
Patterns of Circulating Cytokines and Vascular Markers’ Response in the Presence of COVID-19 in Kidney Transplant Recipients Compared with Non-Transplanted Patients
 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methods
2.1. Design Study, Population, and Setting
2.2. Outcomes
2.3. Blood Sampling and Plasma Detection of Circulating Mediators
2.4. Statistical Analysis
2.5. Principal Component Analysis
2.6. Correlation-Based Network (CBN) Analysis
3. Results
3.1. Baseline Characteristics and Outcomes
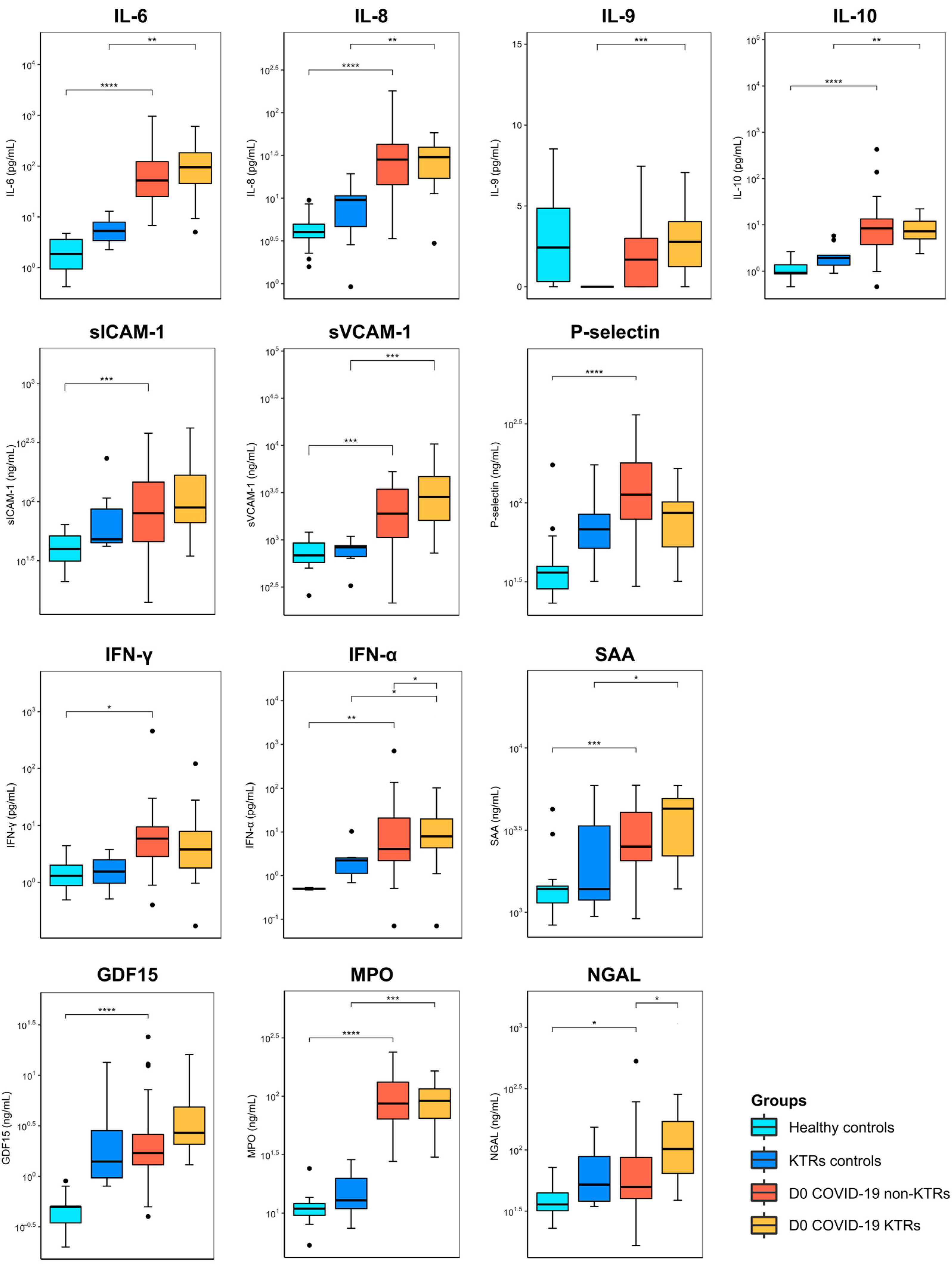
3.2. Cytokines and Vascular Mediators Stratified by the Baseline Condition
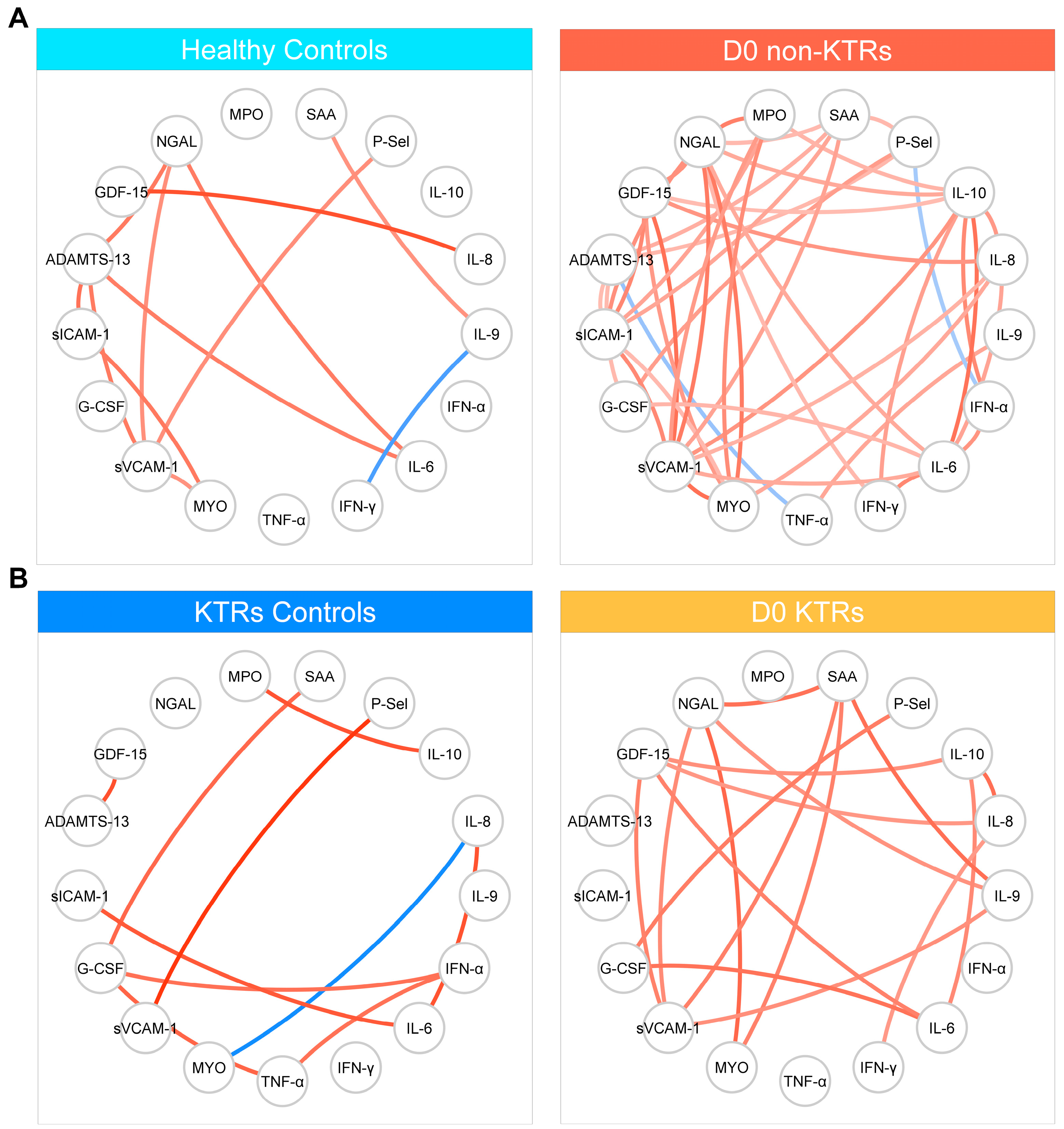
3.3. Correlation-Based Networks
3.4. Cytokines and Vascular Mediators Stratified by Clinical Progression to Critical Illness
3.5. Principal Component Analysis of Plasma Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- Wise, J. COVID-19: WHO declares end of global health emergency. BMJ 2023, 381, 1041. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Hamzaoui, M.; Lemee, V.; Lamulle, J.; Laurent, C.; Etienne, I.; Lemoine, M.; Lebourg, L.; Hanoy, M.; Le Roy, F.; et al. Antibody and T-cell response to a third dose of SARS-CoV-2 mRNA BNT162b2 vaccine in kidney transplant recipients. Kidney Int. 2021, 100, 1337–1340. [Google Scholar] [CrossRef]
- Callaghan, C.J.; Mumford, L.; Curtis, R.M.K.; Williams, S.V.; Whitaker, H.; Andrews, N.; Lopez Bernal, J.; Ushiro-Lumb, I.; Pettigrew, G.J.; Thorburn, D.; et al. Real-world Effectiveness of the Pfizer-BioNTech BNT162b2 and Oxford-AstraZeneca ChAdOx1-S Vaccines against SARS-CoV-2 in Solid Organ and Islet Transplant Recipients. Transplantation 2022, 106, 436. [Google Scholar] [CrossRef]
- Grupper, A.; Rabinowich, L.; Schwartz, D.; Schwartz, I.F.; Ben-Yehoyada, M.; Shashar, M.; Katchman, E.; Halperin, T.; Turner, D.; Goykhman, Y.; et al. Reduced humoral response to mRNA SARS-CoV-2 BNT162b2 vaccine in kidney transplant recipients without prior exposure to the virus. Am. J. Transplant. 2021, 21, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- Medina-Pestana, J.; Cristelli, M.P.; Foresto, R.D.; Tedesco-Silva, H.; Requiao-Moura, L.R. The Higher COVID-19 Fatality Rate Among Kidney Transplant Recipients Calls for Further Action. Transplantation 2022, 106, 908–910. [Google Scholar] [CrossRef]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. COVID-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef]
- Azzi, Y.; Bartash, R.; Scalea, J.; Loarte-Campos, P.; Akalin, E. COVID-19 and Solid Organ Transplantation: A Review Article. Transplantation 2021, 105, 37–55. [Google Scholar] [CrossRef] [PubMed]
- Cravedi, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Perez-Saez, M.J.; Redondo-Pachon, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020, 20, 3140–3148. [Google Scholar] [CrossRef]
- Requiao-Moura, L.R.; Sandes-Freitas, T.V.; Viana, L.A.; Cristelli, M.P.; Andrade, L.G.M.; Garcia, V.D.; Oliveira, C.M.C.; Esmeraldo, R.M.; Abbud Filho, M.; Pacheco-Silva, A.; et al. High mortality among kidney transplant recipients diagnosed with coronavirus disease 2019: Results from the Brazilian multicenter cohort study. PLoS ONE 2021, 16, e0254822. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Yang, Y.; Shen, C.; Li, J.; Yuan, J.; Wei, J.; Huang, F.; Wang, F.; Li, G.; Li, Y.; Xing, L.; et al. Plasma IP-10 and MCP-3 levels are highly associated with disease severity and predict the progression of COVID-19. J. Allergy Clin. Immunol. 2020, 146, 119–127.e114. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Yang, B.; Li, Q.; Wen, L.; Zhang, R. Clinical Features of 69 Cases With Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2020, 71, 769–777. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J.; Hlh Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Wang, B.; Mao, J. The pathogenesis and treatment of the ‘Cytokine Storm’ in COVID-19. J. Infect. 2020, 80, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Dolhnikoff, M.; Duarte-Neto, A.N.; de Almeida Monteiro, R.A.; da Silva, L.F.F.; de Oliveira, E.P.; Saldiva, P.H.N.; Mauad, T.; Negri, E.M. Pathological evidence of pulmonary thrombotic phenomena in severe COVID-19. J. Thromb. Haemost. 2020, 18, 1517–1519. [Google Scholar] [CrossRef]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Marshall, J.C. Such stuff as dreams are made on: Mediator-directed therapy in sepsis. Nat. Rev. Drug Discov. 2003, 2, 391–405. [Google Scholar] [CrossRef]
- Angus, D.C.; van der Poll, T. Severe sepsis and septic shock. N. Engl. J. Med. 2013, 369, 840–851. [Google Scholar] [CrossRef]
- Salomao, R.; Brunialti, M.K.; Rapozo, M.M.; Baggio-Zappia, G.L.; Galanos, C.; Freudenberg, M. Bacterial sensing, cell signaling, and modulation of the immune response during sepsis. Shock 2012, 38, 227–242. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H.; Connors, J.M.; Warkentin, T.E.; Thachil, J.; Levi, M. The unique characteristics of COVID-19 coagulopathy. Crit. Care 2020, 24, 360. [Google Scholar] [CrossRef]
- Syed, F.; Li, W.; Relich, R.F.; Russell, P.M.; Zhang, S.; Zimmerman, M.K.; Yu, Q. Excessive Matrix Metalloproteinase-1 and Hyperactivation of Endothelial Cells Occurred in COVID-19 Patients and Were Associated With the Severity of COVID-19. J. Infect. Dis. 2021, 224, 60–69. [Google Scholar] [CrossRef] [PubMed]
- Pecanha-Pietrobom, P.M.; Leite, G.G.F.; Hunter, J.; Ferreira, P.R.A.; Burattini, M.N.; Bellei, N.; Ota-Arakaki, J.S.; Salomao, R. The clinical course of hospitalized moderately ill COVID-19 patients is mirrored by routine hematologic tests and influenced by renal transplantation. PLoS ONE 2021, 16, e0258987. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. National Institutes of Health. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 1 August 2023).
- WHO. Clinical Management of COVID-19: Living Guideline, 15 September 2022. Available online: https://apps.who.int/iris/handle/10665/362783 (accessed on 1 August 2023).
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A software environment for integrated models of biomolecular interaction networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Leisman, D.E.; Ronner, L.; Pinotti, R.; Taylor, M.D.; Sinha, P.; Calfee, C.S.; Hirayama, A.V.; Mastroiani, F.; Turtle, C.J.; Harhay, M.O.; et al. Cytokine elevation in severe and critical COVID-19: A rapid systematic review, meta-analysis, and comparison with other inflammatory syndromes. Lancet Respir. Med. 2020, 8, 1233–1244. [Google Scholar] [CrossRef]
- D’Alessandro, A.; Thomas, T.; Dzieciatkowska, M.; Hill, R.C.; Francis, R.O.; Hudson, K.E.; Zimring, J.C.; Hod, E.A.; Spitalnik, S.L.; Hansen, K.C. Serum Proteomics in COVID-19 Patients: Altered Coagulation and Complement Status as a Function of IL-6 Level. J. Proteome Res. 2020, 19, 4417–4427. [Google Scholar] [CrossRef]
- Yong, S.J.; Halim, A.; Halim, M.; Liu, S.; Aljeldah, M.; Al Shammari, B.R.; Alwarthan, S.; Alhajri, M.; Alawfi, A.; Alshengeti, A.; et al. Inflammatory and vascular biomarkers in post-COVID-19 syndrome: A systematic review and meta-analysis of over 20 biomarkers. Rev. Med. Virol. 2023, 33, e2424. [Google Scholar] [CrossRef]
- Aird, W.C. Spatial and temporal dynamics of the endothelium. J. Thromb. Haemost. 2005, 3, 1392–1406. [Google Scholar] [CrossRef]
- Krieglstein, C.F.; Granger, D.N. Adhesion molecules and their role in vascular disease. Am J Hypertens 2001, 14, 44S–54S. [Google Scholar] [CrossRef]
- Adela, R.; Banerjee, S.K. GDF-15 as a Target and Biomarker for Diabetes and Cardiovascular Diseases: A Translational Prospective. J. Diabetes Res. 2015, 2015, 490842. [Google Scholar] [CrossRef]
- Wischhusen, J.; Melero, I.; Fridman, W.H. Growth/Differentiation Factor-15 (GDF-15): From Biomarker to Novel Targetable Immune Checkpoint. Front. Immunol. 2020, 11, 951. [Google Scholar] [CrossRef] [PubMed]
- Mazagova, M.; Buikema, H.; Landheer, S.W.; Vavrinec, P.; Buiten, A.; Henning, R.H.; Deelman, L.E. Growth differentiation factor 15 impairs aortic contractile and relaxing function through altered caveolar signaling of the endothelium. Am. J. Physiol. Heart Circ. Physiol. 2013, 304, H709–H718. [Google Scholar] [CrossRef] [PubMed]
- Pode Shakked, N.; de Oliveira, M.H.S.; Cheruiyot, I.; Benoit, J.L.; Plebani, M.; Lippi, G.; Benoit, S.W.; Henry, B.M. Early prediction of COVID-19-associated acute kidney injury: Are serum NGAL and serum Cystatin C levels better than serum creatinine? Clin. Biochem. 2022, 102, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Racovitan, D.; Hogeweg, M.; Doevelaar, A.A.; Seidel, M.; Rohn, B.; Bettag, S.; Rieckmann, S.; Babel, N.; Seibert, F.S.; Westhoff, T.H. Urinary biomarkers to predict acute kidney damage and mortality in COVID-19. Clin. Nephrol. 2023, 99, 161–171. [Google Scholar] [CrossRef]
- Chakraborty, S.; Kaur, S.; Guha, S.; Batra, S.K. The multifaceted roles of neutrophil gelatinase associated lipocalin (NGAL) in inflammation and cancer. Biochim. Biophys. Acta 2012, 1826, 129–169. [Google Scholar] [CrossRef] [PubMed]
- Romejko, K.; Markowska, M.; Niemczyk, S. The Review of Current Knowledge on Neutrophil Gelatinase-Associated Lipocalin (NGAL). Int. J. Mol. Sci. 2023, 24, 10470. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, S.P.J.; Bosio, E.; Neil, C.; Arendts, G.; Burrows, S.; Smart, L.; Brown, S.G.A.; Fatovich, D.M. Resistin and NGAL are associated with inflammatory response, endothelial activation and clinical outcomes in sepsis. Inflamm. Res. 2017, 66, 611–619. [Google Scholar] [CrossRef]
- Ebihara, T.; Matsumoto, H.; Matsubara, T.; Matsuura, H.; Hirose, T.; Shimizu, K.; Ogura, H.; Kang, S.; Tanaka, T.; Shimazu, T. Adipocytokine Profile Reveals Resistin Forming a Prognostic-Related Cytokine Network in the Acute Phase of Sepsis. Shock 2021, 56, 718–726. [Google Scholar] [CrossRef]
- Matsumoto, H.; Ogura, H.; Shimizu, K.; Ikeda, M.; Hirose, T.; Matsuura, H.; Kang, S.; Takahashi, K.; Tanaka, T.; Shimazu, T. The clinical importance of a cytokine network in the acute phase of sepsis. Sci. Rep. 2018, 8, 13995. [Google Scholar] [CrossRef]
- Pierrakos, C.; Vincent, J.L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef]
- Terpstra, M.L.; Aman, J.; van Nieuw Amerongen, G.P.; Groeneveld, A.B. Plasma biomarkers for acute respiratory distress syndrome: A systematic review and meta-analysis. Crit. Care Med. 2014, 42, 691–700. [Google Scholar] [CrossRef] [PubMed]
- Manion, M.; Andrade, B.B.; DerSimonian, R.; Gu, W.; Rupert, A.; Musselwhite, L.W.; Sierra-Madero, J.G.; Belaunzaran-Zamudio, P.F.; Sanne, I.; Lederman, M.M.; et al. Country of residence is associated with distinct inflammatory biomarker signatures in HIV-infected patients. J. Virus Erad. 2017, 3, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Vinhaes, C.L.; Cruz, L.A.B.; Menezes, R.C.; Carmo, T.A.; Arriaga, M.B.; Queiroz, A.T.L.; Barral-Netto, M.; Andrade, B.B. Chronic Hepatitis B Infection Is Associated with Increased Molecular Degree of Inflammatory Perturbation in Peripheral Blood. Viruses 2020, 12, 864. [Google Scholar] [CrossRef]
- Andrade, B.B.; Singh, A.; Narendran, G.; Schechter, M.E.; Nayak, K.; Subramanian, S.; Anbalagan, S.; Jensen, S.M.R.; Porter, B.O.; Antonelli, L.R.; et al. Mycobacterial Antigen Driven Activation of CD14++CD16− Monocytes Is a Predictor of Tuberculosis-Associated Immune Reconstitution Inflammatory Syndrome. PLOS Pathog. 2014, 10, e1004433. [Google Scholar] [CrossRef] [PubMed]
- Vinhaes, C.L.; Oliveira-de-Souza, D.; Silveira-Mattos, P.S.; Nogueira, B.; Shi, R.; Wei, W.; Yuan, X.; Zhang, G.; Cai, Y.; Barry, C.E.; et al. Changes in inflammatory protein and lipid mediator profiles persist after antitubercular treatment of pulmonary and extrapulmonary tuberculosis: A prospective cohort study. Cytokine 2019, 123, 154759. [Google Scholar] [CrossRef]
- Mendonça, V.R.R.; Queiroz, A.T.L.; Lopes, F.M.; Andrade, B.B.; Barral-Netto, M. Networking the host immune response in Plasmodium vivax malaria. Malar. J. 2013, 12, 69. [Google Scholar] [CrossRef]
- Vinhaes, C.L.; Arriaga, M.B.; de Almeida, B.L.; Oliveira, J.V.; Santos, C.S.; Calcagno, J.I.; Carvalho, T.X.; Giovanetti, M.; Alcantara, L.C.J.; de Siqueira, I.C.; et al. Newborns With Zika Virus-Associated Microcephaly Exhibit Marked Systemic Inflammatory Imbalance. J. Infect. Dis. 2020, 222, 670–680. [Google Scholar] [CrossRef]
- Bandopadhyay, P.; D’Rozario, R.; Lahiri, A.; Sarif, J.; Ray, Y.; Paul, S.R.; Roy, R.; Maiti, R.; Chaudhuri, K.; Bagchi, S.; et al. Nature and Dimensions of Systemic Hyperinflammation and its Attenuation by Convalescent Plasma in Severe COVID-19. J. Infect. Dis. 2021, 224, 565–574. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, D.; Hou, J.; Li, H.; Cao, D.; Guo, M.; Ling, Y.; Gao, M.; Zhou, Y.; Wan, Y.; et al. An inter-correlated cytokine network identified at the center of cytokine storm predicted COVID-19 prognosis. Cytokine 2021, 138, 155365. [Google Scholar] [CrossRef]
- Young, B.E.; Ong, S.W.X.; Ng, L.F.P.; Anderson, D.E.; Chia, W.N.; Chia, P.Y.; Ang, L.W.; Mak, T.M.; Kalimuddin, S.; Chai, L.Y.A.; et al. Viral Dynamics and Immune Correlates of Coronavirus Disease 2019 (COVID-19) Severity. Clin. Infect. Dis. 2021, 73, e2932–e2942. [Google Scholar] [CrossRef] [PubMed]
- Schuurman, A.R.; Reijnders, T.D.Y.; van Engelen, T.S.R.; Leopold, V.; de Brabander, J.; van Linge, C.; Schinkel, M.; Pereverzeva, L.; Haak, B.W.; Brands, X.; et al. The host response in different aetiologies of community-acquired pneumonia. EBioMedicine 2022, 81, 104082. [Google Scholar] [CrossRef] [PubMed]
- Peters-Sengers, H.; Butler, J.M.; Uhel, F.; Schultz, M.J.; Bonten, M.J.; Cremer, O.L.; Scicluna, B.P.; van Vught, L.A.; van der Poll, T.; consortium, M. Source-specific host response and outcomes in critically ill patients with sepsis: A prospective cohort study. Intensive Care Med. 2022, 48, 92–102. [Google Scholar] [CrossRef] [PubMed]
- de Sandes-Freitas, T.V.; de Andrade, L.G.M.; Moura, L.R.R.; Cristelli, M.P.; Medina-Pestana, J.O.; Lugon, J.R.; Sesso, R.; Brazilian COVID-19 Dialysis Investigators; COVID-19-KT Brazilian Study Group. Comparison of 30-day case-fatality rate between dialysis and transplant COVID-19 patients: A propensity score matched cohort study. J. Nephrol. 2022, 35, 131–141. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mediators | Methods |
|---|---|
| IL-6 | Cytometric Bead Array (CBA) Flex Set kits |
| IL-8 | The samples were analyzed in LSRFortessa (BD Biosciences, San Jose, CA, USA) |
| IL-9 | |
| IL-10 | |
| Granulocyte colony-stimulating factor (G-CSF) | |
| Tumor necrosis factor alpha (TNF-α) | |
| Interferon alpha (IFN-α) | |
| Interferon gamma (IFN-γ) | |
| Disintegrin and metalloproteinase with thrombospondin motifs 13 (ADAMTS-13) | Cytometry (MAGPIX® Instrument, Luminex Corporation, Austin, TX, USA) |
| Growth/differentiation factor 15 (GDF-15) | Milliplex Map Human Cardiovascular Disease kit Magnetic Bead Panel 2 Cardiovascular Disease Multiplex Assay (Temecula, CA, USA) |
| Myoglobin (MYO) | |
| Soluble intercellular adhesion molecule 1 (sICAM-1) | |
| Myeloperoxidase (MPO) | |
| P-selectin (P-Sel) | |
| Neutrophil gelatinase-associated lipocalin (NGAL) | |
| Soluble circulating vascular cell adhesion molecule 1 (sVCAM-1) | |
| Serum amyloid A (SAA) |
| Variables | KTRs (N = 20) | Non-KTRs (N = 47) | p-Value |
|---|---|---|---|
| Demography | |||
| Male sex, n (%) | 12 (60%) | 30 (64%) | 0.98 |
| Age, median (IQR) | 55.3 (48.9, 60.6) | 62.7 (51.2, 67.1) | 0.11 |
| Comorbidities | |||
| Charlson index, median (IQR) | 4.0 (2.0, 5.0) | 3.0 (1.0, 5.0) | 0.14 |
| Cardiac disease, n (%) | 1 (5.0%) | 12 (25%) | 0.30 |
| Chronic pulmonary disease, n (%) | 0 (0%) | 9 (19%) | 0.08 |
| Diabetes, n (%) | 7 (35%) | 19 (40%) | 0.80 |
| Chronic kidney disease, n (%) | 20 (100%) | 4 (8.5%) | <0.0001 |
| Hypertension, n (%) | 16 (80%) | 26 (55%) | 0.10 |
| Obesity, n (%) | 1 (5.0%) | 7 (15%) | 0.46 |
| Admission Data | |||
| Day of symptoms, median (IQR) | 7.0 (5.0, 9.7) | 7.0 (5.0, 9.0) | 0.93 |
| Fever, n (%) | 16 (80%) | 31 (66%) | 0.30 |
| Cough, n (%) | 14 (70%) | 35 (74%) | 0.90 |
| Shortness of breath, n (%) | 15 (75%) | 30 (64%) | 0.50 |
| Diarrhea, n (%) | 7 (35%) | 13 (28%) | 0.75 |
| Temperature (°C), median (IQR) | 36.4 (36.0, 37.2) | 36.6 (36.0, 37.8) | 0.49 |
| Cardiac rate, bpm | 80.0 (78.5, 86.5) | 86.0 (78.0, 99.0) | 0.23 |
| Respiratory rate, bpm | 24.0 (20.0, 26.0) | 24.0 (20.0, 26.0) | 0.74 |
| SpO2, median of % | 91.3 (89.2, 94.1) | 90.7 (88.9, 93.0) | 0.46 |
| BMI, Kg/m2 | 26.0 (23.4, 27.7) | 27.7 (24.4, 32.5) | 0.07 |
| SOFA score | 2.0 (2.0, 4.0) | 1.0 (0.0, 2.2) | 0.01 |
| Laboratory Admission, Median (IQR) | |||
| Lymphocytes, cells/μL | 599.5 (375.2, 906.2) | 997.0 (720.0, 1312.0) | 0.01 |
| Neutrophils, cells/μL | 4647.0 (3918.0, 6901.0) | 4668.0 (3577.5, 7072.5) | 0.77 |
| Monocytes, cells/μL | 407.5 (149.2, 460.8) | 294.0 (225.5, 497.0) | 0.83 |
| Neutrophil–lymphocyte ratio | 7.3 (5.0, 11.6) | 4.8 (3.8, 8.7) | 0.09 |
| Platelets, cells/μL | 190,500 (153,000 238,500) | 190,000 (153,500, 233,500) | 0.94 |
| Hemoglobin, g/dL | 12.4 (11.6, 13.1) | 13.4 (12.4, 14.6) | 0.02 |
| Hematocrit, median of % | 38.1 (35.7, 39.7) | 40.0 (36.2, 43.2) | 0.08 |
| Creatinine, mg/dL | 1.9 (1.4, 2.3) | 0.9 (0.7, 1.1) | <0.0001 |
| C-reactive protein, mg/L | 103.5 (63.2, 164.5) | 81.9 (57.2, 152.1) | 0.71 |
| Lactate, mg/dL | 14.0 (10.0, 19.0) | 12.0 (10.0, 18.0) | 0.92 |
| D-dimer, μg/mL | 1.0 (0.6, 1.7) | 1.2 (0.7, 2.5) | 0.48 |
| Troponin, ng/L | 19.5 (17.0, 35.0) | 8.0 (5.5, 23.0) | 0.03 |
| Outcomes | |||
| Hospital days, median (IQR) | 14.5 (9.8, 26.0) | 8.0 (5.0, 15.0) | 0.02 |
| Severe, n (%) | 10 (50%) | 13 (28%) | 0.10 |
| Mortality, n (%) | 8 (40%) | 4 (8.5%) | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brunialti, M.K.C.; Leite, G.G.F.; Eburneo, G.S.; de Araujo, O.R.; Peçanha-Pietrobom, P.M.; Ferreira, P.R.A.; Bellei, N.C.J.; Arakaki, J.S.O.; Medina-Pestana, J.; Requião-Moura, L.; et al. Patterns of Circulating Cytokines and Vascular Markers’ Response in the Presence of COVID-19 in Kidney Transplant Recipients Compared with Non-Transplanted Patients. Viruses 2023, 15, 2166. https://doi.org/10.3390/v15112166
Brunialti MKC, Leite GGF, Eburneo GS, de Araujo OR, Peçanha-Pietrobom PM, Ferreira PRA, Bellei NCJ, Arakaki JSO, Medina-Pestana J, Requião-Moura L, et al. Patterns of Circulating Cytokines and Vascular Markers’ Response in the Presence of COVID-19 in Kidney Transplant Recipients Compared with Non-Transplanted Patients. Viruses. 2023; 15(11):2166. https://doi.org/10.3390/v15112166
Chicago/Turabian StyleBrunialti, Milena Karina Coló, Giuseppe G. F. Leite, Gabriela Strafolino Eburneo, Orlei Ribeiro de Araujo, Paula M. Peçanha-Pietrobom, Paulo Roberto Abrão Ferreira, Nancy C. Junqueira Bellei, Jaquelina Sonoe Ota Arakaki, José Medina-Pestana, Lúcio Requião-Moura, and et al. 2023. "Patterns of Circulating Cytokines and Vascular Markers’ Response in the Presence of COVID-19 in Kidney Transplant Recipients Compared with Non-Transplanted Patients" Viruses 15, no. 11: 2166. https://doi.org/10.3390/v15112166