
COVID-19 Disease in Pediatric Solid Organ Transplantation from Alpha to Omicron: A High Monocyte Count in the Preceding Three Months Portends a Risk for Severe Disease
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Statistics
3. Results
3.1. Demographics and Clinical Course
3.2. High Absolute Monocyte Count in the Three Months Preceding Infection and High Tacrolimus Level Are Associated with Severe COVID-19 Disease in Univariate Analysis
3.3. Concomitant Immunosuppression, Steroid Dose, and Protection against Severe Disease
3.4. Acute Rejection and COVID-19 Disease
3.5. High Lymphocyte Count at Diagnosis Decreased, and High Monocyte Count Preceding Infection Increased, the Odds of Having Severe COVID-19 Disease in Multivariable Analysis
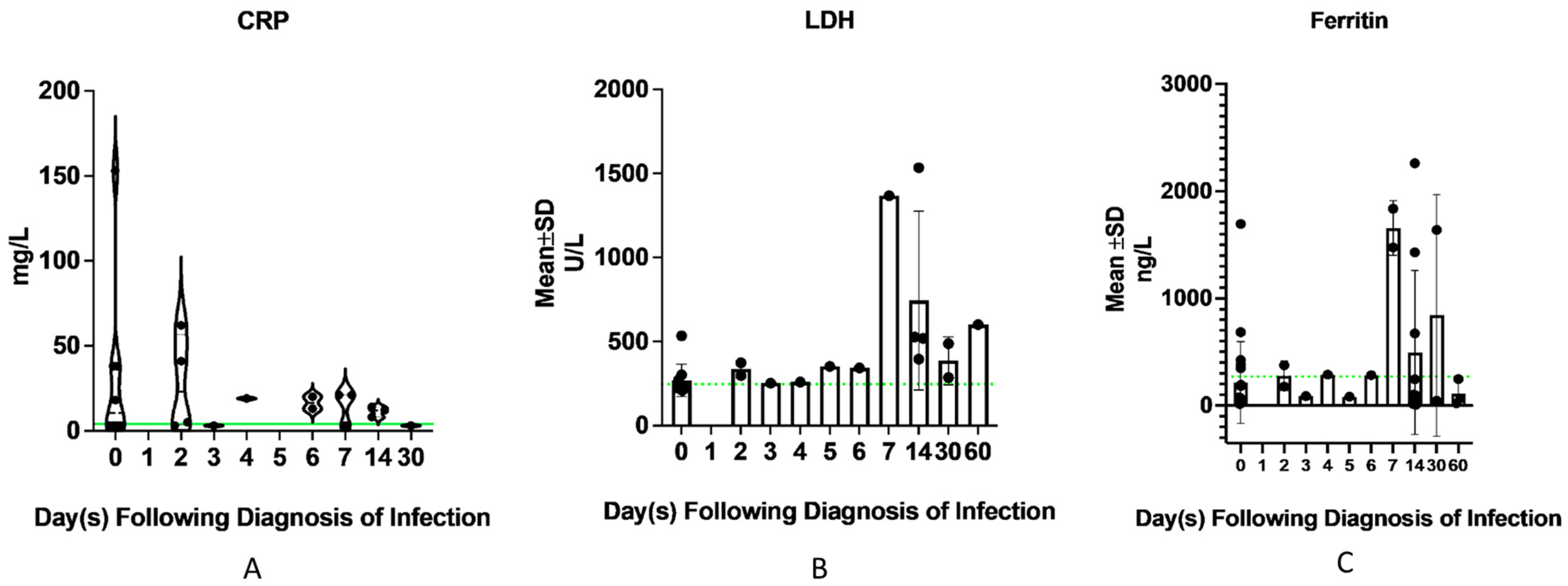
3.6. Evolution of Acute Phase Reactants
4. Discussion
5. Study Strengths
6. Study Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Deng, G.; Yin, M.; Chen, X.; Zeng, F. Clinical determinants for fatality of 44,672 patients with COVID-19. Crit. Care 2020, 24, 179. [Google Scholar] [CrossRef] [PubMed]
- Nacif, L.S.; Zanini, L.Y.; Waisberg, D.R.; Pinheiro, R.S.; Galvao, F.; Andraus, W.; D’Albuquerque, L.C. COVID-19 in solid organ transplantation patients: A systematic review. Clinics 2020, 75, e1983. [Google Scholar] [CrossRef] [PubMed]
- Demetris, A.J.; Batts, K.P.; Dhillon, A.P.; Ferrell, L.; Fung, J.; Geller, S.A.; Hart, J.; Hayry, P.; Hofmann, W.J.; Hubscher, S.; et al. Banff schema for grading liver allograft rejection: An international consensus document. Hepatology 1997, 25, 658–663. [Google Scholar] [CrossRef]
- Ruiz, P.; Bagni, A.; Brown, R.; Cortina, G.; Harpaz, N.; Magid, M.S.; Reyes, J. Histological criteria for the identification of acute cellular rejection in human small bowel allografts: Results of the pathology workshop at the VIII International Small Bowel Transplant Symposium. Transplant. Proc. 2004, 36, 335–337. [Google Scholar] [CrossRef]
- Loupy, A.; Haas, M.; Solez, K.; Racusen, L.; Glotz, D.; Seron, D.; Nankivell, B.J.; Colvin, R.B.; Afrouzian, M.; Akalin, E.; et al. The Banff 2015 Kidney Meeting Report: Current Challenges in Rejection Classification and Prospects for Adopting Molecular Pathology. Am. J. Transplant. 2017, 17, 28–41. [Google Scholar] [CrossRef]
- Haas, M.; Loupy, A.; Lefaucheur, C.; Roufosse, C.; Glotz, D.; Seron, D.; Nankivell, B.J.; Halloran, P.F.; Colvin, R.B.; Akalin, E.; et al. The Banff 2017 Kidney Meeting Report: Revised diagnostic criteria for chronic active T cell-mediated rejection, antibody-mediated rejection, and prospects for integrative endpoints for next-generation clinical trials. Am. J. Transplant. 2018, 18, 293–307. [Google Scholar] [CrossRef] [Green Version]
- Mazzoni, A.; Salvati, L.; Maggi, L.; Capone, M.; Vanni, A.; Spinicci, M.; Mencarini, J.; Caporale, R.; Peruzzi, B.; Antonelli, A.; et al. Impaired immune cell cytotoxicity in severe COVID-19 is IL-6 dependent. J. Clin. Investig. 2020, 130, 4694–4703. [Google Scholar] [CrossRef]
- Cervera, C.; Fernandez-Ruiz, M.; Valledor, A.; Linares, L.; Anton, A.; Angeles Marcos, M.; Sanclemente, G.; Hoyo, I.; Cofan, F.; Ricart, M.J.; et al. Epidemiology and risk factors for late infection in solid organ transplant recipients. Transpl. Infect. Dis. 2011, 13, 598–607. [Google Scholar] [CrossRef]
- Bansal, N.; Ovchinsky, N.; Foca, M.; Lamour, J.M.; Kogan-Liberman, D.; Hsu, D.T.; Beddows, K.; Abraham, L.; Coburn, M.; Cunningham, R.; et al. COVID-19 infection in pediatric solid organ transplant patients. Pediatr. Transplant. 2022, 26, e14156. [Google Scholar] [CrossRef]
- Varnell, C., Jr.; Harshman, L.A.; Smith, L.; Liu, C.; Chen, S.; Al-Akash, S.; Barletta, G.M.; Belsha, C.; Brakeman, P.; Chaudhuri, A.; et al. COVID-19 in pediatric kidney transplantation: The Improving Renal Outcomes Collaborative. Am. J. Transplant. 2021, 21, 2740–2748. [Google Scholar] [CrossRef]
- Cui, X.; Zhao, Z.; Zhang, T.; Guo, W.; Guo, W.; Zheng, J.; Zhang, J.; Dong, C.; Na, R.; Zheng, L.; et al. A systematic review and meta-analysis of children with coronavirus disease 2019 (COVID-19). J. Med. Virol. 2021, 93, 1057–1069. [Google Scholar] [CrossRef] [PubMed]
- Turner, C.J. COVID-19: The disease, the vaccine and the heart. J. Paediatr. Child Health 2023, 59, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; on behalf of the HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Fan, B.E.; Chong, V.C.L.; Chan, S.S.W.; Lim, G.H.; Lim, K.G.E.; Tan, G.B.; Mucheli, S.S.; Kuperan, P.; Ong, K.H. Hematologic parameters in patients with COVID-19 infection. Am. J. Hematol. 2020, 95, E131–E134. [Google Scholar] [CrossRef] [Green Version]
- Henry, B.M.; de Oliveira, M.H.S.; Benoit, S.; Plebani, M.; Lippi, G. Hematologic, biochemical and immune biomarker abnormalities associated with severe illness and mortality in coronavirus disease 2019 (COVID-19): A meta-analysis. Clin. Chem. Lab. Med. 2020, 58, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.; Guo, R.; Lei, L.; Liu, H.; Wang, Y.; Wang, Y.; Qian, H.; Dai, T.; Zhang, T.; Lai, Y.; et al. Frontline Science: COVID-19 infection induces readily detectable morphologic and inflammation-related phenotypic changes in peripheral blood monocytes. J. Leukoc. Biol. 2021, 109, 13–22. [Google Scholar] [CrossRef]
- Junqueira, C.; Crespo, A.; Ranjbar, S.; de Lacerda, L.B.; Lewandrowski, M.; Ingber, J.; Parry, B.; Ravid, S.; Clark, S.; Schrimpf, M.R.; et al. FcgammaR-mediated SARS-CoV-2 infection of monocytes activates inflammation. Nature 2022, 606, 576–584. [Google Scholar] [CrossRef]
- Kroemer, A.; Khan, K.; Plassmeyer, M.; Alpan, O.; Haseeb, M.A.; Gupta, R.; Fishbein, T.M. Inflammasome activation and pyroptosis in lymphopenic liver patients with COVID-19. J. Hepatol. 2020, 73, 1258–1262. [Google Scholar] [CrossRef]
- Sefik, E.; Qu, R.; Junqueira, C.; Kaffe, E.; Mirza, H.; Zhao, J.; Brewer, J.R.; Han, A.; Steach, H.R.; Israelow, B.; et al. Inflammasome activation in infected macrophages drives COVID-19 pathology. Nature 2022, 606, 585–593. [Google Scholar] [CrossRef]
- Liu, N.; Jiang, C.; Cai, P.; Shen, Z.; Sun, W.; Xu, H.; Fang, M.; Yao, X.; Zhu, L.; Gao, X.; et al. Single-cell analysis of COVID-19, sepsis, and HIV infection reveals hyperinflammatory and immunosuppressive signatures in monocytes. Cell Rep. 2021, 37, 109793. [Google Scholar] [CrossRef]
- Li, H.; Li, X.; Lv, S.; Peng, X.; Cui, N.; Yang, T.; Yang, Z.; Yuan, C.; Yuan, Y.; Yao, J.; et al. Single-cell landscape of peripheral immune responses to fatal SFTS. Cell Rep. 2021, 37, 110039. [Google Scholar] [CrossRef] [PubMed]
- Casulleras, M.; Zhang, I.W.; Lopez-Vicario, C.; Claria, J. Leukocytes, Systemic Inflammation and Immunopathology in Acute-on-Chronic Liver Failure. Cells 2020, 9, 2632. [Google Scholar] [CrossRef] [PubMed]
- Varchetta, S.; Mele, D.; Oliviero, B.; Mantovani, S.; Ludovisi, S.; Cerino, A.; Bruno, R.; Castelli, A.; Mosconi, M.; Vecchia, M.; et al. Unique immunological profile in patients with COVID-19. Cell Mol. Immunol. 2021, 18, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Song, H.; Josleyn, N.; Janosko, K.; Skinner, J.; Reeves, R.K.; Cohen, M.; Jett, C.; Johnson, R.; Blaney, J.E.; Bollinger, L.; et al. Monkeypox virus infection of rhesus macaques induces massive expansion of natural killer cells but suppresses natural killer cell functions. PLoS ONE 2013, 8, e77804. [Google Scholar] [CrossRef] [Green Version]
- Zingaropoli, M.A.; Perri, V.; Pasculli, P.; Cogliati Dezza, F.; Nijhawan, P.; Savelloni, G.; La Torre, G.; D’Agostino, C.; Mengoni, F.; Lichtner, M.; et al. Major reduction of NKT cells in patients with severe COVID-19 pneumonia. Clin. Immunol. 2021, 222, 108630. [Google Scholar] [CrossRef]
- Jiang, Y.; Wei, X.; Guan, J.; Qin, S.; Wang, Z.; Lu, H.; Qian, J.; Wu, L.; Chen, Y.; Chen, Y.; et al. COVID-19 pneumonia: CD8(+) T and NK cells are decreased in number but compensatory increased in cytotoxic potential. Clin. Immunol. 2020, 218, 108516. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Tsankov, B.K.; Allaire, J.M.; Irvine, M.A.; Lopez, A.A.; Sauve, L.J.; Vallance, B.A.; Jacobson, K. Severe COVID-19 Infection and Pediatric Comorbidities: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 103, 246–256. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | n (%) |
|---|---|
| Transplant type | |
| 50 (65) |
| 24 (31) |
| 3 (4) |
| Symptoms | |
| 44 (58) |
| 33 (42) |
| Gender | |
| 42 (55) |
| 35 (45) |
| Duration from transplant at infection (months) | |
| 57.4 (19.7–87.2) |
| ≤1 year from transplant at infection | 13 (17) |
| >1 year from transplant at infection | 64 (83) |
| Not hospitalized | 55 (71) |
| Hospitalized | 22 (29) |
| 5 (23) |
| 17 (77) |
| Interval between BPAR in preceding 12 months and infection (months) | |
| 1.67 (1.085–3.92) |
| * Mild Disease | Severe Disease | p-Value | |
|---|---|---|---|
| (n = 55) | (n = 22) | ||
| Age at diagnosis (years) | |||
| Mean (SD) | 7.99 ± 4.83 | 6.91 ± 4.57 | 0.37 |
| Sex | |||
| Male | 29 (53) | 13 (59) | 0.8 |
| Female | 26 (47) | 9 (41) | |
| Race | |||
| African American | 14 (25) | 11 (50) | 0.06 |
| White | 20 (36) | 2 (9) | |
| Asian | 7 (13) | 4 (18) | |
| Other | 14 (25) | 5 (23) | |
| Ethnicity | |||
| Non-Hispanic | 42 (76) | 18 (82) | 0.82 |
| Hispanic | 13 (24) | 4 (18) | |
| Duration from transplant at infection (months) | |||
| Mean (SD) | 66.40 ± 45.96 | 42.09 ± 40.02 | 0.03 |
| Tacrolimus level (ng/dL) | |||
| Mean (SD) | 6.0 ± 5.3 | 8.9 ± 7.2 | 0.05 |
| On predniso(lo)ne at time of infection | |||
| yes | 22 (41) | 14 (64) | 0.11 |
| no | 32 (59) | 8 (36) | |
| Steroid dose | |||
| low | 21 (38) | 13 (59) | 0.11 |
| high | 1 (2) | 1 (5) | |
| not on steroids | 33 (60) | 8 (36) | |
| Chronic lung disease | |||
| no | 42 (76) | 11 (50) | 0.04 |
| yes | 13 (24) | 11 (50) | |
| Hypertension | |||
| yes | 16 (29) | 12 (55) | 0.06 |
| no | 39 (71) | 10 (45) | |
| Hyperlipidemia | |||
| yes | 6 (11) | 3 (14) | 1 |
| no | 49 (89) | 19 (86) | |
| Chronic kidney disease | |||
| yes | 16 (29) | 7 (32) | 1 |
| no | 39 (71) | 15 (68) | |
| Obesity | |||
| yes | 5 (9) | 3 (14) | 0.8 |
| no | 50 (91) | 18 (86) | |
| History of acute rejection | |||
| no | 45 (82) | 17 (77) | 0.89 |
| yes | 10 (18) | 5 (23) | |
| Number of immunosuppression medications at infection | |||
| 1 | 20 (37) | 4 (18) | |
| 2 | 22 (41) | 10 (45) | 0.21 |
| 3 | 12 (22) | 8 (36) | |
| Type of transplant | |||
| Isolated liver | 37 (67) | 13 (59) | 0.31 |
| Simultaneous liver kidney | 3 (5) | 0 (0) | |
| Intestine (composite + isolated intestine) | 15 (27) | 9 (41) | |
| Absolute lymphocyte count at infection (K cells/μL) | |||
| mean ± SD | 2.77 ± 1.43 | 1.79 ± 1.21 | 0.006 |
| Absolute monocyte count at infection (K cells/μL) | |||
| mean ± SD | 0.55 ± 0.29 | 0.66 ± 0.48 | 0.23 |
| Absolute lymphocyte count before infection (K cells/μL) | |||
| mean ± SD | 2.68 ± 1.19 | 3.21 ± 2.31 | 0.18 |
| Absolute monocyte count before infection (K cells/μL) | |||
| mean ± SD | 0.49 ± 0.20 | 0.75 ± 0.73 | 0.01 |
| On mycophenolate at time of infection | |||
| yes | 13 (24) | 6 (27) | 0.96 |
| no | 42 (76) | 16 (73) | |
| On sirolimus at time of infection | |||
| yes | 10 (18) | 5 (23) | 0.89 |
| no | 45 (82) | 17 (77) | |
| SARS-CoV-2 prevailing variant | |||
| Omicron | 25 (45) | 10 (45) | 0.91 |
| Other | 22 (40) | 8 (36) | |
| Delta | 8 (15) | 4 (18) |
| Immunosuppression | Transplant Type | |||
|---|---|---|---|---|
| Isolated Liver | Isolated Small Bowel | Composite | Simultaneous Liver Kidney | |
| Tacrolimus | 49 | 7 | 17 | 3 |
| Sirolimus | 5 | 3 | 6 | 3 |
| Mycophenolate | 17 | 1 | 1 | 0 |
| Predniso(lo)ne | ||||
| Low dose | 7 | 7 | 15 | 2 |
| High dose | 2 | 0 | 0 | 0 |
| Infliximab | 0 | 0 | 1 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sirgi, Y.; Stanojevic, M.; Ahn, J.; Yazigi, N.; Kaufman, S.; Khan, K.; Vitola, B.; Matsumoto, C.; Kroemer, A.; Fishbein, T.; et al. COVID-19 Disease in Pediatric Solid Organ Transplantation from Alpha to Omicron: A High Monocyte Count in the Preceding Three Months Portends a Risk for Severe Disease. Viruses 2023, 15, 1559. https://doi.org/10.3390/v15071559
Sirgi Y, Stanojevic M, Ahn J, Yazigi N, Kaufman S, Khan K, Vitola B, Matsumoto C, Kroemer A, Fishbein T, et al. COVID-19 Disease in Pediatric Solid Organ Transplantation from Alpha to Omicron: A High Monocyte Count in the Preceding Three Months Portends a Risk for Severe Disease. Viruses. 2023; 15(7):1559. https://doi.org/10.3390/v15071559
Chicago/Turabian StyleSirgi, Yasmina, Maja Stanojevic, Jaeil Ahn, Nada Yazigi, Stuart Kaufman, Khalid Khan, Bernadette Vitola, Cal Matsumoto, Alexander Kroemer, Thomas Fishbein, and et al. 2023. "COVID-19 Disease in Pediatric Solid Organ Transplantation from Alpha to Omicron: A High Monocyte Count in the Preceding Three Months Portends a Risk for Severe Disease" Viruses 15, no. 7: 1559. https://doi.org/10.3390/v15071559