
Predictors of Outcome in Patients with Pulmonary Hypertension Undergoing Mitral and Tricuspid Valve Surgery

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Study Population
2.2. Clinical Data
2.3. Echocardiographic (ECHO) Assessment
2.3.1. Qualitative Assessment
2.3.2. Quantitative Parameters
2.4. Statistical Analysis
3. Results
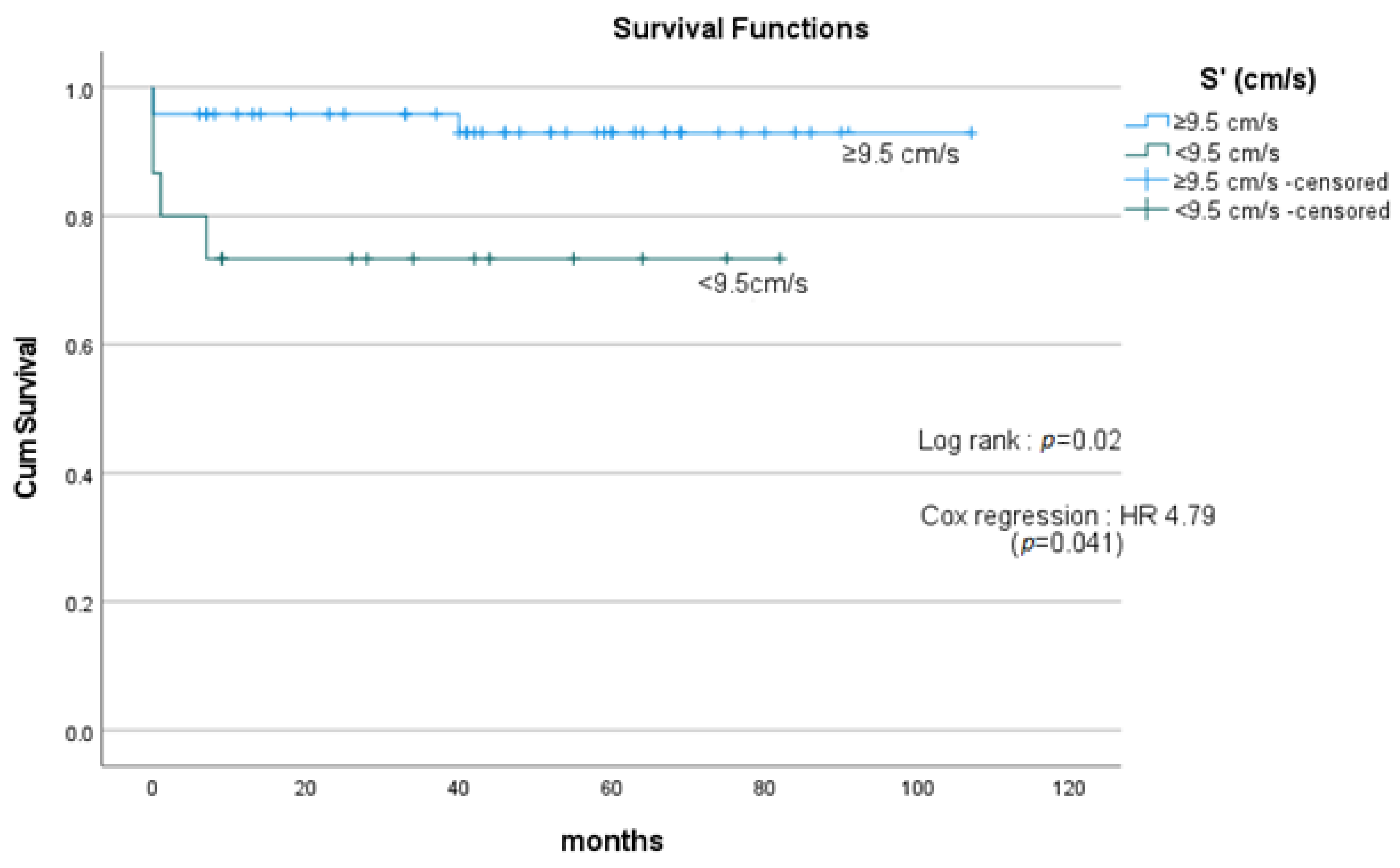
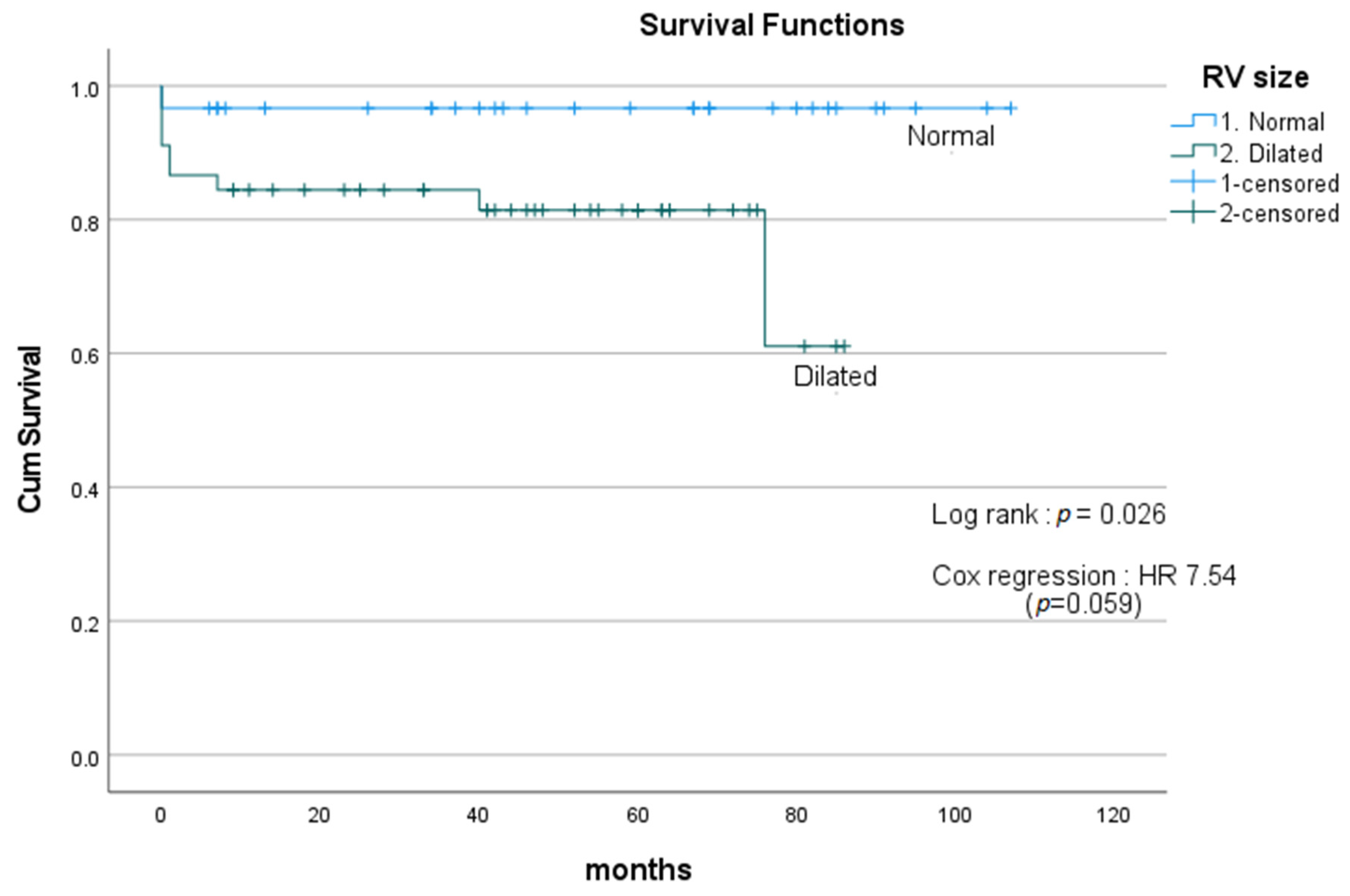
3.1. Primary Outcome and Survival Analysis (Kaplan–Meier)
3.2. Secondary Outcomes
3.3. Prognostic Factors of Survival—Univariate Analysis
3.4. Renal Failure Requiring Dialysis—Univariate Analysis
3.5. Respiratory Failure Requiring Intubation—Univariate Analysis
3.6. Excluding Redo MV Surgery
3.7. Subgroup Analysis of Only Elective Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Magne, J.; Pibarot, P.; Sengupta, P.P.; Donal, E.; Rosenhek, R.; Lancellotti, P. Pulmonary hypertension in valvular disease: A comprehensive review on pathophysiology to therapy from the HAVEC Group. JACC Cardiovasc. Imaging 2015, 8, 83–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, C.; Tsugu, T.; Sugimoto, T.; Lancellotti, P. Pulmonary Hypertension with Valvular Heart Disease: When to Treat the Valve Disease and When to Treat the Pulmonary Hypertension. Curr. Cardiol. Rep. 2019, 21, 151. [Google Scholar] [CrossRef] [PubMed]
- Hoendermis, E.S.; Liu, L.C.; Hummel, Y.M.; van der Meer, P.; de Boer, R.A.; Berger, R.M.; van Veldhuisen, D.J.; Voors, A.A. Effects of sildenafil on invasive haemodynamics and exercise capacity in heart failure patients with preserved ejection fraction and pulmonary hypertension: A randomized controlled trial. Eur. Heart J. 2015, 36, 2565–2573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonderman, D.; Ghio, S.; Felix, S.B.; Ghofrani, H.A.; Michelakis, E.; Mitrovic, V.; Semigran, M.J. Riociguat for patients with pulmonary hypertension caused by systolic left ventricular dysfunction: A phase IIb double-blind, randomized, placebo-controlled, dose-ranging hemodynamic study. Circulation 2013, 128, 502–511. [Google Scholar] [CrossRef] [Green Version]
- Bermejo, J.; Yotti, R.; García-Orta, R.; Sánchez-Fernández, P.L.; Castaño, M.; Segovia-Cubero, J.; Román, J.A.S.; Borrás, X.; Alonso-Gómez, A.; Botas, J.; et al. Sildenafil for improving outcomes in patients with corrected valvular heart disease and persistent pulmonary hypertension: A multicenter, double-blind, randomized clinical trial. Eur. Heart J. 2018, 39, 1255–1264. [Google Scholar] [CrossRef] [Green Version]
- Eskandr, A.M.; Metwally, A.A.; Abu Elkassem, M.S.; Sadik, S.A.; Elmiligy, A.E.; Mourad, M.; Hussein, L. Dobutamine and Nitroglycerin Versus Milrinone for Perioperative Management of Pulmonary Hypertension in Mitral Valve Surgery. A Randomized Controlled Study. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2540–2546. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Voigt, J.U. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar] [CrossRef]
- Howard, L.S.; Grapsa, J.; Dawson, D.; Bellamy, M.; Chambers, J.B.; Masani, N.D.; Nihoyannopoulos, P.; Gibbs, J.S.R. Echocardiographic assessment of pulmonary hypertension: Standard operating procedure. Eur. Respir. Rev. 2012, 21, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Otto, C.M.; Nishimura, R.A.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P., III; Gentile, F.; Jneid, H.; Krieger, E.V.; Mack, M.; McLeod, C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. College Cardiol. 2021, 77, 450–500. [Google Scholar] [CrossRef]
- Baumgartner, H.; Falk, V.; Bax, J.J.; De Bonis, M.; Hamm, C.; Holm, P.J.; Zamorano, J.L. ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. J. Cardiothorac. Surg. 2017, 52, 616–664. [Google Scholar]
- Otterstad, J.E. Measuring left ventricular volume and ejection fraction with the biplane Simpson’s method. Heart 2002, 88, 559–560. [Google Scholar] [CrossRef]
- Le Tourneau, T.; Richardson, M.; Juthier, F.; Modine, T.; Fayad, G.; Polge, A.-S.; Ennezat, P.-V.; Bauters, C.; Vincentelli, A.; Deklunder, G. Echocardiography predictors and prognostic value of pulmonary artery systolic pressure in chronic organic mitral regurgitation. Heart 2010, 96, 1311–1317. [Google Scholar] [CrossRef]
- Barbieri, A.; Bursi, F.; Grigioni, F.; Tribouilloy, C.; Avierinos, J.F.; Michelena, H.I.; Bacchi-Reggiani, M.L. Prognostic and therapeutic implications of pulmonary hypertension complicating degenerative mitral regurgitation due to flail leaflet: A multicentre long term international study. Eur. Heart J. 2011, 32, 751–759. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, J.L.; LaPar, D.J.; Kern, J.A.; Kron, I.L.; Bergin, J.D.; Kamath, S.; Ailawadi, G. Does the Society of Thoracic Surgeons risk score accurately predict operative mortality for patients with pulmonary hypertension? J. Thorac. Cardiovasc. Surg. 2013, 146, 631–637. [Google Scholar] [CrossRef] [Green Version]
- Bootsma, I.T.; Scheeren, T.W.L.; De Lange, F.; Haenen, J.; Boonstra, P.W.; Boerma, E.C. Impaired right ventricular ejection fraction after cardiac surgery is associated with a complicated ICU stay. J. Intensive Care 2018, 6, 85. [Google Scholar] [CrossRef]
- Peyrou, J.; Chauvel, C.; Pathak, A.; Simon, M.; Dehant, P.; Abergel, E. Preoperative right ventricular dysfunction is a strong predictor of 3 years survival after cardiac surgery. Clin. Res. Cardiol. 2017, 106, 734–742. [Google Scholar] [CrossRef]
- Vonk Noordegraaf, A.; Westerhof, B.E.; Westerhof, N. The Relationship Between the Right Ventricle and its Load in Pulmonary Hypertension. J. Am. Coll. Cardiol. 2017, 69, 236–243. [Google Scholar] [CrossRef]
- Maganti, M.D.; Rao, V.; Borger, M.A.; Ivanov, J.; David, T.E. Predictors of low cardiac output syndrome after isolated aortic valve surgery. Circulation 2005, 112 (Suppl. S9), I448–I452. [Google Scholar] [CrossRef]
- Kumon, K.; Tanaka, K.; Hirata, T.; Naito, Y.M.; Fujita, T. Organ failures due to low cardiac output syndrome following open heart surgery. Jpn. Circ. J. 1986, 50, 329–335. [Google Scholar] [CrossRef]
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and Mortality Associated With Postoperative Acute Kidney Injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef]
- Lai, C.-C.; Tseng, K.-L.; Ho, C.-H.; Chiang, S.-R.; Chen, C.-M.; Chan, K.-S.; Chao, C.-M.; Hsing, S.-C.; Cheng, K.-C. Prognosis of patients with acute respiratory failure and prolonged intensive care unit stay. J. Thorac. Dis. 2019, 11, 2051–2057. [Google Scholar] [CrossRef] [PubMed]
- Figuero, S.B.; Mur, J.L.M.; García-Lledó, A.; Centella, T.; Salido, L.; Navarro, A.; Martín, A.G.; García-Andrade, I.; Oliva, E.; Zamorano, J.L. Predictors of persistent pulmonary hypertension after mitral valve replacement. Heart Vessels 2016, 31, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Axtell, A.L.; Bhambhani, V.; Moonsamy, P.; Healy, E.W.; Picard, M.H.; Sundt, T.M., 3rd; Wasfy, J.H. Surgery Does Not Improve Survival in Patients with Isolated Severe Tricuspid Regurgitation. J. Am. Coll. Cardiol. 2019, 74, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Lazam, S.; Vanoverschelde, J.-L.; Tribouilloy, C.; Grigioni, F.; Suri, R.M.; Avierinos, J.-F.; de Meester, C.; Barbieri, A.; Rusinaru, D.; Russo, A.; et al. Twenty-Year Outcome After Mitral Repair Versus Replacement for Severe Degenerative Mitral Regurgitation: Analysis of a Large, Prospective, Multicenter, International Registry. Circulation 2017, 135, 410–422. [Google Scholar] [CrossRef]
- Vassileva, C.M.; Boley, T.; Markwell, S.; Hazelrigg, S. Meta-analysis of short-term and long-term survival following repair versus replacement for ischemic mitral regurgitation. Eur. J. Cardio-Thorac. Surg. 2011, 39, 295–303. [Google Scholar] [CrossRef] [Green Version]
- Gammie, J.S.; O’Brien, S.M.; Griffith, B.P.; Ferguson, T.B.; Peterson, E.D. Influence of hospital procedural volume on care process and mortality for patients undergoing elective surgery for mitral regurgitation. Circulation 2007, 115, 881–887. [Google Scholar] [CrossRef] [Green Version]
- Bolling, S.F.; Li, S.; O’Brien, S.M.; Brennan, J.M.; Prager, R.L.; Gammie, J.S. Predictors of mitral valve repair: Clinical and surgeon factors. Ann. Thorac. Surg. 2010, 90, 1904–1911. [Google Scholar] [CrossRef]
- Jiao, Y.; Luo, T.; Zhang, H.; Han, J.; Li, Y.; Jia, Y.; Zheng, S.; Meng, X. Repair versus replacement of mitral valves in cases of severe rheumatic mitral stenosis: Mid-term clinical outcomes. J. Thorac. Dis. 2019, 11, 3951–3961. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographics | Number (%) |
|---|---|
| 1. Gender | |
| 2. Female | 41 (53.9) |
| 3. Male | 35 (46.1) |
| 1. Pre-op AF | |
| 2. No | 37 (48.7) |
| 3. Yes | 39 (51.3) |
| 1. Pre-existing CKD | |
| 2. Yes | 43 (56.6) |
| 3. No | 33 (43.4) |
| 1. Pre-existing respiratory disease | |
| 2. No | 56 (73.7) |
| 3. Yes | 20 (26.3) |
| 1. Etiology of MV disease | |
| 2. Primary MR | 55 (72.4) |
| 3. Secondary MR | 3 (3.9) |
| 4. Mitral stenosis | 9 (11.8) |
| 5. Failed previous MV surgery | 9 (11.8) |
| 1. Etiology of tricuspid valve disease | |
| 2. Primary TR | 2 (2.6) |
| 3. Secondary TR | 74 (97.4) |
| 1. Operation | |
| 2. Mitral valve replacement + tricuspid valve repair | 33 (43.4) |
| 3. Mitral valve repair + tricuspid valve repair | 41 (53.9) |
| 4. Mitral valve replacement + tricuspid valve replacement | 2 (2.6) |
| 1. Degree of TR | |
| 2. Mild | 2 (2.6) |
| 3. Moderate | 25 (32.9) |
| 4. Severe | 49 (64.5) |
| 1. RV dysfunction | |
| 2. Normal | 34 (44.7) |
| 3. Mild | 11 (14.5) |
| 4. Moderate | 18 (23.7) |
| 5. Severe | 13 (17.1) |
| 1. RA volume index | |
| 2. >28 | 51 (69.9) |
| 3. ≤28 | 22 (30.1) |
| 1. RVMPI | |
| 2. <0.6 | 42 (62.7) |
| 3. ≥0.6 | 25 (37.3) |
| 1. RVFAC | |
| 2. ≥0.35 | 16 (21.6) |
| 3. <0.35 | 58 (78.4) |
| 1. RV size (qualitative) | |
| 2. Normal | 30 (40) |
| 3. Dilated | 45 (60) |
| 1. LVEF | |
| 2. Normal | 66 (86.8) |
| 3. Mild | 6 (7.9) |
| 4. Moderate | 3 (3.9) |
| 5. Severe | 1 (1.3) |
| 1. S’ | |
| 2. <9.5 cm/s | 15 (23.8) |
| 3. ≥9.5 cm/s | 48 (76.2) |
| 1. TAPSE | |
| 2. <1.7 cm | 24 (34.3) |
| 3. ≥1.7 cm | 46 (65.7) |
| Renal Failure, n (%) | Respiratory Failure, n (%) | |
|---|---|---|
| 1. LVEF | p = 0.01 | p < 0.001 |
| 2. Hyperdynamic | 0 (0) | 0 (0) |
| 3. Normal | 5 (8.4) | 2 (3.4) |
| 4. Mild | 0 (0) | 1 (16.7) |
| 5. Moderate | 1 (33.3) | 1 (33.3) |
| 6. Severe | 1 (100) | 1 (100) |
| Urgency of surgery | p < 0.001 | p = 0.002 |
| 1. Routine | 2 (3.6) | 1 (1.8) |
| 2. Urgent | 2 (13.6) | 2 (13.3) |
| 3. Emergency | 3 (60.0) | 2 (40.4) |
| 1. S’ | p < 0.001 | p = 0.013 |
| 2. <9.5 cm/s | 4 (26.7) | 3 (20) |
| 3. ≥9.5 cm/s | 0 (0) | 1(2.1) |
| 1. Etiology of MV disease | p < 0.001 | |
| 2. Primary MR | 2 (3.6) | 1 (1.8) |
| 3. Secondary MR | 2 (66.7) | 2 (66.7) |
| 4. Mitral stenosis | 3 (33.3%) | 2 (22.2) |
| 5. Failed previous MV surgery | 0 (0) | 0 (0) |
| 1. TAPSE | p = 0.179 | p = 0.025 |
| 2. <1.7 cm | 4 (16.7) | 4 (16.7) |
| 3. ≥1.7 cm | 3 (6.5) | 1 (2.2) |
| Predictors | Predictor of Mortality | Predictor of Respiratory Failure | Predictor of Renal Failure |
|---|---|---|---|
| LVEF | Yes | Yes | Yes |
| S’ | Yes | Yes | Yes |
| Urgency of surgery | Yes | Yes | Yes |
| Etiology of MV disease | Yes | Yes | Yes |
| Type of operation | Yes | No | No |
| Degree of TR | No | No | No |
| TAPSE | No | Yes | No |
| RV size | |||
| Including redo MV surgery | No | No | No |
| Excluding redo MV surgery | No | Yes | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kew, E.P.; Caruso, V.; Grapsa, J.; Bosco, P.; Lucchese, G. Predictors of Outcome in Patients with Pulmonary Hypertension Undergoing Mitral and Tricuspid Valve Surgery. Medicina 2023, 59, 1103. https://doi.org/10.3390/medicina59061103
Kew EP, Caruso V, Grapsa J, Bosco P, Lucchese G. Predictors of Outcome in Patients with Pulmonary Hypertension Undergoing Mitral and Tricuspid Valve Surgery. Medicina. 2023; 59(6):1103. https://doi.org/10.3390/medicina59061103
Chicago/Turabian StyleKew, Ee Phui, Vincenzo Caruso, Julia Grapsa, Paolo Bosco, and Gianluca Lucchese. 2023. "Predictors of Outcome in Patients with Pulmonary Hypertension Undergoing Mitral and Tricuspid Valve Surgery" Medicina 59, no. 6: 1103. https://doi.org/10.3390/medicina59061103