
Long-Term Impact of Direct-Acting Antivirals on Liver Fibrosis and Survival in HCV-Infected Liver Transplant Recipients
 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Clinical Data
2.2. The NAVIGATORE Database
2.3. Compassionate Use Program in Italy
2.4. Clinical Outcomes
- (1)
- Efficacy and safety data:
- (2)
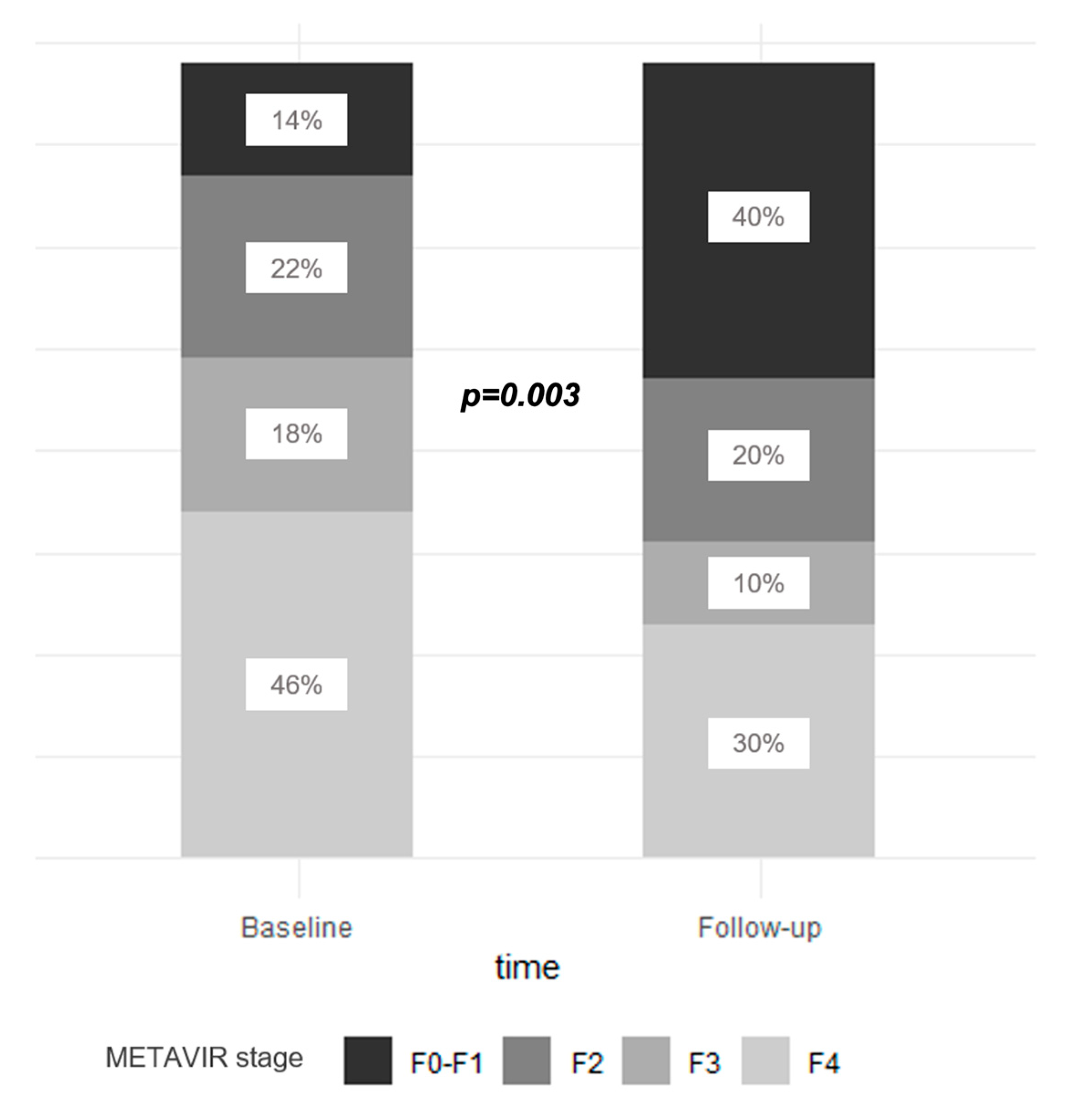
- Fibrosis evolution after SVR:
- -
- Fibrosis improvement: reduction in METAVIR class from F3–4 to F0–2.;
- -
- Fibrosis worsening: increase in METAVIR class from F0–2 to F3–4;
- -
- Fibrosis stabilization: unchanged METAVIR class.
- (3)
- Patient and graft survival:
- (4)
- HCC recurrence after LT:
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of Patient Population
3.2. Efficacy and Safety of DAA Treatment after LT
3.3. Biochemical Tests after SVR
3.4. Liver Stiffness Evolution in LT Recipients after SVR
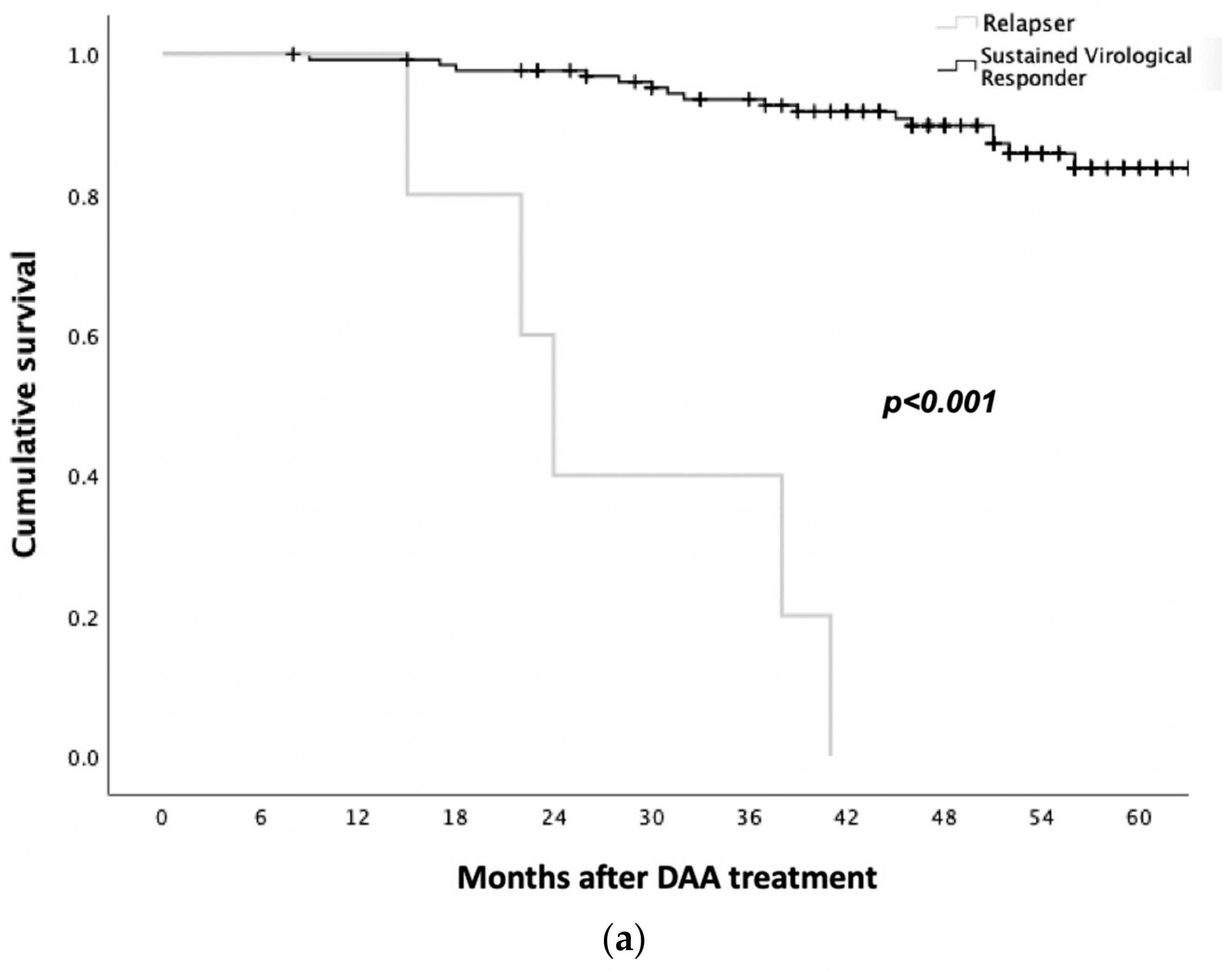
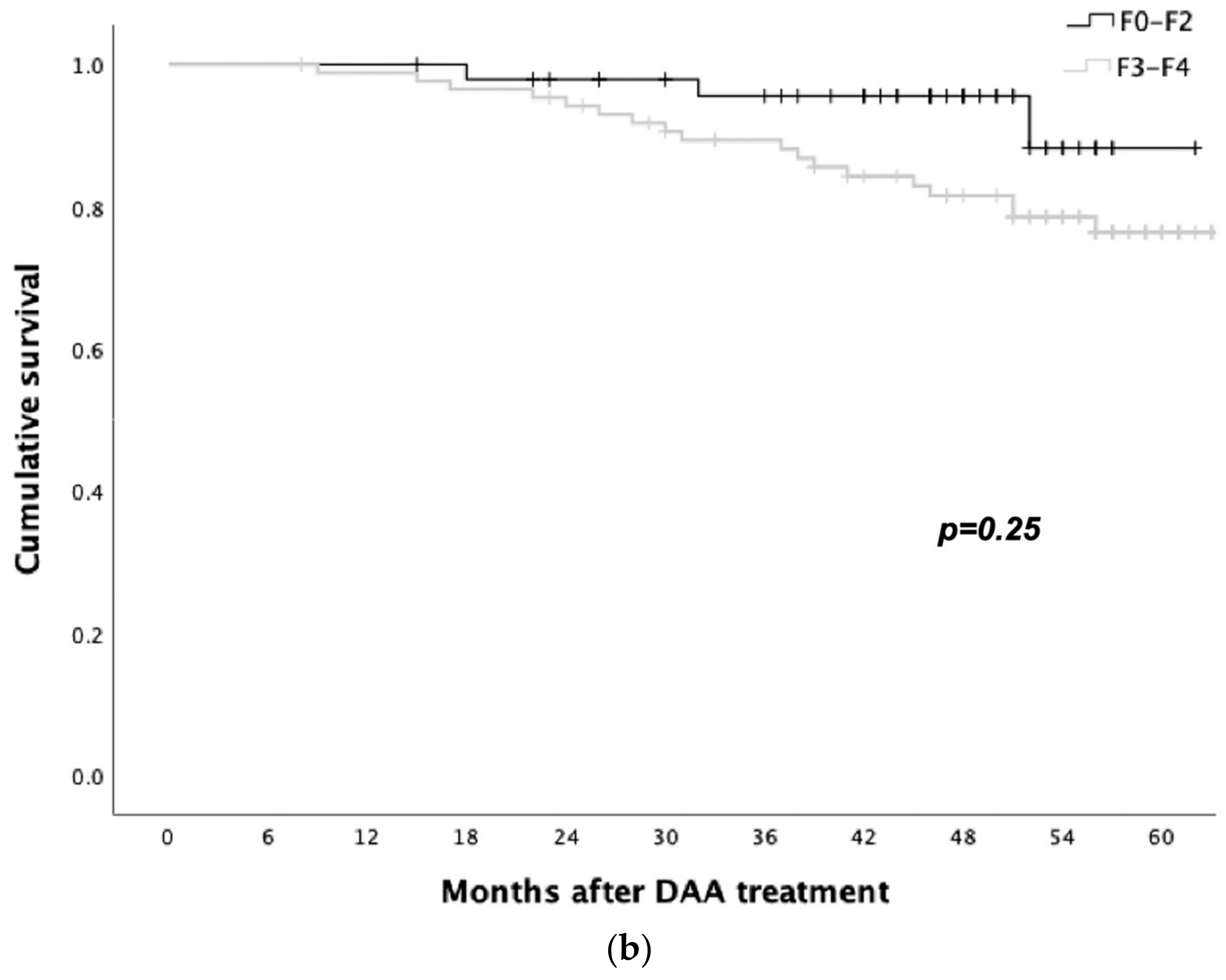
3.5. Survival Analysis
3.6. HCC Recurrence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gambato, M.; Lens, S.; Navasa, M.; Forns, X. Treatment options in patients with decompensated cirrhosis, pre- and post-transplantation. J. Hepatol. 2014, 61, S120–S131. [Google Scholar] [CrossRef] [Green Version]
- Belli, L.S.; Perricone, G.; Adam, R.; Cortesi, P.A.; Strazzabosco, M.; Facchetti, R.; Karam, V.; Salizzoni, M.; Andujar, R.L.; Fondevila, C.; et al. Impact of DAAs on liver transplantation: Major effects on the evolution of indications and results. An ELITA study based on the ELTR registry. J. Hepatol. 2018, 69, 810–817. [Google Scholar] [CrossRef]
- Pascasio, J.M.; Vinaixa, C.; Ferrer, M.T.; Colmenero, J.; Rubin, A.; Castells, L.; Manzano, M.L.; Lorente, S.; Testillano, M.; Xiol, X.; et al. Clinical outcomes of patients undergoing antiviral therapy while awaiting liver transplantation. J. Hepatol. 2017, 67, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Carrat, F.; Fontaine, H.; Dorival, C.; Simony, M.; Hezode, C.; De Ledinghen, V.; Larrey, D.; Haour, G.; Bronowicki, J.P.; Zoulim, F.; et al. Clinical outcomes in patients with chronic hepatitis C after direct-acting antiviral treatment: A prospective cohort study. Lancet 2019, 393, 1453–1464. [Google Scholar] [CrossRef]
- Cheung, M.C.M.; Walker, A.J.; Hudson, B.E.; Verma, S.; McLauchlan, J.; Mutimer, D.J.; Brown, A.; Gelson, W.T.; MacDonald, D.C.; Agarwal, K.; et al. Outcomes after successful direct-acting antiviral therapy for patients with chronic hepatitis C and decompensated cirrhosis. J. Hepatol. 2016, 65, 741–747. [Google Scholar] [CrossRef] [Green Version]
- Innes, H.; McDonald, S.; Hayes, P.; Dillon, J.F.; Allen, S.; Goldberg, D.; Mills, P.R.; Barclay, S.T.; Wilks, D.; Valerio, H.; et al. Mortality in hepatitis C patients who achieve a sustained viral response compared to the general population. J. Hepatol. 2017, 66, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahon, P.; Bourcier, V.; Layese, R.; Audureau, E.; Cagnot, C.; Marcellin, P.; Guyader, D.; Fontaine, H.; Larrey, D.; De Lédinghen, V.; et al. Eradication of Hepatitis C Virus Infection in Patients with Cirrhosis Reduces Risk of Liver and Non-Liver Complications. Gastroenterology 2017, 152, 142.e2–156.e2. [Google Scholar] [CrossRef] [Green Version]
- Ferrarese, A.; Zanetto, A.; Gambato, M.; Bortoluzzi, I.; Nadal, E.; Germani, G.; Senzolo, M.; Burra, P.; Russo, F.P. Liver transplantation for viral hepatitis in 2015. World J. Gastroenterol. 2016, 22, 1570–1581. [Google Scholar] [CrossRef]
- Charlton, M.; Everson, G.T.; Flamm, S.L.; Kumar, P.; Landis, C.; Brown, R.S.; Fried, M.W.; Terrault, N.A.; O’Leary, J.G.; Vargas, H.E.; et al. Ledipasvir and Sofosbuvir Plus Ribavirin for Treatment of HCV Infection in Patients with Advanced Liver Disease. Gastroenterology 2015, 149, 649–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manns, M.; Samuel, D.; Gane, E.J.; Mutimer, D.; McCaughan, G.; Buti, M.; Prieto, M.; Calleja, J.L.; Peck-Radosavljevic, M.; Müllhaupt, B.; et al. Ledipasvir and sofosbuvir plus ribavirin in patients with genotype 1 or 4 hepatitis C virus infection and advanced liver disease: A multicentre, open-label, randomised, phase 2 trial. Lancet Infect. Dis. 2016, 16, 685–697. [Google Scholar] [CrossRef]
- Forns, X.; Charlton, M.; Denning, J.; McHutchison, J.G.; Symonds, W.T.; Brainard, D.; Brandt-Sarif, T.; Chang, P.; Kivett, V.; Castells, L.; et al. Sofosbuvir compassionate use program for patients with severe recurrent hepatitis C after liver transplantation. Hepatology 2015, 61, 1485–1494. [Google Scholar] [CrossRef]
- Saxena, V.; Khungar, V.; Verna, E.C.; Levitsky, J.; Brown, R.S., Jr.; Hassan, M.A.; Sulkowski, M.S.; O’Leary, J.G.; Koraishy, F.; Galati, J.S.; et al. Safety and efficacy of current direct-acting antiviral regimens in kidney and liver transplant recipients with hepatitis C: Results from the HCV-TARGET study. Hepatology 2017, 66, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Pungpapong, S.; Aqel, B.; Leise, M.; Werner, K.T.; Murphy, J.L.; Henry, T.M.; Ryland, K.; Chervenak, A.E.; Watt, K.D.; Vargas, H.E.; et al. Multicenter experience using simeprevir and sofosbuvir with or without ribavirin to treat hepatitis C genotype 1 after liver transplant. Hepatology 2015, 61, 1880–1886. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, K.; Castells, L.; Mullhaupt, B.; Rosenberg, W.; McNabb, B.; Arterburn, S.; Camus, G.; McNally, J.; Stamm, L.M.; Brainard, D.M.; et al. Sofosbuvir/velpatasvir for 12 weeks in genotype 1–4 HCV-infected liver transplant recipients. J. Hepatol. 2018, 69, 603–607. [Google Scholar] [CrossRef] [Green Version]
- Poordad, F.; Schiff, E.R.; Vierling, J.M.; Landis, C.; Fontana, R.J.; Yang, R.; McPhee, F.; Hughes, E.A.; Noviello, S.; Swenson, E.S. Daclatasvir with sofosbuvir and ribavirin for hepatitis C virus infection with advanced cirrhosis or post-liver transplantation recurrence. Hepatology 2016, 63, 1493–1505. [Google Scholar] [CrossRef]
- Martini, S.; Sacco, M.; Strona, S.; Arese, D.; Tandoi, F.; Olio, D.D.; Stradella, D.; Cocchis, D.; Mirabella, S.; Rizza, G.; et al. Impact of viral eradication with sofosbuvir-based therapy on the outcome of post-transplant hepatitis C with severe fibrosis. Liver Int. 2017, 37, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Beinhardt, S.; Al-Zoairy, R.; Kozbial, K.; Stättermayer, A.F.; Maieron, A.; Stauber, R.; Strasser, M.; Zoller, H.; Graziadei, I.; Rasoul-Rockenschaub, S.; et al. Long-term follow-up of ribavirin-free DAA-based treatment in HCV recurrence after orthotopic liver transplantation. Liver Int. 2018, 38, 1188–1197. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pajares, F.; Tejedor-Tejada, J.; Torres-Yuste, R.; Almohalla-Alvárez, C.; Sánchez-Ocaña, R.; Peñas-Herrero, I.; Cimavilla-Román, M.; de Benito-Sanz, M.; Sánchez-Martín, F.; Sánchez-Antolín, G. Efficacy of Direct-acting Antivirals to Improve Clinical Condition, Fibrosis, and Liver Function in Liver Transplant Recipients Infected by Hepatitis C. Transplant. Proc. 2019, 51, 74–76. [Google Scholar] [CrossRef]
- Mauro, E.; Crespo, G.; Montironi, C.; Londoño, M.C.; Hernández-Gea, V.; Ruiz, P.; Sastre, L.; Lombardo, J.; Mariño, Z.; Díaz, A.; et al. Portal pressure and liver stiffness measurements in the prediction of fibrosis regression after sustained virological response in recurrent hepatitis C. Hepatology 2018, 67, 1683–1694. [Google Scholar] [CrossRef]
- Cotter, T.G.; Paul, S.; Sandıkçı, B.; Couri, T.; Bodzin, A.S.; Little, E.C.; Sundaram, V.; Charlton, M. Improved Graft Survival After Liver Transplantation for Recipients with Hepatitis C Virus in the Direct-Acting Antiviral Era. Liver Transpl. 2019, 25, 598–609. [Google Scholar] [CrossRef]
- Young, K.; Liu, B.; Bhuket, T.; Gish, R.G.; Wong, R.J. Improved liver transplant waitlist mortality and lower risk of disease progression among chronic hepatitis C patients awaiting liver transplantation after the introduction of direct-acting antiviral therapies in the United States. J. Viral Hepat. 2019, 26, 350–361. [Google Scholar] [CrossRef]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Iacob, S.; Cerban, R.; Pietrareanu, C.; Ester, C.; Iacob, R.; Gheorghe, C.; Popescu, I.; Gheorghe, L. 100% Sustained Virological Response and Fibrosis Improvement in Real-Life Use of Direct Acting Antivirals in Genotype-1b Recurrent Hepatitis C following Liver Transplantation. J. Gastrointest. Liver Dis. 2018, 27, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Raschzok, N.; Schott, E.; Reutzel-Selke, A.; Damrah, I.; Gül-Klein, S.; Strücker, B.; Sauer, I.M.; Pratschke, J.; Eurich, D.; Stockmann, M. The impact of directly acting antivirals on the enzymatic liver function of liver transplant recipients with recurrent hepatitis C. Transpl. Infect. Dis. 2016, 18, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M.; Gane, E.; Manns, M.P.; Brown, R.S.; Curry, M.P.; Kwo, P.Y.; Fontana, R.J.; Gilroy, R.; Teperman, L.; Muir, A.J.; et al. Sofosbuvir and Ribavirin for Treatment of Compensated Recurrent Hepatitis C Virus Infection After Liver Transplantation. Gastroenterology 2015, 148, 108–117. [Google Scholar] [CrossRef]
- Liu, A.; Angirekula, M.; Elhawary, A.; Mara, K.; Kulai, T.; Leise, M.; Watt, K.D. Progression of fibrosis in liver transplant recipients with hepatitis C before and after sustained virologic response. Clin. Transplant. 2023, e15050. [Google Scholar] [CrossRef]
- Teegen, E.M.; Dürr, M.; Maurer, M.M.; Eurich, F.; Vollbort, A.; Globke, B.; Bahra, M.; Blaeker, H.; Pratschke, J.; Eurich, D. Evaluation of histological dynamics, kidney function and diabetes in liver transplant patients after antiviral treatment with direct-acting antivirals: Therapy of HCV-recurrence. Transpl. Infect. Dis. 2019, 21, e13020. [Google Scholar] [CrossRef]
- Crespo, G.; Trota, N.; Londoño, M.-C.; Mauro, E.; Baliellas, C.; Castells, L.; Castellote, J.; Tort, J.; Forns, X.; Navasa, M. The efficacy of direct anti-HCV drugs improves early post-liver transplant survival and induces significant changes in waiting list composition. J. Hepatol. 2018, 69, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Vukotic, R.; Conti, F.; Fagiuoli, S.; Morelli, M.C.; Pasulo, L.; Colpani, M.; Foschi, F.G.; Berardi, S.; Pianta, P.; Mangano, M.; et al. Long-term outcomes of direct acting antivirals in post-transplant advanced hepatitis C virus recurrence and fibrosing cholestatic hepatitis. J. Viral Hepat. 2017, 24, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Gorgen, A.; Galvin, Z.; Huang, A.C.; Vinaixa, C.; O’Rourke, J.M.; Francoz, C.; Hansen, B.E.; Durand, F.; Elsharkawy, A.M.; Shah, T.; et al. The Impact of Direct-acting Antivirals on Overall Mortality and Tumoral Recurrence in Patients with Hepatocellular Carcinoma Listed for Liver Transplantation: An International Multicenter Study. Transplantation 2020, 104, 2087–2096. [Google Scholar] [CrossRef] [PubMed]
- Piñero, F.; Boin, I.; Chagas, A.; Quiñonez, E.; Marciano, S.; Vilatobá, M.; Santos, L.; Anders, M.; Hoyos Duque, S.; Soares Lima, A.; et al. Direct-Acting Antivirals and Hepatocellular Carcinoma: No Evidence of Higher Wait-List Progression or Posttransplant Recurrence. Liver Transpl. 2020, 26, 640–650. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N = 136 | N (%) Median (IQR) |
|---|---|
| Sex (male) | 108 (79%) |
| Age (years) | 58 (52–66) |
| HCV genotype | |
| 102 (75%) |
| 11 (8%) |
| 17 (13%) |
| 6 (4%) |
| Log HCV-RNA (UI/mL) | 6.2 (5.7–6.7) |
| Compassionate use program/Navigatore | 60 (44%)/76 (56%) |
| DAA regimen | |
| 81 (60%) |
| 5 (4%) |
| 33 (24%) |
| 13 (9%) |
| 3 (2%) |
| 1 (1%) |
| Ribavirin use | 125 (92%) |
| Treatment duration | |
| 94 (69%) |
| 42 (31%) |
| Time between transplant and DAA treatment (months) | 62 (16–122) |
| LT indication | |
| 65 (48%) |
| 71 (52%) |
| Main immunosuppression | |
| 102 (76%) |
| 23 (17%) |
| 3 (2%) |
| 6 (5%) |
| METAVIR stage before DAA * | |
| 19 (14%) |
| 30 (22%) |
| 31 (23%) |
| 56 (41%) |
| Platelet count (×109/L) | 121 (84–157) |
| Platelet count < 50 × 109/L | |
| ALT (IU/L) | 65 (41–105) |
| Total bilirubin (mg/dL) | 0.72 (0.5–1.11) |
| INR | 1.06 (1.1–1.12) |
| Albumin (g/L) | 39 (36–41) |
| Creatinine (mg/dL) | 0.96 (0.81–1.18) |
| MELD score (in patients with cirrhosis) | 8 (7–12) |
| Child–Pugh class (in patients with cirrhosis) | |
| 36 (80%) |
| 9 (20%) |
| Univariate Cox | Multivariate Cox | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age (years) | 1.042 | 0.99–1.09 | 0.116 | |||
| Gender (male) | 4.971 | 0.65–37–54 | 0.120 | |||
| Advanced fibrosis at baseline | 2.094 | 0.59–7.41 | 0.252 | |||
| LT indication (HCC) | 1.265 | 0.48–3.28 | 0.630 | |||
| Time between LT and DAAs | 0.998 | 0.99–1 | 0.530 | |||
| Platelet count < 150,000/mm3 at baseline | 2.372 | 0.53–10.56 | 0.257 | |||
| Platelet count < 50,000/mm3 at baseline | 3.768 | 0.85–16.73 | 0.081 | 5.08 | 1.09–23.61 | 0.038 ** |
| Albumin level at baseline | 0.946 | 0.87–1.02 | 0.165 | |||
| INR at baseline | 0.946 | 0.03–25.53 | 0.946 | |||
| Creatinine level at baseline | 3.918 | 1–15.3 | 0.049 ** | 4.942 | 1.2–20–37 | 0.027 ** |
| Liver decompensation at baseline | 2.019 | 0.51–7.97 | 0.316 | |||
| Median (IQR) N (%) | Overall n = 57 * | Patients with HCC Recurrence after DAA N = 8 ** | Patients without HCC Recurrence after DAA N = 49 *** | p-Value |
|---|---|---|---|---|
| Vascular invasion | 16 (28%) | 3 (38%) | 13 (24%) | 0.522 |
| Milan criteria: | 0.237 | |||
| 24 (42%) | 5 (62%) | 19 (39%) | |
| 21 (37%) | 3 (38%) | 18 (37%) | |
| 12 (21%) | 0 (0%) | 12 24%) | |
| HCC grading | 0.359 | |||
| 1 (2%) | 0 (0%) | 1 (2%) | |
| 33 (58%) | 6 (75%) | 27 (55%) | |
| 8 (14%) | 2 (25%) | 6 (12%) | |
| 12 (21%) | 0 (0%) | 12 (25%) | |
| 3 (5%) | 0 (0%) | 3 (6%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gambato, M.; Manuli, C.; Lynch, E.N.; Battistella, S.; Germani, G.; Senzolo, M.; Zanetto, A.; Ferrarese, A.; Vitale, A.; Gringeri, E.; et al. Long-Term Impact of Direct-Acting Antivirals on Liver Fibrosis and Survival in HCV-Infected Liver Transplant Recipients. Viruses 2023, 15, 1702. https://doi.org/10.3390/v15081702
Gambato M, Manuli C, Lynch EN, Battistella S, Germani G, Senzolo M, Zanetto A, Ferrarese A, Vitale A, Gringeri E, et al. Long-Term Impact of Direct-Acting Antivirals on Liver Fibrosis and Survival in HCV-Infected Liver Transplant Recipients. Viruses. 2023; 15(8):1702. https://doi.org/10.3390/v15081702
Chicago/Turabian StyleGambato, Martina, Chiara Manuli, Erica N. Lynch, Sara Battistella, Giacomo Germani, Marco Senzolo, Alberto Zanetto, Alberto Ferrarese, Alessandro Vitale, Enrico Gringeri, and et al. 2023. "Long-Term Impact of Direct-Acting Antivirals on Liver Fibrosis and Survival in HCV-Infected Liver Transplant Recipients" Viruses 15, no. 8: 1702. https://doi.org/10.3390/v15081702