
Towards Integrated Management of Dengue in Mumbai

 , and
, and 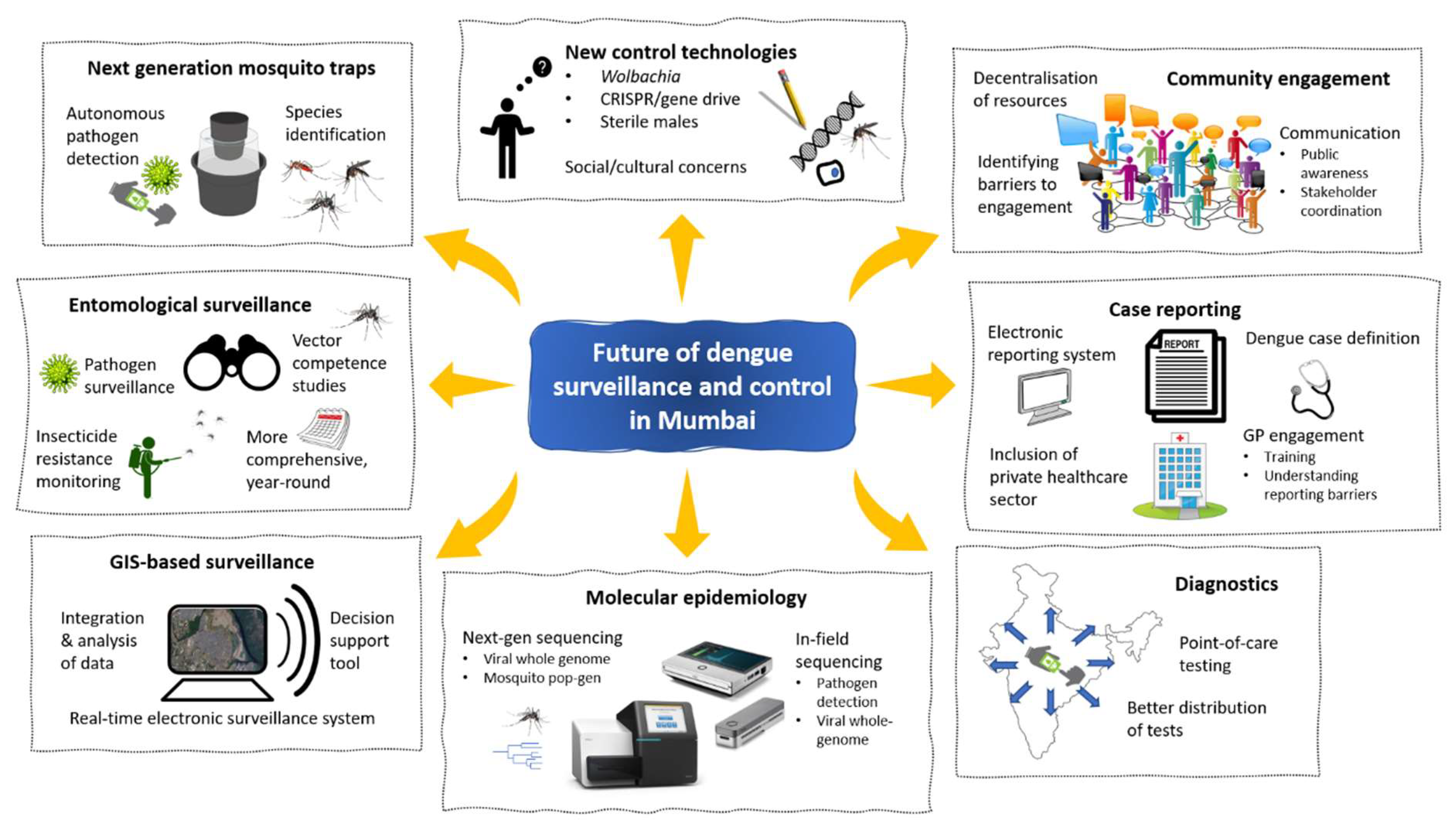{kind=link}
Abstract
:1. Introduction
2. Dengue Burden in India
3. Dengue Surveillance in India
4. Dengue in Mumbai
5. Future of Dengue Surveillance and Control in Mumbai
5.1. Improvement in Dengue Case Reporting
5.2. Supporting Dengue Diagnostics
5.3. Improved Entomological Surveillance
5.4. Use of Novel Mosquito Traps for Surveillance
5.5. Molecular Epidemiology to Support Surveillance
5.6. Use of Geographic Information System (GIS)-Based Surveillance
5.7. Improved Community Engagement and Response
5.8. Use of Novel Technologies for Mosquito Control and Transmission Prevention
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gubler, D.J. The Global Threat of Emergent/Re-Emergent Vector-Borne Diseases. In Vector Biology, Ecology and Control; Atkinson, P.W., Ed.; Springer: Dordrecht, The Netherlands, 2010; pp. 39–62. ISBN 978-90-481-2458-9. [Google Scholar]
- International Catalogue of Arboviruses, including Certain Other Viruses of Vertebrates, 3rd ed.; Karabatsos, N.; Rockefeller Foundation; American Committee on Arthropod-Borne Viruses; American Society of Tropical Medicine and Hygiene (Eds.) American Society of Tropical Medicine and Hygiene for the Subcommittee on Information Exchange of the American Committee on Arthropod-Borne Viruses: San Antonio, TX, USA, 1985. [Google Scholar]
- World Malaria Report 2020. Available online: https://www.who.int/publications-detail-redirect/9789240015791 (accessed on 13 September 2021).
- Brady, O.J.; Gething, P.W.; Bhatt, S.; Messina, J.P.; Brownstein, J.S.; Hoen, A.G.; Moyes, C.L.; Farlow, A.W.; Scott, T.W.; Hay, S.I. Refining the Global Spatial Limits of Dengue Virus Transmission by Evidence-Based Consensus. PLoS Negl. Trop. Dis. 2012, 6, e1760. [Google Scholar] [CrossRef]
- Murray, N.E.A.; Quam, M.B.; Wilder-Smith, A. Epidemiology of Dengue: Past, Present and Future Prospects. Clin. Epidemiol. 2013, 5, 299–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gubler, D.J. Dengue, Urbanization and Globalization: The Unholy Trinity of the 21st Century. Trop. Med. Health 2011, 39, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The Global Distribution and Burden of Dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.P.; Tuladhar, R.; Kurmi, R.; Manandhar, K.D. Dengue Periodic Outbreaks and Epidemiological Trends in Nepal. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 6. [Google Scholar] [CrossRef] [Green Version]
- Cummings, D.A.T.; Irizarry, R.A.; Huang, N.E.; Endy, T.P.; Nisalak, A.; Ungchusak, K.; Burke, D.S. Travelling Waves in the Occurrence of Dengue Haemorrhagic Fever in Thailand. Nature 2004, 427, 344–347. [Google Scholar] [CrossRef]
- Gubler, D.J. Dengue and Dengue Hemorrhagic Fever. Clin. Microbiol. Rev. 1998, 11, 480–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johansson, M.A.; Dominici, F.; Glass, G.E. Local and Global Effects of Climate on Dengue Transmission in Puerto Rico. PLoS Negl. Trop. Dis. 2009, 3, e382. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.C.; Twiddy, S.S. The Origin, Emergence and Evolutionary Genetics of Dengue Virus. Infect. Genet. Evol. 2003, 3, 19–28. [Google Scholar] [CrossRef]
- Vasilakis, N.; Weaver, S.C. Chapter 1 The History and Evolution of Human Dengue Emergence. In Advances in Virus Research; Academic Press: Cambridge, MA, USA, 2008; Volume 72, pp. 1–76. [Google Scholar]
- Halstead, S.B.; Chow, J.S.; Marchette, N.J. Immunological Enhancement of Dengue Virus Replication. Nat. New Biol. 1973, 243, 24–26. [Google Scholar]
- World Health Organization. Regional Office for South-East Asia. In Comprehensive Guideline for Prevention and Control of Dengue and Dengue Haemorrhagic Fever; Revised and Expanded Edition; WHO Regional Office for South-East Asia: New Delhi, India, 2011; ISBN 978-92-9022-387-0. [Google Scholar]
- Phakhounthong, K.; Chaovalit, P.; Jittamala, P.; Blacksell, S.D.; Carter, M.J.; Turner, P.; Chheng, K.; Sona, S.; Kumar, V.; Day, N.P.J.; et al. Predicting the Severity of Dengue Fever in Children on Admission Based on Clinical Features and Laboratory Indicators: Application of Classification Tree Analysis. BMC Pediatr. 2018, 18, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duong, V.; Lambrechts, L.; Paul, R.E.; Ly, S.; Lay, R.S.; Long, K.C.; Huy, R.; Tarantola, A.; Scott, T.W.; Sakuntabhai, A.; et al. Asymptomatic Humans Transmit Dengue Virus to Mosquitoes. Proc. Natl. Acad. Sci. USA 2015, 112, 14688–14693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reich, N.G.; Shrestha, S.; King, A.A.; Rohani, P.; Lessler, J.; Kalayanarooj, S.; Yoon, I.-K.; Gibbons, R.V.; Burke, D.S.; Cummings, D.A.T. Interactions between Serotypes of Dengue Highlight Epidemiological Impact of Cross-Immunity. J. R. Soc. Interface 2013, 10, 20130414. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, R.V.; Kalanarooj, S.; Jarman, R.G.; Nisalak, A.; Vaughn, D.W.; Endy, T.P.; Mammen, M.P.; Srikiatkhachorn, A. Analysis of Repeat Hospital Admissions for Dengue to Estimate the Frequency of Third or Fourth Dengue Infections Resulting in Admissions and Dengue Hemorrhagic Fever, and Serotype Sequences. Am. J. Trop. Med. Hyg. 2007, 77, 910–913. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bournazos, S.; Gupta, A.; Ravetch, J.V. The Role of IgG Fc Receptors in Antibody-Dependent Enhancement. Nat. Rev. Immunol. 2020, 20, 633–643. [Google Scholar] [CrossRef]
- Halstead, S.B.; O’rourke, E.J. Antibody-Enhanced Dengue Virus Infection in Primate Leukocytes. Nature 1977, 265, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Vaddadi, K.; Gandikota, C.; Jain, P.K.; Prasad, V.S.V.; Venkataramana, M. Co-Circulation and Co-Infections of All Dengue Virus Serotypes in Hyderabad, India 2014. Epidemiol. Infect. 2017, 145, 2563–2574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinodkumar, C.S.; Kalapannavar, N.K.; Basavarajappa, K.G.; Sanjay, D.; Gowli, C.; Nadig, N.G.; Prasad, B.S. Episode of Coexisting Infections with Multiple Dengue Virus Serotypes in Central Karnataka, India. J. Infect. Public Health 2013, 6, 302–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, S.J.; Yoon, I.-K. A Review of Dengvaxia®: Development to Deployment. Hum. Vaccine Immunother. 2019, 15, 2295–2314. [Google Scholar] [CrossRef] [Green Version]
- Halstead, S.B. Safety Issues from a Phase 3 Clinical Trial of a Live-Attenuated Chimeric Yellow Fever Tetravalent Dengue Vaccine. Hum. Vaccine Immunother. 2018, 14, 2158–2162. [Google Scholar] [CrossRef] [Green Version]
- Dengue Vaccine: WHO Position Paper, September 2018–Recommendations. Vaccine 2019, 37, 4848–4849. [CrossRef]
- Reinhold, J.M.; Lazzari, C.R.; Lahondère, C. Effects of the Environmental Temperature on Aedes Aegypti and Aedes Albopictus Mosquitoes: A Review. Insects 2018, 9, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, R.; Xu, L.; Bjørnstad, O.N.; Liu, K.; Song, T.; Chen, A.; Xu, B.; Liu, Q.; Stenseth, N.C. Climate-Driven Variation in Mosquito Density Predicts the Spatiotemporal Dynamics of Dengue. Proc. Natl. Acad. Sci. USA 2019, 116, 3624–3629. [Google Scholar] [CrossRef] [Green Version]
- Gan, S.J.; Leong, Y.Q.; bin Barhanuddin, M.F.H.; Wong, S.T.; Wong, S.F.; Mak, J.W.; Ahmad, R.B. Dengue Fever and Insecticide Resistance in Aedes Mosquitoes in Southeast Asia: A Review. Parasites Vectors 2021, 14, 315. [Google Scholar] [CrossRef] [PubMed]
- Moyes, C.L.; Vontas, J.; Martins, A.J.; Ng, L.C.; Koou, S.Y.; Dusfour, I.; Raghavendra, K.; Pinto, J.; Corbel, V.; David, J.-P.; et al. Contemporary Status of Insecticide Resistance in the Major Aedes Vectors of Arboviruses Infecting Humans. PLoS Negl. Trop. Dis. 2017, 11, e0005625. [Google Scholar] [CrossRef]
- Ranson, H.; Burhani, J.; Lumjuan, N.; Black, W.C.I. Insecticide Resistance in Dengue Vectors. TropIKA.net 2010, 1. Available online: https://archive.lstmed.ac.uk/999/ (accessed on 3 December 2021).
- Vontas, J.; Kioulos, E.; Pavlidi, N.; Morou, E.; della Torre, A.; Ranson, H. Insecticide Resistance in the Major Dengue Vectors Aedes Albopictus and Aedes Aegypti. Pestic. Biochem. Physiol. 2012, 104, 126–131. [Google Scholar] [CrossRef]
- Walshe, D.P.; Garner, P.; Adeel, A.A.; Pyke, G.H.; Burkot, T.R. Larvivorous Fish for Preventing Malaria Transmission. Cochrane Database Syst. Rev. 2017, 2017, CD008090. [Google Scholar] [CrossRef] [Green Version]
- Accoti, A.; Engdahl, C.S.; Dimopoulos, G. Discovery of Novel Entomopathogenic Fungi for Mosquito-Borne Disease Control. Front. Fungal Biol. 2021, 2, 28. [Google Scholar] [CrossRef]
- Niu, G.; Wang, B.; Zhang, G.; King, J.B.; Cichewicz, R.H.; Li, J. Targeting Mosquito FREP1 with a Fungal Metabolite Blocks Malaria Transmission. Sci. Rep. 2015, 5, 14694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, A.A.; Montgomery, B.L.; Popovici, J.; Iturbe-Ormaetxe, I.; Johnson, P.H.; Muzzi, F.; Greenfield, M.; Durkan, M.; Leong, Y.S.; Dong, Y.; et al. Successful Establishment of Wolbachia in Aedes Populations to Suppress Dengue Transmission. Nature 2011, 476, 454–457. [Google Scholar] [CrossRef]
- Thomas, D.D.; Donnelly, C.A.; Wood, R.J.; Alphey, L.S. Insect Population Control Using a Dominant, Repressible, Lethal Genetic System. Science 2000, 287, 2474–2476. [Google Scholar] [CrossRef] [PubMed]
- Windbichler, N.; Papathanos, P.A.; Crisanti, A. Targeting the X Chromosome during Spermatogenesis Induces Y Chromosome Transmission Ratio Distortion and Early Dominant Embryo Lethality in Anopheles Gambiae. PLoS Genet. 2008, 4, e1000291. [Google Scholar] [CrossRef] [Green Version]
- Pham, T.B.; Phong, C.H.; Bennett, J.B.; Hwang, K.; Jasinskiene, N.; Parker, K.; Stillinger, D.; Marshall, J.M.; Carballar-Lejarazú, R.; James, A.A. Experimental Population Modification of the Malaria Vector Mosquito, Anopheles Stephensi. PLoS Genet. 2019, 15, e1008440. [Google Scholar] [CrossRef] [PubMed]
- Buchman, A.; Gamez, S.; Li, M.; Antoshechkin, I.; Li, H.-H.; Wang, H.-W.; Chen, C.-H.; Klein, M.J.; Duchemin, J.-B.; Crowe, J.E., Jr.; et al. Broad Dengue Neutralization in Mosquitoes Expressing an Engineered Antibody. PLoS Pathog. 2020, 16, e1008103. [Google Scholar] [CrossRef] [Green Version]
- Buchman, A.; Gamez, S.; Li, M.; Antoshechkin, I.; Li, H.-H.; Wang, H.-W.; Chen, C.-H.; Klein, M.J.; Duchemin, J.-B.; Paradkar, P.N.; et al. Engineered Resistance to Zika Virus in Transgenic Aedes Aegypti Expressing a Polycistronic Cluster of Synthetic Small RNAs. Proc. Natl. Acad. Sci. USA 2019, 116, 3656–3661. [Google Scholar] [CrossRef] [Green Version]
- Wilder-Smith, A.; Rupali, P. Estimating the Dengue Burden in India. Lancet Glob. Health 2019, 7, e988–e989. [Google Scholar] [CrossRef] [Green Version]
- Chakravarti, A.; Arora, R.; Luxemburger, C. Fifty Years of Dengue in India. Trans. R. Soc. Trop. Med. Hyg. 2012, 106, 273–282. [Google Scholar] [CrossRef]
- Kakkar, M. Dengue Fever Is Massively Under-Reported in India, Hampering Our Response. BMJ 2012, 345, e8574. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Sarfraz, A.; Jaiswal, N.; Das, P. Impediments of Reporting Dengue Cases in India. J. Infect. Public Health 2017, 10, 494–498. [Google Scholar] [CrossRef]
- Mutheneni, S.R.; Morse, A.P.; Caminade, C.; Upadhyayula, S.M. Dengue Burden in India: Recent Trends and Importance of Climatic Parameters. Emerg. Microbes Infect. 2017, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Oki, M.; Yamamoto, T. Climate Change, Population Immunity, and Hyperendemicity in the Transmission Threshold of Dengue. PLoS ONE 2012, 7, e48258. [Google Scholar] [CrossRef] [Green Version]
- Dwivedi, A.; Khire, M.V. Application of Split- Window Algorithm to Study Urban Heat Island Effect in Mumbai through Land Surface Temperature Approach. Sustain. Cities Soc. 2018, 41, 865–877. [Google Scholar] [CrossRef]
- Mehrotra, S.; Bardhan, R.; Ramamritham, K. Urban Informal Housing and Surface Urban Heat Island Intensity: Exploring Spatial Association in the City of Mumbai. Environ. Urban. ASIA 2018, 9, 158–177. [Google Scholar] [CrossRef]
- Knudsen, A.B.; Slooff, R. Vector-Borne Disease Problems in Rapid Urbanization: New Approaches to Vector Control. Bull. World Health Organ. 1992, 70, 1. [Google Scholar]
- DENGUE/DHF SITUATION IN INDIA: National Vector Borne Disease Control Programme (NVBDCP). Available online: https://nvbdcp.gov.in/index4.php?lang=1&level=0&linkid=431&lid=3715 (accessed on 15 September 2021).
- Pilot, E.; Murthy, G.V.S.; Nittas, V. Understanding India’s Urban Dengue Surveillance: A Qualitative Policy Analysis of Hyderabad District. Glob. Public Health 2020, 15, 1702–1717. [Google Scholar] [CrossRef] [PubMed]
- Modi, A.; Vaishnav, K.G.; Pandya, R.C.; Sahu, G.C.; Naik, A. Urban Dengue Surveillance over Sixteen Years: Integration, Trend Analysis and Participation of Private Medical Sector. J. Commun. Dis. 2018, 50, 52–59. [Google Scholar] [CrossRef]
- Shepard, D.S.; Halasa, Y.A.; Tyagi, B.K.; Adhish, S.V.; Nandan, D.; Karthiga, K.S.; Chellaswamy, V.; Gaba, M.; Arora, N.K. Economic and Disease Burden of Dengue Illness in India. Am. J. Trop. Med. Hyg. 2014, 91, 1235–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Srivastava, S.; Jain, A.; Chaturvedi, U.C. Dengue in India. Indian J. Med. Res. 2012, 136, 373–390. [Google Scholar]
- Messina, J.P.; Brady, O.J.; Scott, T.W.; Zou, C.; Pigott, D.M.; Duda, K.A.; Bhatt, S.; Katzelnick, L.; Howes, R.E.; Battle, K.E.; et al. Global Spread of Dengue Virus Types: Mapping the 70 Year History. Trends Microbiol. 2014, 22, 138–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, A.; Abdullah, M.; Tazeen, A.; Naqvi, I.H.; Kazim, S.N.; Ahmed, A.; Alamery, S.F.; Malik, A.; Parveen, S. Circulation of Dengue Virus Serotypes in Hyperendemic Region of New Delhi, India during 2011–2017. J. Infect. Public Health 2020, 13, 1912–1919. [Google Scholar] [CrossRef]
- Rao, T.R. Distribution, Density and Seasonal Prevalence of Aedes Aegypti in the Indian Subcontinent and South-East Asia. Bull. World Health Organ. 1967, 36, 547–551. [Google Scholar]
- Singh, R.K.; Singh, S. Prevalence of Aedes Mosquitoes during the First Outbreak of Zika in Jaipur City, India. J. Commun. Dis. 2019, 51, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Vijayakumar, K.; Kumar, T.K.S.; Nujum, Z.T.; Umarul, F.; Kuriakose, A. A Study on Container Breeding Mosquitoes with Special Reference to Aedes (Stegomyia) Aegypti and Aedes Albopictus in Thiruvananthapuram District, India. J. Vector Borne Dis. 2014, 51, 27. [Google Scholar] [PubMed]
- Gilotra, S.K.; Rozeboom, L.E.; Bhattacharya, N.C. Observations on Possible Competitive Displacement between Populations of Aedes Aegypti Linnaeus and Aedes Albopictus Skuse in Calcutta. Bull. World Health Organ. 1967, 37, 437–446. [Google Scholar]
- Tikar, S.N.; Mendki, M.J.; Chandel, K.; Parashar, B.D.; Prakash, S. Susceptibility of Immature Stages of Aedes (Stegomyia) Aegypti; Vector of Dengue and Chikungunya to Insecticides from India. Parasitol. Res. 2008, 102, 907. [Google Scholar] [CrossRef]
- Tikar, S.N.; Mendki, M.J.; Sharma, A.K.; Sukumaran, D.; Veer, V.; Prakash, S.; Parashar, B.D. Resistance Status of the Malaria Vector Mosquitoes, Anopheles Stephensi and Anopheles Subpictus Towards Adulticides and Larvicides in Arid and Semi-Arid Areas of India. J. Insect Sci. 2011, 11, 85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mani, T.R.; Arunachalam, N.; Rajendran, R.; Satyanarayana, K.; Dash, A.P. Efficacy of Thermal Fog Application of Deltacide, a Synergized Mixture of Pyrethroids, against Aedes Aegypti, the Vector of Dengue. Trop. Med. Int. Health 2005, 10, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Shastri, J.; Williamson, M.; Vaidya, N.; Agrawal, S.; Shrivastav, O. Nine Year Trends of Dengue Virus Infection in Mumbai, Western India. J. Lab. Physicians 2017, 9, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Guidelines: National Vector Borne Disease Control Programme (NVBDCP). Available online: https://nvbdcp.gov.in/index1.php?lang=1&level=1&sublinkid=5851&lid=3686 (accessed on 16 September 2021).
- Chinnakali, P.; Gurnani, N.; Upadhyay, R.P.; Parmar, K.; Suri, T.M.; Yadav, K. High Level of Awareness but Poor Practices Regarding Dengue Fever Control: A Cross-Sectional Study from North India. N. Am. J. Med. Sci. 2012, 4, 278. [Google Scholar] [CrossRef]
- Quarterly Dengue Surveillance Data. Available online: https://www.nea.gov.sg/dengue-zika/dengue/quarterly-dengue-surveillance-data (accessed on 30 November 2021).
- Indonesia Ministry of Health. Dengue Data January–December 2020; Kementrian Kesehatan: Jakarta, Indonesia, 2020. [Google Scholar]
- Thailand Reports 71,000 Dengue Cases in 2020-Outbreak News Today. Available online: http://outbreaknewstoday.com/thailand-reports-71000-dengue-cases-in-2020/ (accessed on 30 November 2021).
- Dengue Update. Available online: https://www.epid.gov.lk/web/index.php?option=com_content&view=article&id=171%3Adengue-update&catid=51%3Amessage-for-public&Itemid=487&lang=en (accessed on 30 November 2021).
- Bagcchi, S. Dengue Surveillance Poor in India. Lancet 2015, 386, 1228. [Google Scholar] [CrossRef]
- Daudé, É.; Mazumdar, S. Combating Dengue in India: Challenges and Strategies. Econ. Political Wkly. 2016, 51, 77. [Google Scholar]
- 4, LABORATORY DIAGNOSIS AND DIAGNOSTIC TESTS. In Dengue: Guidelines for Diagnosis, Treatment, Prevention and Control: New Edition; World Health Organization: Geneva, Switzerland, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK143156/ (accessed on 3 December 2021).
- Yow, K.-S.; Aik, J.; Tan, E.Y.-M.; Ng, L.-C.; Lai, Y.-L. Rapid Diagnostic Tests for the Detection of Recent Dengue Infections: An Evaluation of Six Kits on Clinical Specimens. PLoS ONE 2021, 16, e0249602. [Google Scholar] [CrossRef] [PubMed]
- Felix, A.C.; Souza, N.C.S.; Figueiredo, W.M.; Costa, A.A.; Inenami, M.; da Silva, R.M.G.; Levi, J.E.; Pannuti, C.S.; Romano, C.M. Cross Reactivity of Commercial Anti-Dengue Immunoassays in Patients with Acute Zika Virus Infection. J. Med. Virol. 2017, 89, 1477–1479. [Google Scholar] [CrossRef]
- Garg, A.; Garg, J.; Singh, D.V.; Dhole, T. Can Rapid Dengue Diagnostic Kits Be Trusted? A Comparative Study of Commercially Available Rapid Kits for Serodiagnosis of Dengue Fever. J. Lab. Physicians 2019, 11, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Kalra, N.L.; Kaul, S.M.; Rastogi, R.M. Prevalence of Aedes Aegypti and Aedes Albopictus-Vectors of Dengue Haemorrhagic Fever in North, North-East and Central India. Dengue Bulletin. 1997, 21, 84. [Google Scholar]
- Fulmali, P.V.; Walimbe, A.; Mahadev, P.V.M. Spread, Establishment & Prevalence of Dengue Vector Aedes Aegypti (L.) in Konkan Region, Maharashtra, India. Indian J. Med. Res. 2006, 127, 589. [Google Scholar]
- Gill, K.S.; Rahman, S.J.; Datta, K.K.; Kumar, K.; Katyal, R. Larval Indices of Aedes Aegypti at Air and Sea Ports of Mumbai, India. Dengue Bulletin. 1996, 20, 71. [Google Scholar]
- Rajavel, A.R.; Natarajan, R.; Vaidyanathan, K.; Soniya, V.P. Mosquitoes of the Mangrove Forests of India: Part 5--Chorao, Goa, and Vikhroli, Maharashtra. J. Am. Mosq. Control Assoc. 2007, 23, 91–94. [Google Scholar] [CrossRef]
- Kumar, K.; Sharma, A.K.; Sarkar, M.; Chauhan, A.; Sharma, R. Surveillance of Aedes Aegypti (L.) Mosquitoes in Mumbai International Seaport (India) to Monitor Potential Global Health Risks. J. Insects 2014, 2014, e951015. [Google Scholar] [CrossRef]
- Eiras, A.E.; Buhagiar, T.S.; Ritchie, S.A. Development of the Gravid Aedes Trap for the Capture of Adult Female Container-Exploiting Mosquitoes (Diptera: Culicidae). J. Med. Entomol. 2014, 51, 200–209. [Google Scholar] [CrossRef]
- Mackay, A.J.; Amador, M.; Barrera, R. An Improved Autocidal Gravid Ovitrap for the Control and Surveillance of Aedes Aegypti. Parasit Vectors 2013, 6, 225. [Google Scholar] [CrossRef] [Green Version]
- Sriwichai, P.; Karl, S.; Samung, Y.; Sumruayphol, S.; Kiattibutr, K.; Payakkapol, A.; Mueller, I.; Yan, G.; Cui, L.; Sattabongkot, J. Evaluation of CDC Light Traps for Mosquito Surveillance in a Malaria Endemic Area on the Thai-Myanmar Border. Parasites Vectors 2015, 8, 636. [Google Scholar] [CrossRef] [Green Version]
- Edman, J.; Kittayapong, P.; Linthicum, K.; Scott, T. Attractant Resting Boxes for Rapid Collection and Surveillance of Aedes Aegypti (L.) inside Houses. J. Am. Mosq. Control Assoc. 1997, 13, 24–27. [Google Scholar]
- Ritchie, S.A.; Cortis, G.; Paton, C.; Townsend, M.; Shroyer, D.; Zborowski, P.; Hall-Mendelin, S.; Van Den Hurk, A.F. A Simple Non-Powered Passive Trap for the Collection of Mosquitoes for Arbovirus Surveillance. J. Med. Entomol. 2013, 50, 185–194. [Google Scholar] [CrossRef]
- Gu, W.; Novak, R.J. Short Report: Detection Probability of Arbovirus Infection in Mosquito Populations. Am. J. Trop. Med. Hyg. 2004, 71, 636–638. [Google Scholar] [CrossRef]
- Microsoft Premonition. Microsoft Research. Available online: https://www.microsoft.com/en-us/research/project/project-premonition/. (accessed on 3 December 2021).
- Filipović, I.; Hapuarachchi, H.C.; Tien, W.-P.; Razak, M.A.B.A.; Lee, C.; Tan, C.H.; Devine, G.J.; Rašić, G. Using Spatial Genetics to Quantify Mosquito Dispersal for Control Programs. BMC Biol. 2020, 18, 104. [Google Scholar] [CrossRef]
- Batovska, J.; Lynch, S.E.; Cogan, N.O.I.; Brown, K.; Darbro, J.M.; Kho, E.A.; Blacket, M.J. Effective Mosquito and Arbovirus Surveillance Using Metabarcoding. Mol. Ecol. Resour. 2018, 18, 32–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balingit, J.C.; Carvajal, T.M.; Saito-Obata, M.; Gamboa, M.; Nicolasora, A.D.; Sy, A.K.; Oshitani, H.; Watanabe, K. Surveillance of Dengue Virus in Individual Aedes Aegypti Mosquitoes Collected Concurrently with Suspected Human Cases in Tarlac City, Philippines. Parasites Vectors 2020, 13, 594. [Google Scholar] [CrossRef] [PubMed]
- Mishra, G.; Jain, A.; Prakash, O.; Prakash, S.; Kumar, R.; Garg, R.K.; Pandey, N.; Singh, M. Molecular Characterization of Dengue Viruses Circulating during 2009–2012 in Uttar Pradesh, India. J. Med. Virol. 2015, 87, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, R.H.; Bathoorn, E.; Chlebowicz, M.A.; Couto, N.; Ferdous, M.; García-Cobos, S.; Kooistra-Smid, A.M.D.; Raangs, E.C.; Rosema, S.; Veloo, A.C.M.; et al. Application of next Generation Sequencing in Clinical Microbiology and Infection Prevention. J. Biotechnol. 2017, 243, 16–24. [Google Scholar] [CrossRef]
- Goldberg, B.; Sichtig, H.; Geyer, C.; Ledeboer, N.; Weinstock, G.M. Making the Leap from Research Laboratory to Clinic: Challenges and Opportunities for Next-Generation Sequencing in Infectious Disease Diagnostics. mBio 2015, 6, e01888-15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adikari, T.N.; Riaz, N.; Sigera, C.; Leung, P.; Valencia, B.M.; Barton, K.; Smith, M.A.; Bull, R.A.; Li, H.; Luciani, F.; et al. Single Molecule, near Full-Length Genome Sequencing of Dengue Virus. Sci. Rep. 2020, 10, 18196. [Google Scholar] [CrossRef]
- Amarasinghe, S.L.; Su, S.; Dong, X.; Zappia, L.; Ritchie, M.E.; Gouil, Q. Opportunities and Challenges in Long-Read Sequencing Data Analysis. Genome Biol. 2020, 21, 30. [Google Scholar] [CrossRef] [Green Version]
- Pollett, S.; Melendrez, M.C.; Maljkovic Berry, I.; Duchêne, S.; Salje, H.; Cummings, D.A.T.; Jarman, R.G. Understanding Dengue Virus Evolution to Support Epidemic Surveillance and Counter-Measure Development. Infect. Genet. Evol. 2018, 62, 279–295. [Google Scholar] [CrossRef] [PubMed]
- DengueNet--WHO’s Internet-Based System for the Global Surveillance of Dengue Fever and Dengue Haemorrhagic Fever (Dengue/DHF) Http://Www.Who.Int/Denguenet. Dengue/DHF--Global Public Health Burden. Wkly. Epidemiol. Rec. 2002, 77, 300–304.
- DengueMap: New HealthMap Collaboration with CDC|HealthMap. Available online: http://www.diseasedaily.org/diseasedaily/article/denguemap-new-healthmap-collaboration-cdc-8910 (accessed on 19 September 2021).
- Hernández-Ávila, J.E.; Rodríguez, M.-H.; Santos-Luna, R.; Sánchez-Castañeda, V.; Román-Pérez, S.; Ríos-Salgado, V.H.; Salas-Sarmiento, J.A. Nation-Wide, Web-Based, Geographic Information System for the Integrated Surveillance and Control of Dengue Fever in Mexico. PLoS ONE 2013, 8, e70231. [Google Scholar] [CrossRef] [Green Version]
- Kolopack, P.A.; Parsons, J.A.; Lavery, J.V. What Makes Community Engagement Effective?: Lessons from the Eliminate Dengue Program in Queensland Australia. PLoS Negl. Trop. Dis. 2015, 9, e0003713. [Google Scholar] [CrossRef]
- Tapia-Conyer, R.; Méndez-Galván, J.; Burciaga-Zúñiga, P. Community Participation in the Prevention and Control of Dengue: The Patio Limpio Strategy in Mexico. Paediatr. Int. Child Health 2012, 32, 10–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whittaker, M.; Smith, C. Reimagining Malaria: Five Reasons to Strengthen Community Engagement in the Lead up to Malaria Elimination. Malar J. 2015, 14, 410. [Google Scholar] [CrossRef] [Green Version]
- Utarini, A.; Indriani, C.; Ahmad, R.A.; Tantowijoyo, W.; Arguni, E.; Ansari, M.R.; Supriyati, E.; Wardana, D.S.; Meitika, Y.; Ernesia, I.; et al. Efficacy of Wolbachia-Infected Mosquito Deployments for the Control of Dengue. N. Engl. J. Med. 2021, 384, 2177–2186. [Google Scholar] [CrossRef]
- Beebe, N.W.; Pagendam, D.; Trewin, B.J.; Boomer, A.; Bradford, M.; Ford, A.; Liddington, C.; Bondarenco, A.; Barro, P.J.D.; Gilchrist, J.; et al. Releasing Incompatible Males Drives Strong Suppression across Populations of Wild and Wolbachia-Carrying Aedes Aegypti in Australia. Proc. Natl. Acad. Sci. USA 2021, 118, e2106828118. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Yang, T.; Bui, M.; Gamez, S.; Wise, T.; Kandul, N.P.; Liu, J.; Alcantara, L.; Lee, H.; Edula, J.R.; et al. Suppressing Mosquito Populations with Precision Guided Sterile Males. Nat. Commun. 2021, 12, 5374. [Google Scholar] [CrossRef] [PubMed]
- Waltz, E. First Genetically Modified Mosquitoes Released in the United States. Nature 2021, 593, 175–176. [Google Scholar] [CrossRef]
- Waltz, E. GM Mosquitoes Fire First Salvo against Zika Virus. Nat. Biotechnol. 2016, 34, 221–222. [Google Scholar] [CrossRef] [Green Version]
- Letting the Bugs out of the Bag. Nature 2011, 470, 139. [CrossRef] [PubMed]
- Long, K.C.; Alphey, L.; Annas, G.J.; Bloss, C.S.; Campbell, K.J.; Champer, J.; Chen, C.-H.; Choudhary, A.; Church, G.M.; Collins, J.P.; et al. Core Commitments for Field Trials of Gene Drive Organisms. Science 2020, 370, 1417–1419. [Google Scholar] [CrossRef]
- Garcia, G.A.; Hoffmann, A.A.; Maciel-de-Freitas, R.; Villela, D.A.M. Aedes Aegypti Insecticide Resistance Underlies the Success (and Failure) of Wolbachia Population Replacement. Sci. Rep. 2020, 10, 63. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paradkar, P.N.; Sahasrabudhe, P.R.; Ghag Sawant, M.; Mukherjee, S.; Blasdell, K.R. Towards Integrated Management of Dengue in Mumbai. Viruses 2021, 13, 2436. https://doi.org/10.3390/v13122436
Paradkar PN, Sahasrabudhe PR, Ghag Sawant M, Mukherjee S, Blasdell KR. Towards Integrated Management of Dengue in Mumbai. Viruses. 2021; 13(12):2436. https://doi.org/10.3390/v13122436
Chicago/Turabian StyleParadkar, Prasad N., Pallavi R. Sahasrabudhe, Mrunal Ghag Sawant, Sandeepan Mukherjee, and Kim R. Blasdell. 2021. "Towards Integrated Management of Dengue in Mumbai" Viruses 13, no. 12: 2436. https://doi.org/10.3390/v13122436