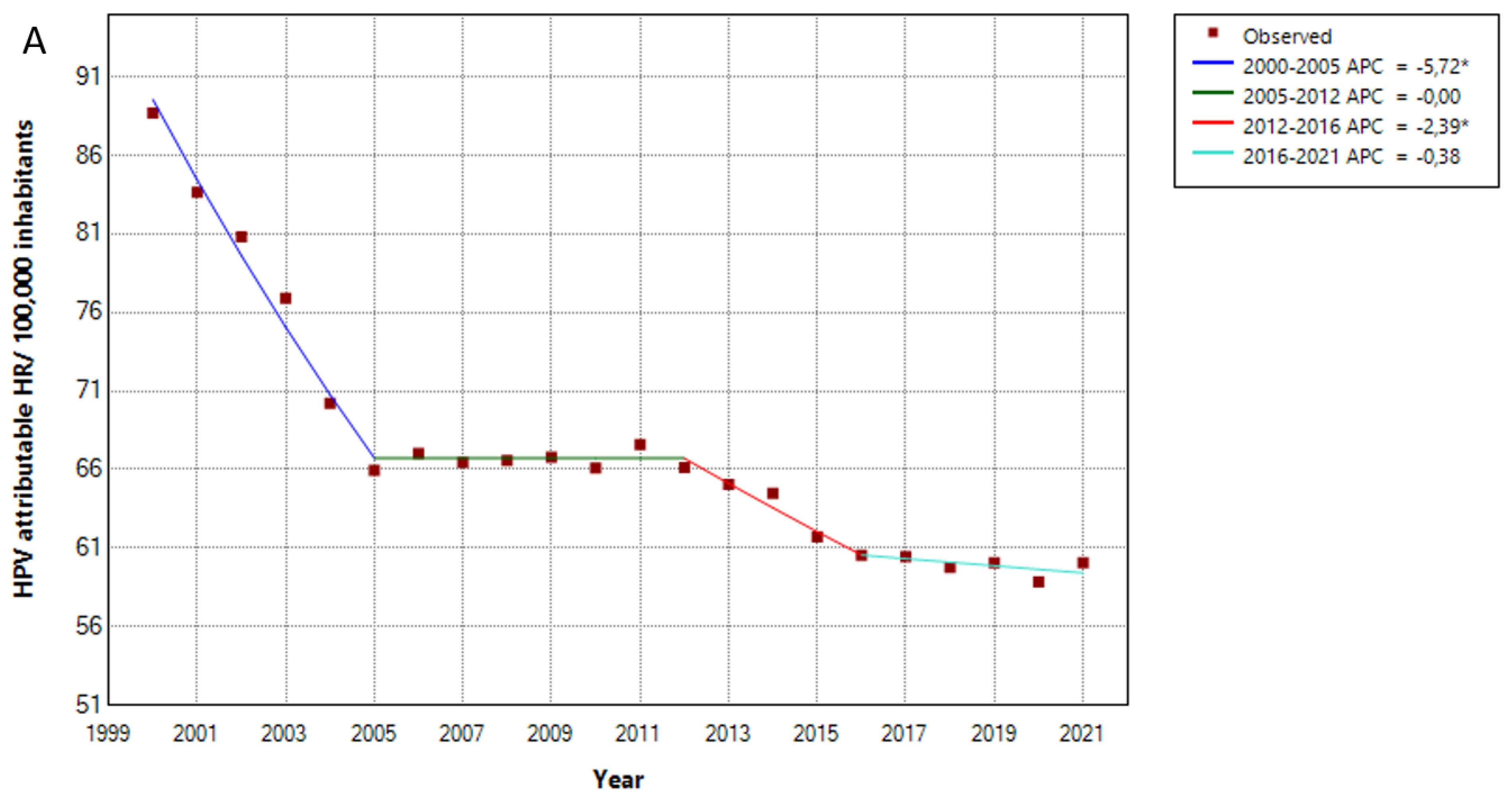
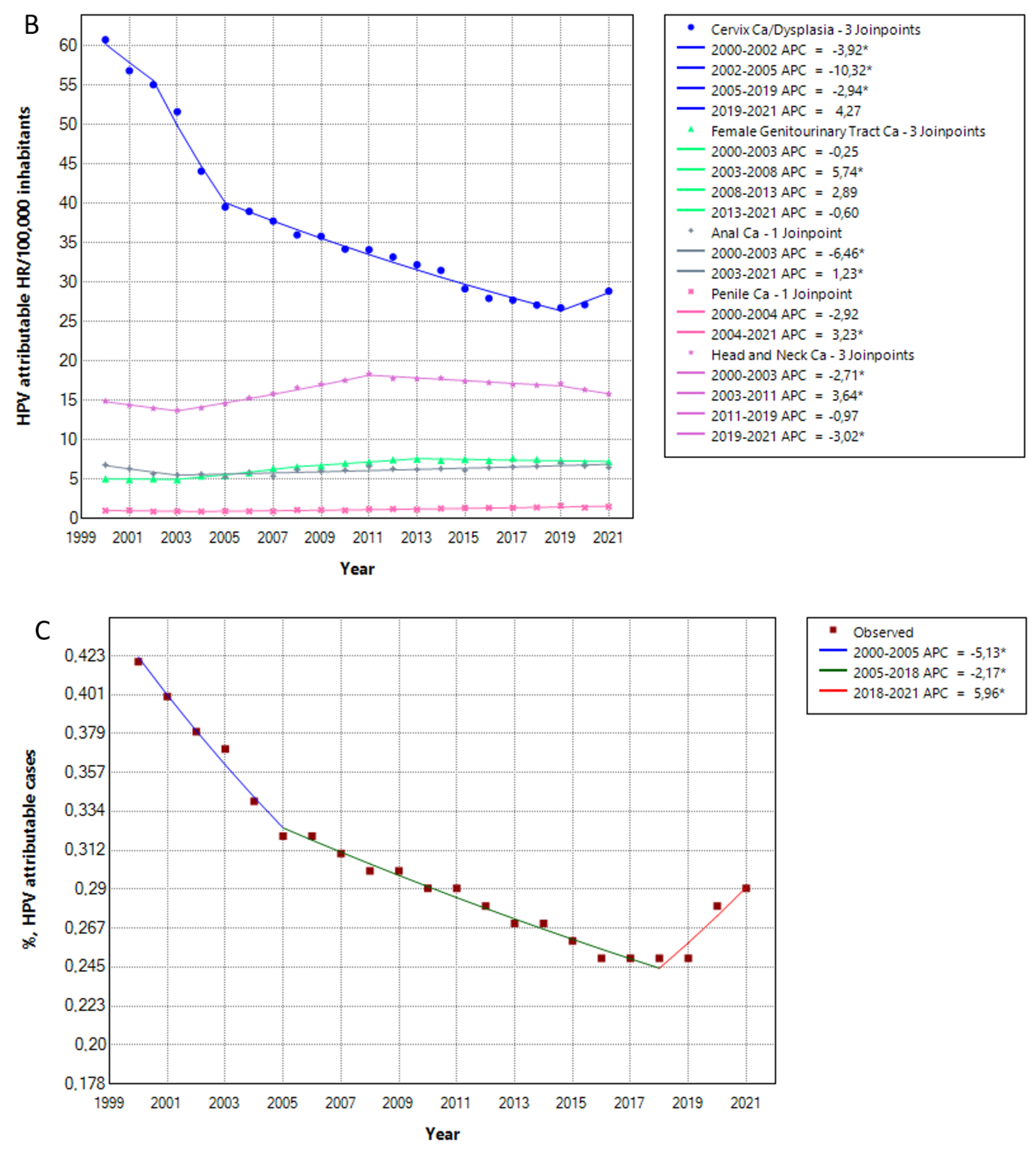
3.1. The Hospitalization Rate of HPV Attributable Diseases Has Decreased over Time
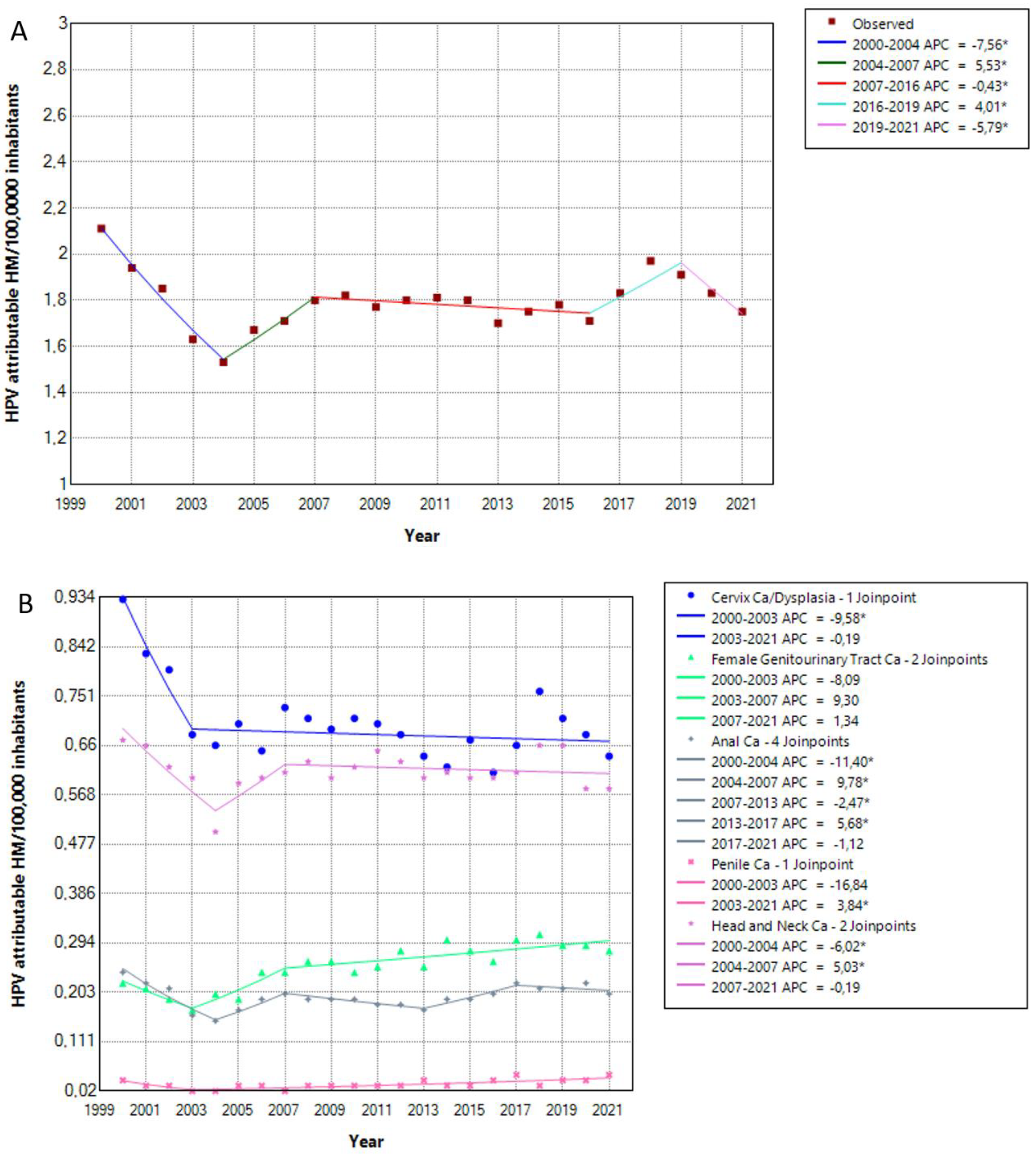
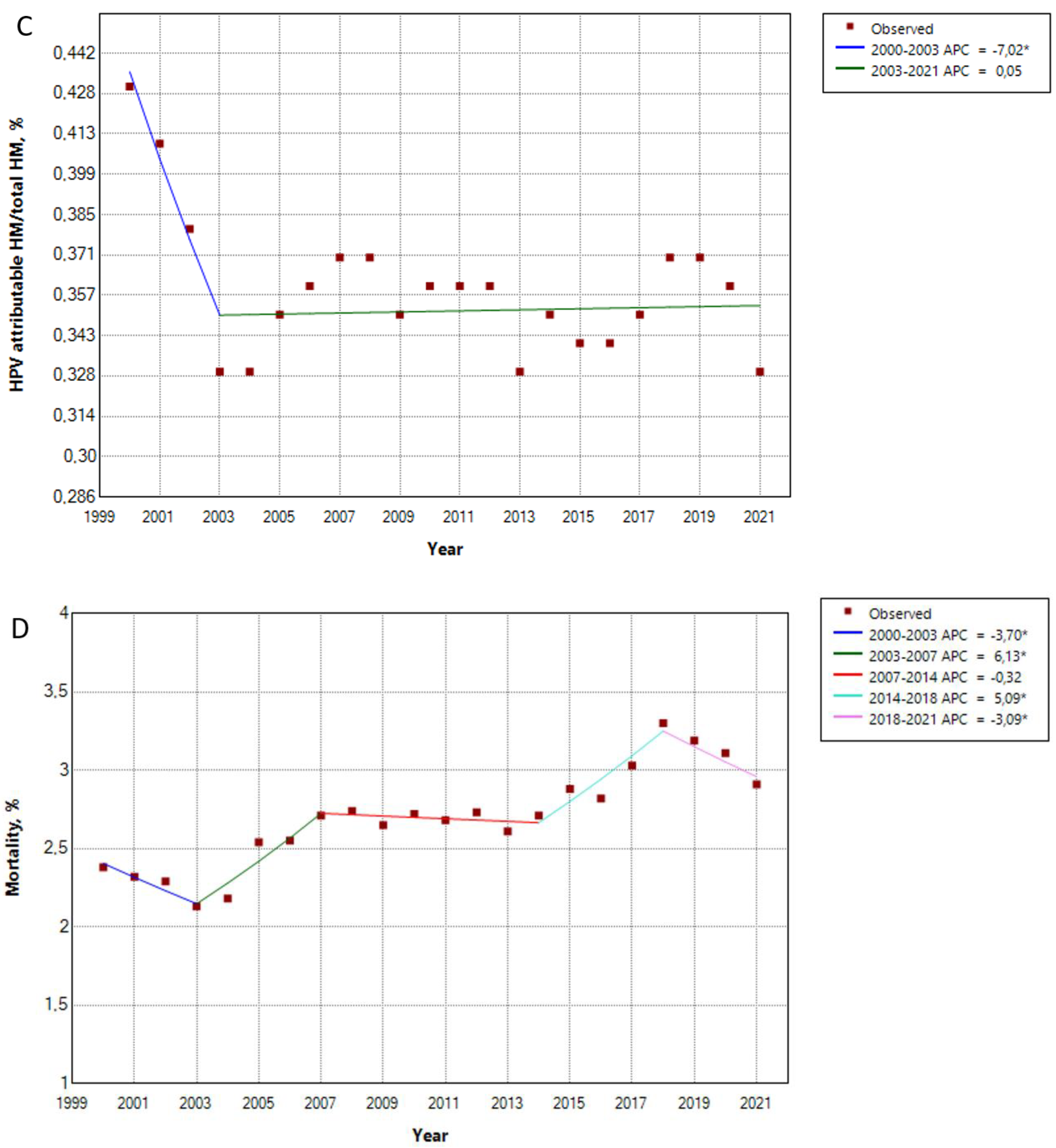
3.2. Inpatient Death Rates for HPV Attributable Diseases Undulate over Time
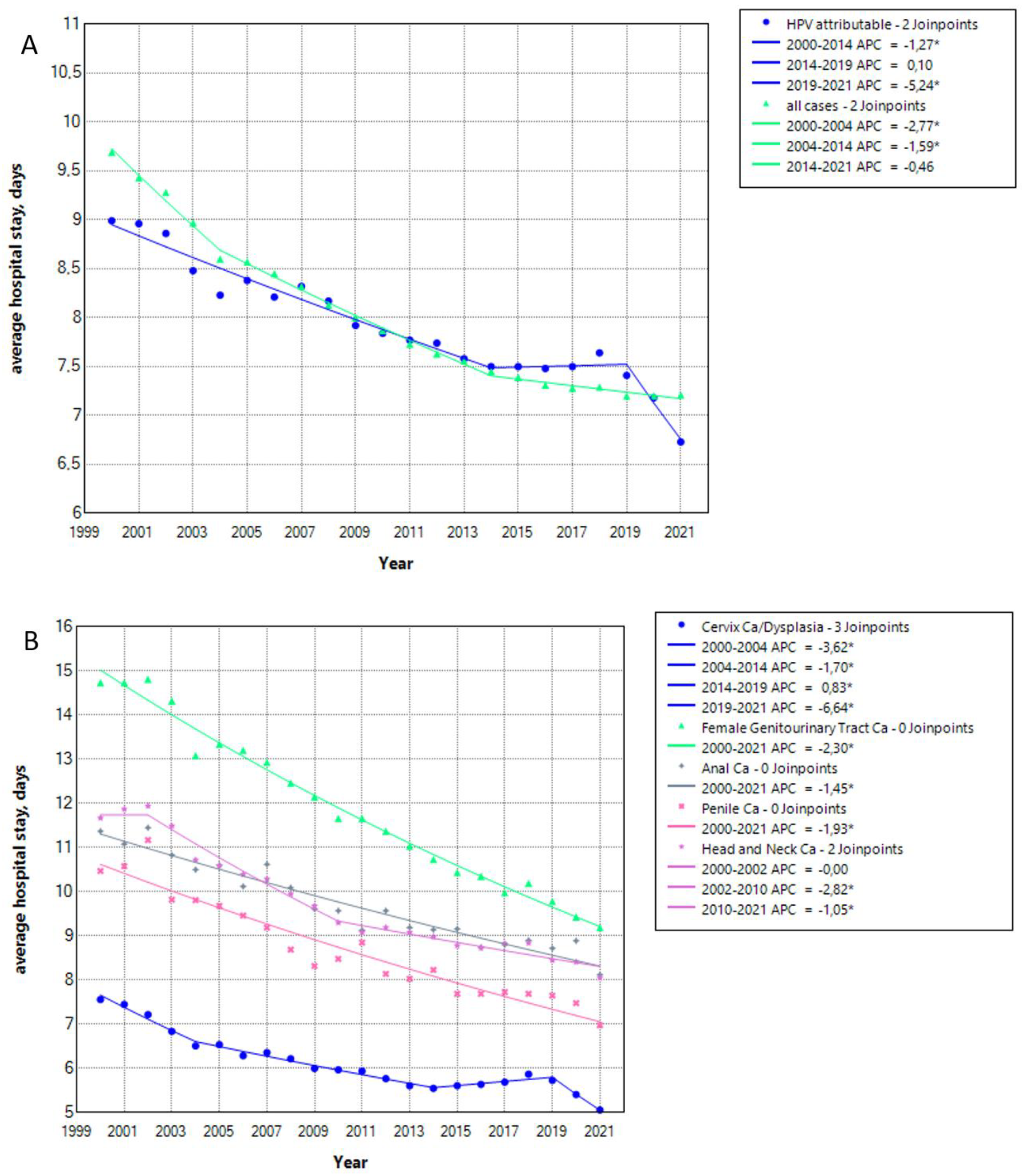
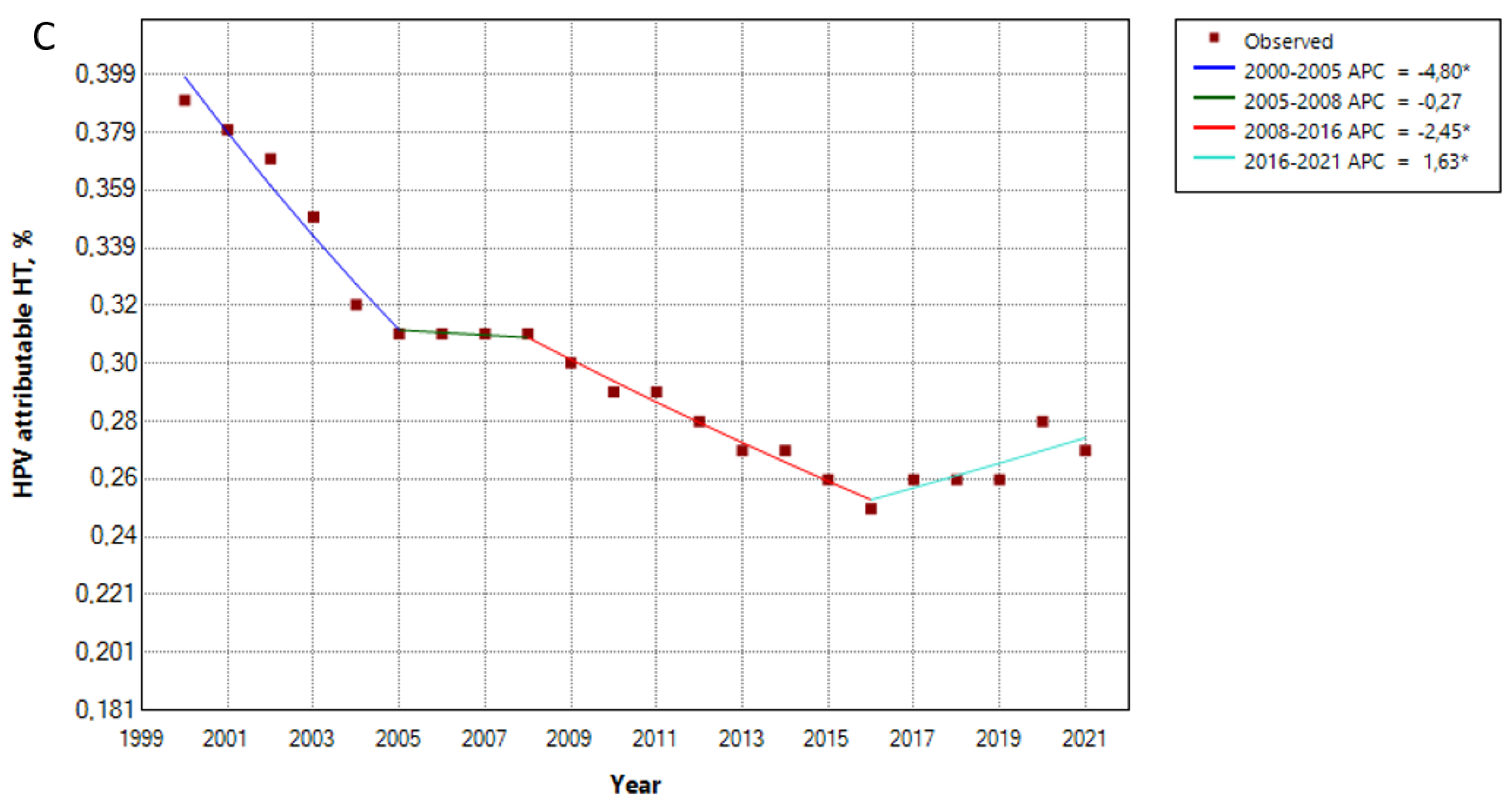
3.3. The Average Hospital Stay for HPV Attributable Cases Decreased over Time
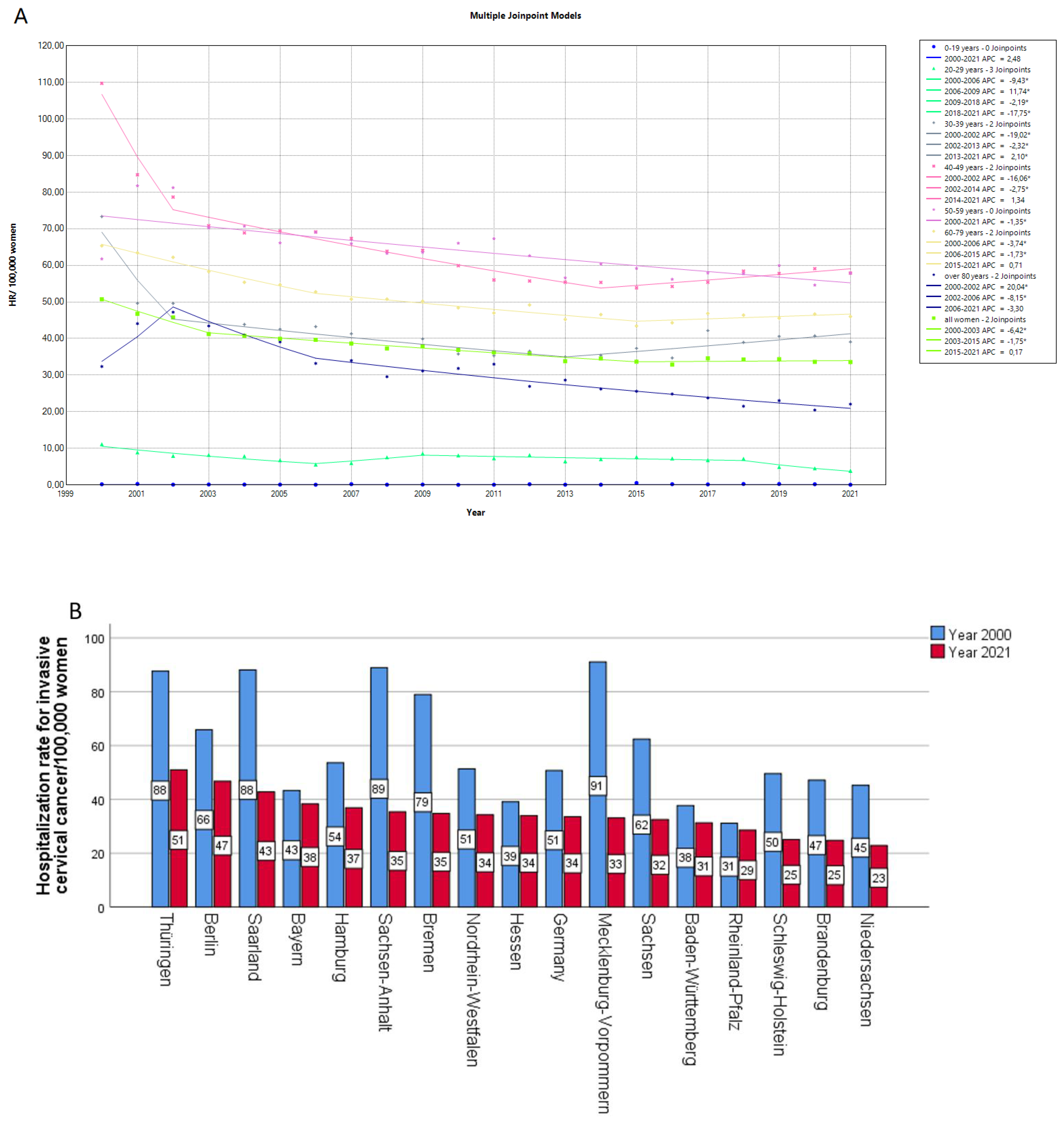
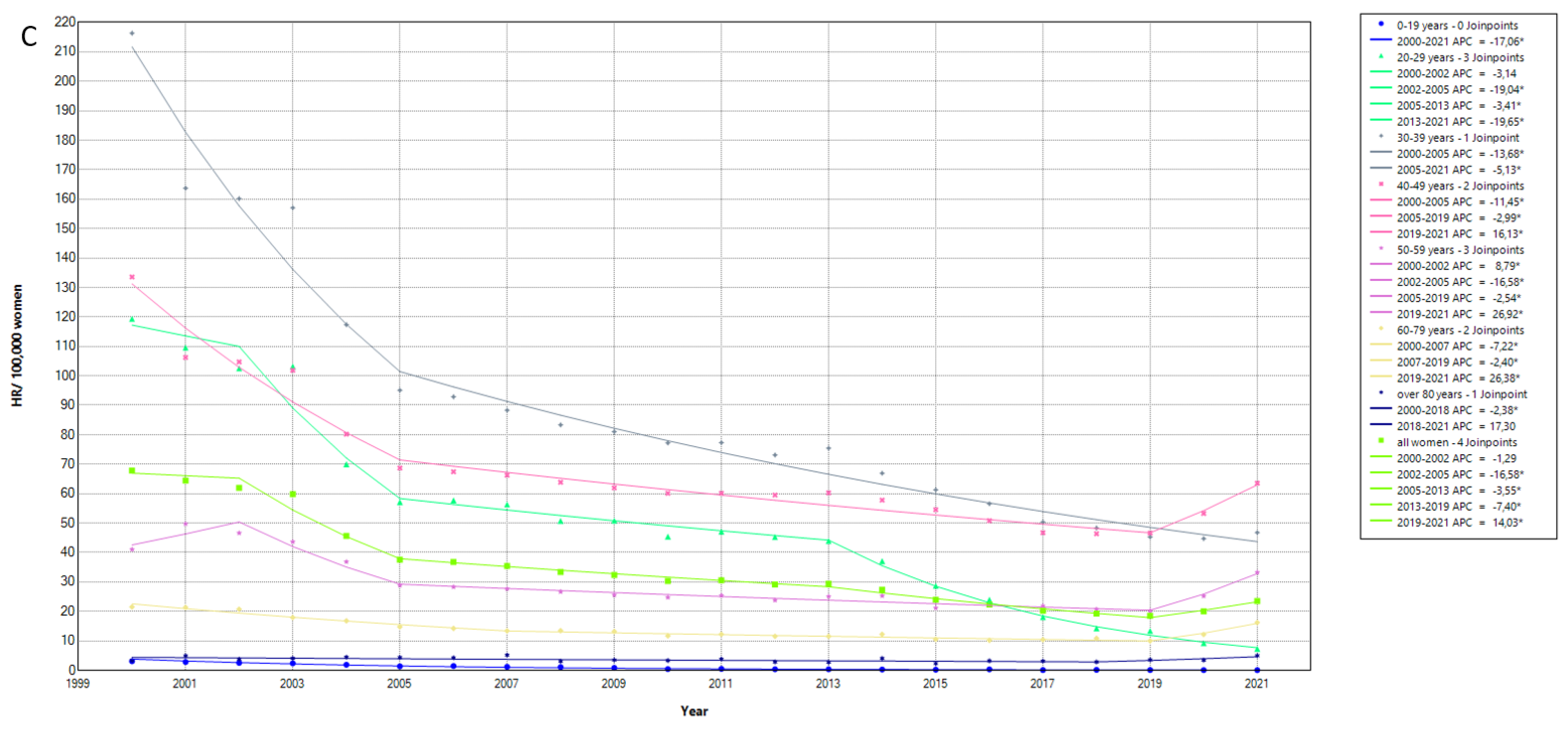
3.4. Cervical Cancer Hospitalization Rates Have Decreased over Time but to a Different Degree in Different Federal States
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- IARC. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 100 B. A Review of Human Carcinogens: Biological Agents; IARC: Lyon, France, 2012; Volume 100, Pt B, pp. 1–441. [Google Scholar]
- RKI, Human Papillomviren. Available online: https://www.ecdc.europa.eu/en/human-papillomavirus (accessed on 8 August 2023).
- WHO, Human Papillomavirus (HPV). Available online: https://www.who.int/news-room/fact-sheets/detail/human-papilloma-virus-and-cancer (accessed on 8 August 2023).
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global burden of cancers attributable to infections in 2012: A synthetic analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA. Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Deleré, Y.; Remschmidt, C.; Leuschner, J.; Schuster, M.; Fesenfeld, M.; Schneider, A.; Wichmann, O.; Kaufmann, A.M. Human Papillomavirus prevalence and probable first effects of vaccination in 20 to 25 year-old women in Germany: A population-based cross-sectional study via home-based self-sampling. BMC. Infect. Dis. 2014, 14, 87. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; Sanjosé, S. ICO/IARC Information Centre on HPV and Cancer. Human Papillomavirus and Related Diseases in Germany. Summary Report 10 March 2023. Available online: https://hpvcentre.net/statistics/reports/DEU.pdf (accessed on 1 August 2023).
- Deleré, Y.; Meyer, C.; Reiter, S. Universal immunisation with human papillomavirus (HPV) vaccine among females aged 12–17 recommended in Germany. Euro. Surveill. 2007, 12, E070405.2. [Google Scholar] [CrossRef] [PubMed]
- Reuschenbach, M.; Mihm, S.; Wölle, R.; Schneider, K.M.; Jacob, C.; Braun, S.; Greiner, W.; Hampl, M. Burden of HPV related anogenital diseases in young women in Germany—An analysis of German statutory health insurance claims data from 2012 to 2017. BMC. Infect. Dis. 2020, 20, 297. [Google Scholar] [CrossRef]
- Statistisches Bundesamt Deutschland. Available online: https://www-genesis.destatis.de/genesis/online (accessed on 12 July 2023).
- Giuliano, A.R.; Nyitray, A.G.; Kreimer, A.R.; Pierce Campbell, C.M.; Goodman, M.T.; Sudenga, S.L.; Monsonego, J.; Franceschi, S. EUROGIN 2014 roadmap: Differences in human papillomavirus infection natural history, transmission and human papillomavirus-related cancer incidence by gender and anatomic site of infection. Int. J. Cancer 2015, 136, 2752–2760. [Google Scholar] [CrossRef]
- Kreimer, A.R.; Clifford, G.M.; Boyle, P.; Franceschi, S. Human Papillomavirus Types in Head and Neck Squamous Cell Carcinomas Worldwide: A Systematic Review. Cancer Epidemiology. Biomark. Prev. 2005, 14, 467–475. [Google Scholar] [CrossRef]
- Kuhdari, P.; Previato, S.; Giordani, M.; Biavati, P.; Ferretti, S.; Gabutti, G. The burden of HPV-related diseases in Italy, 2001–2012. J. Public Health 2017, 39, 730–737. [Google Scholar] [CrossRef]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Joinpoint Regression Program, Version 5.0.2—May 2023; Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 15 June 2023).
- Restivo, V.; Minutolo, G.; Maranto, M.; Maiorana, A.; Vitale, F.; Casuccio, A.; Amodio, E. Impact of Preventive Strategies on HPV-Related Diseases: Ten-Year Data from the Italian Hospital Admission Registry. Cancers 2023, 15, 1452. [Google Scholar] [CrossRef] [PubMed]
- Restivo, V.; Costantino, C.; Amato, L.; Candiloro, S.; Casuccio, A.; Maranto, M.; Marrella, A.; Palmeri, S.; Pizzo, S.; Vitale, F.; et al. Evaluation of the Burden of HPV-Related Hospitalizations as a Useful Tool to Increase Awareness: 2007–2017 Data from the Sicilian Hospital Discharge Records. Vaccines 2020, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Baldo, V.; Cocchio, S.; Buja, A.; Baldovin, T.; Furlan, P.; Bertoncello, C.; Saia, M. Hospitalization for diseases attributable to human papillomavirus in the Veneto Region (North-East Italy). BMC Infect. Dis. 2013, 13, 462. [Google Scholar] [CrossRef] [PubMed]
- López, N.; Gil-de-Miguel, Á.; Pascual-García, R.; Gil-Prieto, R. Reduction in the burden of hospital admissions due to cervical disease from 2003-2014 in Spain. Hum. Vaccin. Immunother. 2018, 14, 917–923. [Google Scholar] [CrossRef]
- Gil-Prieto, R.; Ester, P.V.; Álvaro-Meca, A.; Rodríguez, M.S.; De Miguel, Á.G. The burden of hospitalizations for anus and penis neoplasm in Spain (1997–2008). Hum. Vaccines Immunother. 2012, 8, 201–207. [Google Scholar] [CrossRef]
- Di Martino, G.; Cedrone, F.; Di Giovanni, P.; Tognaccini, L.; Trebbi, E.; Romano, F.; Staniscia, T. The Burden of HPV-Related Hospitalizations: Analysis of Hospital Discharge Records from the Years 2015–2021 from a Southern Italian Region. Pathogens 2023, 12, 725. [Google Scholar]
- Fu, L.; Tian, T.; Yao, K.; Chen, X.F.; Luo, G.; Gao, Y.; Lin, Y.F.; Wang, B.; Sun, Y.; Zheng, W.; et al. Global Pattern and Trends in Penile Cancer Incidence: Population-Based Study. JMIR Public Health Surveill. 2022, 8, e34874. [Google Scholar] [CrossRef]
- Yang, M.; Du, J.; Lu, H.; Xiang, F.; Mei, H.; Xiao, H. Global trends and age-specific incidence and mortality of cervical cancer from 1990 to 2019: An international comparative study based on the Global Burden of Disease. BMJ Open 2022, 12, e055470. [Google Scholar] [CrossRef]
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001-2015. J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef]
- Damgacioglu, H.; Sonawane, K.; Zhu, Y.; Li, R.; Balasubramanian, B.A.; Lairson, D.R.; Giuliano, A.R.; Deshmukh, A.A. Oropharyngeal Cancer Incidence and Mortality Trends in All 50 States in the US, 2001-2017. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 155–165. [Google Scholar] [CrossRef]
- Deng, X.; Liu, Y.; Zhan, X.; Chen, T.; Jiang, M.; Jiang, X.; Chen, L.; Fu, B. Trends in Incidence, Mortality, and Survival of Penile Cancer in the United States: A Population-Based Study. Front. Oncol. 2022, 12, 891623. [Google Scholar] [CrossRef] [PubMed]
- Piechocki, M.; Koziołek, W.; Sroka, D.; Matrejek, A.; Miziołek, P.; Saiuk, N.; Sledzik, M.; Jaworska, A.; Bereza, K.; Pluta, E.; et al. Trends in Incidence and Mortality of Gynecological and Breast Cancers in Poland (1980–2018). Clin. Epidemiol. 2022, 14, 95–114. [Google Scholar] [CrossRef] [PubMed]
- S3-Leitlinie Analkarzinom. Diagnostik, Therapie und Nachsorge von Analkanal und Analrandkarzinomen. Langversion 1.2-Dezember 2020. AWMF-Registernummer: 081/004OL. Available online: https://register.awmf.org/assets/guidelines/081-004OLl_Analkarzinom_Diagnostik-Therapie-Nachsorge-Analkanalkarzinom-Analrandkarzinom_2020-12.pdf (accessed on 28 August 2023).
- S3-Leitlinie Diagnostik. Therapie und Nachsorge des Peniskarzinoms. Version 1.0-August 2020. AWMF-Registernummer: 043-042OL. Available online: https://register.awmf.org/assets/guidelines/043-042OLl_S3_Peniskarzinom_2020-08.pdf (accessed on 28 August 2023).
- Fink, D.; Ghisu, G.P. Das Screening auf Zervix-, Vulva- und Analkarzinom. Schweizer Zeitschrift für Gynäkologie, 06.03.2020. Available online: https://www.rosenfluh.ch/media/gynaekologie/2020/01/Das-Screening-auf-Zervix-Vulva-und-Analkarzinom.pdf (accessed on 28 August 2023).
- Buttmann-Schweiger, N.; Klug, S.J.; Luyten, A.; Holleczek, B.; Heitz, F.; du Bois, A.; Kraywinkel, K. Incidence patterns and temporal trends of invasive nonmelanotic vulvar tumors in Germany 1999–2011. A population-based cancer registry analysis. PLoS ONE 2015, 10, e0128073. [Google Scholar] [CrossRef]
- Wilking, H.; Thamm, M.; Stark, K.; Aebischer, T.; Seeber, F. Prevalence, incidence estimations and risk factors of Toxoplasma gondii infection in Germany: A representative, cross-sectional, serological study. Sci. Rep. 2016, 6, 22551. [Google Scholar] [CrossRef]
- Reinhold, T.; Thierfelder, K.; Müller-Riemenschneider, F.; Willich, S.N. Health economic effects after DRG-implementation—A systematic overview. Gesundheitswesen 2009, 71, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Horn, J.; Damm, O.; Kretzschmar, M.E.; Deleré, Y.; Wichmann, O.; Kaufmann, A.M.; Garbe, E.; Krämer, A.; Greiner, W.; Mikolajczyk, R.T. Estimating the long-term effects of HPV vaccination in Germany. Vaccine 2013, 31, 2372–2380. [Google Scholar] [CrossRef] [PubMed]
- Vaccarella, S.; Lortet-Tieulent, J.; Plummer, M.; Franceschi, S.; Bray, F. Worldwide trends in cervical cancer incidence: Impact of screening against changes in disease risk factors. Eur. J. Cancer 2013, 49, 3262–3273. [Google Scholar] [CrossRef]
- Sharma, S.J.; Schartinger, V.H.; Wuerdemann, N.; Langer, C.; Möllenhoff, K.; Collin, L.; Sutton, L.; Riedl, D.; Kreuter, A.; Lechner, M.; et al. Awareness of Human Papillomavirus (HPV) and HPV Vaccination amongst the General Population in Germany: Lack of Awareness and Need for Action. Oncol. Res. Treat. 2022, 45, 561–567. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | AAPC | Confidence Interval |
|---|---|---|
| Invasive cervical cancer | ||
| All women | −1.89 | −2.07–−1.65 |
| 0–19 years | 2.48 | −22.62–35.56 |
| 20–29 years | −4.86 | −5.83–−4.09 |
| 30–39 years | −2.42 | −2.98–−1.52 |
| 40–49 years | −2.78 | −3.14–−2.17 |
| 50–59 years | −1.35 | −1.84–−0.85 |
| 60–79 years | −1.62 | −1.86–−1.36 |
| Over 80 years | −2.25 | −2.84–−1.3 |
| Carcinoma in situ/Dysplasia | ||
| All women | −4.91 | −5.34–−4.49 |
| 0–19 years | −17.06 | −18.63–−15.45 |
| 20–29 years | −12.17 | −12.91–−11.57 |
| 30–39 years | −7.24 | −7.88–−6.51 |
| 40–49 years | −3.43 | −4.05–−2.9 |
| 50–59 years | −1.23 | −1.82–−0.65 |
| 60–79 years | −1.64 | −2.32–−1.15 |
| Over 80 years | 0.21 | −2–1.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tampakoudis, G.; Anastasiou, O.E. Burden of HPV-Related Hospitalization in Germany from 2000 to 2021. Viruses 2023, 15, 1857. https://doi.org/10.3390/v15091857
Tampakoudis G, Anastasiou OE. Burden of HPV-Related Hospitalization in Germany from 2000 to 2021. Viruses. 2023; 15(9):1857. https://doi.org/10.3390/v15091857
Chicago/Turabian StyleTampakoudis, Georgios, and Olympia E. Anastasiou. 2023. "Burden of HPV-Related Hospitalization in Germany from 2000 to 2021" Viruses 15, no. 9: 1857. https://doi.org/10.3390/v15091857