
Combination of Risks of BMI and Health-Related Lifestyles on Kidney Function in the Prediabetic Japanese Population: A Prospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
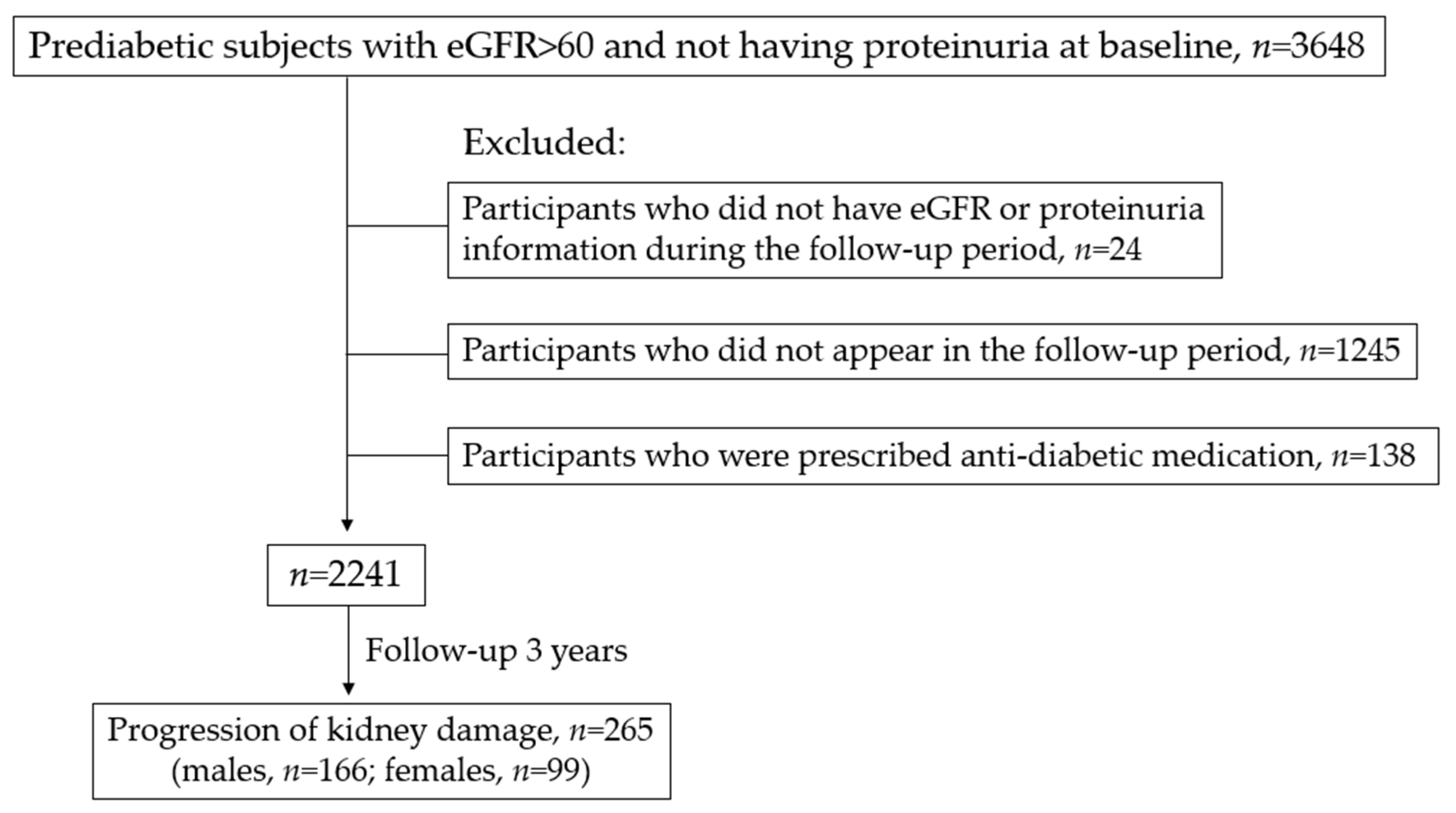
2.1. Study Subjects and Data Extraction
2.2. Study Design
2.3. Measures and Definitions
2.4. Statistical Analysis
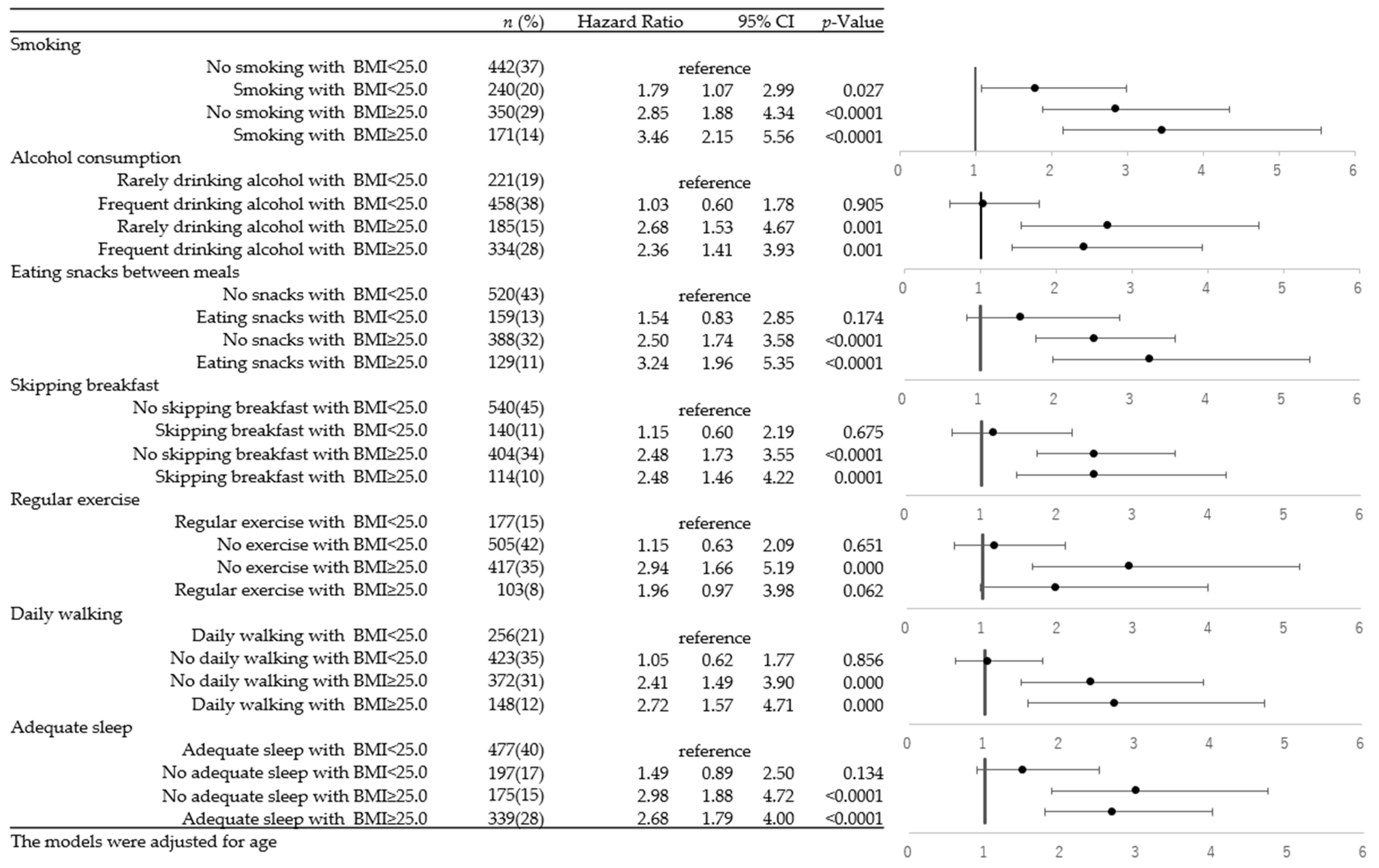
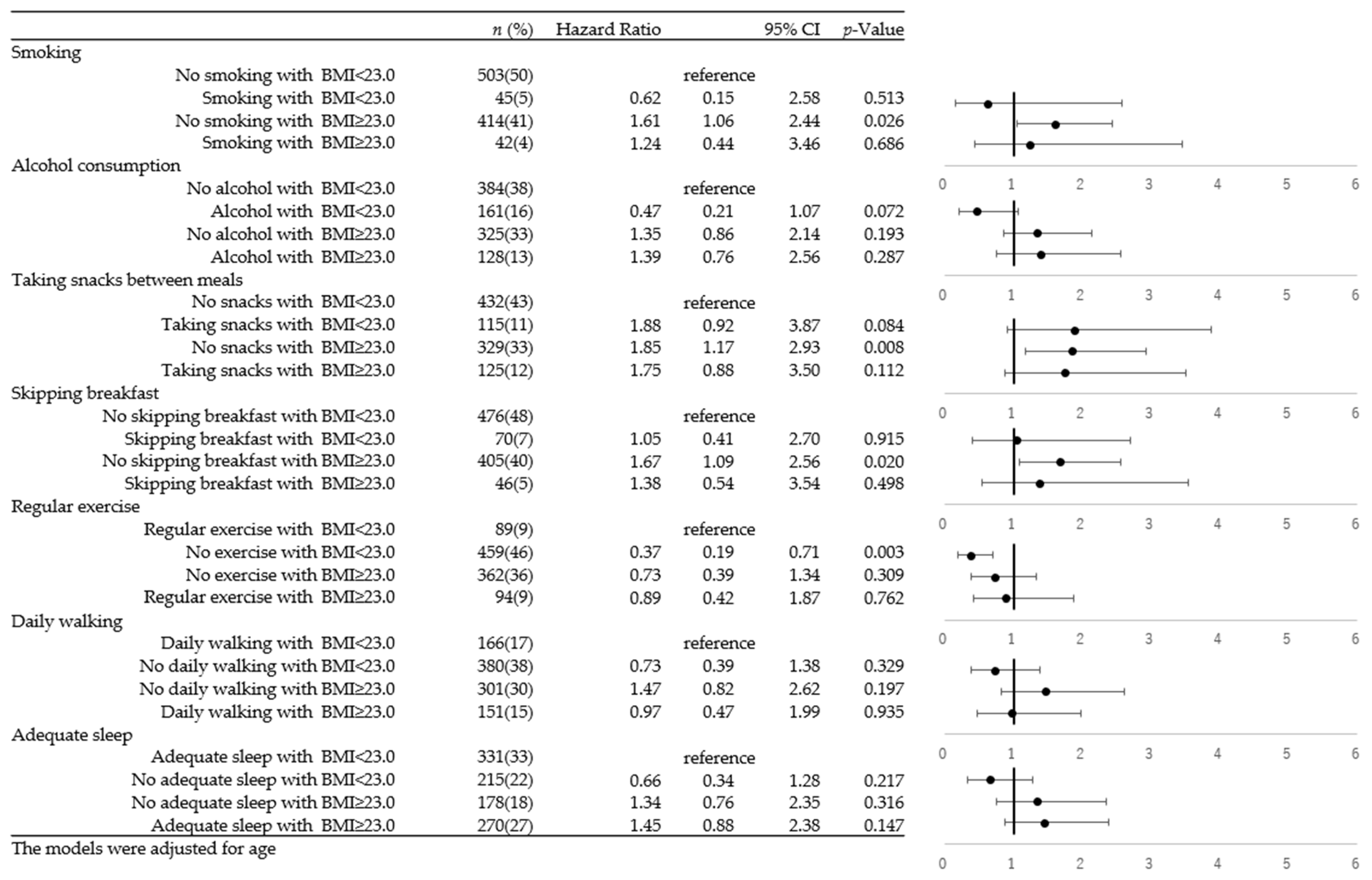
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nagata, M.; Ninomiya, T.; Doi, Y.; Yonemoto, K.; Kubo, M.; Hata, J.; Tsuruya, K.; Iida, M.; Kiyohara, Y. Trends in the prevalence of chronic kidney disease and its risk factors in a general Japanese population: The Hisayama Study. Nephrol. Dial. Transplant. 2010, 25, 2557–2564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levey, A.S.; Coresh, J.; Balk, E.; Kausz, A.T.; Levin, A.; Steffes, M.W.; Hogg, R.J.; Perrone, R.D.; Lau, J.; Eknoyan, G.; et al. National Kidney Foundation practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Ann. Intern. Med. 2003, 139, 137–147. [Google Scholar] [CrossRef]
- Yoshida, Y.; Kashiwabara, K.; Hirakawa, Y.; Tanaka, T.; Noso, S.; Ikegami, H.; Ohsugi, M.; Ueki, K.; Mita, T.; Watada, H.; et al. Conditions, pathogenesis, and progression of diabetic kidney disease and early decliner in Japan. BMJ Open Diabetes Res. Care 2020, 8, e000902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Boer, I.H.; Rue, T.C.; Hall, Y.N.; Heagerty, P.J.; Weiss, N.S.; Himmelfarb, J. Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA 2011, 305, 2532–2539. [Google Scholar] [CrossRef]
- Rabkin, R. Diabetic nephropathy. Clin. Cornerstone 2003, 5, 1–11. [Google Scholar] [CrossRef]
- Afkarian, M.; Sachs, M.C.; Kestenbaum, B.; Hirsch, I.B.; Tuttle, K.R.; Himmelfarb, J.; de Boer, I.H. Kidney disease and increased mortality risk in type 2 diabetes. J. Am. Soc. Nephrol. 2013, 24, 302–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jude, E.B.; Anderson, S.G.; Cruickshank, J.K.; Srivatsa, A.; Tentolouris, N.; Chandrasekaran, R.; Gokal, R.; Boulton, A.J. Natural history and prognostic factors of diabetic nephropathy in type 2 diabetes. QJM 2002, 95, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Park, S.W.; Cho, Y.W.; Kim, S.K. Higher Prevalence and Progression Rate of Chronic Kidney Disease in Elderly Patients with Type 2 Diabetes Mellitus. Diabetes Metab. J. 2018, 42, 224–232. [Google Scholar] [CrossRef]
- Thornton Snider, J.; Sullivan, J.; van Eijndhoven, E.; Hansen, M.K.; Bellosillo, N.; Neslusan, C.; O’Brien, E.; Riley, R.; Seabury, S.; Kasiske, B.L. Lifetime benefits of early detection and treatment of diabetic kidney disease. PLoS ONE 2019, 14, e0217487. [Google Scholar] [CrossRef] [PubMed]
- Schrauben, S.J.; Apple, B.J.; Chang, A.R. Modifiable Lifestyle Behaviors and CKD Progression: A Narrative Review. Kidney360 2022, 3, 752–778. [Google Scholar] [CrossRef]
- Ozieh, M.N.; Egede, L.E. A Lifestyle Intervention to Delay Early Chronic Kidney Disease in African Americans with Diabetic Kidney Disease: Pre-Post Pilot Study. JMIR Form. Res. 2022, 6, e34029. [Google Scholar] [CrossRef] [PubMed]
- Docherty, N.G.; Canney, A.L.; Le Roux, C.W. Weight loss interventions and progression of diabetic kidney disease. Curr. Diabetes Rep. 2015, 15, 55. [Google Scholar] [CrossRef] [PubMed]
- Duan, J.; Wang, C.; Liu, D.; Qiao, Y.; Pan, S.; Jiang, D.; Zhao, Z.; Liang, L.; Tian, F.; Yu, P.; et al. Prevalence and risk factors of chronic kidney disease and diabetic kidney disease in Chinese rural residents: A cross-sectional survey. Sci. Rep. 2019, 9, 10408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyazawa, I.; Kadota, A.; Miura, K.; Okamoto, M.; Nakamura, T.; Ikai, T.; Maegawa, H.; Ohnishi, A. Twelve-year trends of increasing overweight and obesity in patients with diabetes: The Shiga Diabetes Clinical Survey. Endocr. J. 2018, 65, 527–536. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.Y.; Choi, D.H.; Jung, C.H.; Mok, J.O.; Kim, C.H. Associations between obesity, weight change and decreased renal function in Korean type 2 diabetic patients: A longitudinal follow-up study. BMC Endocr. Disord. 2021, 21, 188. [Google Scholar] [CrossRef]
- Sakurai, M.; Kobayashi, J.; Takeda, Y.; Nagasawa, S.Y.; Yamakawa, J.; Moriya, J.; Mabuchi, H.; Nakagawa, H. Sex Differences in Associations among Obesity, Metabolic Abnormalities, and Chronic Kidney Disease in Japanese Men and Women. J. Epidemiol. 2016, 26, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Araki, E.; Goto, A.; Kondo, T.; Noda, M.; Noto, H.; Origasa, H.; Osawa, H.; Taguchi, A.; Tanizawa, Y.; Tobe, K.; et al. Japanese Clinical Practice Guideline for Diabetes 2019. Diabetol. Int. 2020, 11, 165–223. [Google Scholar] [CrossRef]
- Anuurad, E.; Shiwaku, K.; Nogi, A.; Kitajima, K.; Enkhmaa, B.; Shimono, K.; Yamane, Y. The new BMI criteria for asians by the regional office for the western pacific region of WHO are suitable for screening of overweight to prevent metabolic syndrome in elder Japanese workers. J. Occup. Health 2003, 45, 335–343. [Google Scholar] [CrossRef]
- Morisaki, N.; Nagata, C.; Jwa, S.C.; Sago, H.; Saito, S.; Oken, E.; Fujiwara, T. Pre-pregnancy BMI-specific optimal gestational weight gain for women in Japan. J. Epidemiol. 2017, 10, 492–498. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Kinoshita, M.; Yokote, K.; Arai, H.; Iida, M.; Ishigaki, Y.; Ishibashi, S.; Umemoto, S.; Egusa, G.; Ohmura, H.; Okamura, T.; et al. Japan Atherosclerosis Society (JAS) Guidelines for Prevention of Atherosclerotic Cardiovascular Diseases 2017. J. Atheroscler. Thromb. 2018, 25, 846–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olivo, R.E.; Davenport, C.A.; Diamantidis, C.J.; Bhavsar, N.A.; Tyson, C.C.; Hall, R.; Bidulescu, A.; Young, B.; Mwasongwe, S.E.; Pendergast, J.; et al. Obesity and synergistic risk factors for chronic kidney disease in African American adults: The Jackson Heart Study. Nephrol. Dial. Transplant. 2018, 33, 992–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gündoğdu, Y.; Anaforoğlu, I. Effects of Smoking on Diabetic Nephropathy. Front. Clin. Diabetes Healthc. 2022, 3, 826383. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.C.; Burrell, L.M.; Black, M.J.; Wu, L.L.; Dilley, R.J.; Cooper, M.E.; Johnston, C.I. Salt induces myocardial and renal fibrosis in normotensive and hypertensive rats. Circulation 1998, 98, 2621–2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Curhan, G.C. Associations of sugar and artificially sweetened soda with albuminuria and kidney function decline in women. Clin. J. Am. Soc. Nephrol. 2011, 6, 160–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St-Onge, M.P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K.; American Heart Association Obesity Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- García-Carro, C.; Vergara, A.; Bermejo, S.; Azancot, M.A.; Sellarés, J.; Soler, M.J. A Nephrologist Perspective on Obesity: From Kidney Injury to Clinical Management. Front. Med. 2021, 8, 655871. [Google Scholar] [CrossRef]
- Fan, Z.; Yun, J.; Yu, S.; Yang, Q.; Song, L. Alcohol Consumption Can be a “Double-Edged Sword” for Chronic Kidney Disease Patients. Med. Sci. Monit. 2019, 25, 7059–7072. [Google Scholar] [CrossRef]
- Joo, Y.S.; Koh, H.; Nam, K.H.; Lee, S.; Kim, J.; Lee, C.; Yun, H.R.; Park, J.T.; Kang, E.W.; Chang, T.I.; et al. Alcohol Consumption and Progression of Chronic Kidney Disease: Results from the Korean Cohort Study for Outcome in Patients with Chronic Kidney Disease. Mayo Clin. Proc. 2020, 95, 293–305. [Google Scholar] [CrossRef]
- Xiong, J.; Peng, H.; Yu, Z.; Chen, Y.; Pu, S.; Li, Y.; Huang, X.; Tang, X.; He, J.; Shi, Y.; et al. Daily Walking Dose and Health-related Quality of Life in Patients with Chronic Kidney Disease. J. Ren. Nutr. 2022, 32, 710–717. [Google Scholar] [CrossRef]
- Maric-Bilkan, C. Obesity and diabetic kidney disease. Med. Clin. N. Am. 2013, 97, 59–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva Junior, G.B.; Bentes, A.C.; Daher, E.F.; Matos, S.M. Obesity and kidney disease. J. Bras. Nefrol. 2017, 39, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Martin, W.P.; White, J.; López-Hernández, F.J.; Docherty, N.G.; Le Roux, C.W. Metabolic Surgery to Treat Obesity in Diabetic Kidney Disease, Chronic Kidney Disease, and End-Stage Kidney Disease; What Are the Unanswered Questions? Front. Endocrinol. 2020, 11, 289. [Google Scholar] [CrossRef] [PubMed]
- Maskarinec, G.; Raquinio, P.; Kristal, B.S.; Franke, A.A.; Buchthal, S.D.; Ernst, T.M.; Monroe, K.R.; Shepherd, J.A.; Shvetsov, Y.B.; Le Marchand, L.; et al. Body Fat Distribution, Glucose Metabolism, and Diabetes Status Among Older Adults: The Multiethnic Cohort Adiposity Phenotype Study. J. Epidemiol. 2022, 32, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Pop, L.M.; Iorga, M.; Șipoș, L.R.; Iurcov, R. Gender Differences in Healthy Lifestyle, Body Consciousness, and the Use of Social Networks among Medical Students. Medicina 2021, 57, 648. [Google Scholar] [CrossRef] [PubMed]
- Bärebring, L.; Palmqvist, M.; Winkvist, A.; Augustin, H. Gender differences in perceived food healthiness and food avoidance in a Swedish population-based survey: A cross sectional study. Nutr. J. 2020, 19, 140. [Google Scholar] [CrossRef]
- Kattah, A.G.; Garovic, V.D. Understanding sex differences in progression and prognosis of chronic kidney disease. Ann. Transl. Med. 2020, 8, 897. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Total, n = 2241 | Male, n = 1226 | Female, n = 1015 | p-Value | |
|---|---|---|---|---|
| Demographic | ||||
| Age, years | 52.7 ± 13.3 | 50.4 ± 13.6 | 55.4 ± 12.2 | <0.001 |
| Age group | <0.001 | |||
| <40 years | 391 (17.5%) | 287 (23.4%) | 104 (10.3%) | |
| 40–65 years | 1492 (66.5%) | 780 (63.6%) | 712 (70.1%) | |
| >65 years | 358 (16.0%) | 159 (13.0%) | 199 (19.6%) | |
| Comorbidities and clinical values | ||||
| Baseline eGFR | 77.4 ± 12.0 | 78.1 ± 12.0 | 76.6 ± 12.0 | 0.002 |
| BMI | 24.1 ± 3.9 | 24.9 ± 3.8 | 23.2 ± 3.9 | <0.001 |
| BMI category | <0.001 | |||
| ≥30 | 167 (7.5%) | 111 (9.1%) | 56 (5.5%) | |
| 25–29 | 639 (28.5%) | 416 (33.9%) | 223 (22.0%) | |
| <25 | 1435 (64.0%) | 699 (57.0%) | 736 (72.5%) | |
| Hypertension | 0.003 | |||
| Yes | 767 (34.2%) | 453 (37.0%) | 314 (30.9%) | |
| No | 1474 (65.8%) | 773 (63.1%) | 701 (69.1%) | |
| Dyslipidemia | <0.001 | |||
| Yes | 1001 (44.7%) | 609 (49.7%) | 392 (38.6%) | |
| No | 1240 (55.3%) | 617 (50.3%) | 623 (61.4%) | |
| Uric acid 1 | 5.3 ± 1.4 | 6.0 ± 1.2 | 4.5 ± 1.0 | <0.001 |
| Hemoglobin A1c 2 | 5.9 ± 0.5 | 5.9 ± 0.6 | 5.9 ± 0.4 | 0.857 |
| Lifestyle factors | ||||
| Smoking 3 | <0.001 | |||
| Yes | 498 (22.6%) | 411 (34.2%) | 87 (8.7%) | |
| No | 1709 (77.4%) | 792 (65.8%) | 917 (91.3%) | |
| Regular exercise 4 | 0.004 | |||
| Yes | 463 (21.0%) | 280 (23.3%) | 183 (18.2%) | |
| No | 1743 (79.0%) | 922 (76.7%) | 821 (81.8%) | |
| Alcohol consumption 5 | <0.001 | |||
| Everyday | 474 (21.6%) | 404 (33.7%) | 70 (7.0%) | |
| Sometimes | 607 (27.6%) | 388 (32.4%) | 219 (21.9%) | |
| Rarely | 1115 (50.8%) | 406 (33.9%) | 709 (71.0%) | |
| Daily walking 6 | 0.337 | |||
| Yes | 721 (32.8%) | 404 (33.7%) | 317 (31.8%) | |
| No | 1476 (67.2%) | 795 (66.3%) | 681 (68.2%) | |
| Eating snacks 6 | 0.955 | |||
| Yes | 528 (24.0%) | 288 (24.1%) | 240 (24.0%) | |
| No | 1669 (76.0%) | 908 (75.9%) | 761 (76.0%) | |
| Skipping breakfast 7 | <0.001 | |||
| Yes | 370 (16.9%) | 254 (21.2%) | 116 (11.6%) | |
| No | 1825 (83.1%) | 944 (78.8%) | 881 (88.4%) | |
| Adequate sleep 8 | <0.001 | |||
| Yes | 1417 (65.0%) | 816 (68.7%) | 601 (60.5%) | |
| No | 765 (35.0%) | 372 (31.3%) | 393 (39.5%) | |
| Kidney damage progression | 0.005 | |||
| Yes | 265 (11.8%) | 166 (13.5%) | 99 (9.7%) | |
| No | 1976 (88.2%) | 1060 (86.5%) | 916 (90.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-Y.; Deng, S.; Wagatsuma, Y. Combination of Risks of BMI and Health-Related Lifestyles on Kidney Function in the Prediabetic Japanese Population: A Prospective Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 5338. https://doi.org/10.3390/ijerph20075338
Chen J-Y, Deng S, Wagatsuma Y. Combination of Risks of BMI and Health-Related Lifestyles on Kidney Function in the Prediabetic Japanese Population: A Prospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(7):5338. https://doi.org/10.3390/ijerph20075338
Chicago/Turabian StyleChen, Jou-Yin, Shiqi Deng, and Yukiko Wagatsuma. 2023. "Combination of Risks of BMI and Health-Related Lifestyles on Kidney Function in the Prediabetic Japanese Population: A Prospective Cohort Study" International Journal of Environmental Research and Public Health 20, no. 7: 5338. https://doi.org/10.3390/ijerph20075338