1. Introduction
Organizations have been transforming the way they create and fulfill value for customers by leveraging a mix of internal and external actors and resources to become service centric (
Vargo and Lusch 2008;
Lusch and Nambisan 2015). Such transformations, however, confront organizations with a dual challenge of continuing to run regular business at one speed while running at a faster speed to identify gaps in the value created (i.e., value created vis-à-vis value in use as perceived by the customer) and explore the viability of new value propositions and/or business models using inter-organizational partners (
Wieland et al. 2018). There have been recommendations to use an agile organizational model with its own governance, structure, and processes to support exploration and evaluation (
Aghena et al. 2015) and to use adaptive leadership processes in such explorations to stay competitive and sustain growth (
Uhl-Bien and Arena 2018). This dual challenge calls for organizations to demonstrate ambidexterity (
O’reilly and Tushman 2013), which is often used to address complex supply chain governance (
Im et al. 2019). The goal is to develop such ambidexterity on the demand side by using a number of external actors and resources to address evolving customer expectations.
The demand side calls for identifying innovative processes that create differentiated value (
Nambisan et al. 2017), developing capabilities to support inter-organizational collaboration (
Bryson et al. 2006), and using agile digital platforms to support collaboration by integrating the disparate systems used by customers and partners (
Yoo et al. 2010). Recently, there has been discussion on the need for organizations to develop inter-organizational dynamic capabilities (
Sandberg et al. 2021) based on how the focal firm controls the coordination of value cycle activities (creation, fulfillment, and assessment of value in use) for the benefit of all, including customers or participates as a partner in a network of actors who control the coordination. The coordination of the value cycle activities within a network still needs a mechanism, such as a distribution among a set of network members or the use of an external entity, to address collaboration responsibility. Independent of the typologies used, the dynamic capabilities call for relationship governance and resource orchestration.
Network theory argues that governing the relationships of network partners calls for allowing each to weigh the costs against the benefits of participating in the value cycle activities (
Håkansson and Ford 2002), i.e., to seek alignment in goals towards a shared outcome. Communication theory (
Blaschke et al. 2012) argues that communication processes are key to supporting inter-organizational collaboration. If applied to resource orchestration, it means that there is a need for a structure and space that defines what resources are provided by each partner, along with a platform to share these resources. Businesses have been transforming their operations using various agile models to align goals to create value, and they have been using a mix of centralized or distributed digital platforms to fulfill and assess value in use to meet changing customer expectations (
Lusch and Nambisan 2015). However, developing such a capability is a challenge for many public and non-profit organizations due to their social dynamic nature (
Fligstein and McAdam 2012) in value creation and their lack of a single governance mechanism (
O’reilly and Tushman 2013) to share resources to fulfill and assess value in use.
Such dynamic capability is especially complex in healthcare systems (hospitals, public health agencies, primary clinics), as they use many external partners to reach and support patient populations that often face different health conditions. This has become critical as hospitals have begun to transform the care coordination of patients within their ecosystem to reduce costs (
Dreyer 2014) and meet regulatory changes on reimbursement policies, especially with the introduction of the Affordable Care Act (ACA) in the US. With advanced technologies such as IoT, social media, smart phones, and AI/machine learning (
Johnston et al. 2018;
Kim 2015;
Carretero et al. 2015), there is increasing demand from patients to be actively involved in their own care. Some hospitals have begun to extend their electronic health records (EHR) to connect with patients through secure portals and remote care management using telehealth, and to share patient data with clinical partners (such as skilled nursing homes, physicians, and home care facilities). However, these are still point-to-point solutions and are not generalizable across diverse patient populations that face multiple social determinants (i.e., conditions in which people are born, grow, live, work, and age) and economic inequities (
Link and Phelan 1995;
Mead et al. 2008;
Harring 2011).
What is required is a network model of an inter-organizational type with dynamic or agile capabilities to bring together select partners, clinical and non-clinical, to address the distinct needs of a particular patient (or client) population, using a coordinating mechanism that aligns their goals and a digital platform to support resource sharing to address evolving patient needs. While some regional health exchanges have begun to act as the outside organization to coordinate the interactions among a network of hospitals and physicians as they share patient data, the lack of alignment in the goals of all involved has still led to low adoption (
Agarwal et al. 2010b). Specifically, this coordination does not include the roles of the many social and community organizations upon which health systems must rely to address social determinants and influence patient adherence to practices. Therefore, there is a need for a distributed network architecture that supports agility in creating a network of different partners, including health systems and clients, to build relationships to align goals and share resources to support care coordination. Recent research in blockchain has shown that it can be a viable architecture to address care coordination by engaging patients, health systems, and partners through resource sharing in a secure manner with provisions for auditability and real-time feedback on care coordination activities. Hence, the research question:
How can such a platform use the resource sharing characteristic of blockchain to support both the goal alignment and resource orchestration needed to support care coordination activities?
Our goal in this paper is to answer this question at a broader level. While we illustrate a few instances of blockchain implementation and discuss research on other applications of blockchain in healthcare, what is needed is a higher-level abstraction, with the use of the entity–relationship model, to begin to consider its use for any healthcare application addressing care coordination in various contexts, especially in preventive health by public health agencies. This leads to a reformulation of the research question:
How can we develop a conceptual, blockchain based digital platform model that supports health system applications developed in various contexts to improve patient outcomes?
This paper is organized as follows. The next section will discuss prior research on resource sharing in healthcare and specific challenges in its ability to align goals to share resources.
Section 3 will discuss research in blockchain and its potential viability as a platform to support resource sharing among actors as they seek goal alignment.
Section 4 proposes a resource sharing model artefact for building blockchain applications using two different blockchain applications and develops a conceptual model using high-level constructs for building such blockchain applications.
Section 5 illustrates the generalizability of this conceptual model to explore the use of blockchain technology to support preventive care in public health. The last section provides a discussion of the model with concluding comments and directions for future research.
2. Prior Research in Healthcare and Some Challenges
Recent changes in healthcare reimbursement models, such as bundled payments for care provided over 30 days and penalties for unanticipated patient readmissions or low patient satisfaction, have begun to transform care inside hospitals (under rules associated with accountable care organization or ACA). New innovative care delivery models are used to engage external partners (e.g., nursing homes and home care facilities) as well as patients by leveraging technologies. In addition, facilities such as urgent care centers and mini-clinics, ambulatory care centers for specialized clinical care, and medical homes and patient homes have become places to support preventive as well as care transition post-discharge (
Nuckols et al. 2017;
Beans 2016;
Sanborn 2018).
With multiple facilities extending care, aligning the goals of all involved has become a high priority. An early focus has been on aligning care for high-risk patients by partnering with nursing homes, as they both are impacted by patient readmission penalties (
Tanniru et al. 2019). Hospitals have used extended electronic health record (EHR) systems to share patient knowledge and coordinate activities (
Pinsonneault et al. 2017). Additionally, hospital systems have begun to align their goals with those of patients who want to stay at home post-discharge by allowing them to track vital signs at home and use community partners such as emergency management technicians to engage in remote consultation, if needed, while the patient is at home (
Tanniru et al. 2019). Additionally, tools are being deployed to remotely monitor cancer patients and have their information integrated with electronic health records using blockchain technology (
Chiauzzi et al. 2015). Apps, social media, and other personal technologies are being used to educate patients and caregivers on how to address their health conditions (
Sendler 2018;
Guo et al. 2017). However, many of these are point-to-point solutions explored with a provider-centric focus, i.e., reducing costs by managing high-risk patients while aligning with partner goals.
Health exchanges were considered by several states as part of the ACA to support patient data sharing among hospitals and clinical care providers, with limited success (
Khuntia et al. 2017), as they are not quite aligned with the goals of physicians or health systems except in some specific cases (e.g., opioid disorder reduction (
Dowell et al. 2019)). The meaningful use legislation in the US (HITECH Act) provided incentives for physicians to upgrade their technology to streamline patient data sharing with hospitals and improve patient quality. With HL-7 standards beginning to streamline the communication of patient information among actors, several new mobile applications have begun to support patient–provider communication to reduce costs and improve convenience (
Agarwal et al. 2010a). Some private exchanges are used to support peer-to-peer communication and sharing of knowledge among patients (
Lim et al. 2020).
Many of these platforms still do not effectively integrate resource sharing with non-clinical care providers, such as social and community health organizations, which service underserved populations. Except during pandemics (
Tanniru 2020), many of these organizations are unable to connect with care providers to gather and provide the needed viral infection information or answer their questions, except using minimal technology such as phone calls and text messaging, when feasible. While there is an increasing availability of technology platforms, such as telehealth consultation and portals for sharing information, their use is either limited by being too provider centric or not accessible to some vulnerable populations. With an increasing number of external actors, clinical and non-clinical, supporting patient services using a myriad of technologies, there is a broader
technical challenge, namely the need for a distributed digital platform that can support resource sharing by being agnostic to the partner technologies employed to create and use the resources shared.
Alignment of Goals
Businesses have used incentives to align their goals with those of external customers using several strategies, including membership in special programs, entering customers into special promotional draws, designating them as advocates or ambassadors (
Nyangwe and Buhalis 2018) or making them a part of a product design team (
El Sawy et al. 2020). The American Psychological Association (APA) defines an “incentive” as an external stimulus, such as a condition or an object, that enhances or serves as a motive to influence behavior. An incentive system must create explicit or implicit value for all actors involved in a resource exchange. An external stimulus such as a rewarding scheme can incentivize bloggers to share knowledge (
Chai et al. 2011), or an intrinsic stimulus may empower actors to engage in a behavior that addresses their own goals and aspirations (
Tanniru et al. 2021). The diversity of actors outside a hospital makes creating incentives to align the goals of these actors a
social challenge.
Consider a health system that used four different point-to-point solutions to address different health conditions of patients using a mix of clinical and non-clinical partners, community organizations, and patients to develop community strategies (CS).
- CS1.
It used a remote care management system that connected high-risk patients living at home with hospital staff and a local emergency management technician (EMT) to visit the patient at home for examination if health complications were observed.
- CS2.
It sent patients to a skilled nursing facility (SNF) after cardiac surgery for recuperative care before patients were discharged to their home. To improve the quality of care these patients received and reduce their readmission to the hospital, it partnered with a specialist team (cardiac surgeon and an advanced nurse practitioner) to consult with the SNF staff when the patient condition became unstable.
- CS3.
It decided that some of its patients were immigrants and/or poor and have diabetic conditions that need prevention. So, it provided them with glucose monitors and a mobile app for recording their readings. It decided to use a community organization to help the population learn about healthy cooking, track their glucose levels, and answer any of their questions.
- CS4.
It recognized that some of its minority patients were obese and had high blood pressure. It referred them to a non-profit organization (project healthy community) that educated the patients (also called participants) on improved nutrition, physical activity, and behavioral health. The goal here was for these patients to use digital tools provided by the non-profit to track their physical activity, blood pressure, and weight and share this information with the educators to obtain insight into how to improve their adherence. It used a community facility for the students to meet and engage in conversations or practice activities.
In summary, the health system provided technology and a community partner to coordinate the care of high-risk patients (CS1), distributed the responsibility of care coordination of cardiac patients to an SNF using specialist teams (CS2), provided devices to patients and distributed the coordination responsibility to a community organization to reduce diabetes in an immigrant population (CS3), and provided a referral for some minority patients to a non-profit educator who used devices to practice what they learned to reduce obesity and hypertension (CS4). There is goal alignment between the patient, EMT, and hospital in CS1, as it is coordinated by the hospital, but the goal alignment to support patients is left up to other organizations in all the other community strategies. The alignment of goals between the healthcare provider system and patients was contingent on how this goal was aligned by partners and their ability to provide the needed feedback to influence adherence and potentially incentivize patients to engage in the practices.
In all the cases discussed above, assigning the distribution of coordination responsibility to different network partners is needed to ensure that the capabilities of each of these partners is leveraged. The challenge often is in the ability of all actors who can influence the success of care coordination to take the necessary action to make the community strategy effective. Social action theory suggests that relational or inter-organizational goal alignment among actors requires certain functional specificity, i.e., how each actors’ engagement in activities leads to meeting client or customer expectations (
Kim and Schneider 2005). This is critical to engender trust among patients and motivate them to participate in their care management (
Cormican and Dooley 2007). Incentives used to provide this motivation must consider the need for change (content theories), define the value for undergoing the change (process theories), and motivate actors to contribute to change (contemporary theories) (
Saif et al. 2012).
For example, lack of adherence to healthy eating habits in CS3 (need for change) can be improved by providing coupons for fresh fruit and vegetables (process change), but only if all the actors in that network can track lack of adherence and adapt their activities to contribute to the change. Similarly, lack of adherence to reduce obesity in CS4 (need for change) can only be improved if this information is tracked by all patients to come up with unique opportunities to practice their physical activity and learn about healthy cooking (process change), especially during COVID-19. Identifying the opportunities for patient empowerment and self-efficacy and seeking goal alignment on incentives and resources to help patients overcome their constraints and/or social and economic barriers is a social challenge.
With this background, in the rest of this paper we will discuss how blockchain technology can be used by healthcare organizations as a digital platform to share information to assess adherence gaps and share resources to address these gaps, i.e., it is both a technical and social challenge.
3. Prior Research on Blockchain Technology as a Platform for Resource Sharing
Blockchain is one type of distributed data or resource sharing technology with some unique characteristics. Called digital ledger technology, it connects several transactions, called blocks, using a cryptographic hash and a timestamp along with the information about previous blocks forming a chain. Multiple methods to create the hash have been discussed in the literature (
Maetoug et al. 2018), and the hash function used in multi-chain is similar to what is used in bitcoin (Secure Hash Algorithm 256-bit). By distributing the resource across several computer systems and using smart contracts to implement the terms and conditions on how transactions recorded on blockchain are collected, transferred, and stored, blockchain technology supports peer-to-peer resource sharing with no central authority coordinating such resource sharing.
Blockchain has evolved from 1.0 currency to 2.0 smart contracts, to decentralized applications using different settings for resource sharing: public chains, private chains, etc. (
Anjum et al. 2017). As a decentralized digital platform or architecture, actors from distributed and different enterprises share resources if there is alignment in their goals (
Glaser 2017). For example, actors who share financial transactions (
Gomber et al. 2018) seek efficiencies, and public sector actors share transactions to improve public service efficiency and effectiveness (
Cheng et al. 2017). Blockchain can help manage distributed records to ensure authenticity and provide provenance. It can also help actors use a decentralized marketplace to engage in value sharing (
Subramanian 2018).
The resource sharing is supported by two distinct features: (1) resources stored are confirmed based on agreed upon rules on who can participate in such resource sharing, with each node capable of checking for such confirmation, and (2) the confirmed records are immutable. This makes it ideal for multiple parties in the healthcare value network to trust the integrity of how healthcare data are created and transferred to others who may own and distribute it or simply access and use the data. With further segmentation of the patient data, including lab tests, consultation history, clinical trials, research information, and patient consent, healthcare data can be reliably stored and better managed, with fewer risks of misuse.
The healthcare industry has started to explore the use of blockchain as a health information exchange when there is no trusted network with clear standards or access rules to facilitate sharing of patient information (
Krawiec et al. 2016). It was used for physician credentialing among healthcare agencies for ensuring quality of care, pharmaceutical supply chain management to track drug development needed for approvals, opioid prescription tracking, patient-controlled cancer data sharing, and insurance claim adjudication (
Sotos and Houlding 2017;
Lacity 2018;
Zhang et al. 2018;
Mattke et al. 2019). Some applications are proposed to consolidate patient data for hospital and physician use (OmniPHR by
Ekblaw et al. 2016), and others are offered as a single source for secure, fast, and transparent access (
Medicalchain 2017).
Borioli and Couturier (
2018) discussed the potential of blockchain to conduct clinical trials using smart contracts, and
Mamoshina et al. (
2018) proposed a roadmap for decentralizing the personal health data ecosystem for drug discovery, biomarker development, and preventative healthcare. MeDShare provides data provenance, auditing, and control of shared medical data in cloud repositories and monitors any malicious use of the data (
Xia et al. 2017).
In general, blockchain has demonstrated its viability as a platform for multiple actors to share resources in a secure manner if these actors have a shared goal and an entity exists that is trusted to manage the platform. The trust building, robustness/fault tolerance, security, and redundancy features of blockchain (
Ruoti et al. 2020) make it a viable platform for resource sharing among actors operating in different contexts. For example, the resource shared to coordinate a clinical diagnosis is patient data; the resource shared to transport a patient to a rehabilitation center can be financial funds for a taxicab; and the resource shared to remind a patient to go for a physical exam at a clinic is a text message. In each of these cases, blockchain provided a secure and efficient way to share the needed resources to coordinate several actors as they work toward a desired outcome: provide a second opinion for patients, provide a taxi for patient to visit the rehab facility, or get the patient to visit the clinic for the physical exam.
By allowing all participating actors to determine the type of resource they need to share (e.g., clinical data, financial data, text alert data) to accomplish their goals, we make the blockchain technology platform agnostic to specific applications. We believe this is the novelty of our approach, as it implicitly addresses both the technical challenge (the need to have a coordinating entity to connect a disparate number of actors using myriad information technology sources to share and use information) and the social challenge (allow actors of the health network to track adherence and assess gaps and engage the actors to develop incentives to address these gaps). Sometimes, one may need two or more sets of resource sharing mechanisms to achieve both these two different objectives and may use the same blockchain platform or a hybrid (i.e., a mix of blockchain and other coordinated platforms). The scalability of such a platform is still a major challenge, and this will be addressed in the last section. The next section will discuss the research methodology used to design a resource sharing platform in healthcare using blockchain technology.
4. Developing a Resource Sharing Model Using Blockchain
The design science research methodology is used to develop a resource sharing model as a novel artefact that allows multiple actors to coordinate their activities in support of patient care delivery outside a hospital system. The artefact developed is a conceptual model with distinct constructs used to share resources using a blockchain technology platform. The artefact is novel because of its ability to support resource sharing that aligns both the goals of a distributed set of clinical and non-clinical actors and the resources they need to coordinate activities in support of care delivery outside a hospital. Once developed, such an artefact (e.g., tool, model, etc.) is applied to solve other problems in healthcare to demonstrate its viability.
This methodology is illustrated first by developing a general resource sharing model using blockchain technology and demonstrating its applicability to two healthcare blockchain implementations, where different actors (patient–provider and patient–partner) align their goals and share resources to coordinate care delivery. From this resource sharing model, a conceptual model with a set of high-level constructs for building blockchain applications is developed.
4.1. General Resource Sharing Model on Blockchain
The general resource sharing model discussed below uses an abstraction of resource generation and sharing in the development of blockchain applications.
Creator (C): This entity is responsible for creating the resource and storing it in the blockchain. In healthcare, a patient record is the resource shared (such as an electronic health record), and healthcare providers often are the creators.
Owner (O): This entity is the owner of the information, and they have the right to control who can access what information. In healthcare, the healthcare provider creates a health record and can potentially assign the patient as the owner, thus allowing a patient to control who can access that record for future use.
User (U): To access information stored in blockchain storage, the user first needs to send a request to the owner of the record. Once the owner has provided access, the user can use the information. In healthcare, a patient may want to a seek a second opinion from a new healthcare provider. In this case, this care provider seeks access to the patient record by sending a request to the patient. Once a patient provides the right to access this record, the provider can use such access to review and complete their consultation service.
Next, we define a few basic operations needed to manage resources (e.g., patient data) on blockchain. These resource managing operations are used by the Creator, Owner, and User to interact with the system. C, O, and U denotes the set of Creators, Owners, and Users in the system, respectively.
Register (u)/Register (o): Register a user or owner to the blockchain system.
Write (d, c, o): With this operation, the Creator writes the information d associated with the owner .
Permit (d, o, u): With this operation, the Owner provides the read access of information d to the user .
Read (d, u): With this operation, the user can read the information d.
Execute (Event e, EventHandler f, Message m): When an event e (a specific type of transaction) occurs, the blockchain executes EventHandler f and passes a message “m” into the blockchain (writing another transaction in the blockchain). In Ethereum and Hyperledger blockchain, this can be implemented as a smart contract. The EventHander is the contract here. The contract can be executed when a condition is met within a specific transaction, and the result of the execution of the contract is one or more transactions being written into the blockchain.
These resource sharing operations are not unique to blockchain applications as these are used in centrally coordinated data management systems. However, these basic operations in blockchain allow healthcare information to be shared by multiple actors without a trusted party centrally coordinating the data. Features such as (1) private–public keys, (2) chaining the blocks using hashing, and (3) replication of blocks in all nodes help support such distributed data sharing. Such an approach allows clinical and non-clinical actors to share information using blockchain based resource sharing model with the added advantage that ensures data consistency, in-built incentive mechanisms, and data privacy. Private–public keys and streams to chain blocks are used in the basic operators (register, write, permit, and read). See
Appendix A for a potential implementation using streams.
Within healthcare, the creator of a “resource” may or may not be “clinical care provider”, and the owners and users can be patients, other healthcare providers, or even those who access patient information for research. In the next subsection, we describe two healthcare use cases where health information is created, owned, and used by different actors.
4.2. Resource Sharing Models in Blockchain Implementation
In this section, we first describe two healthcare use cases of blockchain implementations and illustrate how they can be instantiated by the resource sharing model discussed in the previous section.
Use Case 1: Aligning goals of patient–provider by giving patients control over data.
In this case, patients are provided access to their data from their caregivers and care centers, such as hospitals, physical therapy centers, etc. This information is stored on the blockchain using HL7 CCDA format and segmented into multiple sections. These are 1: Allergies; 2: Medications; 3: Problems; 4: Procedures; 5: Results; 6: Social History, and 7: Vital Signs. The patient can provide all or some sections of this information to other caregivers and is informed every time their data are accessed. Only the patient can provide access to the data, and the data are not transferred to the provider. Providers do not have to collect the data they need repeatedly and use shared data to fulfill their role, for example providing patients with a second opinion or suggesting a specific treatment such as rehabilitation. This reduces their need to engage in the administrative costs involved in collecting, validating, or using such information to fulfill their role, thus providing them with an incentive to use this platform for such information.
Blockchain based implementation.
The solution is implemented on a private Ethereum blockchain. There is permissioned access, that is, all users are verified before they get on the system, thus eliminating spurious users who would potentially cause denial of service to genuine users. Ethereum IDs are created by patients and providers when they begin to interact with the system. These are public–private key pairs, with the private key being known only to the respective user. The blockchain is replicated across multiple physical locations. Some blockchain nodes are supported by hospitals and care providers. The system includes a server-side business layer that processes clinical care data and provides services for access to the data. The front-end can be a desktop (as it is now) or other platforms, such as tablets. Administrators of the blockchain ensure that the blockchain is working properly and restore any blockchain nodes that are down. They cannot obtain access to the patient data. Ethereum enables contract code via the Solidity language. The code is open source and can be examined by anyone for security and privacy.
The architecture of the system has been designed to keep all the protected health information (PHI) on the blockchain, while keeping non-PHI information out of the blockchain. Examples of non-PHI information include publicly available information about providers as well as non-identifiable patient information such as state of residence. Because of the size limits of records in Ethereum, if the patient record is lengthy, then the mapping is made between what is in the system and what is stored outside the chain. The Ethereum also keeps track of each provider to whom a patient has given access and the sections they accessed. The history of provider access to the data is also maintained for the patient to review at any time.
Use Case 2: Aligning goals of patients and partners by providing payment for data shared.
The case study presented here allows patients to share their health data, including diagnoses and treatments, with research organizations for payment. The payments increase patients’ willingness to share their data for research purposes, and research institutions will benefit by paying a small amount to gather a large amount of patient data to support analysis. While such a payment of small amounts to patients may be viewed as too complicated, research organizations today spend large sums of money to solicit patient participation in clinical trials, and a large proportion of this money goes to intermediaries.
Within a blockchain, the patient can control and monetize their data, thus providing an added incentive to use the platform. Since blockchain tracks every access, the payment is coupled with access, thus leading to immediacy and accuracy. Such transparency can lead to increased patient participation and improve the quality of clinical trials. The system here uses fiat currency (USD) as opposed to crypto tokens so patients can have a determined value for each transaction.
Blockchain based implementation.
Hyperledger Fabric (
2020) was used to implement the system. Patients upload their health data in the form of CCD (Continuity of Care Document) or FHIR (Fast Healthcare Interoperability Resources). These data come either from hospitals and clinics or else from direct uploads from patient devices (e.g., via Fitbits). The data can either relate to a patient’s visit to a care center (encounter) or an episode related to their health/wellness. The data are uploaded one record at a time by the system frontend and is stored in the blockchain. The metadata about that data are stored in local storage, and this can include the nature of the data uploaded.
Patients publish the names of the files they want to share. When a buyer wants to purchase data, he or she is shown different types of data and the corresponding information (e.g., time range). Once a buyer decides to purchase some data, the system determines the owner of the data and checks whether permission was provided. If permission was not already provided, the system informs the patient of the buyer’s request and the incentive offered by the buyer. If the patient provides permission, then the system stores the permission (for one patient, one buyer, and one piece of data) in the blockchain and notifies the buyer of the permission. The buyer can request the data to be read. This data access is stored, and payment is deducted from the buyer account and credited to the patient account. The blockchain keeps health data, permission data, and the monetary amounts belonging to both the patient and the buyer. The payment for data shared here is used for research. However, it also can be used to incentivize patients who need financial resources to get to a care facility (e.g., transportation), external care providers such as pharmacies or diagnostic labs to follow-up on patients after hospital discharge, or social service providers such as community health workers to address health inequities (
Tanniru and Tanniru 2020).
In both use cases, the focus is on giving ownership of certain data to a patient or patient representative and allowing them to selectively provide access to others to use the data, thus aligning patient goals for control or access to resources they view as critical to gain access to care. The data may be created by care providers with a stated purpose, i.e., the goal of the blockchain application. The next section provides a generalized model for such resource sharing within blockchain technology.
4.3. Conceptual Model for Blockchain Applications
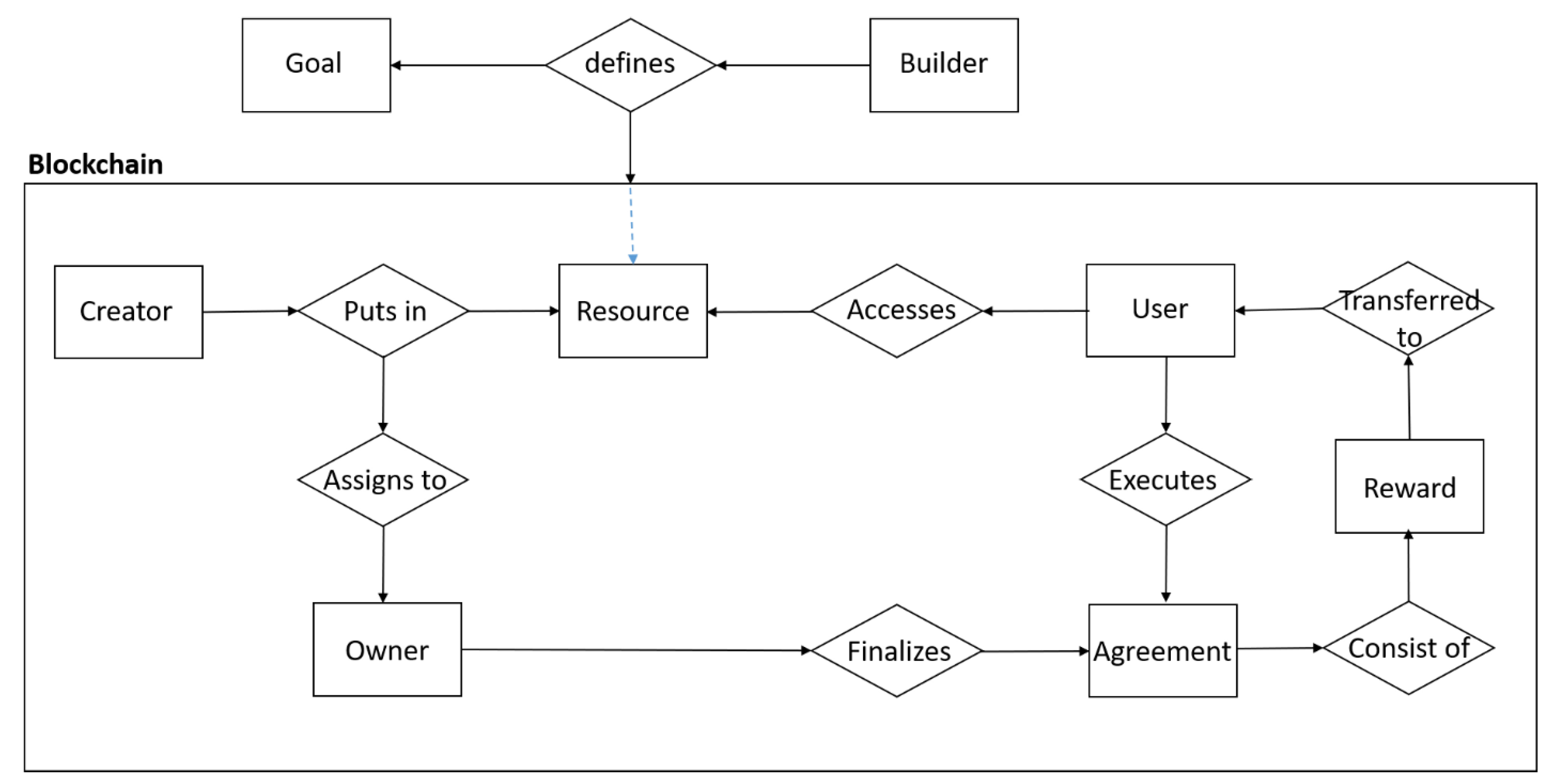
The resource sharing model embedded in the two blockchain applications can be viewed at a higher level of abstraction for generalizability. In principle, resources are created by someone, their ownership can be assigned to another person, and this person in turn can allow others to use this resource once they have permission for such usage. There can be agreements on how this resource is shared and what incentives, explicit or implicit, can guide such resource sharing. This is shown as a conceptual model in
Figure 1 and as a modelling language in
Figure 2. The constructs are represented as rectangular boxes: Builder (of the platform), Goal (of the platform), Creator (who puts in the resource), Owner (who can be the creator or assigned by the creator), and a User (who is permitted to access the resource). There are agreements on how roles are assigned and what rewards are shared to motivate or incentivize individuals to share the resource.
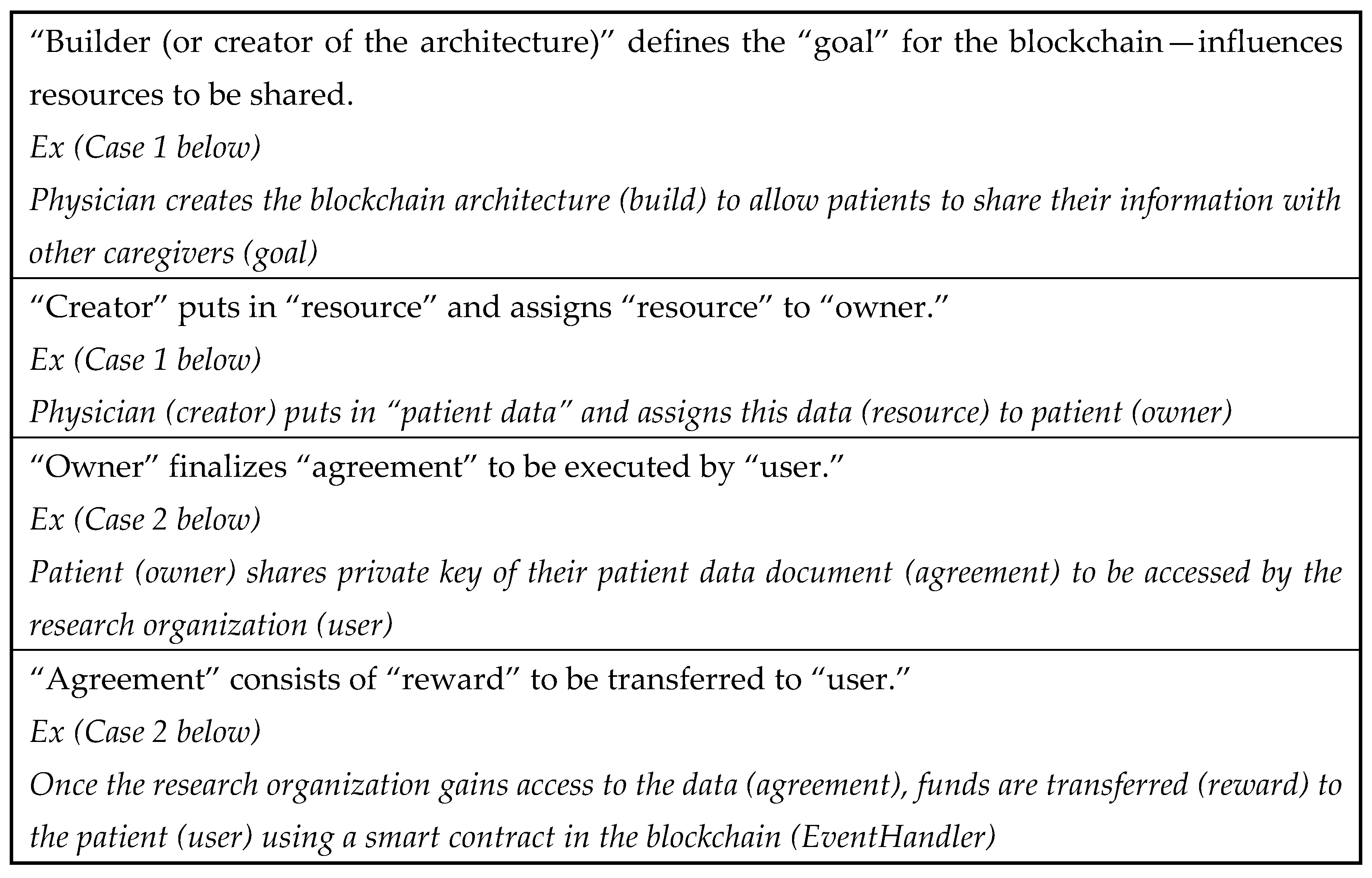
Table 1 summarizes how these constructs play a role in the two cases discussed earlier and Bitcoin. Here, the term “sharing” is used in the two use cases as it is a conventional term used in healthcare. Depending on the role one plays, the resource is created by a provider, assigned to an owner (shared with patients so they can control the resource distribution), and shared with a user (another care provider), based on an explicit agreement such as contract with a reward or giving a private key for the resource they can share with others. In other words, owners share the resource with a user based on a formal agreement. Additionally, the roles individuals play in resource sharing may change. For example, in Use Case 1, a provider creates a resource (patient record), assigns it to patient (owner), and the patient can act as a creator of a part of this resource (patient record) and give access to a consulting physician (user). On the other hand, in Use Case 2, a patient plays both roles: creator/owner for one resource (patient data) to share this resource with a research organization (user) and a user of a different resource (funds) provided by a research organization (creator/owner).
The research question posed in
Section 1 calls for a resource sharing model that aligns the goals of multiple actors so they can share their data or resource to help coordinate the activities of those involved in care continuity. By aligning the goals of patients using empowerment (Case 1), financial incentives (Case 2), and convenience (Bitcoin), the actors are motivated to engage in resource sharing. The partner goals in some cases are implicitly supported by getting reimbursed for the services provided and obtaining access to quality data for research. These are not explicit parts of the activities listed here and are outside the scope of the blockchain application.
Additionally, not all activities needed to accomplish the broader goals of those who are involved in setting up this platform (permissioned, permission-less, private, etc.) have to use blockchain. For example, some activities may be best accomplished using other mechanisms, such as point-to-point link to provider EMR systems (e.g., send specialist consultation report to provider directly in Case 1), social media focused digital infomediary (e.g., allow patients to consult with other patients on treatment in Case 1), or electronic funds transfer (e.g., deposit funds into patient account for sharing data for research instead of blockchain in Case 2).
In the next section, we will go back to the four scenarios discussed in
Section 2 and illustrate the how generalizability of the conceptual model developed for blockchain application can help healthcare organizations address the needs of each patient group, using the right digital platform.
5. Generalizability of Blockchain Conceptual Model—Care Continuity
In this section, we use the constructs used to describe each of the four community strategies illustrated in
Section 2 and discuss the model generalizability and other factors organizations must consider in deciding on the right architecture for healthcare applications.
Community Strategy 1. As discussed earlier, the healthcare organization is coordinating the network that includes patients and EMTs and using a centralized digital platform that is connected to the patient’s electronic medical record to track patient adherence and develop innovative ways to motivate the patients to use the technology to self-manage their health. Since it is interacting with the EMTs, it can solicit their ideas on how to improve patient adherence, given that they visit the patients and potentially have insight on any patient barriers. This example is represented using the modeling language discussed in the previous section.
| Health system creates the blockchain architecture (build) to allow patients and EMTs to share information |
| Physician (creator) gains approval from patient (agreement), provides equipment (reward) to the patient (user) using a smart contract in the blockchain (EventHandler) |
| Patient (creator) puts in “patient data” and assigns these data (resource) to the physician (owner) |
| Physician (creator) puts in “patient visit alert” and assigns these data (resource) to EMT |
| Physician (creator) provides financial support (reward) to the EMT (user) using a smart contract in the blockchain (EventHandler) |
| EMT (creator) puts in patient status data and assigns these data (resource) to physician |
| Physician (creator) puts in “patient revisit to hospital” and assigns these data (resource) to user (EMT) and user (patient) |
Community Strategy 2. The patient data are created by the healthcare organization, which gives ownership to the SNF. The SNF can provide access to this patient data and create a separate resource on changes in patient conditions and provide access to the specialist team. The specialist team can create changes to patient treatment that can be accessed by the SNF staff. Both the changes in the patient conditions created by the SNF and changes in treatment created by the specialist team can be accessed by the hospital to assess patient progress. A smart contract may be used to determine if patient progress is not meeting expectations, and the hospital, specialist team, and SNF may be alerted for possible readmission of the patient back to the hospital or to recommend patient discharge. This example is represented using the modeling language below.
| Health system creates the blockchain architecture (build) to allow health system and specialist team to share information |
| Health system staff (creator) puts in authorization (resource) to hospital physician |
| Physician (creator) puts in “patient data” and assigns these data (resource) to the health system staff (owner) |
| Health system staff (creator) puts in “patient status alert” (resource) and assigns these data (resource) to specialist team |
| Physician (creator) provides financial support (reward) to the specialist team (user) using a smart contract in the blockchain (EventHandler) |
| Specialist team (creator) puts in patient consultation data and assigns these data (resource) to health system staff |
| Health system staff (creator) puts in “patient revisit to hospital” and assigns these data (resource) to user (specialist team) and user (physician) |
Community Strategy 3. The patient data are created by the healthcare organization, and both the patient and community organization may be provided access on the patient’s diabetic condition (e.g., glucose levels). The community organization can create nutritional educational material and provide patients access to it. Patients can track their glucose levels, create these data, and provide both hospital and community organization staff with access to it. The community organization can consult with the patient outside the blockchain platform, create any changes in diet-related treatments on the blockchain, and provide access to all relevant patients. A smart contract may be designed by the hospital to alert the hospital on whether there is enough progress made on glucose levels, and the hospital can decide if it needs to contact the patient to visit the hospital for further examination. Of course, the hospital or community organization can create financial incentives or access to support services and share this with the relevant patient population.
| Physician creates the blockchain architecture (build) to allow the patient and community organization to share information |
| Physician (creator) puts in patient diabetic data (resource) and assigns it to patient (user) and community organization staff (user) |
| Physician (creator) puts in financial support (reward) to the community organization staff (user) using a smart contract in the blockchain (EventHandler) |
| Physician (creator) puts in coupons to purchase personal tools (reward) to the patient (user) using a smart contract in the blockchain (EventHandler) |
| Community organization staff (creator) puts in “nutrition education material” and assigns these data (resource) to the patient (user) |
| Patient (creator) puts in “patient activity data” (resource) and assigns these data (resource) to community organization staff and physician |
| Community organization staff (creator) puts in guidance information (resource) and assigns this to patient (user) |
| Community organization staff (creator) puts in patient analysis of glucose levels (resource) and assigns these data to physician |
| A smart contract can create an alert (resource) to physician (user) for potential revisit to the hospital. Alternatively, physician (creator) can analyze patient progress and put in “patient revisit to hospital” and assign these data (resource) to the patient (user) and community organization staff (user) |
Community Strategy 4. The relevant patient data are created by the hospital, which provides access to the project healthy community (PHC). The PHC provides devices, and the patients create their performance metrics (weight, blood pressure, physical activity measures) and provide access to both the hospital physician and PHC staff. PHC staff can track a patient’s improvement and consult with the patient outside the blockchain to learn about any barriers. The PHC can share any incentives or ideas to overcome barriers with patients and physicians using blockchain. Again, a smart contract can be used to assess patient progress and alert both PHC staff and the physician on the need for additional intervention.
| Project health community (PHC) staff creates the blockchain architecture (build) to allow physicians and patients to share information |
| PHC staff (creator) puts in patient referral template (resource) and assigns it to physician (user) |
| Physician (creator) puts in patient referral data (resource) and assigns it to PHC staff (user) |
| PHC staff (creator) puts in coupons to purchase personal tools (reward) to the patient (user) using a smart contract in the blockchain (EventHandler) |
| PHC staff (creator) puts in program education information (resource) and assigns these data (resource) to the patient (user) |
| Patient (creator) puts in weekly activity data (resource) and assigns these data (resource) to PHC staff and potentially the physician |
| PHC staff (creator) puts in guidance information (resource) and assigns this to patient (user) |
| PHC staff (creator) puts in patient analysis of activity levels (resource) and assigns these data to physician (user) and funding organization (user) |
| Physician (creator) puts in “patient revisit to hospital for consultation” and assigns these data (resource) to the patient (user) and PHC staff (user) |
In CS3 and CS4, if the incentive is financial, the reward is created on the blockchain along with a smart contract that distributes this reward once the target goal is reached by the patient or to begin the prevention strategy. If the incentive is to support a social service, a payment for the service is provided once the social service provider engages the patient in this service and enters the completion of the service.
In summary, each of the four examples are represented using the blockchain model even though one may not choose to use blockchain architecture to support sharing of data. For example, the health system that is using Community Strategy 1 currently coordinates the design of the IT infrastructure and data sharing mechanism. However, this is an expensive strategy if it needs to be generalized for broader populations, and they have their own tools to monitor their health and share their data using a web-portal service. The health system can track their progress and use a clinical or community organization to consult with the patient if their tracked health condition is not as expected. There can still be a reward for the patient to record their data on the portal and for the partners who consult with the patient. In the case of all other strategies, while other organizations are used to track patient progress, using blockchain to share some of the patient progress data can provide health systems with real time access to patient conditions for potential intervention, even if some of the strategies are centrally coordinated by separate digital platforms used by the other health system partners.
Such real time information on population adherence to preventive practices is one of the big challenges for public health organizations as they try to use feedback to tailor practices to specific patient or client population contexts. For example, the use of community strategies in each case addresses the preventive needs of patients, high-risk patients, cardiac patients, diabetic patients, and obese patients. Public health agencies often promote various preventive methods to address chronic care conditions or patients with heart, diabetic, or other conditions. However, they cannot gain access to these populations to either gather feedback or provide preventive health information. This has been especially challenging during COVID-19, as many of the infection control practices tailored to address patients with comorbidity conditions and those who are serving them often do not have a direct link to public health agencies. Therefore, even if the community strategies discussed here are coordinated either by the health systems or their partners, the use of a blockchain can as an inter-organizational platform or gateway to track patient progress. The demographic characteristics of the de-identified patient information can even be shared with public health agencies using blockchain technology for epidemiological research. In fact, many public health agencies partner with other organizations that address smoking cessation, health screening of rural or minority populations, recuperative and rehabilitative care of homeless populations, and glucose monitoring of diabetic patients, etc. However, they do not have a mechanism to track services provided to similar population groups.
In summary, a blockchain architecture created by public health agencies or healthcare systems can allow multiple agencies that use their own strategies to address different health conditions of populations to share the progress made by patients for real time analysis of patient adherence and create opportunities for greater collaboration among partnering organizations servicing diverse needs of populations within a particular region. Supporting collaboration in developing community strategies to create preventive strategies that address multiple social determinants has been advocated as a part of Public Health 3.0 (
DeSalvo et al. 2016), and blockchain architecture can be an effective trusted distributed digital platform to support the data sharing needed to coordinate preventive care and improve health outcomes.
6. Conclusions, Limitations, and Directions for Future Research
In this paper, we present a general resource sharing conceptual model in blockchain. We demonstrate using multiple use cases in coordinated care in health how this resource sharing model can help implement the system using blockchain such that multiple care providers and patients can participate to support continuity of care. Current limitations in the sharing of data and coordinating activities using a single trusted entity led to the consideration of a blockchain architecture that supports the engagement of a distributed set of actors using a secure platform that has shown promise in healthcare and other domains. Using a design science approach, a resource sharing model was proposed to align the goals of actors through the resource they share, while simultaneously using that or other resources to coordinate their activities. Two implementations of blockchain are used to illustrate how such goal alignment is needed in support of care delivery outside a hospital. This led to identifying constructs such as creators, owners, and users and how they interact to share resources in a generalized resource sharing model. This model is compared with Bitcoin to develop a conceptual model that leverages resource sharing to support both care delivery and stakeholder goal alignment. Currently, one of the use cases that provides resources to patients who participated in a clinical trial is using visualization of resource sharing to improve ease of use and engender trust in the overall system (
Peral et al. 2020).
Limitations and Directions for Future Research
The primary focus of this paper is on developing a conceptual model to design blockchain applications to support care continuity or prevention in healthcare. We discussed how the model can be validated by using it in other cases discussed in
Section 5. The focus is on the model’s generalization capability at a conceptual level. One can argue that we have not used this model to build an application and validated its capability to meet the desired goals of stakeholders involved. We view validation at a conceptual level separate from validation of application effectiveness to reach a desired outcome. The following discussion looks at the validation effectiveness as a limitation of our current research and suggests three directions for future research, along with the technical and social challenges discussed in the paper. These include establishing the metrics for outcome evaluation, evaluating applications on established metrics to reach desired outcomes, and using data analytics to improve the outcomes.
Establishing the metrics for outcome evaluation: While business organizations have specific drivers to transform their operations so they can share resources among their partners to support customer related outcomes, public sector agencies are often challenged in establishing the metrics for transforming their operations to support citizens. For example, one of the studies that used blockchain technology to transform public sector operations used public sector theory to categorize dimensions of public value along improved administration and improved social value and chose improved administration as a metric for its transformation and validation (
Shahaab et al. 2023). One of the cases discussed in
Section 5 (PHC) is currently reviewing how its current model of engaging participants using wearable technologies can be validated as social value metrics such as the wellness behavior by reducing obesity and hypertension using blockchain (
Tanniru 2023).
Evaluating applications on established metrics to reach desired outcomes: There has been significant discussion on how much of the resource gathered in system design should be off-the-chain and how much will remain on-the-chain to ensure privacy and security of the resource shared (
Miyachi and Mackey 2021). Since the amount of data shared to support care continuity can be extensive, it is critical to decide how this resource is managed. We discuss in Case 2 of the paper how storage efficiency has guided the clinical data to be categorized along a number of dimensions for making off-the-chain and on-the-chain decisions. In the PHC case, the partners include clinical providers as well as community organizations and they both need different types of information from patient wearables to analyze patient adherence on clinical or behavioral dimensions. Our future work will explore what data will be off-the-chain and on-the-chain to support patient privacy and who will have access to this data.
Using data analytics to improve outcomes: As discussed in prior research on how Industry 4.0 is creating opportunities to collect large amount of sensor data to track and analyze data to improve performance (
Khan et al. 2019), and how the use of such sensor data can lead to big data and machine learning algorithms to predict diseases (
Ali et al. 2022), the challenge is in determining how such sensor data become a part of the blockchain for real time analysis of patient adherence. While we have analyzed the potential use of non-clinical data using blockchain technology for understanding gaps in adherence to address a social goal (
Tanniru and Tanniru 2020) and the role of patient consent data to improve their engagement in clinical trials as an administrative goal (
Peral et al. 2020), we have not looked at the use of data challenges when patient wearables create opportunities to collect large volume of sensor data. However, this is an area we need to explore in the future for the PHC case, as we collect wearable data and share it with primary care physicians for clinical analysis and with wellness educators for behavioral analysis.
Addressing technical and social challenges: The complexity of the partner network (heterogeneity of the actors involved and number of actors who need to share resources) can increase the technical challenge of supporting resource sharing among these actors. The diversity of goals of actors and the resources that align these goals may also pose a larger social challenge. For example, patients needing to share information on their diagnosis and treatment decisions may want to interact with peers and experts outside the hospital network and/or physicians (e.g., financing a treatment that can be expensive), and no single blockchain network platform may be appropriate given the nature of information shared (e.g., clinical, opinion based, experiences, etc.). While all are a part of the resource bundle that can influence patient decision making, some may be left outside the blockchain exchange system to reduce complexities associated with privacy and security.
The technical complexity of dealing with large partner networks to address scalability (
Croman et al. 2016) has been widely discussed using multiple approaches. Some of the strategies here include segmenting the network when appropriate (i.e., into networks supporting different user types: pharmacists, diagnostic labs, researchers who want to analyze anonymized data, etc.), coding the resource to reduce size (i.e., Case 1 stores large volumes of data outside the network with only coded links stored in the blockchain), or segmenting of the users (i.e., Case 2 separates payers of patients’ clinical data from those who provide patients for social services). Even when multiple side-networks are used to address scalability, auditability of the resources shared across networks can be addressed using synchronization of the resources shared among multiple networks.
Within healthcare, as health systems focused on reducing readmission costs, they may segment the patient ecosystem into those who go to nursing homes from those who go home but need to maintain their health condition. For example, patients who go to nursing homes want to connect with family members to stay connected, and nursing home staff and hospitals want to consult with specialists to improve quality of care. This means the resource shared in the platform is different in each case: social interaction between patients and family; patient clinical consultation between physicians and specialists; and patient diagnostic and prescription data between hospitals and nursing home staff. A mix of resource sharing platforms may be needed to support the alignment of goals of each of these actors, while maintaining consistency and auditability if resources are shared across these platforms.
If patients return home to maintain their health, their goals to seek answers to questions and receive reminders on any follow-up activities may be influenced by availability and confidentiality of the data shared. Similarly, hospitals refer the patients to social service agencies for access to care. It is not necessary that all these needs have to be supported by blockchain and one may use a mix of social media, hospital coordinated systems, and blockchain for resource sharing. Similarly, urban patient populations who are economically challenged, educated older populations interested in self-management of their health, seniors with chronic care conditions, etc., may have different goals and this may call for segmentation of data to ensure confidentiality as well as integrity, so it is consistently shared among a number of social and community service providers.
In summary, the extended healthcare network of patients, providers, and partners may have to address not just the technology and operational risk associated with the mix of platforms that support communication of resource and coordination of activities, but also the alignment of customer or patient goals as they seek to share information with their clinical and non-clinical care providers. In these cases, the platform chosen has to address some of the customer risks when they move from a centrally controlled and coordinated system to a distributed blockchain architecture. Models that support these decisions are needed as the application space spans a broader collection of actors with varying goals and technological maturity and need a mix of resources to be shared to influence their participation.





{kind=link}
{kind=link}