
Establishment of Outbreak Thresholds for Hepatitis A in South Africa Using Laboratory Surveillance, 2017–2020


Abstract
:1. Introduction
2. Methods
3. Results
3.1. Hepatitis A Positivity, Incidence, and Testing Rates
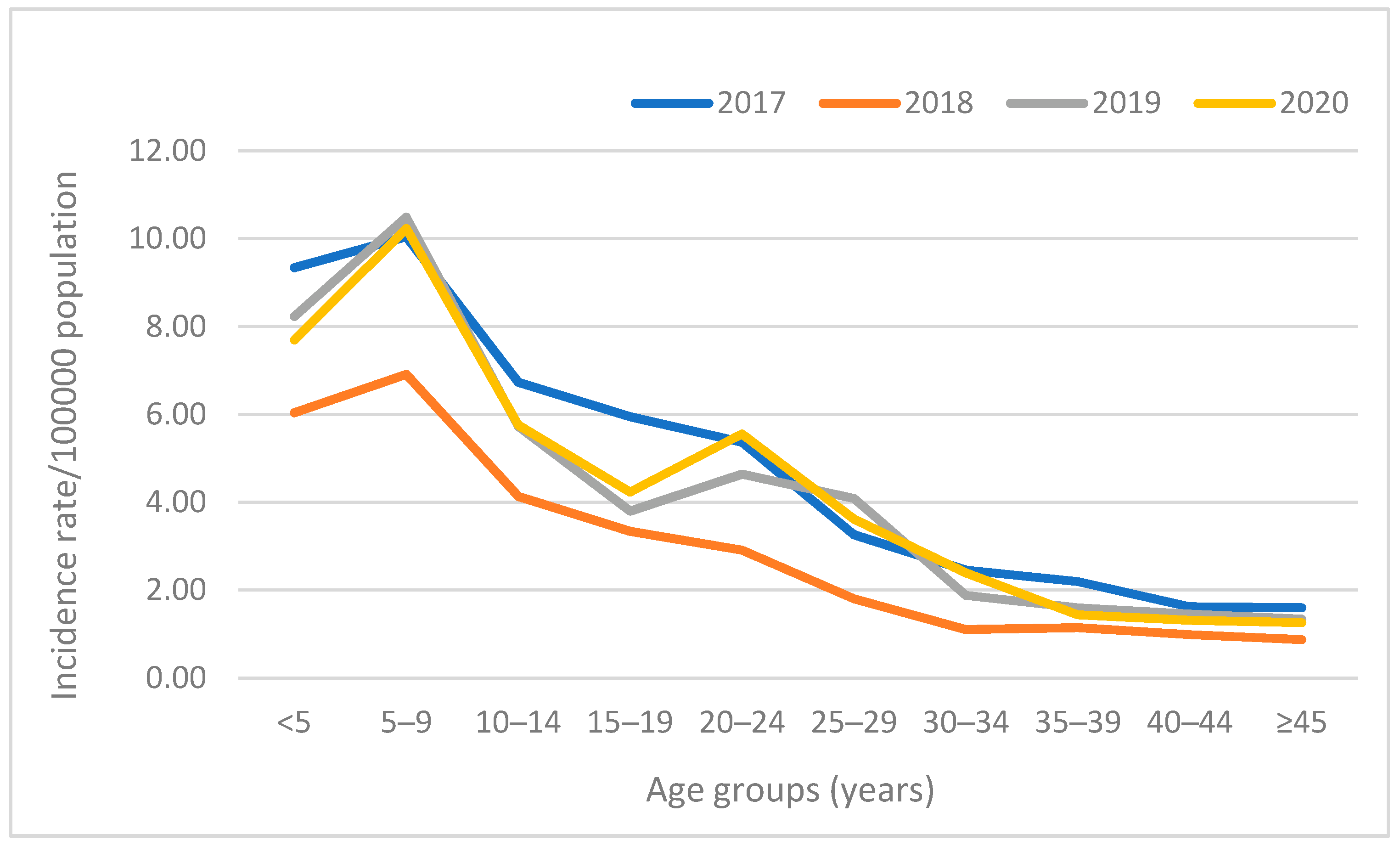
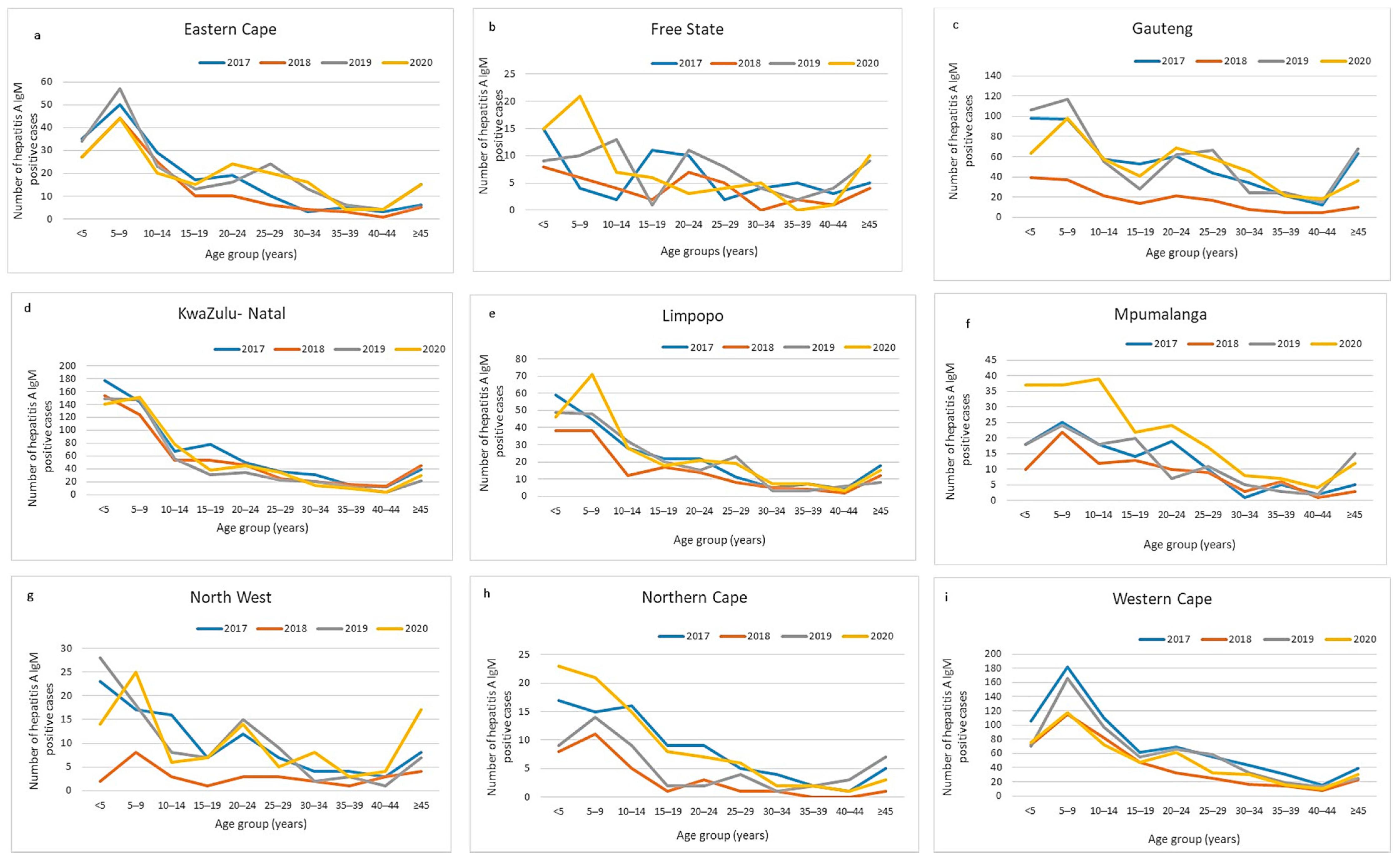
3.2. Hepatitis A Incidence by Age Distribution and by Province
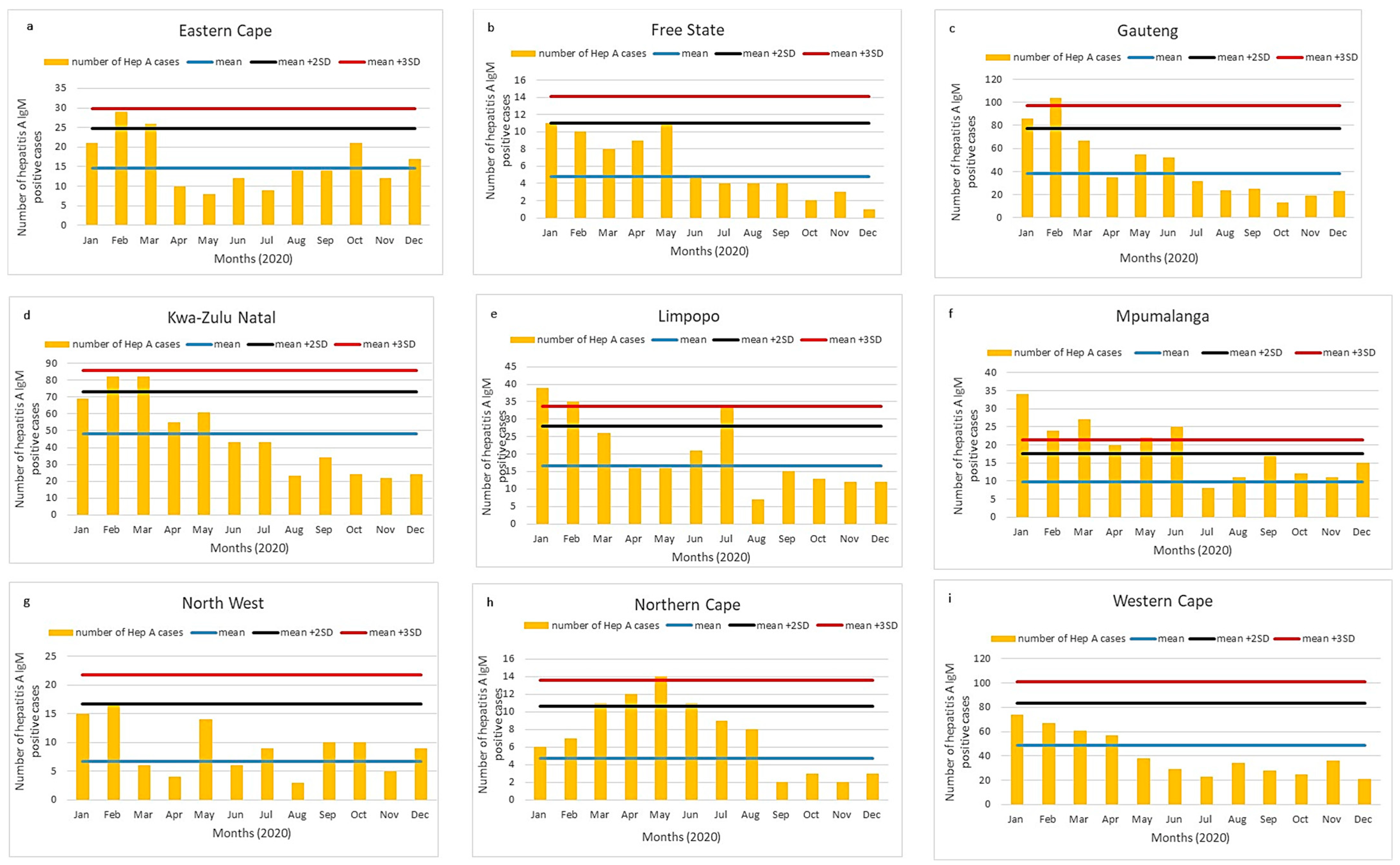
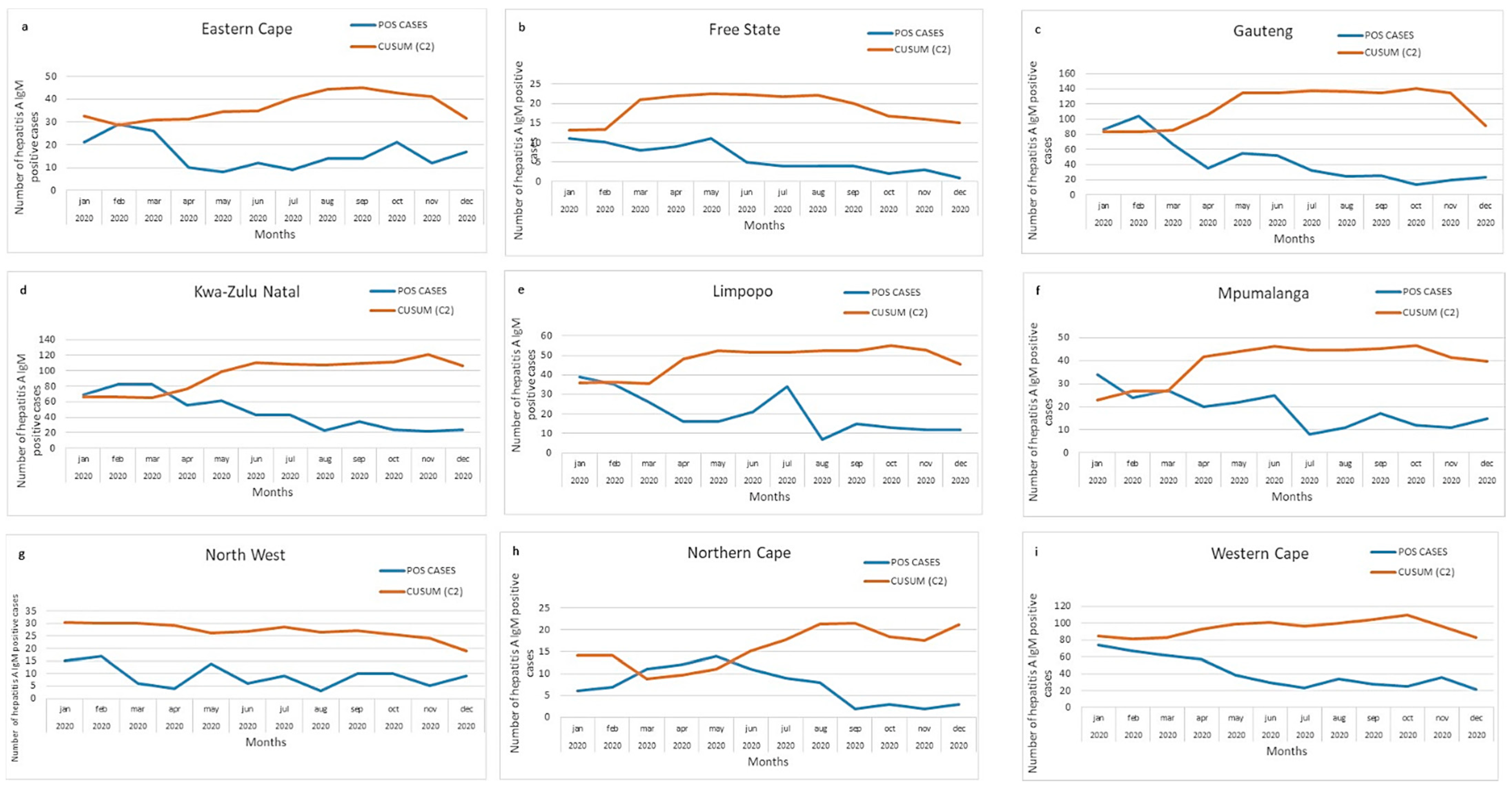
3.3. Provincial Hepatitis A Incidence Thresholds
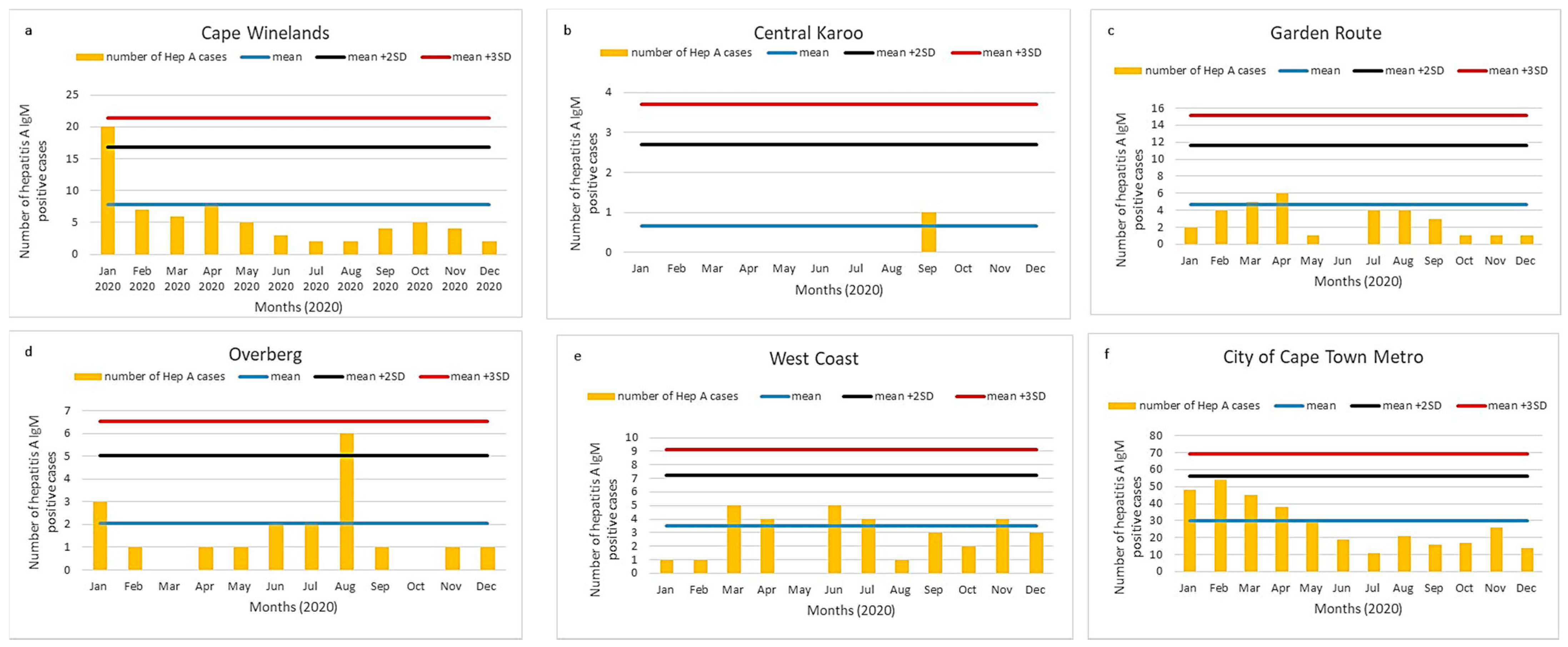
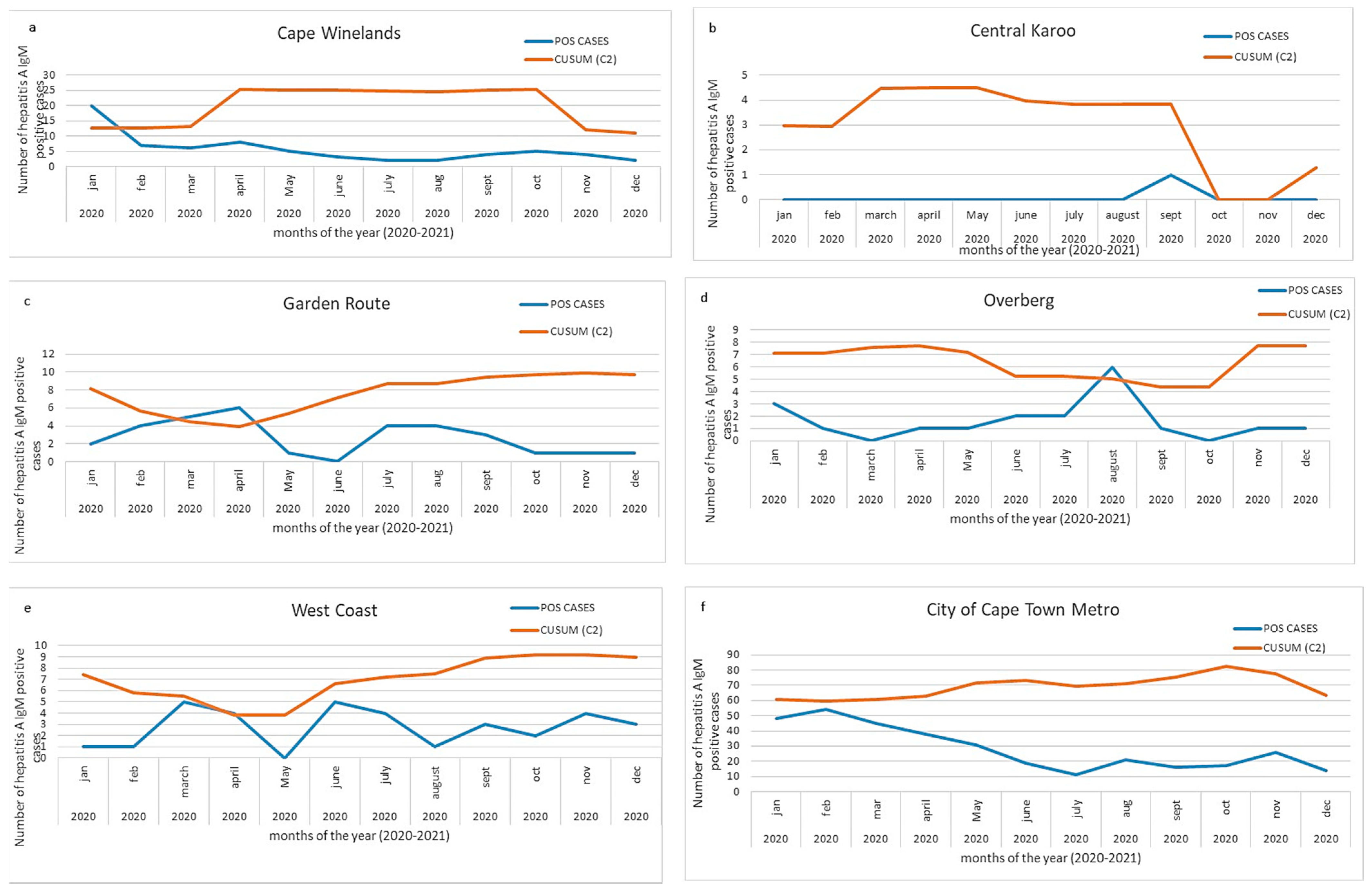
3.4. District Hepatitis A Incidence Thresholds
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pan American Health Organization of the World Health Organization. Plan of Action for the Prevention and Control of Viral Hepatitis. Available online: https://www.paho.org/hq/dmdocuments/2016/2016-cha-plan-action-prev-hep-en.pdf (accessed on 25 November 2021).
- Foster, M.A.; Haber, P.; Nelson, N.P. Chapter 9: Hepatitis A. In Epidemiology and Prevention of Vaccine-Preventable Disease. Available online: https://www.cdc.gov/vaccines/pubs/pinkbook/hepa.html (accessed on 1 March 2020).
- World Health Organization (WHO). WHO Position Paper on Hepatitis A Vaccines. Available online: http://www.who.int/wer (accessed on 1 April 2020).
- Jefferies, M.; Rauff, B.; Rashid, H.; Lam, T.; Rafiq, S. Update on global epidemiology of viral hepatitis and preventive strategies. World J. Clin. Cases 2018, 6, 589–599. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Hepatitis A. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-a (accessed on 25 November 2021).
- Foster, M.; Ramachandran, S.; Myatt, K.; Donovan, D.; Bohm, S.; Fiedler, J.; Barbeau, B.; Collins, J.; Thoroughman, D.; McDonald, E.; et al. Hepatitis A Virus Outbreaks Associated with Drug Use and Homelessness California, Kentucky, Michigan, and Utah, 2017. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 1208–1210. [Google Scholar] [CrossRef] [PubMed]
- Charre, C.; Ramiere, C.; Roque-Afonso, A.M.; Chidiac, C.; Zoulim, F.; Godinot, M.; Koffi, R.; Scholtès, C.; Livrozet, J.-M.; HAV Lyon Study Group; et al. Hepatitis A outbreak in HIV-infected MSM and in PrEP-using MSM despite a high level of immunity, Lyon, France, January to June 2017. Eurosurveillance 2017, 22, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazanderani, A.H.; Motaze, N.V.; McCarthy, K.; Suchard, M.; du Plessis, N.M. Hepatitis A virus seroprevalence in South Africa–Estimates using routine laboratory data, 2005–2015. PLoS ONE 2019, 14, 216033. [Google Scholar] [CrossRef]
- Amayeza Information Services. The What, Why and When of Childhood Vaccination in South Africa—2019. Available online: http://www.amayeza-info.co.za/wp-content/uploads/2018/08/2018-schedule-updated.pdf (accessed on 20 March 2021).
- Western Cape Provincial Epidemiology Team. Preliminary Report–Hepatitis A Outbreak, Investigation and Response. Villiersdorp, Overberg, Western Cape, 2020; Unpublished work.
- O’Brien, S.J.; Christie, P. Do CuSums have a role in routine communicable disease surveillance? Public Health 1997, 111, 255–258. [Google Scholar] [CrossRef]
- Hutwagner, L.; Thompson, W.; Seeman, G.M.T.T. The Bioterrorism Preparedness and Response Early Aberration Reporting System (EARS). J. Urban Health 2003, 80, i89–i96. [Google Scholar] [PubMed]
- Zhou, H.; Burkom, H.; Strine, T.W.; Katz, S.; Jajosky, R.; Anderson, W.A.U. Comparing the historical limits method with regression models for weekly monitoring of national notifiable diseases reports. J. Biomed. Inform. 2017, 76, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Watkins, R.E.; Eagleson, S.; Veenendaal, B.; Wright, G.; Plant, A.J. Applying cusum-based methods for the detection of outbreaks of Ross River virus disease in Western Australia. BMC Med. Inform. Decis. Mak. 2008, 8, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutwagner, L.C.; Thompson, W.W.; Seeman, G.M.; Treadwell, T. A simulation model for assessing aberration detection methods used in public health surveillance for systems with limited baselines. Stat. Med. 2005, 24, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.Z.D.; Yan, P. Infectious Disease Informatics. In Syndromic Surveillance for Public Health EARS and Biodefense, Intergrated Series in Information Systems; Springer Science and Business Media: Berlin/Heidelberg, Germany, 2010; pp. 167–170. [Google Scholar]
- Stern, L. A Practical Algorithm for the Detection of Clusters in Sparse Epidemiological Data. Available online: http://citeseerx.ist.psu.edu/viewdoc/summary?doi=10.1.1.43.6658 (accessed on 22 March 2021).
- Vega, T.; Lozano, J.E.; Meerhoff, T.; Snacken, R.; Mott, J.; Ortiz de Lejarazu, R.; Nunes, B. Influenza surveillance in Europe: Establishing epidemic thresholds by the Moving Epidemic Method. Influenza Other Respi. Viruses 2013, 7, 546–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, R.; Jiang, Y.; Michael, E.; Zhao, G. How to select a proper early warning threshold to detect infectious disease outbreaks based on the China infectious disease automated alert and response system (CIDARS). BMC Public Health 2017, 17, 570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics South Africa. Stats South Africa Mid-Year Population Estimates 2017. Available online: https://www.statssa.gov.za/publications/P0302/P03022017.pdf (accessed on 1 March 2020).
- Statistics South Africa. Stats South Africa Mid-Year Population Estimates 2018. Available online: https://www.statssa.gov.za/publications/P0302/P03022018.pdf (accessed on 1 March 2020).
- Statistics South Africa. Midyear Population Estimate 2019. Available online: https://www.statssa.gov.za/publications/P0302/P03022019.pdf (accessed on 1 March 2020).
- Statistics South Africa. Stats South Africa Mid-Year Population Estimates 2020. Available online: https://www.statssa.gov.za/publications/P0302/P03022020.pdf (accessed on 1 March 2020).
- South African Human Rights Commission. Report on the Right to Access Sufficient Water and Decent Sanitation in South Africa: 2014. Available online: https://www.gov.za/sites/default/files/gcis_document/201409/reportrightaccesswatersanitation2014a.pdf (accessed on 23 October 2021).
- Statistics South Africa. General Household Survey: 2019. Available online: http://www.ncbi.nlm.nih.gov/pubmed/11469378 (accessed on 20 March 2021).
- Socio- Economic Rights Institute of South Africa (SERI) Informal Settlements and Human Rights in South Africa. Available online: https://www.ohchr.org/Documents/Issues/Housing/InformalSettlements/SERI.pdf (accessed on 20 August 2021).
- Shakespear, M. Unpacking Water and Sanitation Access in South Africa: A Renewed Call for More Action. 2020. Available online: https://www.tips.org.za/research-archive/inequality-and-economic-inclusion/inequality-and-economic-inclusion/item/download/1843_6142986b7de6729c7f47178f5215a83b (accessed on 23 October 2021).
- Sun, X.; Wang, F.; Zheng, H.; Miao, N.; Yuan, Q.; Cui, F.; Yin, Z.; Zhang, G.; Levine, H. The impact of expanded program on immunization with live attenuated and inactivated Hepatitis A vaccines in China, 2004–2016. Vaccine 2018, 36, 1279–1284. [Google Scholar] [CrossRef] [PubMed]
- de Almeida e Araújo, D.C.; de Oliveira, J.M.; Haddad, S.K.; da Roza, D.L.; de Oliveira Bottino, F.; Faria, S.B.S.C.; Bellíssimo-Rodrigues, F.; Passos, A.D.C. Declining prevalence of hepatitis A and silent circulation of hepatitis E virus infection in southeastern Brazil. Int. J. Infect. Dis. 2020, 101, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Singh, S.; Kolhapure, S.; Hoet, B.; Arankalle, V.; Mitra, M. Increasing Burden of Hepatitis A in Adolescents and Adults and the Need for Long-Term Protection: A Review from the Indian Subcontinent. Infect. Dis. Ther. 2019, 8, 483–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobsen, K. Hepatitis A virus in West Africa: Is an epidemiological transition beginning? Niger. Med. J. 2014, 55, 279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, J.; Abdullahi, L.; Hussey, G.D.; Muloiwa, R.; Kagina, B.M. A systematic review of the epidemiology of hepatitis A in Africa. BMC Infect. Dis. 2019, 19, 651. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L. The Use and Impacts of a Corporate Data Warehouse: The Case of the National Health Laboratory Service. 2018. Available online: https://hdl.handle.net/10539/26811 (accessed on 20 August 2021).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2017 | ||||||
| Province in South Africa | Population (Mid-Year) | Hep A IgM Tests | Hep A IgM Pos | Positivity Rate (%) | Testing Rate/100,000 | Incidence Rate/100,000 |
| Eastern Cape | 6,498,700 | 15,247 | 178 | 1.17 | 234.62 | 2.74 |
| Free State | 2,866,700 | 4333 | 61 | 1.41 | 151.15 | 2.13 |
| Gauteng | 14,278,700 | 40,653 | 583 | 1.43 | 284.71 | 4.08 |
| KwaZulu-Natal | 11,074,800 | 38,721 | 665 | 1.72 | 349.63 | 6.00 |
| Limpopo | 5,778,400 | 10,112 | 226 | 2.23 | 175.00 | 3.91 |
| Mpumalanga | 4,444,200 | 13,664 | 128 | 0.94 | 307.46 | 2.88 |
| North West | 1,214,000 | 6398 | 105 | 1.64 | 527.02 | 8.65 |
| Northern Cape | 3,856,200 | 4090 | 84 | 2.05 | 106.06 | 2.18 |
| Western Cape | 6,510,300 | 10,368 | 711 | 6.86 | 159.26 | 10.92 |
| Total | 56,521,900 | 143,586 | 2741 | 1.91 | 254.04 | 4.85 |
| 2018 | ||||||
| Eastern Cape | 6,522,700 | 8871 | 136 | 1.53 | 136.00 | 2.09 |
| Free State | 2,954,300 | 2090 | 40 | 1.91 | 70.74 | 1.35 |
| Gauteng | 14,717,000 | 14,079 | 188 | 1.34 | 95.66 | 1.28 |
| KwaZulu-Natal | 11,384,700 | 37,827 | 564 | 1.49 | 332.26 | 4.95 |
| Limpopo | 5,797,300 | 6629 | 156 | 2.35 | 114.35 | 2.69 |
| Mpumalanga | 4,523,900 | 7717 | 92 | 1.19 | 170.58 | 2.03 |
| North West | 3,979,000 | 3625 | 30 | 0.83 | 91.10 | 0.75 |
| Northern Cape | 1,225,600 | 1432 | 32 | 2.23 | 116.84 | 2.61 |
| Western Cape | 6,621,100 | 5163 | 434 | 8.41 | 77.98 | 6.55 |
| Total | 57,725,600 | 87,433 | 1672 | 1.91 | 151.46 | 2.90 |
| 2019 | ||||||
| Eastern Cape | 6,712,276 | 12,350 | 211 | 1.71 | 183.99 | 3.14 |
| Free State | 2,887,465 | 4618 | 71 | 1.54 | 159.93 | 2.46 |
| Gauteng | 15,176,115 | 37,552 | 615 | 1.64 | 247.44 | 4.05 |
| KwaZulu-Natal | 11,289,086 | 33,792 | 509 | 1.51 | 299.33 | 4.51 |
| Limpopo | 5,982,584 | 10,149 | 213 | 2.10 | 169.64 | 3.56 |
| Mpumalanga | 4,592,187 | 9544 | 134 | 1.40 | 207.83 | 2.92 |
| North West | 4,027,160 | 7379 | 104 | 1.41 | 183.23 | 2.58 |
| Northern Cape | 1,263,875 | 3769 | 54 | 1.43 | 298.21 | 4.27 |
| Western Cape | 6,844,272 | 10,453 | 602 | 5.76 | 152.73 | 8.80 |
| Total | 58,775,020 | 129,606 | 2513 | 1.94 | 220.51 | 4.28 |
| 2020 | ||||||
| Eastern Cape | 6,734,001 | 11,377 | 193 | 1.70 | 168.95 | 2.87 |
| Free State | 2,928,903 | 4409 | 72 | 1.63 | 150.53 | 2.46 |
| Gauteng | 15,488,137 | 32,847 | 535 | 1.63 | 212.08 | 3.45 |
| KwaZulu-Natal | 11,531,628 | 30628 | 562 | 1.83 | 265.60 | 4.87 |
| Limpopo | 5,852,553 | 9830 | 246 | 2.50 | 167.96 | 4.20 |
| Mpumalanga | 4,679,786 | 10,361 | 226 | 2.18 | 221.40 | 4.83 |
| North West | 4,108,816 | 6155 | 108 | 1.75 | 149.80 | 2.63 |
| Northern Cape | 1,292,786 | 3340 | 88 | 2.63 | 258.36 | 6.81 |
| Western Cape | 7,005,741 | 9726 | 493 | 5.07 | 138.83 | 7.04 |
| Total | 59,622,351 | 118,673 | 2523 | 2.13 | 199.04 | 4.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prabdial-Sing, N.; Motaze, V.; Manamela, J.; McCarthy, K.; Suchard, M. Establishment of Outbreak Thresholds for Hepatitis A in South Africa Using Laboratory Surveillance, 2017–2020. Viruses 2021, 13, 2470. https://doi.org/10.3390/v13122470
Prabdial-Sing N, Motaze V, Manamela J, McCarthy K, Suchard M. Establishment of Outbreak Thresholds for Hepatitis A in South Africa Using Laboratory Surveillance, 2017–2020. Viruses. 2021; 13(12):2470. https://doi.org/10.3390/v13122470
Chicago/Turabian StylePrabdial-Sing, Nishi, Villyen Motaze, Jack Manamela, Kerrigan McCarthy, and Melinda Suchard. 2021. "Establishment of Outbreak Thresholds for Hepatitis A in South Africa Using Laboratory Surveillance, 2017–2020" Viruses 13, no. 12: 2470. https://doi.org/10.3390/v13122470