
Characteristics of Anti-Measles Immunity in Lung Transplant Candidates
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Patients
2.3. Methods
2.4. Statistical Analysis
3. Results
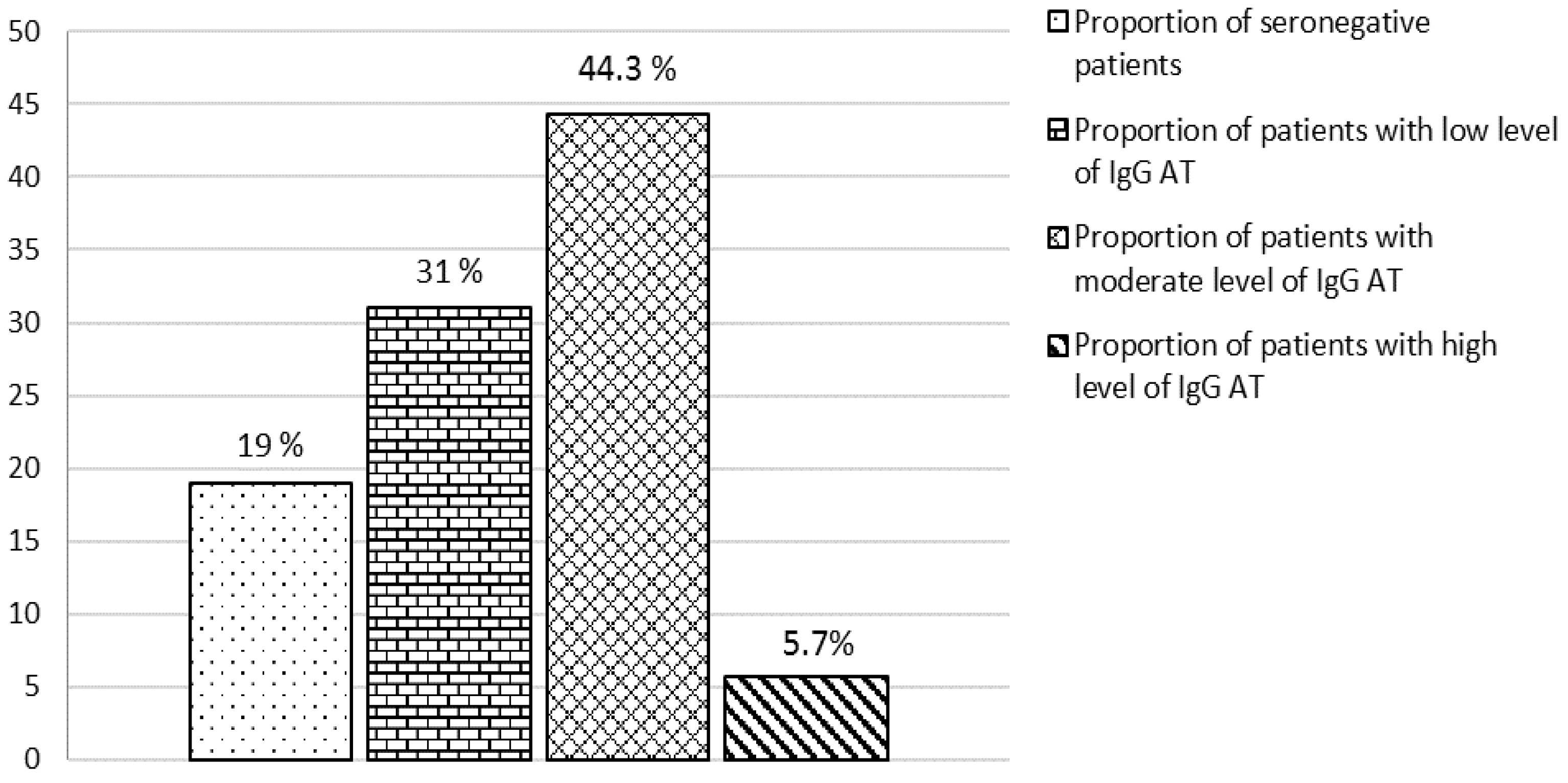
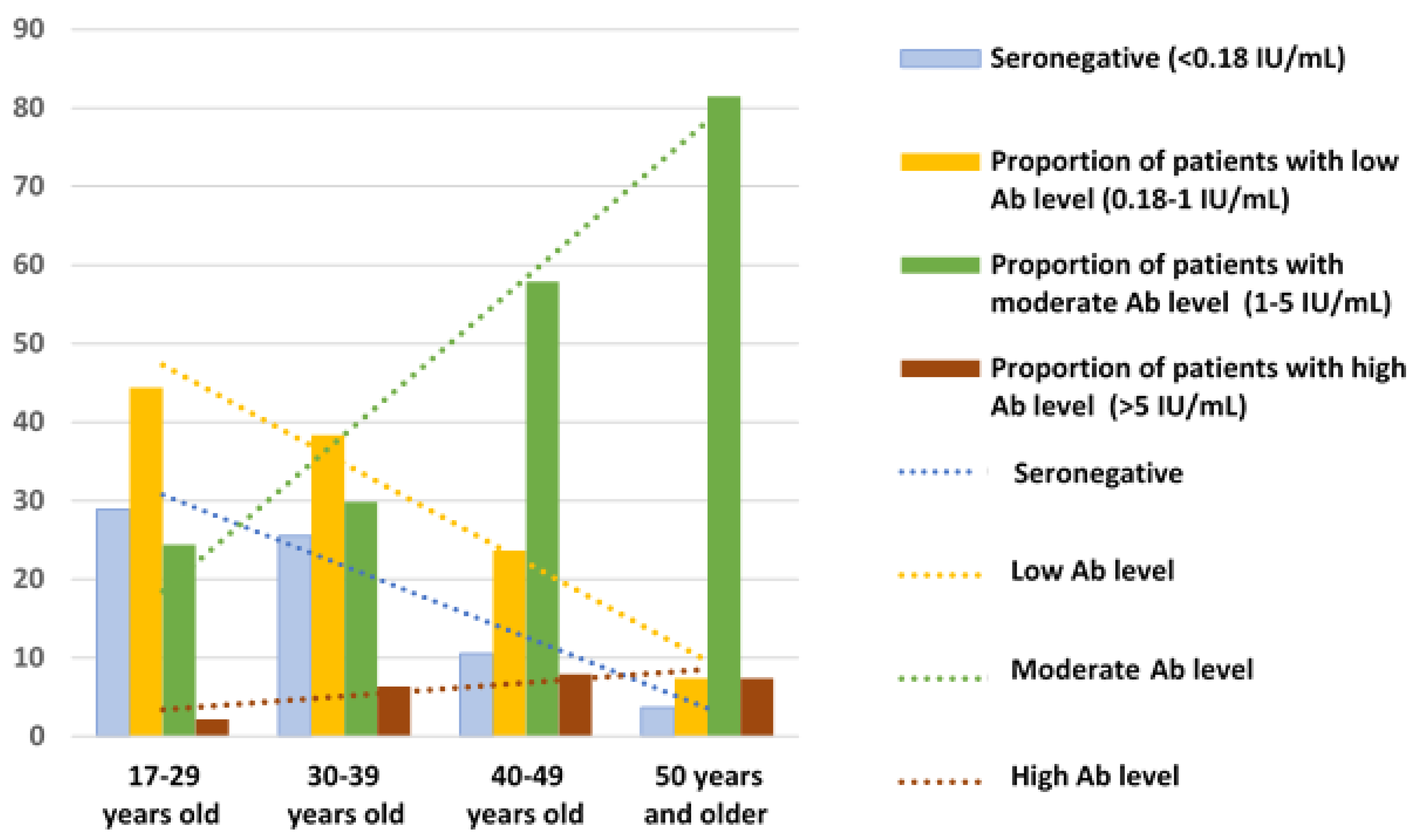
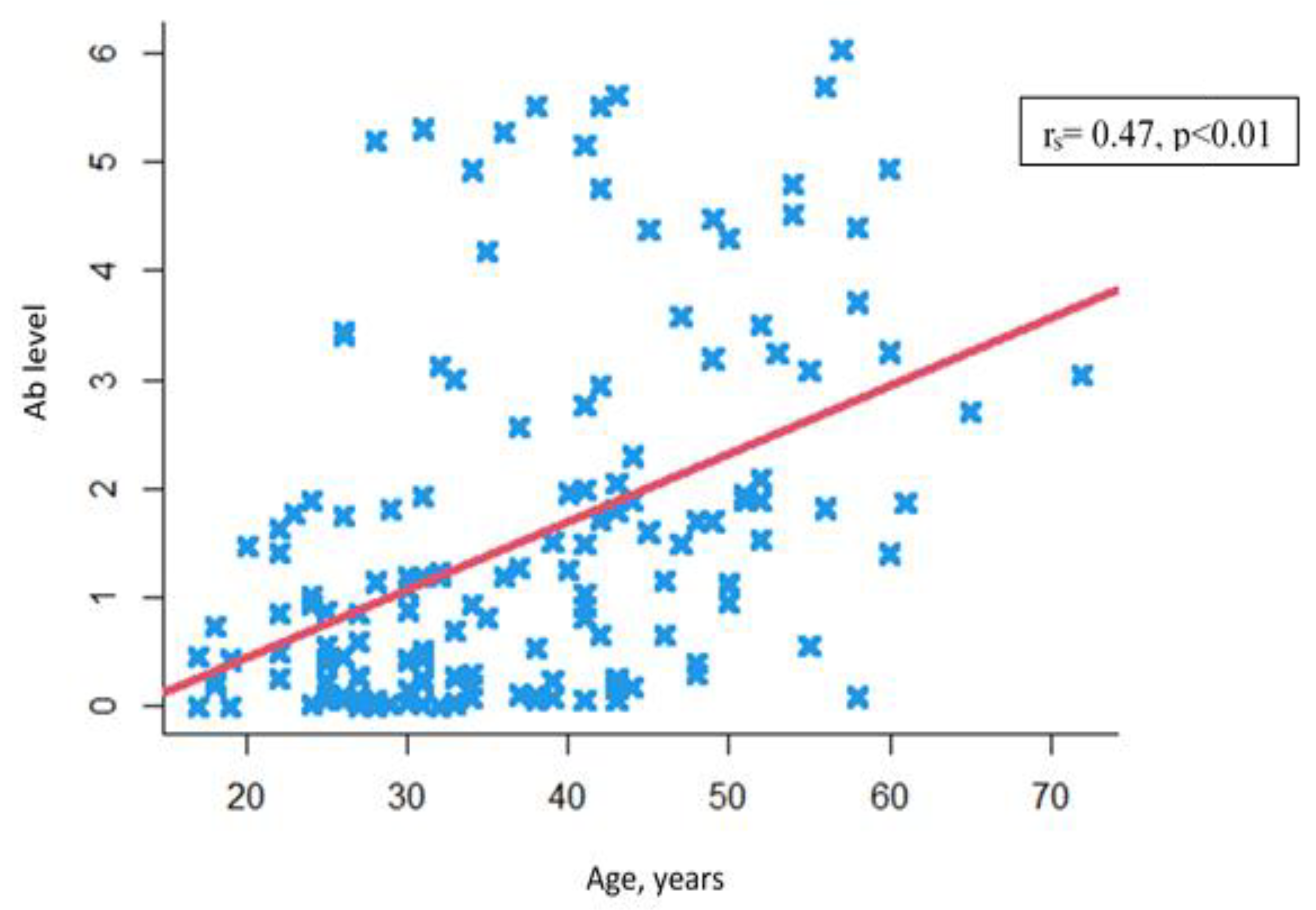
3.1. Analysis of the Relationship between Levels of Anti-Measles IgG Antibodies and Age in Patients with Severe Progressive Bronchopulmonary Disorders
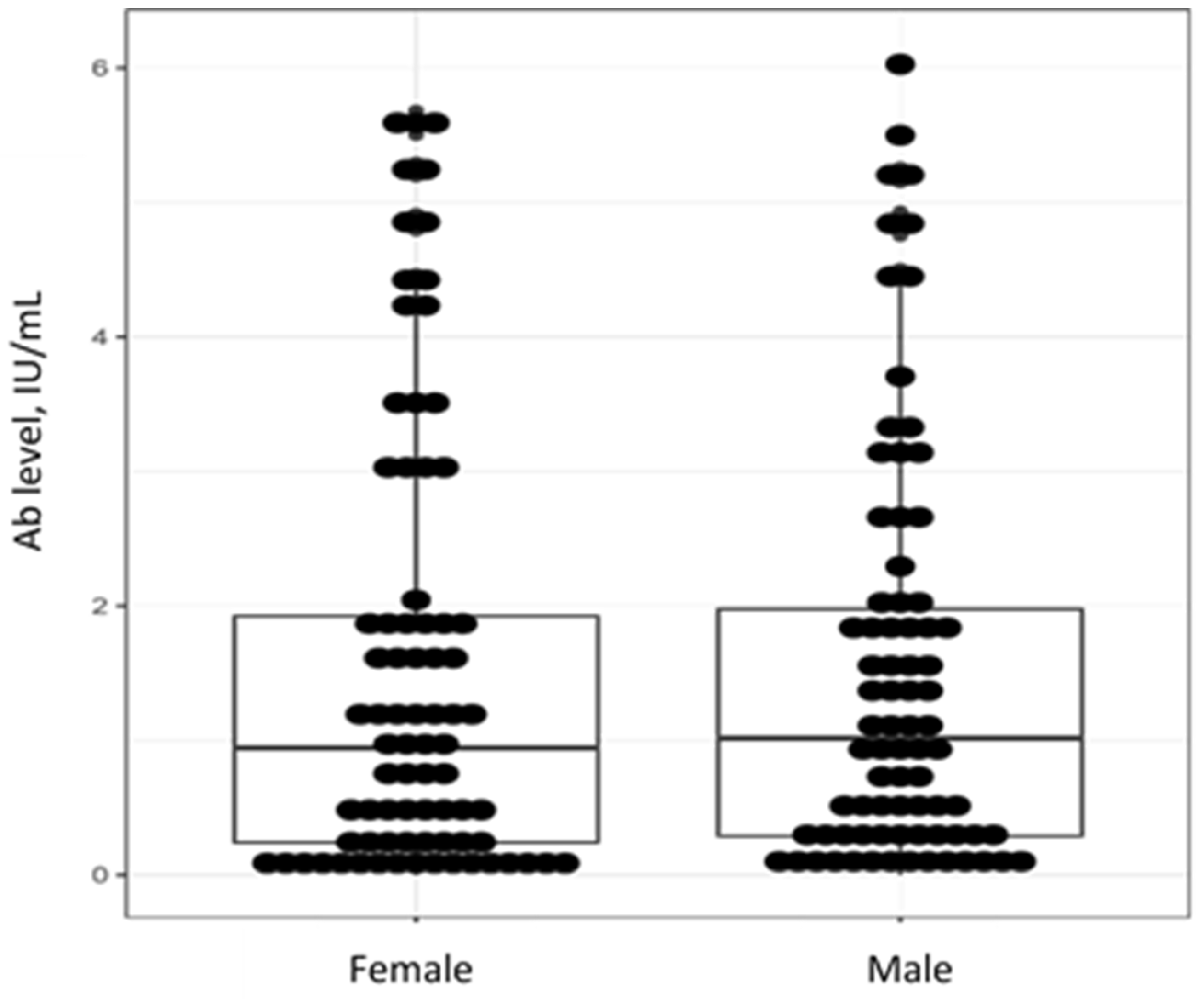
3.2. Analysis of the Relationship between Levels of Anti-Measles IgG Antibodies and Gender in Patients with Severe Progressive Bronchopulmonary Disorders
3.3. Age- and Gender-Adjusted Analysis of Anti-Measles IgG Antibodies in Patients with Severe Progressive Bronchopulmonary Disorders
3.4. Analysis of Anti-Measles IgG Antibodies by Type of Pulmonary Disease
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avery, R.K.; Ljungman, P. Prophylactic measures in the solid-organ recipient before transplantation. Clin. Infect. Dis. 2001, 33, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Bahakel, H.; Feldman, A.G.; Danziger-Isakov, L. Immunization of Solid Organ Transplant Candidates and Recipients: A 2022 Update. Infect. Dis. Clin. N. Am. 2023, 37, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Danziger-Isakov, L.; Kumar, D.; AST ID Community of Practice. Vaccination of solid organ transplant candidates and recipients: Guidelines from the American society of transplantation infectious diseases community of practice. Clin. Transplant. 2019, 33, e13563:1–e13563:10. [Google Scholar] [CrossRef] [PubMed]
- Donato-Santana, C.; Theodoropoulos, N.M. Immunization of Solid Organ Transplant Candidates and Recipients: A 2018 Update. Infect. Dis. Clin. N. Am. 2018, 32, 517–533. [Google Scholar] [CrossRef] [PubMed]
- Rubin, L.G.; Levin, M.J.; Ljungman, P.; Davies, E.G.; Avery, R.; Tomblyn, M.; Bousvaros, A.; Dhanireddy, S.; Sung, L.; Keyserling, H.; et al. Infectious Diseases Society of America. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 2014, 58, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Stucchi, R.S.B.; Lopes, M.H.; Kumar, D.; Manuel, O. Vaccine Recommendations for Solid-Organ Transplant Recipients and Donors. Transplantation 2018, 102, S72–S80. [Google Scholar] [CrossRef]
- Bruscia, E.M.; Bonfield, T.L. Innate and adaptive immunity in cystic fibrosis. Clin. Chest Med. 2016, 37, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Speich, R.; van der Bij, W. Epidemiology and management of infections after lung transplantation. Clin. Infect. Dis. 2001, 33, 58–65. [Google Scholar] [CrossRef]
- Countries in the European Region Stepping up to Stop the Spread of Measles as Cases in 2023 Already Exceed All Those in 2022. Available online: https://www.who.int/europe/news/item/26-04-2023-countries-in-the-european-region-stepping-up-to-stop-the-spread-of-measles-as-cases-in-2023-already-exceed-all-those-in-2022 (accessed on 1 September 2023).
- Mina, M.J.; Kula, T.; Leng, Y.; Li, M.; de Vries, R.D.; Knip, M.; Siljander, H.; Rewers, M.; Choy, D.F.; Wilson, M.S.; et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science 2019, 366, 599–606. [Google Scholar] [CrossRef]
- Laksono, B.M.; Grosserichter-Wagener, C.; de Vries, R.D.; Langeveld, S.A.G.; Brem, M.D.; van Dongen, J.J.M.; Katsikis, P.D.; Koopmans, M.P.G.; van Zelm, M.C.; de Swart, R.L. In Vitro Measles Virus Infection of Human Lymphocyte Subsets Demonstrates High Susceptibility and Permissiveness of both Naive and Memory B Cells. J. Virol. 2018, 28, e00131-18. [Google Scholar] [CrossRef]
- Griffin, D.E. Measles virus-induced suppression of immune responses. Immunol. Rev. 2010, 236, 176–189. [Google Scholar] [CrossRef] [PubMed]
- Drozdenko, T.S.; Dovgaluk, I.F. Vaccinal prevention of controlled infections in children with local forms of primary tuberculosis. Epidemiol. Vaccinal Prev. 2011, 4, 49–52. (In Russian) [Google Scholar]
- Yoo, K.H.; Jacobson, R.M.; Poland, G.A.; Weaver, A.; Lee, L.; Chang, T.; Juhn, Y.J. Asthma Status and Waning of Measles Antibody Concentrations after Measles Immunization. Pediatr. Infect. Dis. J. 2014, 33, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Avdonina, L.G.; Patyashina, M.A.; Isaeva, G.S.; Reshetnikova, I.D.; Tyurin, Y.A.; Kulikov, S.N.; Yuzlibaeva, L.R.; Gilyazutdinova, G.F.; Hakimov, N.M. Collective immunity to virus measles o medical workers and students of medical colleges in the republic of Tatarstan. Epidemiol. Vaccinal Prev. 2019, 18, 43–49. (In Russian) [Google Scholar] [CrossRef]
- Kostinov, M.P.; Filatov, N.N.; Zhuravlev, P.I.; Gladkova, L.S.; Polishchuk, V.B.; Shmit’ko, A.D.; Pakhomov, D.V.; Khromova, E.A.; Vasilyeva, G.V.; Tikhonova, I.A.; et al. Level of measles herd immunity assessed in hospital medical workers within a framework of the state measles elimination program. Russ. J. Infect. Immun. 2020, 10, 129–136. (In Russian) [Google Scholar] [CrossRef]
- Sarmometov, E.V.; Mokova, N.M.; Voldshmidt, N.B.; Sergevnin, V.I.; Tsvirkun, O.V.; Metelkina, N.A. Evaluation of measles immunity intensity among medical workers in the city of Perm. Epidemiol. Vaccinal Prev. 2011, 4, 45–48. (In Russian) [Google Scholar]
- Tkachenko, T.G.; Dmitriev, A.V.; Gudkov, R.A.; Fedina, N.V. Assessment of the state of anti-measles immunity in medicine personnel of a children’s hospital. Epidemiol. Vaccinal Prev. 2021, 20, 73–78. (In Russian) [Google Scholar] [CrossRef]
- Kostinov, M.P.; Zhuravlev, P.I.; Gladkova, L.S.; Mashilov, K.V.; Polishchuk, V.B.; Shmitko, A.D.; Zorina, V.N.; Blagovidov, D.A.; Pahomov, D.V.; Vlasenko, A.E.; et al. Comparative Analysis of the Measles Antibody Levels in Healthy Medical Personnel of Maternity Ward and Women in Labor. Front. Immunol. 2021, 12, 680506. [Google Scholar] [CrossRef]
- Sticchi, L.; Astengo, M.; Iavarone, I.G.; Icardi, G. Utility of serological screening for measles, mumps and rubella in immunocompromised patients. Hum. Vaccin. Immunother. 2019, 15, 2854–2855. [Google Scholar] [CrossRef]
- Marquis, S.R.; Logue, J.K.; Chu, H.Y.; Loeffelholz, T.; Quinn, Z.Z.; Liu, C.; Stewart, F.M.; Carpenter, P.A.; Pergam, S.A.; Krantz, E.M. Seroprevalence of Measles and Mumps Antibodies Among Individuals with Cancer. JAMA Netw. Open 2021, 4, e2118508. [Google Scholar] [CrossRef]
- Nozdracheva, A.V.; Semenenko, T.A. The status of herd immunity to measles in Russia: A systematic review and meta-analysis of epidemiological studies. J. Microbiol. Epidemiol. Immunobiol. 2020, 97, 445–456. [Google Scholar] [CrossRef]
- Tikhonova, N.T.; Ignateva, G.V.; Gerasimova, A.G.; Moskaleva, T.N.; Sadykova, D.K.; Tsvirkun, O.V.; Selezneva, T.S.; Titova, N.S.; Zargariants, A.I.; Mikheeva, I.V.; et al. Epidemiological Surveillance of Measles, Rubella and Mumps. Methodical Instructions; Federal Center for State Sanitary and Epidemiological Surveillance of the Ministry of Health of Russia: Moscow, Russia, 2003; p. 34. (In Russian)
- Smerdova, M.A.; Toptygina, A.P.; Andreev, Y.Y.; Sennikova, S.V.; Zetkin, A.Y.; Klykova, T.G.; Belyakov, S.I. Humoral and cellular immunity to measles and rubella virus antigens in healthy subjects. Russ. J. Infect. Immun. 2019, 9, 607–611. (In Russian) [Google Scholar] [CrossRef]
- Samoilovich, E.O.; Semeiko, G.V.; Yermalovich, M.A.; Glinskaya, I.N.; Vysotskaya, V.S. Population immunity to measles in the Republic of Belarus following long-standing vaccination. Epidemiol. Vaccinal Prev. 2020, 19, 43–50. (In Russian) [Google Scholar] [CrossRef]
- Friedrich, N.; Poethko-Müller, C.; Kuhnert, R.; Matysiak-Klose, D.; Koch, J.; Wichmann, O.; Santibanez, S.; Mankertz, A. Seroprevalence of Measles-, Mumps-, and Rubella-specific antibodies in the German adult population—Cross-sectional analysis of the German Health Interview and Examination Survey for Adults (DEGS1). Lancet Reg. Health Eur. 2021, 7, 100128. [Google Scholar] [CrossRef]
- Nasika, A.; Bogogiannidou, Z.; Mouchtouri, V.A.; Dadouli, K.; Kyritsi, M.A.; Vontas, A.; Voulgaridi, I.; Tsinaris, Z.; Kola, K.; Matziri, A.; et al. Measles Immunity Status of Greek Population after the Outbreak in 2017-2018: Results from a Seroprevalence National Survey. Vaccines 2023, 11, 1220. [Google Scholar] [CrossRef] [PubMed]
- Kostinov, M.P.; Filatov, N.N.; Zhuravlev, P.I.; Gladkova, L.S.; Polishchuk, V.B.; Shmit’ko, A.D.; Pakhomov, D.V.; Khromova, E.A.; Kostinova, A.M.; Vasil’yeva, G.V.; et al. Age-related immune response to measles virus in staff of a large city hospital. Russ. Pulmonol. J. 2018, 28, 701–707. (In Russian) [Google Scholar] [CrossRef]
- Štěpánek, L.; Nakládalová, M.; Boriková, A.; Horáková, D.; Štěpánek, L. Measles immunity in a Czech tertiary care hospital. Vaccine 2020, 38, 2889–2892. [Google Scholar] [CrossRef] [PubMed]
- Coppeta, L.; Pietroiusti, A.; Lieto, P.; Ferraro, M.; Grelli, S.; Stillo, M.; Magrini, A. Measles immunity in an Italian teaching hospital. Occup. Med. 2019, 69, 143–145. [Google Scholar] [CrossRef]
- Lin, M.Y.; Shao, H.H.; Tsou, M.T. Measles immunity in medical center staff after changes in national and local hospital vaccination policies. BMC Infect. Dis. 2022, 22, 427. [Google Scholar] [CrossRef]
- Lucca, A.; Bayoumi, N.; Ramanathan, L.V.; Sepkowitz, K.; Kamboj, M. Lower Rate of Seropositivity to Measles Among Young Healthcare Personnel in New York City. Clin. Infect. Dis. 2020, 71, 3241–3243. [Google Scholar] [CrossRef]
- Gardiner, A.; Liu, K.; Bonnichsen, M.; Joshi, V.; Davis, R.J.; Strasser, S.I. Immunity to Vaccine-preventable Viral Infections in Australians Being Evaluated for Liver Transplantation. Transplantation 2019, 103, 2318–2322. [Google Scholar] [CrossRef] [PubMed]
- Hostetler, H.P.; Neely, M.L.; Lydon, E.; Danziger-Isakov, L.A.; Todd, J.L.; Palmer, S.M. Immunity to varicella, measles, and mumps in patients evaluated for lung transplantation. Am. J. Transplant. 2021, 21, 2864–2870. [Google Scholar] [CrossRef] [PubMed]
- Rezahosseini, O.; Sørensen, S.S.; Perch, M.; Ekenberg, C.; Møller, D.L.; Knudsen, A.D.; Kirkby, N.; Lundgren, J.; Lodding, I.P.; Wareham, N.E.; et al. Measles, Mumps, Rubella, and Varicella Zoster Virus Serology and Infections in Solid Organ Transplant Recipients During the First Year Posttransplantation. Clin. Infect. Dis. 2021, 73, e3733–e3739. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Carlson, A.; Sirandas, B.; Clark, B.; Truax, C. Serologic evaluation of vaccine preventable infections and vaccination rates in kidney transplant candidates. Transpl. Infect. Dis. 2022, 24, e13973. [Google Scholar] [CrossRef] [PubMed]
- Zibolenová, J.; Hudečková, H.; Chladná, Z.; Malobická, E.; Novák, M.; Waczulíková, I.; Mikas, J.; Mečochová, A. Quantification of Waning Immunity After Measles Vaccination-Evidence from a Seroprevalence Study. Am. J. Epidemiol. 2023, 192, 1379–1385. [Google Scholar] [CrossRef]
- Bianchi, F.P.; Mascipinto, S.; Stefanizzi, P.; De Nitto, S.; Germinario, C.; Tafuri, S. Long-term immunogenicity after measles vaccine vs. wild infection: An Italian retrospective cohort study. Hum. Vaccin. Immunother. 2021, 17, 2078–2084. [Google Scholar] [CrossRef]
- Schulman, S.L.; Deforest, A.; Kaiser, B.A.; Polinsky, M.S.; Baluarte, H.J. Response to measles-mumps-rubella vaccine in children on dialysis. Pediatr. Nephrol. 1992, 6, 187–189. [Google Scholar] [CrossRef]
- Lakotkina, E.A.; Kharit, S.M.; Mironova, Z.G.; Freidlin, I.S.; Chernyaeva, T.V.; Kirilkina, T.A.; Smirnov, V.V.; Koval’skaya, S.Y.; Vaganov, P.D.; Martynova, M.I.; et al. Vaccination of Children with Impaired Health. In Guidelines for Doctors, 1st ed.; Kostinov, M.P., Ed.; Medicine for Everybody: Moscow, Russia, 1996; p. 78. (In Russian) [Google Scholar]
- Blagovidov, D.A.; Kostinov, M.P.; Simonova, O.I.; Shmit’ko, A.D.; Burkina, N.I.; Gorinova, Y.V.; Lazareva, A.V. Clinical effect of vaccination against P. aeruginosa in children with cystic fibrosis and lungs congenital malformations. J. Pediatr. Named G.N. Speransky 2017, 96, 150–158. (In Russian) [Google Scholar] [CrossRef]
- Borisova, V.N.; Bulgakova, V.A.; Vaneeva, N.P.; Kostinov, M.P.; Kusel’man, A.I.; Lavrov, V.F.; Lukachev, I.V.; Lukushkina, E.F.; Magarshak, O.O.; Malinovskaya, V.V.; et al. Immunomodulators and Vaccination; Kostinov, M.P., Solovyova, I.L., Eds.; 4Mpress: Moscow, Russia, 2013; p. 272. ISBN 978-5-905343-08-7. (In Russian) [Google Scholar]
- Kostinov, M.P.; Shmit’ko, A.D.; Solovyova, I.L.; Savisko, A.A.; Cherdantsev, A.P. Are children with allergic diseases and sickly children resistant to measles after revaccination? J. Pediatr. Named G.N. Speransky 2017, 96, 140–145. (In Russian) [Google Scholar] [CrossRef]
- Kharit, S.M.; Chernyaeva, T.V.; Voronina, O.L.; Monakhova, N.E.; Mukomolova, A.L. The use of immunotropic drugs in vaccination of frequently ill children against measles. Infect. Dis. 2008, 6, 73–77. (In Russian) [Google Scholar]
- Toptygina, A.; Semikina, E.; Alioshkin, V. Influence of an immunopotentiator Polyoxidonium on cytokine profile and antibody production in children vaccinated with Priorix. Arch. Physiol. Biochem. 2012, 118, 197–203. (In Russian) [Google Scholar] [CrossRef]
- Kharit, S.M.; Cherniaeva, T.V.; Cherniaeva, E.V.; Brusov, N.K. Vaccination of patients with oncology diseases against measles and mumps. Russ. J. Infect. Immun. 2011, 1, 85–91. (In Russian) [Google Scholar] [CrossRef]
- Fridman, I.V.; Kharit, S.M.; Chernyaeva, T.V.; Nacharova, Y.P.; Goleva, O.V. The application of recombinant interferon alpha-2 under vaccination with divalent vaccine against measles and epidemic parotitis in frequently ill children. Lechenie Profil. 2013, 4, 13–16. (In Russian) [Google Scholar]


 —Individual values.
—Individual values.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age Group | Anti-Measles IgG Ab, Me (Q1–Q3) | Distribution of Patients by Level of IgG Ab * | |||
|---|---|---|---|---|---|
| Seronegative | Low Ab Level | Moderate Ab Level | High Ab Level | ||
| Group 1 17–29 (n = 45) | 0.43 (0.094; 1.02) | 28.9 (16.4–44.4) | 44.4 (29.6–60) | 24.4 (12.9–39.5) | 2.2 (0.06–11.8) |
| Group 2 30–39 (n = 47) | 0.48 (0.15; 1.22) | 25.5 (13.9–40.4) | 38.3 (24.5–53.6) | 29.8 (17.3–44.9) | 6.4 (1.3–17.5) |
| Group 3 40–49 (n = 38) | 1.65 (0.65; 2.76) | 10.5 (2.9–24.8) | 23.7 (11.4–40.2) | 57.9 (40.8–73.7) | 7.9 (1.7–21.4) |
| Group 4 50 years and older (n = 27) | 2.71 (1.52; 4.3) | 3.7 (0.09–19) | 7.4 (0.9–24.3) | 81.5 (61.9–93.7) | 7.4 (0.9–24.3) |
| Comparison between age groups | H = 37.18, p < 0.001 | χ2 (3, N = 157) = 34.78, p < 0.0001 | |||
| p1–2 = 0.99 p1–3 < 0.001 p1–4 < 0.001 p2–3 = 0.017 p2–4 < 0.001 p3–4 = 0.119 | p1–4 = 0.021 p2–4 = 0.024 | p1–3 = 0.048 p1–4 < 0.001 p2–4 = 0.009 | p1–3 = 0.002 p1–4 < 0.001 p2–3 = 0.009 p2–4 < 0.001 | ||
| Patient Group | Anti-Measles IgG Ab, Me (Q1–Q3) | Distribution of Patients by Level of IgG Ab * | |||
|---|---|---|---|---|---|
| Seronegative | Low Ab Level | Moderate Ab Level | High Ab Level | ||
| Male (n = 79) | 1.02 (0.28; 1.99) | 16.5 (9.1–26.5) | 32.9 (22.7–44.4) | 45.6 (34.3–57.2) | 5.1 (1.4–12.5) |
| Female (n = 78) | 0.94 (0.25; 1.94) | 21.8 (13.2–32.6) | 29.5 (19.7–40.9) | 42.3 (31.2–54) | 6.4 (2.1–14.3) |
| Comparison | p = 0.78 | χ2 (1, N = 157) = 0.95, p = 0.81 | |||
| Age Group | Gender | p Level | ||
|---|---|---|---|---|
| Male | Female | |||
| Group 1 17–29 years old (n = 45) | IgG Ab level | 0.67 (0.24–1.41) | 0.26 (0.06–0.85) | p = 0.11 |
| n | 22 | 23 | ||
| Group 2 30–39 years old (n = 47) | IgG Ab level | 0.36 (0.08–1.1) | 0.69 (0.25–1.22) | p = 0.27 |
| n | 18 | 29 | ||
| Group 3 40–49 years old (n = 38) | IgG Ab level | 1.49 (0.3–2.3) | 1.7 (1.03–2.95) | p = 0.36 |
| n | 21 | 17 | ||
| Group 4 50 years and older (n = 27) | IgG Ab level | 2.4 (1.4–3.71) | 3.09 (1.88–4.3) | p = 0.5 |
| n | 18 | 9 | ||
| Comparison | p1–4 < 0.01 p2–4 < 0.001 | p1–3 < 0.01 p1–4 < 0.001 p2–4 < 0.01 | ||
| Age Group | Proportion of Seronegative Patients | p Level * | ||
|---|---|---|---|---|
| Male | Female | |||
| Group 1 17–29 years old (n = 45) | % | 13 (2.91–34.9) | 43.5 (21.5–69.2) | p = 0.047 |
| n/N | 3/22 | 10/23 | ||
| Group 2 30–39 years old (n = 47) | % | 33.3 (13.3–65.8) | 20.7 (8–39.7) | p = 0.49 |
| n/N | 6/18 | 6/29 | ||
| Group 3 40–49 years old (n = 38) | % | 14.3 (3–36.3) | 5.9 (0.1–28.7) | p = 0.61 |
| n/N | 3/21 | 1/17 | ||
| Group 4 50 years and older (n = 27) | % | 5.6 (0.1–27.3) | 0 (0–33.6) | p = 1.0 |
| n/N | 1/18 | 0/9 | ||
| Comparison | χ2 = 5.4844 p = 0.14 | p1–3 < 0.011 p 1–4 = 0.03 | ||
| Type of Disease | Age | Anti-Measles IgG Ab, Me (Q1-Q3) | Distribution of Patients by Level of IgG Ab * | |||
|---|---|---|---|---|---|---|
| Seronegative | Low Ab Level | Moderate Ab Level | High Ab Level | |||
| 1. Obstructive (n = 52) | 41 (32.5–47.5) | 1.22 (0.27–1.97) | 13.5 (5.6–25.8) | 32.7 (20.3–47.1) | 48.1 (34–62.5) | 5.8 (1.2–15.9) |
| 2. Vascular (n = 15) | 30 (20–35) | 0.66 (0.43–1.75) | 13.3 (1.7–40.5) | 40 (16.3–67.7) | 46.7 (21.3–73.4) | 0 (0–21.8) |
| 3. Cystic fibrosis (n = 32) | 26 (24–28) | 0.34 (0.08–0.97) | 34.4 (18.6–53.2) | 40.6 (23.7–59.4) | 21.9 (9.3–40) | 3.1 (0.08–16.2) |
| 4. Restrictive (n = 58) | 41 (32–50) | 0.98 (0.26–1.96) | 17.2 (8.6–29.4) | 22.4 (12.5–35.2) | 51.7 (38.2–65) | 8.6 (2.9–19) |
| Comparison | p1–2 < 0.049 p1–3 < 0.001 p2–4 < 0.0085 p3–4 < 0.001 | H = 12, p = 0.01 p1–3 < 0.024 p3–4 < 0.002 | p = 0.096 | p = 0.26 | p = 0.043 | p > 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Polishchuk, V.B.; Kostinov, M.P.; Ryzhov, A.A.; Karchevskaya, N.A.; Solov’eva, I.L.; Cherdantsev, A.P.; Kostinova, A.M.; Poddubikov, A.A. Characteristics of Anti-Measles Immunity in Lung Transplant Candidates. Viruses 2023, 15, 2121. https://doi.org/10.3390/v15102121
Polishchuk VB, Kostinov MP, Ryzhov AA, Karchevskaya NA, Solov’eva IL, Cherdantsev AP, Kostinova AM, Poddubikov AA. Characteristics of Anti-Measles Immunity in Lung Transplant Candidates. Viruses. 2023; 15(10):2121. https://doi.org/10.3390/v15102121
Chicago/Turabian StylePolishchuk, Valentina B., Mikhail P. Kostinov, Aleksey A. Ryzhov, Natalia A. Karchevskaya, Irina L. Solov’eva, Alexander P. Cherdantsev, Aristitsa M. Kostinova, and Arseniy A. Poddubikov. 2023. "Characteristics of Anti-Measles Immunity in Lung Transplant Candidates" Viruses 15, no. 10: 2121. https://doi.org/10.3390/v15102121