

Prevalence and Etiology of Community- and Hospital-Acquired Pneumonia in Saudi Arabia and Their Antimicrobial Susceptibility Patterns: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Design
2.2. Identification of the Research Question
2.3. Eligibility Criteria
2.4. Information Sources
2.5. Search Strategy
2.6. Study Selection
2.7. Data Extraction
2.8. Quality Assessment
2.9. Data Synthesis and Reporting
3. Results
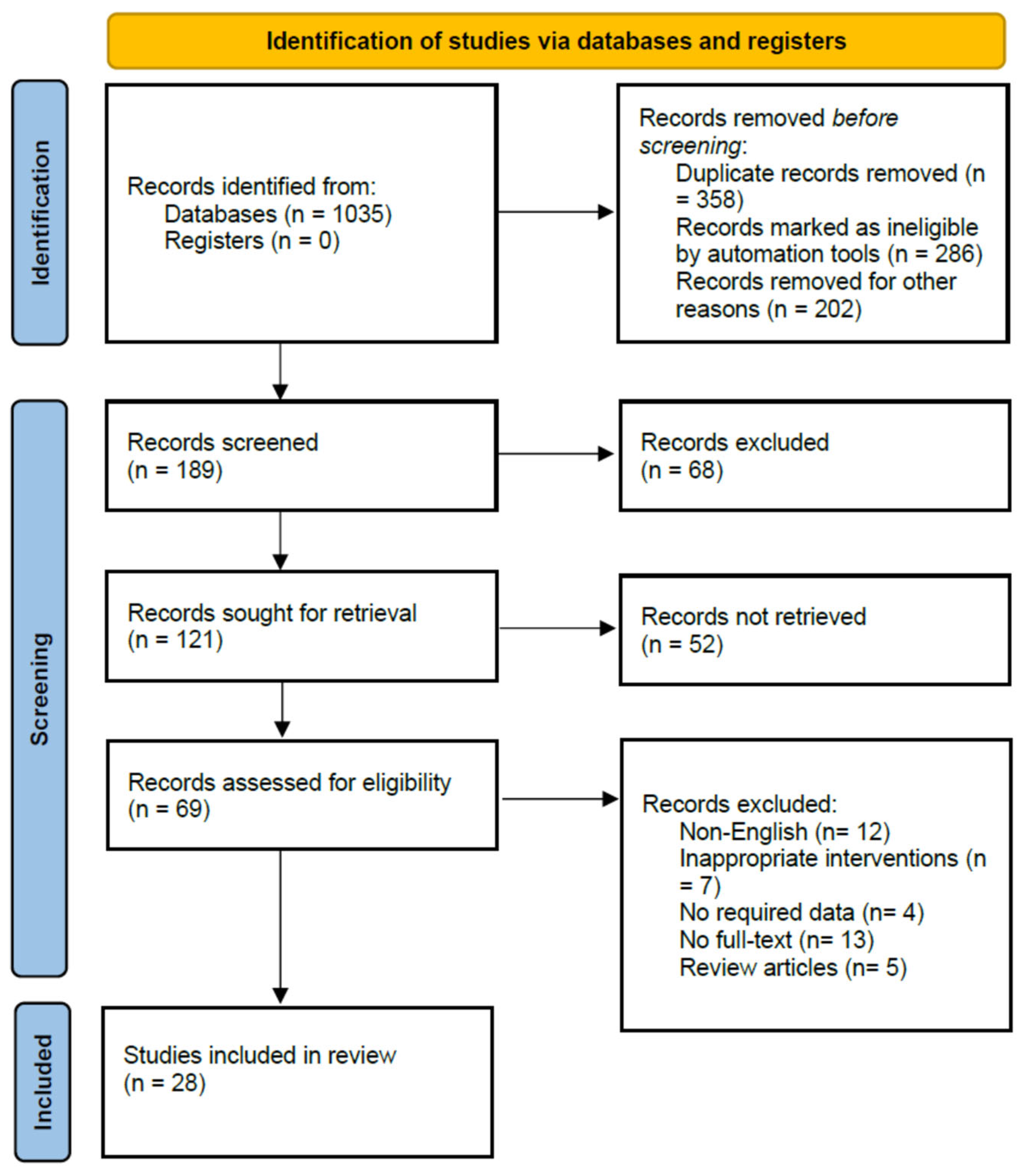
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Antimicrobial Susceptibility/Resistance Pattern
3.4. Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Troeger, C.E.; Blacker, B.F.; Khalil, I.A.; Zimsen, S.R.; Albertson, S.B.; Abate, D.; Abdela, J.; Adhikari, T.B.; Aghayan, S.A.; Agrawal, S. Mortality, morbidity, and hospitalisations due to influenza lower respiratory tract infections, 2017: An analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2019, 7, 69–89. [Google Scholar] [CrossRef] [Green Version]
- Lanks, C.W.; Musani, A.I.; Hsia, D.W. Community-acquired pneumonia and hospital-acquired pneumonia. Med. Clin. 2019, 103, 487–501. [Google Scholar] [CrossRef]
- Torres, A.; Peetermans, W.E.; Viegi, G.; Blasi, F. Risk factors for community-acquired pneumonia in adults in Europe: A literature review. Thorax 2013, 68, 1057–1065. [Google Scholar] [CrossRef] [Green Version]
- Almirall, J.; Serra-Prat, M.; Bolíbar, I.; Balasso, V. Risk factors for community-acquired pneumonia in adults: A systematic review of observational studies. Respiration 2017, 94, 299–311. [Google Scholar] [CrossRef]
- Ghia, C.J.; Dhar, R.; Koul, P.A.; Rambhad, G.; Fletcher, M.A. Streptococcus pneumoniae as a cause of community-acquired pneumonia in Indian adolescents and adults: A systematic review and meta-analysis. Clin. Med. Insights Circ. Respir. Pulm. Med. 2019, 13, 1179548419862790. [Google Scholar] [CrossRef] [Green Version]
- Peto, L.; Nadjm, B.; Horby, P.; Ngan, T.T.D.; van Doorn, R.; Kinh, N.V.; Wertheim, H.F. The bacterial aetiology of adult community-acquired pneumonia in Asia: A systematic review. Trans. R. Soc. Trop. Med. Hyg. 2014, 108, 326–337. [Google Scholar] [CrossRef] [Green Version]
- Welte, T.; Torres, A.; Nathwani, D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 2012, 67, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Aston, S.J.; Ho, A.; Jary, H.; Huwa, J.; Mitchell, T.; Ibitoye, S.; Greenwood, S.; Joekes, E.; Daire, A.; Mallewa, J. Etiology and risk factors for mortality in an adult community-acquired pneumonia cohort in Malawi. Am. J. Respir. Crit. Care Med. 2019, 200, 359–369. [Google Scholar] [CrossRef]
- Ojuawo, O.B.; Desalu, O.O.; Fawibe, A.E.; Ojuawo, A.B.; Aladesanmi, A.O.; Opeyemi, C.M.; Adio, M.O.; Jimoh, A.O.; Amadu, D.O.; Fadeyi, A. Clinical and microbiological profile of adult inpatients with community acquired pneumonia in Ilorin, North Central, Nigeria. Afr. Health Sci. 2020, 20, 1655–1668. [Google Scholar] [CrossRef]
- Temesgen, D.; Bereded, F.; Derbie, A.; Biadglegne, F. Bacteriology of community acquired pneumonia in adult patients at Felege Hiwot Referral Hospital, Northwest Ethiopia: A cross-sectional study. Antimicrob. Resist. Infect. Control 2019, 8, 101. [Google Scholar] [CrossRef] [Green Version]
- Regasa, B.; Yilma, D.; Sewunet, T.; Beyene, G. Antimicrobial susceptibility pattern of bacterial isolates from community-acquired pneumonia patients in Jimma University specialized hospital, Jimma, Ethiopia. Saudi J. Health Sci. 2015, 4, 59. [Google Scholar]
- Torres, A.; Ewig, S.; Lode, H.; Carlet, J.; Group, E.H.W. Defining, treating and preventing hospital acquired pneumonia: European perspective. Intensive Care Med. 2009, 35, 9–29. [Google Scholar] [CrossRef]
- Saleem, Z.; Godman, B.; Hassali, M.A.; Hashmi, F.K.; Azhar, F.; Rehman, I.U. Point prevalence surveys of health-care-associated infections: A systematic review. Pathog. Glob. Health 2019, 113, 191–205. [Google Scholar] [CrossRef]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur. Respir. J. 2017, 50, 1700582. [Google Scholar]
- Godman, B.; Egwuenu, A.; Haque, M.; Malande, O.O.; Schellack, N.; Kumar, S.; Saleem, Z.; Sneddon, J.; Hoxha, I.; Islam, S. Strategies to improve antimicrobial utilization with a special focus on developing countries. Life 2021, 11, 528. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A.; Godman, B.; Versporten, A.; Hashmi, F.K.; Saeed, H.; Saleem, F.; Salman, M.; Rehman, I.U.; Khan, T.M. Point prevalence surveys of antimicrobial use: A systematic review and the implications. Expert Rev. Anti-Infect. Ther. 2020, 18, 897–910. [Google Scholar] [CrossRef]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 47. [Google Scholar] [CrossRef]
- Saleem, Z.; Godman, B.; Cook, A.; Khan, M.A.; Campbell, S.M.; Seaton, R.A.; Siachalinga, L.; Haseeb, A.; Amir, A.; Kurdi, A. Ongoing efforts to improve antimicrobial utilization in hospitals among African countries and implications for the future. Antibiotics 2022, 11, 1824. [Google Scholar] [CrossRef]
- Saleem, Z.; Hassali, M.A. Travellers take heed: Outbreak of extensively drug resistant (XDR) typhoid fever in Pakistan and a warning from the US CDC. Travel. Med. Infect. Dis. 2019, 27, 127. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W. Update in adult community-acquired pneumonia: Key points from the new American Thoracic Society/Infectious Diseases Society of America 2019 guideline. Curr. Opin. Pulm. Med. 2020, 26, 203–207. [Google Scholar] [CrossRef]
- Haseeb, A.; Saleem, Z.; Altaf, U.; Batool, N.; Godman, B.; Ahsan, U.; Ashiq, M.; Razzaq, M.; Hanif, R.; E-Huma, Z. Impact of positive culture reports of E. coli or MSSA on de-escalation of antibiotic use in a teaching hospital in Pakistan and the implications. Infect. Drug Resist. 2022, 16, 77–86. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Batool, S.; Almaghaslah, D.; Alqahtani, A.; Almanasef, M.; Alasmari, M.; Vasudevan, R.; Attique, S.; Riaz, F. Aetiology and antimicrobial susceptibility pattern of bacterial isolates in community acquired pneumonia patients at Asir region, Saudi Arabia. Int. J. Clin. Pract. 2021, 75, e13667. [Google Scholar] [CrossRef]
- Balkhy, H.H.; El-Saed, A.; Maghraby, R.; Al-Dorzi, H.M.; Khan, R.; Rishu, A.H.; Arabi, Y.M. Drug-resistant ventilator associated pneumonia in a tertiary care hospital in Saudi Arabia. Ann. Thorac. Med. 2014, 9, 104. [Google Scholar] [CrossRef]
- Farahat, F.M.; Bukhari, O.K.; Basfar, I.A.; Alammari, A.M.; Zaatari, A.Z.; Alsaedi, A.A.; Alshamrani, M.M. Clinical characteristics and outcomes of community-acquired pneumonia in western Saudi Arabia: A four-year retrospective analysis of medical records. J. Infect. Public Health 2021, 14, 960–966. [Google Scholar] [CrossRef]
- Abdel-Rahman, E.M.; Ismael, N.A.; Dixon, R.A. Antibiotic resistance and prevalence of beta-lactamase in Haemophilus influenzae isolates-a surveillance study of patients with respiratory infection in Saudi Arabia. Diagn. Microbiol. Infect. Dis. 2000, 36, 203–208. [Google Scholar] [CrossRef]
- Memish, Z.A.; Balkhy, H.H.; Shibl, A.M.; Barrozo, C.P.; Gray, G.C. Streptococcus pneumoniae in Saudi Arabia: Antibiotic resistance and serotypes of recent clinical isolates. Int. J. Antimicrob. Agents 2004, 23, 32–38. [Google Scholar] [CrossRef]
- Alshahwan, S.I.; Alsowailmi, G.; Alsahli, A.; Alotaibi, A.; Alshaikh, M.; Almajed, M.; Omair, A.; Almodaimegh, H. The prevalence of complications of pneumonia among adults admitted to a tertiary care center in Riyadh from 2010–2017. Ann. Saudi Med. 2019, 39, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Akbar, D.H. Bacterial pneumonia: Comparison between diabetics and non-diabetics. Acta Diabetol. 2001, 38, 77–82. [Google Scholar] [CrossRef]
- Babay, H.A. Isolation of Moraxella catarrhalis in patients at King Khalid University Hospital, Riyadh. Saudi Med. J. 2000, 21, 860–863. [Google Scholar]
- AlBarrak, A.; Alotaibi, B.; Yassin, Y.; Mushi, A.; Maashi, F.; Seedahmed, Y.; Alshaer, M.; Altaweel, A.; Elshiekh, H.; Turkistani, A. Proportion of adult community-acquired pneumonia cases attributable to Streptococcus pneumoniae among Hajj pilgrims in 2016. Int. J. Infect. Dis. 2018, 69, 68–74. [Google Scholar] [CrossRef] [Green Version]
- Al-Obeid, S.; Jabri, L.; Al-Agamy, M.; Al-Omari, A.; Shibl, A. Epidemiology of extensive drug resistant Acinetobacter baumannii (XDRAB) at Security Forces Hospital (SFH) in Kingdom of Saudi Arabia (KSA). J. Chemother. 2015, 27, 156–162. [Google Scholar] [CrossRef]
- Almuneef, M.; Memish, Z.A.; Balkhy, H.H.; Alalem, H.; Abutaleb, A. Ventilator-associated pneumonia in a pediatric intensive care unit in Saudi Arabia: A 30-month prospective surveillance. Infect. Control Hosp. Epidemiol. 2004, 25, 753–758. [Google Scholar] [CrossRef]
- Saleem, M.; Syed Khaja, A.S.; Hossain, A.; Alenazi, F.; Said, K.B.; Moursi, S.A.; Almalaq, H.A.; Mohamed, H.; Rakha, E. Molecular Characterization and Antibiogram of Acinetobacter baumannii Clinical Isolates Recovered from the Patients with Ventilator-Associated Pneumonia. Healthcare 2022, 10, 2210. [Google Scholar] [CrossRef]
- El-Saed, A.; Balkhy, H.H.; Al-Dorzi, H.M.; Khan, R.; Rishu, A.H.; Arabi, Y.M. Acinetobacter is the most common pathogen associated with late-onset and recurrent ventilator-associated pneumonia in an adult intensive care unit in Saudi Arabia. Int. J. Infect. Dis. 2013, 17, e696–e701. [Google Scholar] [CrossRef] [Green Version]
- Osman, S.; Al Talhi, Y.M.; AlDabbagh, M.; Baksh, M.; Osman, M.; Azzam, M. The incidence of ventilator-associated pneumonia (VAP) in a tertiary-care center: Comparison between pre- and post-VAP prevention bundle. J. Infect. Public Health 2020, 13, 552–557. [Google Scholar] [CrossRef]
- Kabrah, A.M.; Kabrah, S.M.; Bahwerth, F.S.; Alredaini, N.F. Antibiotic Resistance Profile of Common Bacteria Isolated from Blood Stream, Lower Respiratory Tract and Urinary Infections in Intensive Care Unit in Saudi Arabia: A Retrospective Study. Ethiop. J. Health Sci. 2021, 31, 1231–1240. [Google Scholar]
- Ibrahim, M.E. High antimicrobial resistant rates among gram-negative pathogens in intensive care units: A retrospective study at a tertiary care hospital in Southwest Saudi Arabia. Saudi Med. J. 2018, 39, 1035. [Google Scholar] [CrossRef] [Green Version]
- Al-Dorzi, H.M.; El-Saed, A.; Rishu, A.H.; Balkhy, H.H.; Memish, Z.A.; Arabi, Y.M. The results of a 6-year epidemiologic surveillance for ventilator-associated pneumonia at a tertiary care intensive care unit in Saudi Arabia. Am. J. Infect. Control 2012, 40, 794–799. [Google Scholar] [CrossRef]
- Saleem, M.; Syed Khaja, A.S.; Hossain, A.; Alenazi, F.; Said, K.B.; Moursi, S.A.; Almalaq, H.A.; Mohamed, H.; Rakha, E.; Alharbi, M.S. Pathogen Burden Among ICU Patients in a Tertiary Care Hospital in Hail Saudi Arabia with Particular Reference to β-Lactamases Profile. Infect. Drug Resist. 2023, 16, 769–778. [Google Scholar] [CrossRef]
- Abdelrazik Othman, A.; Salah Abdelazim, M. Ventilator-associated pneumonia in adult intensive care unit prevalence and complications. Egypt. J. Crit. Care Med. 2017, 5, 61–63. [Google Scholar] [CrossRef]
- Balkhy, H.H.; Cunningham, G.; Chew, F.K.; Francis, C.; Al Nakhli, D.J.; Almuneef, M.A.; Memish, Z.A. Hospital- and community-acquired infections: A point prevalence and risk factors survey in a tertiary care center in Saudi Arabia. Int. J. Infect. Dis. 2006, 10, 326–333. [Google Scholar] [CrossRef] [Green Version]
- Al Johani, S.M.; Akhter, J.; Balkhy, H.; El-Saed, A.; Younan, M.; Memish, Z. Prevalence of antimicrobial resistance among gram-negative isolates in an adult intensive care unit at a tertiary care center in Saudi Arabia. Ann. Saudi Med. 2010, 30, 364–369. [Google Scholar] [CrossRef] [Green Version]
- Mwanri, L.; AlSaleh, E. Multi-drug resistant organisms and patients’ risk factors in the intensive care unit of King Fahad Hofuf Hospital, Saudi Arabia. Int. J. Health Psychol. Res. 2014, 2, 8–25. [Google Scholar]
- Al Bshabshe, A.; Joseph, M.R.P.; Al Hussein, A.; Haimour, W.; Hamid, M.E. Multidrug resistance Acinetobacter species at the intensive care unit, Aseer Central Hospital, Saudi Arabia: A one year analysis. Asian Pac. J. Trop. Med. 2016, 9, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Zaki, A.; Abdelwahab, S.; Awad, M.H. Bacterial pathogens in sputum of children with community-acquired pneumonia, unexpected results: A single hospital-based study. Alex. J. Pediatr. 2021, 34, 183. [Google Scholar] [CrossRef]
- Hakami, A.Y.; Felemban, L.H.; Aljifri, N.A.; Alyamani, G.M.; Abosallamh, K.A.; Aljohani, R.A.; Aldosary, T.; Basheikh, A. Antibacterial Resistance Patterns Among Common Infections in a Tertiary Care Hospital in Saudi Arabia. Cureus 2022, 14, e31695. [Google Scholar] [CrossRef]
- Walid, J.; Moshref, L.; Alzanbagi, M.; Moshref, R.; Baabdullah, W.; Aldigs, E.; AlAhmadi, T.; Kari, J.; Alharbi, S.; Safdar, O. Antibiotic resistance pattern in healthy children diagnosed with community acquired respiratory tract infections in King Abdulaziz University Hospital. J. Med. Microb. Diagn. 2016, 5, 232. [Google Scholar] [CrossRef] [Green Version]
- Al Munjem, M.F.; Thabit, A.K.; Rasool, S.T.; Emeka, P.M.; Al Munajjim, F.F.; Al Habeeb, M. Prescription patterns and antibiotic resistance rates of respiratory tract infections in a Saudi tertiary medical centre. Saudi J. Clin. Pharm. 2022, 1, 128. [Google Scholar] [CrossRef]
- Marie, M.A.M. Incidence and antimicrobial susceptibility of Mycoplasma pneumoniae in Saudi Arabia. J. Bacteriol. Virol. 2010, 40, 159–162. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.E. Prevalence of Acinetobacter baumannii in Saudi Arabia: Risk factors, antimicrobial resistance patterns and mechanisms of carbapenem resistance. Ann. Clin. Microbiol. Antimicrob. 2019, 18, 1. [Google Scholar] [CrossRef]
- Zar, H.J.; Ferkol, T.W. The Global Burden of Respiratory Disease—Impact on Child Health; Wiley Online Library: Hoboken, NJ, USA, 2014; Volume 49, pp. 430–434. [Google Scholar]
- Tegenu, K.; Geleto, G.; Tilahun, D.; Bayana, E.; Bereke, B. Severe pneumonia: Treatment outcome and its determinant factors among under-five patients, Jimma, Ethiopia. SAGE Open Med. 2022, 10, 20503121221078445. [Google Scholar] [CrossRef]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Lee, J.W.; Falsey, A.R.; Demont, C.; Nyawanda, B.O.; Cai, B.; Fuentes, R.; Stoszek, S.K.; et al. Global and regional burden of hospital admissions for pneumonia in older adults: A systematic review and meta-analysis. J. Inf. Dis. 2020, 222, S570–S576. [Google Scholar] [CrossRef] [Green Version]
- Nguyen-Van-Tam, J.S.; O’Leary, M.; Martin, E.T.; Heijnen, E.; Callendret, B.; Fleischhackl, R.; Comeaux, C.; Tran, T.M.P.; Weber, K. Burden of respiratory syncytial virus infection in older and high-risk adults: A systematic review and meta-analysis of the evidence from developed countries. Eur. Respir. Rev. 2022, 31, 220105. [Google Scholar] [CrossRef]
- Fagerli, K.; Ulziibayar, M.; Suuri, B.; Luvsantseren, D.; Narangerel, D.; Batsaikhan, P.; Tsolmon, B.; Gessner, B.D.; Dunne, E.M.; Grobler, A.C. Epidemiology of pneumonia in hospitalized adults ≥ 18 years old in four districts of Ulaanbaatar, Mongolia, 2015–2019. Lancet Reg. Health West. Pac. 2023, 30, 100591. [Google Scholar] [CrossRef]
- Seramo, R.K.; Awol, S.M.; Wabe, Y.A.; Ali, M.M. Determinants of pneumonia among children attending public health facilities in Worabe town. Sci. Rep. 2022, 12, 6175. [Google Scholar] [CrossRef]
- Antalová, N.; Klučka, J.; Říhová, M.; Poláčková, S.; Pokorná, A.; Štourač, P. Ventilator-Associated Pneumonia Prevention in Pediatric Patients: Narrative Review. Children 2022, 9, 1540. [Google Scholar] [CrossRef]
- Safdar, N.; Crnich, C.J.; Maki, D.G. The pathogenesis of ventilator-associated pneumonia: Its relevance to developing effective strategies for prevention. Respir. Care 2005, 50, 725–741. [Google Scholar]
- Barzilay, Z.; Mandel, M.; Keren, G.; Davidson, S. Nosocomial bacterial pneumonia in ventilated children: Clinical significance of culture-positive peripheral bronchial aspirates. J. Pediatr. 1988, 112, 421–424. [Google Scholar] [CrossRef]
- Elward, A.M.; Warren, D.K.; Fraser, V.J. Ventilator-associated pneumonia in pediatric intensive care unit patients: Risk factors and outcomes. Pediatrics 2002, 109, 758–764. [Google Scholar] [CrossRef]
- Chawla, R. Epidemiology, etiology, and diagnosis of hospital-acquired pneumonia and ventilator-associated pneumonia in Asian countries. Am. J. Infect. Control 2008, 36, S93–S100. [Google Scholar] [CrossRef]
- Manikam, L.; Lakhanpaul, M. Epidemiology of community acquired pneumonia. Paediatr. Child Health 2012, 22, 299–306. [Google Scholar] [CrossRef]
- Song, J.-H.; Oh, W.S.; Kang, C.-I.; Chung, D.R.; Peck, K.R.; Ko, K.S.; Yeom, J.S.; Kim, C.K.; Kim, S.W.; Chang, H.-H. Epidemiology and clinical outcomes of community-acquired pneumonia in adult patients in Asian countries: A prospective study by the Asian network for surveillance of resistant pathogens. Int. J. Antimicrob. Agents 2008, 31, 107–114. [Google Scholar] [CrossRef]
- Alamoudi, O.S. Prevalence of respiratory diseases in hospitalized patients in Saudi Arabia: A 5 years study 1996–2000. Ann. Thorac. Med. 2006, 1, 76. [Google Scholar] [CrossRef]
- Mohan, S.; Almutairi, M.; Alnaimi, R.; Alshehri, T.; Philip, W.; Ismaiel, Y.; Ismaeil, T. Incidence and Outcomes of Community Acquired Pneumonia in Patients with Chronic Obstructive Pulmonary Disease at King Abdulaziz Medical City, Riyadh. Methodology 2018, 29, 1–7. [Google Scholar] [CrossRef]
- Memish, Z.A.; Shibl, A.M.; Ahmed, Q.A.A.; Saudi Arabian Community-Acquired Pneumonia Working Group. Guidelines for the management of community-acquired pneumonia in Saudi Arabia: A model for the Middle East region. Int. J. Antimicrob. Agents 2002, 20, 1–12. [Google Scholar] [CrossRef]
- Matute, A.J.; Brouwer, W.P.; Hak, E.; Delgado, E.; Alonso, E.; Hoepelman, I.M. Aetiology and resistance patterns of community-acquired pneumonia in Leon, Nicaragua. Int. J. Antimicrob. Agents 2006, 28, 423–427. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Momattin, H.; Hinedi, K. Empiric Antibiotic Therapy in the Treatment of Community-acquired Pneumonia in a General Hospital in Saudi Arabia. J. Glob. Infect. Dis. 2019, 11, 69–72. [Google Scholar] [CrossRef]
- Mahboub, B.; Al Zaabi, A.; Al Ali, O.M.; Ahmed, R.; Niederman, M.S.; El-Bishbishi, R. Real life management of community-acquired Pneumonia in adults in the Gulf region and comparison with practice guidelines: A prospective study. BMC Pulm. Med. 2015, 15, 112. [Google Scholar] [CrossRef] [Green Version]
- Rothberg, M.B. Community-acquired pneumonia. Ann. Intern. Med. 2022, 175, ITC49–ITC64. [Google Scholar] [CrossRef]


{kind=link}
| Author and Year | Study Setting | Study Period | Sample Size | Population Type | Study Design | Prevalence of Infection | Top 3 Isolated Pathogens | ||
|---|---|---|---|---|---|---|---|---|---|
| Batool et al., 2021 [23] | 1 hospital | May 2019–October 2019 | 165 | Adults | Cross-sectional study | CAP (46.6%) | S. pneumoniae (34%) | H. influenzae (16%) | S. aureus (30%) |
| Balkhy et al., 2014 [24] | ICU | October 2004–June 2009 | 248 | Adults | Retrospective study | VAP (100%) | Acinetobacter spp. (35.1%) | P. aeruginosa (25.4%) | S. aureus (17.3%) |
| Farahat et al., 2021 [25] | 1 hospital | 2016 -2019 | 218 | Adults | Retrospective study | CAP (100%) | S. aureus (2.5%) | MRSA (2.3%) | Klebsiella spp. (1.3%) |
| Rahman et al., 2000 [26] | 5 medical centers | January–July | 129 | - | Retrospective study | LRTIs (100%) | H. influenzae (100%) | - | - |
| Memish et al., 2004 [27] | 3 hospitals | January 2000–December 2000 | 154 | Mixed | Cross-sectional study | CAP (100%) | S. pneumoniae (100%) | - | - |
| Alshahwan et al., 2019 [28] | Pulmonary department | 2010–2017 | 800 | Adults | Retrospective study | CAP (80%) | - | - | - |
| HAP (20%) | |||||||||
| Akbar et al., 2001 [29] | 1 hospital | January 1998–December 1999 | 354 | Adults | Prospective study | CAP (24%) | H. influenzae (51.7%) | S. aureus (14.1%) | M. catarrhalis (11.7%) |
| HAP (76%) | Pseudomonas spp. (27.1%) | S. aureus (15.2%) | H. influenzae (14.4%) | ||||||
| Babay et al., 2000 [30] | 1 hospital | July 1998–December 1999 | 32 | Mixed | Retrospective study | Pneumonia (21.8%) | M. catarrhalis (100%) | - | - |
| Albarak et al., 2018 [31] | 13 hospitals | August 2016–September 2016 | 266 | Adults | Prospective case series | CAP (100%) | S. pneumoniae (18%) | - | - |
| Obeid et al., 2015 [32] | 1 hospital | 2006, 2009 and 2012 | 1952 | - | Retrospective study | VAP (100%) | A. Baumannii (100%) | - | - |
| Almuneef et al., 2004 [33] | ICU | May 2000–December 2002 | 361 | Children | Prospective study | VAP (10.2%) | P. aeruginosa (56.8%) | S. aureus (18.9%) | K. pneumoniae (10.8%) |
| Saleem et al., 2022 [34] | ICU | 2019–2022 | 591 | Adults | Prospective study | VAP (27.5%) | A. baumannii (21.4%) | - | - |
| El-Saed et al., 2013 [35] | ICU | August 2003–June 2009 | 457 | Adults | Prospective study | VAP (100%) | Acinetobacter spp. (26.5%) | P. aeruginosa (21.7%) | S. aureus (15.3%) |
| Osman et al., 2020 [36] | PICU | January 2015–March 2018 | 141 | Children | Prospective study | VAP (100%) | P. aeruginosa (34.0%) | K. pneumoniae (18.1%) | S. maltophilia (13.6%) |
| Kabrah et al., 2021 [37] | ICU | November 2020–January 2021 | 96 | Adults | Retrospective study | LRTIs (53.1%) | P. aeruginosa (66.7%) | A. baumannii (13.7%) | K. oxytica (4.0%) |
| Ibrahim et al., 2018 [38] | ICU | December 2016–January 2018 | 3736 | Adults | Retrospective study | 9.6% | Acinetobacter spp. (34.6%) | P. aeruginosa (24.5%) | K. pneumoniae (14.9%) |
| Al-Dorzi et al., 2012 [39] | ICU | August 2003–June 2009 | 2812 | Adults | Prospective study | VAP (15.4%) | - | - | - |
| Saleem et al., 2023 [40] | ICU | January 2019–December 2019 | 591 | - | Prospective study | VAP (43%) | K. pneumoniae (24%) | A. baumannii (21.5%) | P. aeruginosa (15.3%) |
| Othman et al., 2017 [41] | ICU | September 2012–August 2013 | 48 | Adults | Prospective study | VAP (35.4%) | P. aeruginosa (41.1%) | S. aureus (17.6%) | K. pneumoniae (11.7%) |
| Balkhy et al., 2006 [42] | 1 hospital | May 2003 | 562 | Adults | PPS | CAP (34.9%) | P. aeruginosa (21.3%) | Klebsiella spp. (10.1%) | Pseudomonas spp. (7.9%) |
| Al-Johani et al., 2010 [43] | ICU | January 2004–June 2009 | 4192 | Adults | Retrospective study | VAP (43%) | Acinetobacter spp. (31.7%) | P. aeruginosa (30.6%) | E. coli (14.0%) |
| Mwanri et al., 2014 [44] | ICU | 2010–2012 | 496 | Mixed | Retrospective study | VAP (14.8%) | Acinetobacter spp. (57.4%) | Klebsiella ESBL (13.2%) | MRSA (9.8%) |
| Bshabshe et al., 2016 [45] | ICU | 2014–2015 | 105 | Adults | Observational study | 100% | A. baumannii (46.6%) | A. haemolyticus (30.4%) | A. complex (18.0%) |
| Zaki et al., 2021 [46] | 1 hospital | January 2017–December 2019 | 163 | Children | Retrospective study | CAP (26.4%) | S. aureus (37.2%) | K. pneumoniae (30.2%) | Streptococcus spp. (14%) |
| Hakami et al., 2022 [47] | 1 hospital | May 2016–December 2019 | 1151 | Mixed | Cross-sectional study | 49.3% | P. aeruginosa (28.5%) | K. pneumoniae (17.6%) | A. baumannii (15.1%) |
| Walid et al., 2016 [48] | 1 hospital | January 2019–Jan 2015 | 122 | Children | Retrospective study | Pneumonia (26.2%) | P. aeruginosa (11.5%) | S. pneumoniae (7.6%) | S. aureus (7.6%) |
| Al-Munjem et al., 2022 [49] | 1 medical center | January 2016–December 2017 | 405 | Mixed | Retrospective study | Pneumonia (47.4%) | S. pneumoniae (90.9%) | P. aeruginosa (84.1%) | K. pneumoniae (84.1%) |
| Marie et al., 2010 [50] | 1 hospital | - | 552 | Mixed | Retrospective study | Pneumonia (49.4%) | M. pneumoniae (42.2%) | - | - |
| Author and Year | Isolated Organism | Top 3 Most Sensitive Antibitoics | Top 3 Most Resistant Antibiotic | ||||
|---|---|---|---|---|---|---|---|
| Batool et al., 2021 [23] | S. pneumoniae | Amoxicillin/Sulbactam (96%) | Ceftriaxone (92%) | Amikacin (92%) | Co-trimoxazole (43%) | Ampicillin (39%) | Ciprofloxacin (39%) |
| H. influenzae | Levofloxacin (91%) | Ciprofloxacin (83%) | Amikacin (83%) | Doxycycline (59%) | Clarithromycin (59%) | Azithromycin (59%) | |
| S. aureus | Amikacin (90%) | Ceftriaxone (80%) | Ampicillin (80%) | Co-trimoxazole (60%) | Clarithromycin (40%) | Doxycycline (40%) | |
| Balkhy et al., 2014 [24] | Acinetobacter spp. | Meropenem (25%) | Piperacillin/Tazobactam (17%) | Amikacin (11%) | Imipenem (95%) | Ciprofloxacin (98%) | Gentamicin (97%) |
| P. aeruginosa | Amikacin (68%) | Meropenem (43%) | Piperacillin/Tazobactam (8%) | Gentamicin (100%) | Cefepime (98%) | Ciprofloxacin (97%) | |
| S. aureus | Gentamicin (56%) | Ciprofloxacin (35%) | Penicillin (37%) | Oxacillin (100%) | Vancomycin (100%) | Erythromycin (88%) | |
| Farahat et al., 2021 [25] | - | - | - | - | - | - | - |
| Rahman et al., 2000 [26] | H. influenzae | Ciprofloxacin (100%) | Ceftazidime (100%) | Amoxiclav (98%) | Ampicillin (13.2%) | Tetracycline (7%) | Chloramphenicol (5%) |
| Memish et al., 2004 [27] | S. pneumoniae | Vancomycin (100%) | Levofloxacin (98%) | Ceftriaxone (85%) | Erythromycin (15%) | Penicillin (14%) | Sulfamethoxazole/trimethoprim (9%) |
| Alshahwan et al., 2019 [28] | - | - | - | - | - | - | - |
| Akbar et al., 2001 For CAP [29] | H. influenzae | Cefuroxime (97%) | Ciprofloxacin (84%) | Ceftriaxone (87%) | Vancomycin (97%) | Gentamicin (97%) | Imipenem (94%) |
| S. pneumoniae | Co-amoxiclav (100%) | Cefuroxime (100%) | Erythromycin (100%) | Penicillin (67%) | Gentamicin (67%) | Aztreonam (67%) | |
| M. Catarrhalis | Co-amoxiclav (100%) | Cefuroxime (100%) | Erythromycin (100%) | Penicillin (87%) | Ceftriaxone (87%) | Erythromycin (14%) | |
| Akbar et al., 2001 For HAP [29] | Pseudomonas spp. | Amikacin (85%) | Gentamicin (84%) | Piperacillin (70%) | Erythromycin (98%) | Co-amoxiclav (93%) | Ampicillin (93%) |
| S. aureus | Vancomycin (86%) | Oxacillin (81%) | Erythromycin (67%) | Ampicillin (86%) | Co-amoxiclav (86%) | Ciprofloxacin (86%) | |
| Enterobacter spp. | Imipenem (100%) | Amikacin (100%) | Ciprofloxacin (79%) | Ampicillin (93%) | Co-amoxiclav (93%) | Cefuroxime (86%) | |
| Babay et al., 2000 [30] | M. catarrhalis | Ciprofloxacin (-) | Gentamicin (-) | Tetracycline (-) | - | - | - |
| Albarrak et al., 2018 [31] | - | - | - | - | - | - | - |
| Obeid et al., 2015 [32] | A. baumannii | Colistin (-) | Gentamicin (-) | Tigecycline (-) | Amikacin (-) | Ceftazidime (-) | Ciprofloxacin (-) |
| Almuneef et al., 2004 [33] | - | - | - | - | - | - | - |
| Saleem et al., 2022 [34] | A. baumannii | Colistin (100%) | Amikacin (48%) | Gentamicin (17%) | Co-amoxiclav (-) | Ciprofloxacin (-) | Ampicillin (-) |
| Al-Saed et al., 2013 [35] | - | - | - | - | - | - | - |
| Osman et al., 2020 [36] | - | - | - | - | - | - | - |
| Kabrah et al., 2018 [37] | Overall | Teicoplanin (100%) | Vancomycin (100%) | Synercid (100%) | Penicillin (100%) | Aztreonam (96%) | Cefotaxime (88%) |
| Ibrahim et al., 2018 [38] | Acinetobacter spp. | Colistin (96%) | Sulfamethoxazole/Trimethoprim (7%) | Gentamicin (4%) | Aztreonam (97%) | Cefepime (97%) | Ceftazidime (97%) |
| P. aeruginosa | Amikacin (82%) | Tobramycin (80%) | Gentamicin (69%) | Cefuroxime (66%) | Cefotaxime (63%) | Cefepime (53%) | |
| K. pneumoniae | Colistin (100%) | Imipenem (59%) | Amikacin (54%) | Cefuroxime (71%) | Sulfamethoxazole/Trimethoprim (71%) | Ceftazidime (67%) | |
| Al-Dorzi et al., 2012 [39] | - | - | - | - | - | - | - |
| Saleem et al., 2023 [40] | K. pneumoniae | Colistin (59%) | Piperacillin/Tazobactam (52%) | Gentamicin (52%) | Ampicillin (92%) | Levofloxacin (92%) | Amoxiclav (89%) |
| A. baumannii | Tigecycline (40%) | Piperacillin/Tazobactam (26%) | Gentamicin (20%) | Amoxiclav (100%) | Ciprofloxacin (100%) | Meropenem (100%) | |
| P. aeruginosa | Tigecycline (96%) | Colistin (72%) | Amikacin (72%) | Amoxiclav (84%) | Cefuroxime (84%) | Cephalothin (84%) | |
| Othman et al., 2017 [41] | - | - | - | - | - | - | - |
| Balkhy et al., 2006 [42] | - | - | - | - | - | - | - |
| Al-Johani et al., 2010 [43] | Acinetobacter spp. | Imipenem (10%) | Meropenem (10%) | Ciprofloxacin (10%) | Cefepime (-) | Ciprofloxacin (-) | Ceftazidime (-) |
| P. aeruginosa | Ciprofloxacin (49%) | Ceftazidime (44%) | Carbapenems (26%) | Meropenem (-) | Meropenem (-) | Cefepime (-) | |
| E.coli | Cefepime (50%) | Ceftazidime (46%) | Cefotaxime (46%) | Ampicillin (-) | Sulfamethoxazole/Trimethoprim (-) | Ciprofloxacin (-) | |
| Mwanri et al., 2014 [44] | - | - | - | - | - | - | - |
| Bshabshe et al., 2016 [45] | A. baumannii | Colistin (100%) | Sulfamethoxazole/Trimethoprim (74%) | Amikacin (16%) | Moxifloxacin (100%) | Meropenem (100%) | Fosfomycin (100%) |
| A. haemolyticus | Colistin (100%) | Sulfamethoxazole/Trimethoprim (68%) | Amikacin (18%) | Ampicillin (100%) | Moxifloxacin (100%) | Fosfomycin (100%) | |
| A. complex | Colistin (100%) | Rifampicin (100%) | Sulfamethoxazole/Trimethoprim (78%) | Amikacin (100%) | Ciprofloxacin (100%) | Imipenem (100%) | |
| Zaki et al., 2021 [46] | - | - | - | - | - | - | - |
| Hakami et al., 2022 [47] | P. aeruginosa | Cefepime (99%) | Tigecycline (99%) | Imipenem (98%) | Piperacillin/Tazobactam (51%) | Ciprofloxacin (25%) | Ampicillin (10%) |
| K. pneumoniae | Amoxicillin (99%) | - | - | Ampicillin (82%) | Ceftriaxone (9%) | Piperacillin/Tazobactam (7%) | |
| A. baumannii | Meropenem (99%) | Ceftriaxone (99%) | Amoxiclav (98%) | Piperacillin/Tazobactam (52%) | Ampicillin (38%) | Ciprofloxacin (5%) | |
| Walid et al., 2016 [48] | Overall | - | - | - | Ceftriaxone (24%) | Cefuroxime (21%) | Cefotaxime (3%) |
| Al Munjem et al., 2022 [49] | S. pneumoniae | Levofloxacin (67%) | Oxacillin (52%) | Ciprofloxacin (32%) | Azithromycin (100%) | Amoxicillin (98%) | Co-amoxiclav (98%) |
| P. aeruginosa | Levofloxacin (70%) | Ciprofloxacin (29%) | - | - | - | - | |
| K. pneumoniae | Levofloxacin (67%) | Ciprofloxacin (35%) | Amoxicillin (2%) | Co-amoxiclav (100%) | Amoxicillin (98%) | Azithromycin (98%) | |
| Marie et al., 2010 [50] | - | - | - | - | - | - | - |
| Selection | Comparability | Outcomes | ||||||
|---|---|---|---|---|---|---|---|---|
| Reference | Representative of Sample A | Sample Size B | Non-Respondents C | Ascertainment of Exposure D | Comparability of Cohort Studies on Basis of Design E | Assessment of Outcomes F | Statistical Analysis G | Quality Score |
| Batool et al., 2021 [23] | * | * | - | ** | * | ** | - | 7 |
| Balkhy et al., 2014 [24] | * | * | - | ** | * | ** | * | 8 |
| Farahat et al., 2021 [25] | * | * | - | * | * | ** | * | 7 |
| Rahman et al., 2000 [26] | * | * | - | ** | * | ** | * | 8 |
| Memish et al., 2004 [27] | * | * | - | ** | * | ** | * | 8 |
| Alshahwan et al., 2019 [28] | * | * | - | * | * | ** | * | 7 |
| Akbar et al., 2001 For CAP [29] | * | * | - | ** | * | ** | * | 8 |
| Babay et al., 2000 [30] | * | * | - | ** | * | ** | - | 7 |
| Albarrak et al., 2018 [31] | * | * | - | * | * | ** | * | 7 |
| Obeid et al., 2015 [32] | * | * | - | ** | * | ** | - | 7 |
| Almuneef et al., 2004 [33] | * | * | - | * | * | ** | * | 7 |
| Saleem et al., 2022 [34] | * | * | - | ** | * | ** | * | 8 |
| Al-Saed et al., 2013 [35] | * | * | - | * | * | ** | * | 7 |
| Osman et al., 2020 [36] | * | * | - | * | * | ** | * | 7 |
| Kabrah et al., 2018 [37] | * | * | - | ** | * | ** | * | 8 |
| Ibrahim et al., 2018 [38] | * | * | - | ** | * | ** | * | 8 |
| Al-Dorzi et al., 2012 [39] | * | * | - | * | * | ** | * | 7 |
| Saleem et al., 2023 [40] | * | * | - | ** | * | ** | * | 8 |
| Othman et al., 2017 [41] | * | * | - | * | * | ** | * | 7 |
| Balkhy et al., 2006 [42] | * | * | - | * | * | ** | * | 7 |
| Al-Johani et al., 2010 [43] | * | * | - | ** | * | ** | * | 8 |
| Mwanri et al., 2014 [44] | * | * | - | * | * | ** | * | 7 |
| Bshabshe et al., 2016 [45] | * | * | - | ** | * | ** | * | 8 |
| Zaki at al., 2021 [46] | * | * | - | * | * | ** | * | 7 |
| Hakami et al., 2022 [47] | * | * | - | ** | * | ** | * | 8 |
| Walid et al., 2016 [48] | * | * | - | ** | * | ** | * | 8 |
| Al Munjem et al., 2022 [49] | * | * | - | ** | * | ** | * | 8 |
| Marie et al., 2010 [50] | * | * | - | * | * | ** | - | 6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshammari, M.K.; Alotaibi, M.A.; AlOtaibi, A.S.; Alosaime, H.T.; Aljuaid, M.A.; Alshehri, B.M.; AlOtaibi, Y.B.; Alasmari, A.A.; Alasmari, G.A.; Mohammed, M.H.; et al. Prevalence and Etiology of Community- and Hospital-Acquired Pneumonia in Saudi Arabia and Their Antimicrobial Susceptibility Patterns: A Systematic Review. Medicina 2023, 59, 760. https://doi.org/10.3390/medicina59040760
Alshammari MK, Alotaibi MA, AlOtaibi AS, Alosaime HT, Aljuaid MA, Alshehri BM, AlOtaibi YB, Alasmari AA, Alasmari GA, Mohammed MH, et al. Prevalence and Etiology of Community- and Hospital-Acquired Pneumonia in Saudi Arabia and Their Antimicrobial Susceptibility Patterns: A Systematic Review. Medicina. 2023; 59(4):760. https://doi.org/10.3390/medicina59040760
Chicago/Turabian StyleAlshammari, Mohammed Kanan, Mzoun Abdulaziz Alotaibi, Ahad Sanad AlOtaibi, Hanan Tareq Alosaime, Mona Awadh Aljuaid, Budur Mohammed Alshehri, Yasmen Bejad AlOtaibi, Asma Ali Alasmari, Ghadi Ali Alasmari, Maram Hussain Mohammed, and et al. 2023. "Prevalence and Etiology of Community- and Hospital-Acquired Pneumonia in Saudi Arabia and Their Antimicrobial Susceptibility Patterns: A Systematic Review" Medicina 59, no. 4: 760. https://doi.org/10.3390/medicina59040760