
Point Prevalence Survey of Antimicrobial Use in Selected Tertiary Care Hospitals of Pakistan Using WHO Methodology: Results and Inferences

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Settings
2.3. Duration
2.4. Sample Size and Sampling Technique
2.5. Survey Tool and Data Collection
2.6. Inclusion Criteria
- ∘
- Patients in acute tertiary care hospitals registered in GLASS sentinel sites;
- ∘
- Patients hospitalized before or at 08:00 hours on the days of the PPS whether they are receiving antibiotics or not and those patients who have complete medical record;
- ∘
- Data of all patients admitted in acute care settings were included;
- ∘
- Only antibiotics included in list administered by oral, parenteral, rectal, or inhalation routes;
- ∘
- Antibiotic therapy initiated by 08:00 am on survey day.
2.7. Exclusion Criteria
- ∘
- Patients from nursing homes, rehabilitation centers, and psychiatric centers are excluded as per WHO PPS methodology;
- ∘
- Patients admitted after 08:00 am on day of survey, all day care patients;
- ∘
- Inpatients from long-term care wards, Emergency departments, day surgery wards, day care wards (e.g., renal dialysis), outpatient clinic, day surgery/day treatment, outpatient dialysis, discharged patients, and waiting for transportation;
- ∘
- Patients receiving ophthalmologic antibiotics.
2.8. Analysis Plan
3. Results
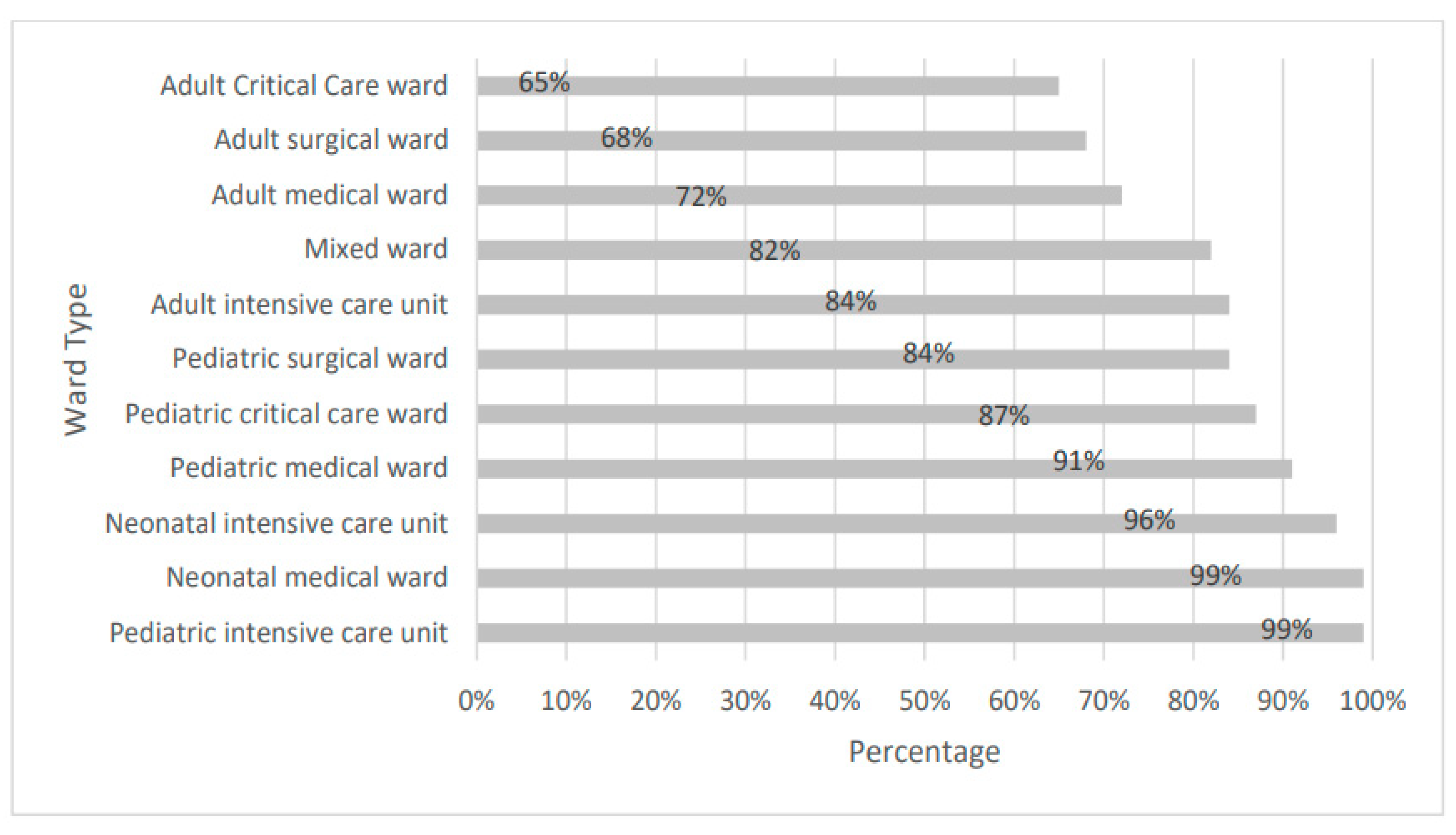
3.1. Prevalence and Demographics
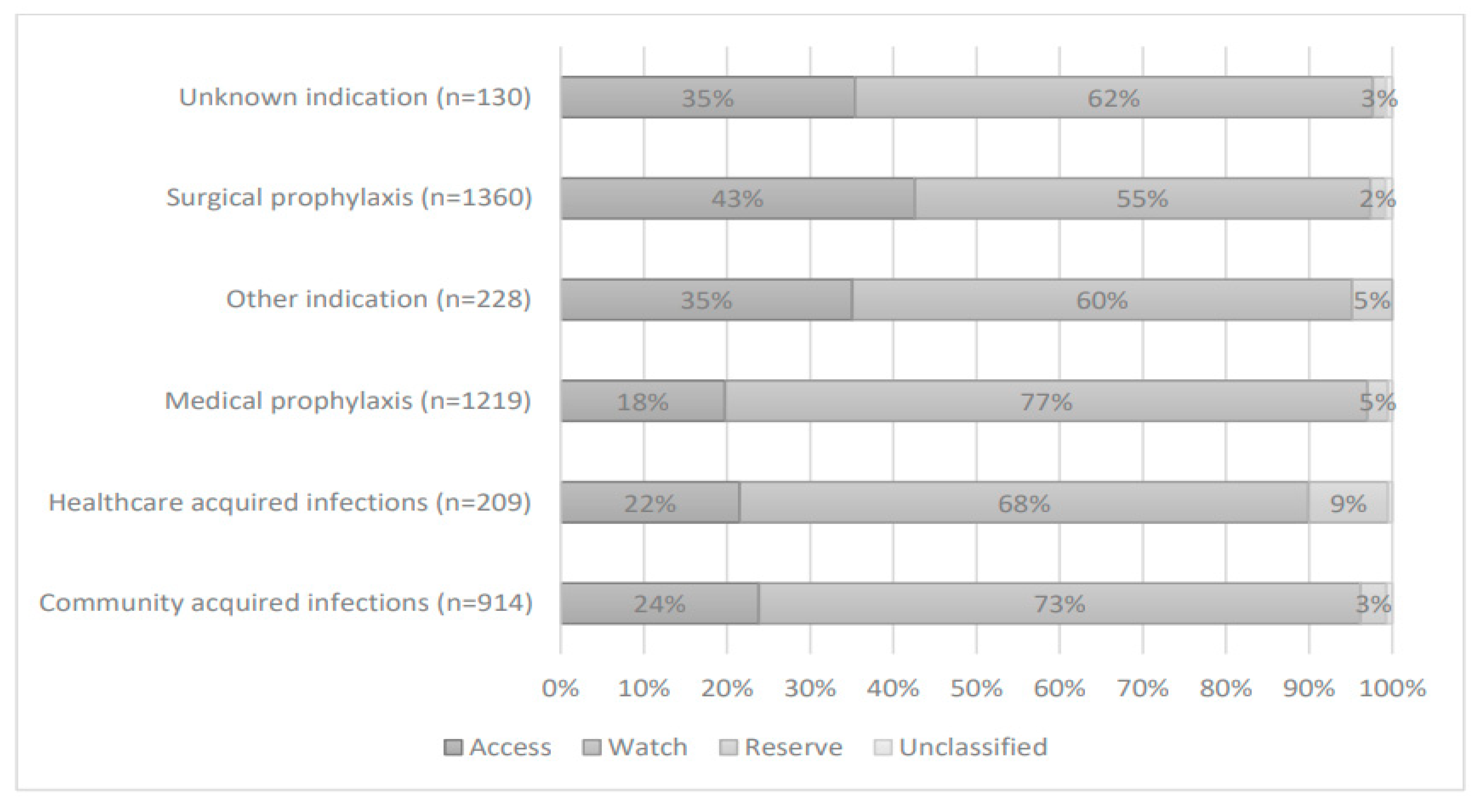
3.2. Antibiotic Use and Prescription Rate
3.3. Factors Affecting Compliance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saleem, Z.; Hassali, M.A. Travellers take heed: Outbreak of extensively drug resistant (XDR) typhoid fever in Pakistan and a warning from the US CDC. Travel Med. Infect. Dis. 2019, 27, 127. [Google Scholar] [CrossRef]
- Majumder, M.A.A.; Rahman, S.; Cohall, D.; Bharatha, A.; Singh, K.; Haque, M.; Gittens-St Hilaire, M. Antimicrobial stewardship: Fighting antimicrobial resistance and protecting global public health. Infect. Drug Resist. 2020, 13, 4713–4738. [Google Scholar] [CrossRef] [PubMed]
- Robert, J.; Pean, Y.; Varon, E.; Bru, J.P.; Bedos, J.P.; Bertrand, X.; Lepape, A.; Stahl, J.P.; Gauzit, R. Point prevalence survey of antibiotic use in French hospitals in 2009. J. Antimicrob. Chemother. 2012, 67, 1020–1026. [Google Scholar] [CrossRef] [Green Version]
- Kiggundu, R.; Wittenauer, R.; Waswa, J.; Nakambale, H.N.; Kitutu, F.E.; Murungi, M.; Okuna, N.; Morries, S.; Lawry, L.L.; Joshi, M.P.; et al. Point Prevalence Survey of Antibiotic Use across 13 Hospitals in Uganda. Antibiotics 2022, 11, 199. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. 2016. Available online: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (accessed on 12 May 2023).
- Brogan, D.M.; Mossialos, E. A critical analysis of the review on antimicrobial resistance report and the infectious disease financing facility. Glob. Health 2016, 12, 8. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, C.; Sarkar, P.; Issa, R.; Haldar, J. Alternatives to Conventional Antibiotics in the Era of Antimicrobial Resistance. Trends Microbiol. 2019, 27, 323–338. [Google Scholar] [CrossRef]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.-F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. 2018, 6, e619–e629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Versporten, A.; Hashmi, F.K.; Saeed, H.; Saleem, F.; Salman, M.; Rehman, I.U.; Khan, T.M. Point prevalence surveys of antimicrobial use: A systematic review and the implications. Expert Rev. Anti-Infect. Ther. 2020, 18, 897–910. [Google Scholar] [CrossRef]
- Zhang, J.-S.; Liu, G.; Zhang, W.-S.; Shi, H.-Y.; Lu, G.; Zhao, C.-A.; Li, C.-C.; Li, Y.-Q.; Shao, Y.-N.; Tian, D.-Y.; et al. Antibiotic usage in Chinese children: A point prevalence survey. World J. Pediatr. 2018, 14, 335–343. [Google Scholar] [CrossRef]
- Klein, E.Y.; Van Boeckel, T.P.; Martinez, E.M.; Pant, S.; Gandra, S.; Levin, S.A.; Laxminarayan, R. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc. Natl. Acad. Sci. USA 2018, 115, E3463–E3470. [Google Scholar] [CrossRef] [Green Version]
- Saleem, Z.; Hassali, M.A.; Hashmi, F.K. Pakistan’s national action plan for antimicrobial resistance: Translating ideas into reality. Lancet Infect. Dis. 2018, 18, 1066–1067. [Google Scholar] [CrossRef] [PubMed]
- Boucher, H.W.; Bakken, J.S.; Murray, B.E. The United Nations and the Urgent Need for Coordinated Global Action in the Fight Against Antimicrobial Resistance. Ann. Intern. Med. 2016, 165, 812–813. [Google Scholar] [CrossRef] [PubMed]
- Arif, S.; Sadeeqa, S.; Saleem, Z. Patterns of Antimicrobial Use in Hospitalized Children: A Repeated Point Prevalence Survey from Pakistan. J. Pediatr. Infect. Dis. Soc. 2021, 10, 970–974. [Google Scholar] [CrossRef] [PubMed]
- Versporten, A.; Bielicki, J.; Drapier, N.; Sharland, M.; Goossens, H.; ARPEC Project Group; Calle, G.M.; Garrahan, J.P.; Clark, J.; Cooper, C.; et al. The Worldwide Antibiotic Resistance and Prescribing in European Children (ARPEC) point prevalence survey: Developing hospital-quality indicators of antibiotic prescribing for children. J. Antimicrob. Chemother. 2016, 71, 1106–1117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plachouras, D.; Kärki, T.; Hansen, S.; Hopkins, S.; Lyytikäinen, O.; Moro, M.L.; Reilly, J.; Zarb, P.; Zingg, W.; Kinross, P.; et al. Antimicrobial use in European acute care hospitals: Results from the second point prevalence survey (PPS) of healthcare-associated infections and antimicrobial use, 2016 to 2017. Eurosurveillance 2018, 23, 1800393. [Google Scholar] [CrossRef] [Green Version]
- Amponsah, O.K.O.; Buabeng, K.O.; Owusu-Ofori, A.; Ayisi-Boateng, N.K.; Hämeen-Anttila, K.; Enlund, H. Point prevalence survey of antibiotic consumption across three hospitals in Ghana. JAC-Antimicrob. Resist. 2021, 3, dlab008. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Hashmi, F.K.; Godman, B.; Bhutta, O.A. A repeated point prevalence survey of antimicrobial use in specialized cancer care hospital of Pakistan: Findings and implications. Hosp. Pract. 2019, 47, 149–154. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.A.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Zaidi, S.; Bigdeli, M.; Aleem, N.; Rashidian, A. Access to Essential Medicines in Pakistan: Policy and Health Systems Research Concerns. PLoS ONE 2013, 8, e63515. [Google Scholar] [CrossRef] [Green Version]
- Riaz, H.; Godman, B.; Hussain, S.; Malik, F.; Mahmood, S.; Shami, A.; Bashir, S. Prescribing of bisphosphonates and antibiotics in Pakistan: Challenges and opportunities for the future. J. Pharm. Health Serv. Res. 2015, 6, 111–121. [Google Scholar] [CrossRef] [Green Version]
- Saleem, Z.; Saeed, H.; Ahmad, M.; Yousaf, M.; Hassan, H.B.; Javed, A.; Anees, N.; Maharjan, S. Antibiotic Self-Prescribing Trends, Experiences and Attitudes in Upper Respiratory Tract Infection among Pharmacy and Non-Pharmacy Students: A Study from Lahore. PLoS ONE 2016, 11, e0149929. [Google Scholar] [CrossRef]
- Shaikh, Q.; Sarfaraz, S.; Rahim, A.; Hussain, A.; Behram, S.; Kazi, A.S.; Hussain, M.; Salahuddin, N. WHO Point Prevalence Survey to Describe the Use of Antimicrobials at a Tertiary Care Center in Pakistan: A Situation Analysis for Establishing an Antimicrobial Stewardship Program. Antibiotics 2022, 11, 1555. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Hashmi, F.K.; Godman, B.; Ahmed, Z. Snapshot of antimicrobial stewardship programs in the hospitals of Pakistan: Findings and implications. Heliyon 2019, 5, e02159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2011; WHO Collaborating Centre for Drug Statistics Methodology Norwegian Institute of Public Health: Oslo, Norway, 2010. Available online: https://www.whocc.no/filearchive/publications/2011guidelines.pdf (accessed on 15 September 2022).
- The 2019 WHO AWaRe Classification of Antibiotics for Evaluation and Monitoring of Use; World Health Organization: Geneva, Switzerland, 2019. Available online: https://apps.who.int/iris/handle/10665/327957 (accessed on 15 September 2022).
- Pauwels, I.; Versporten, A.; Drapier, N.; Vlieghe, E.; Goossens, H.; Koraqi, A.; Hoxha, I.; Tafaj, S.; Cornistein, W.; Quiros, R.; et al. Hospital antibiotic prescribing patterns in adult patients according to the WHO Access, Watch and Reserve classification (AWaRe): Results from a worldwide point prevalence survey in 69 countries. J. Antimicrob. Chemother. 2021, 76, 1614–1624. [Google Scholar] [CrossRef]
- Saleem, Z.; Godman, B.; Cook, A.; Khan, M.A.; Campbell, S.M.; Seaton, R.A.; Siachalinga, L.; Haseeb, A.; Amir, A.; Kurdi, A.; et al. Ongoing Efforts to Improve Antimicrobial Utilization in Hospitals among African Countries and Implications for the Future. Antibiotics 2022, 11, 1824. [Google Scholar] [CrossRef] [PubMed]
- Paramadhas, B.D.A.; Tiroyakgosi, C.; Mpinda-Joseph, P.; Morokotso, M.; Matome, M.; Sinkala, F.; Gaolebe, M.; Malone, B.; Molosiwa, E.; Shanmugam, M.G.; et al. Point prevalence study of antimicrobial use among hospitals across Botswana; findings and implications. Expert Rev. Anti-Infect. Ther. 2019, 17, 535–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zain, R.; Ismail, R.; Noor, S.S.; Mohamed, M.; Samsudin, N. Developing an Infection Prevention and Control Educational Program for Critical Care Nurses: Intervention Mapping Protocol and Social Cognitive Theory. Indian J. Forensic Med. Toxicol. 2021, 15, 265–276. [Google Scholar]
- Saleem, Z.; Godman, B.; Hassali, M.A.; Hashmi, F.K.; Azhar, F.; Rehman, I.U. Point prevalence surveys of health-care-associated infections: A systematic review. Ann. Trop. Med. Parasitol. 2019, 113, 191–205. [Google Scholar] [CrossRef]
- Saleem, Z.; Godman, B.; Azhar, F.; Kalungia, A.C.; Fadare, J.; Opanga, S.; Markovic-Pekovic, V.; Hoxha, I.; Saeed, A.; Al-Gethamy, M.; et al. Progress on the national action plan of Pakistan on antimicrobial resistance (AMR): A narrative review and the implications. Expert Rev. Anti-Infect. Ther. 2022, 20, 71–93. [Google Scholar] [CrossRef]
- Afriyie, D.K.; Amponsah, S.; Dogbey, J.; Agyekum, K.; Kesse, S.; Truter, I.; Meyer, J.; Godman, B. A pilot study evaluating the prescribing of ceftriaxone in hospitals in Ghana: Findings and implications. Hosp. Pract. 2017, 45, 143–149. [Google Scholar] [CrossRef]
- Sharland, M.; Gandra, S.; Huttner, B.; Moja, L.; Pulcini, C.; Zeng, M.; Mendelson, M.; Cappello, B.; Cooke, G.; Magrini, N.; et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use—The new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect. Dis. 2019, 19, 1278–1280. [Google Scholar] [CrossRef] [PubMed]
- Labi, A.-K.; Obeng-Nkrumah, N.; Sunkwa-Mills, G.; Bediako-Bowan, A.; Akufo, C.; Bjerrum, S.; Owusu, E.; Enweronu-Laryea, C.; Opintan, J.A.; Kurtzhals, J.A.L.; et al. Antibiotic prescribing in paediatric inpatients in Ghana: A multi-centre point prevalence survey. BMC Pediatr. 2018, 18, 391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haseeb, A.; Saleem, Z.; Altaf, U.; Batool, N.; Godman, B.; Ahsan, U.; Ashiq, M.; Razzaq, M.; Hanif, R.; E-Huma, Z.; et al. Impact of Positive Culture Reports of E. coli or MSSA on De-Escalation of Antibiotic Use in a Teaching Hospital in Pakistan and the Implications. Infect. Drug Resist. 2022, 16, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Godman, B.; Egwuenu, A.; Haque, M.; Malande, O.O.; Schellack, N.; Kumar, S.; Saleem, Z.; Sneddon, J.; Hoxha, I.; Islam, S.; et al. Strategies to Improve Antimicrobial Utilization with a Special Focus on Developing Countries. Life 2021, 11, 528. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, S.W.; Gans, S.L.; Atema, J.J.; Solomkin, J.S.; Dellinger, P.E.; Boermeester, M.A. Timing of preoperative antibiotic prophylaxis in 54,552 patients and the risk of surgical site infection: A systematic review and meta-analysis. Medicine 2017, 96, 29. [Google Scholar] [CrossRef]
- Sefah, I.A.; Denoo, E.Y.; Bangalee, V.; Kurdi, A.; Sneddon, J.; Godman, B. Appropriateness of surgical antimicrobial prophylaxis in a teaching hospital in Ghana: Findings and implications. JAC-Antimicrob. Resist. 2022, 4, dlac102. [Google Scholar] [CrossRef]
- Mwita, J.C.; Ogunleye, O.O.; Olalekan, A.; Kalungia, A.C.; Kurdi, A.; Saleem, Z.; Sneddon, J.; Godman, B. Key Issues Surrounding Appropriate Antibiotic Use for Prevention of Surgical Site Infections in Low- and Middle-Income Countries: A Narrative Review and the Implications. Int. J. Gen. Med. 2021, 14, 515–530. [Google Scholar] [CrossRef]
- Godman, B.; Egwuenu, A.; Wesangula, E.; Schellack, N.; Kalungia, A.C.; Tiroyakgosi, C.; Kgatlwane, J.; Mwita, J.C.; Patrick, O.; Niba, L.L.; et al. Tackling antimicrobial resistance across sub-Saharan Africa: Current challenges and implications for the future. Expert Opin. Drug Saf. 2022, 21, 1089–1111. [Google Scholar] [CrossRef]
- Fadare, J.O.; Ogunleye, O.; Iliyasu, G.; Adeoti, A.; Schellack, N.; Engler, D.; Massele, A.; Godman, B. Status of antimicrobial stewardship programmes in Nigerian tertiary healthcare facilities: Findings and implications. J. Glob. Antimicrob. Resist. 2019, 17, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Godman, B.; Haque, M.; McKimm, J.; Abu Bakar, M.; Sneddon, J.; Wale, J.; Campbell, S.; Martin, A.P.; Hoxha, I.; Abilova, V.; et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: Findings and implications for the future. Curr. Med. Res. Opin. 2019, 36, 301–327. [Google Scholar] [CrossRef]
- Saleem, Z.; Saeed, H.; Hassali, M.A.; Godman, B.; Asif, U.; Yousaf, M.; Ahmed, Z.; Riaz, H.; Raza, S.A. Pattern of inappropriate antibiotic use among hospitalized patients in Pakistan: A longitudinal surveillance and implications. Antimicrob. Resist. Infect. Control 2019, 8, 188. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Cao, S.; Marsh, N.; Ray-Barruel, G.; Flynn, J.; Larsen, E.; Rickard, C. Infection risks associated with peripheral vascular catheters. J. Infect. Prev. 2016, 17, 207–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalsi, J.; Arya, M.; Wilson, P.; Mundy, A. Hospital-acquired urinary tract infection. Int. J. Clin. Pract. 2003, 57, 388–391. [Google Scholar] [CrossRef]
- Saeed, D.K.; Farooqi, J.; Shakoor, S.; Hasan, R. Antimicrobial resistance among GLASS priority pathogens from Pakistan: 2006–2018. BMC Infect. Dis. 2021, 21, 1231. [Google Scholar] [CrossRef]
- Haque, A.; Hussain, K.; Ibrahim, R.; Abbas, Q.; Ahmed, S.A.; Jurair, H.; Ali, S.A. Impact of pharmacist-led antibiotic stewardship program in a PICU of low/middle-income country. BMJ Open Qual. 2018, 7, e000180. [Google Scholar] [CrossRef] [PubMed]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the immune system in humans from infancy to old age. Proc. R. Soc. B Biol. Sci. 2015, 282, 20143085. [Google Scholar] [CrossRef] [Green Version]
- Jamaluddin, N.A.H.; Periyasamy, P.; Lau, C.L.; Ponnampalavanar, S.; Lai, P.S.M.; Ramli, R.; Tan, T.L.; Kori, N.; Yin, M.K.; Azman, N.J.; et al. Point Prevalence Survey of Antimicrobial Use in a Malaysian Tertiary Care University Hospital. Antibiotics 2021, 10, 531. [Google Scholar] [CrossRef] [PubMed]
- National Centre for Antimicrobial Stewardship; Australian Commission on Safety and Quality in Health Care. Antimicrobial Prescribing Practice in Australian Hospitals: Results of the 2015 National Antimicrobial Prescribing Survey; ACSQHC: Sydney, Australia, 2016. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Antimicrobial-prescribing-practice-in-Australian-hospitals-Results-of-the-2015-National-Antimicrobial-Prescribing-Survey.pdf (accessed on 15 September 2022).



{kind=link}
{kind=link}
| Characteristics | Total | |
|---|---|---|
| No. | % | |
| No. of surveyed patients | 3587 | - |
| Mean age of surveyed patients ± SD | 33.4 ± 22.5 | |
| Gender | ||
| Male | 1828 | 51% |
| Female | 1759 | 49% |
| Admission specialty | ||
| Gynecology | 151 | 4% |
| ICU | 152 | 4% |
| Medical | 1276 | 36% |
| Obstetrics/maternity | 150 | 4% |
| Pediatrics and Neonates | 521 | 15% |
| Surgery | 1337 | 37% |
| Length to stay until day of PPS, days median (IQR) | 7 (0–399) | |
| Surgery since admission | 735 | 21% |
| Use of invasive devices | ||
| Central vascular catheter | 155 | 4% |
| Peripheral vascular catheter | 2871 | 80% |
| Endotracheal tube | 123 | 3% |
| Urinary catheter | 943 | 26% |
| Antimicrobials | Antibiotic Use N (%) |
|---|---|
| Ceftriaxone | 1206 (44.0%) |
| Metronidazole | 484 (18.0%) |
| Amoxicillin/Clavulanic acid | 302 (11.0%) |
| Piperacillin/Tazobactam | 297 (10.9%) |
| Amikacin | 257 (9.50%) |
| Meropenem | 200 (7.4%) |
| Cefoperazone + Sulbactum | 183 (6.77%) |
| Vancomycin | 164 (6.0%) |
| Cefotaxime | 151 (5.59%) |
| Moxifloxacin | 132 (4.88%) |
| Factors | Received AM (n = 2701) | Did Not Receive AM (n = 886) | Total | OR | 95% CI | p Value |
|---|---|---|---|---|---|---|
| No. (%) | No. (%) | No. | ||||
| Age | ||||||
| Adults (≥18 yrs.) | 1850 (71) | 760 (29) | 2610 | Ref | ||
| Pediatrics (<18 yrs.) | 666 (85) | 119 (15) | 751 | 2.3 | 1.86–2.84 | 0.000 |
| Neonates (≤1 month) | 185 (96) | 7(4) | 192 | 10.9 | 5.1–23.2 | 0.000 |
| Gender | ||||||
| Male | 1381 (76) | 447 (24) | 1828 | Ref | ||
| Female | 1320 (75) | 439 (25) | 1759 | 0.97 | 0.84–1.13 | 0.726 |
| Surgery (n = 3580) | ||||||
| No Surgery | 2035 (72) | 810 (28) | 2845 | Ref | ||
| Non-NHS (National Healthcare Safety Network) Surgery | 174 (83) | 37 (17) | 211 | 1.87 | 1.3–2.69 | 0.001 |
| NHSN Surgery | 488 (93) | 36 (7) | 524 | 5.4 | 3.8–7.6 | 0.000 |
| Median Length of stay | 4 | 3 | 1.012 | 1.003–1.022 | 0.012 | |
| Admission Specialty | ||||||
| Medical | 909 (71) | 367 (29) | 1276 | Ref | ||
| Gynecology | 108 (72) | 43 (28) | 151 | 1.01 | 0.7–1.47 | 0.942 |
| ICU | 126 (83) | 26 (17) | 152 | 1.96 | 1.26–3.04 | 0.003 |
| OBS and maternity | 120 (80) | 30 (20) | 150 | 1.61 | 1.06–2.45 | 0.025 |
| Pediatrics and Neonates | 494 (95) | 27 (5) | 521 | 7.39 | 4.92–11.09 | 0.000 |
| Surgery | 944 (71) | 393 (29) | 1337 | 0.97 | 0.82–1.15 | 0.722 |
| Invasive procedures | ||||||
| Central vascular catheter (n = 155) | 146 (94) | 9 (6) | 155 | 5.6 | 2.83–10.96 | 0.000 |
| Peripheral vascular catheter (n = 2871) | 2403 (84) | 468 (16) | 2871 | 7.2 | 6.02–8.61 | 0.000 |
| Endotracheal tube (n = 123) | 117 (95) | 6 (5) | 123 | 6.64 | 2.9–15.14 | 0.000 |
| Urinary catheter (n = 943) | 830 (88) | 113 (12) | 943 | 3.03 | 2.45–3.76 | 0.000 |
| Hospital size | ||||||
| Less than 500 | 456 (74) | 160 (26) | 616 | Ref | ||
| From 500 to 1000 beds | 738 (82) | 167 (18) | 905 | 1.55 | 1.21–1.98 | 0.000 |
| More than 1000 beds | 1507 (73) | 559 (27) | 2066 | 0.95 | 0.77–1.16 | 0.594 |
| Hospital Type | ||||||
| Government | 2354 (77) | 719 (23) | 3073 | Ref | ||
| Private | 347 (68) | 167 (32) | 514 | 0.63 | 0.52–0.78 | 0.000 |
| Referred from other hospital (n = 191) | 173 (91) | 18 (9) | 191 | 3.3 | 2.02–5.4 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ambreen, S.; Safdar, N.; Ikram, A.; Baig, M.Z.I.; Farooq, A.; Amir, A.; Saeed, A.; Sabih, F.; Ahsan, Q.; Zafar, A.; et al. Point Prevalence Survey of Antimicrobial Use in Selected Tertiary Care Hospitals of Pakistan Using WHO Methodology: Results and Inferences. Medicina 2023, 59, 1102. https://doi.org/10.3390/medicina59061102
Ambreen S, Safdar N, Ikram A, Baig MZI, Farooq A, Amir A, Saeed A, Sabih F, Ahsan Q, Zafar A, et al. Point Prevalence Survey of Antimicrobial Use in Selected Tertiary Care Hospitals of Pakistan Using WHO Methodology: Results and Inferences. Medicina. 2023; 59(6):1102. https://doi.org/10.3390/medicina59061102
Chicago/Turabian StyleAmbreen, Saadia, Numrah Safdar, Aamer Ikram, Mirza Zeeshan Iqbal Baig, Ayesha Farooq, Afreenish Amir, Asim Saeed, Farah Sabih, Qadeer Ahsan, Alia Zafar, and et al. 2023. "Point Prevalence Survey of Antimicrobial Use in Selected Tertiary Care Hospitals of Pakistan Using WHO Methodology: Results and Inferences" Medicina 59, no. 6: 1102. https://doi.org/10.3390/medicina59061102