
Radiographic Outcomes of Conservative and Operative Treatment in Isolated L1 Fractures
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spiegl, U.J.; Fischer, K.; Schmidt, J.; Schnoor, J.; Delank, S.; Josten, C.; Schulte, T.; Heyde, C.-E. The Conservative Treatment of Traumatic Thoracolumbar Vertebral Fractures. Dtsch. Ärzteblatt Int. 2018, 115, 697–704. [Google Scholar] [CrossRef] [PubMed]
- Knop, C.; Blauth, M.; Bühren, V.; Hax, P.M.; Kinzl, L.; Mutschler, W.; Pommer, A.; Ulrich, C.; Wagner, S.; Weckbach, A.; et al. Surgical treatment of injuries of the thoracolumbar transition. 1: Epidemiology. Unfallchirurg 1999, 102, 924–935. [Google Scholar] [CrossRef] [PubMed]
- den Ouden, L.P.; Smits, A.J.; Stadhouder, A.; Feller, R.; Deunk, J.; Bloemers, F.W. Epidemiology of Spinal Fractures in a Level One Trauma Center in the Netherlands: A 10 Years Re-view. Spine 2019, 44, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Heinzelmann, M. Thoracolumbar Spinal Injuries. In Spinal Disorders Fundamentals of Diagnosis and Treatment; Boos, M.N.A., Ed.; Springer: Berlin, Germany, 2008; pp. 883–919. [Google Scholar]
- Azam, M.Q.; Sadat-Ali, M. The Concept of Evolution of Thoracolumbar Fracture Classifications Helps in Surgical Deci-sions. Asian Spine J. 2015, 9, 984–994. [Google Scholar] [CrossRef] [Green Version]
- Soultanis, K.C.; Mavrogenis, A.F.; Starantzis, K.A.; Markopoulos, C.; Stavropoulos, N.A.; Mimidis, G.; Kokkalis, Z.T.; Papagelopoulos, P.J. When and how to operate on thoracic and lumbar spine fractures? Eur. J. Orthop. Surg. Traumatol. 2014, 24, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, A.P.; Spiegl, U.J.; Ekkerlein, H.; Gercek, E.; Hauck, S.; Josten, C.; Kandziora, F.; Katscher, S.; Kobbe, P.; Knop, C.; et al. Treatment of Fractures of the Thoracolumbar Spine: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Glob. Spine J. 2018, 8 (Suppl. 2), 34S–45S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegl, U.J.; Josten, C.; Devitt, B.M.; Heyde, C.-E. Incomplete burst fractures of the thoracolumbar spine: A review of literature. Eur. Spine J. 2017, 26, 3187–3198. [Google Scholar] [CrossRef]
- Weinstein, J.N.; Collalto, P.; Lehmann, T.R. Long-term follow-up of nonoperatively treated thoracolumbar spine fractures. J. Orthop. Trauma 1987, 1, 152–159. [Google Scholar] [CrossRef]
- Moller, A.; Hasserius, R.; Redlund-Johnell, I.; Ohlin, A.; Karlsson, M.K. Nonoperatively treated burst fractures of the thoracic and lumbar spine in adults: A 23- to 41-year follow-up. Spine J. 2007, 7, 701–707. [Google Scholar] [CrossRef]
- Giangregorio, L.M.; MacIntyre, N.; Thabane, L.; Skidmore, C.J.; Papaioannou, A. Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst. Rev. 2013, CD008618. [Google Scholar] [CrossRef]
- Aono, H.; Tobimatsu, H.; Ariga, K.; Kuroda, M.; Nagamoto, Y.; Takenaka, S.; Furuya, M.; Iwasaki, M. Surgical outcomes of temporary short-segment instrumentation without augmentation for thoracolumbar burst fractures. Injury 2016, 47, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Curfs, I.; Grimm, B.; Van Der Linde, M.; Willems, P.; Van Hemert, W. Radiological Prediction of Posttraumatic Kyphosis after Thoracolumbar Fracture. Open Orthop. J. 2016, 10, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Vaccaro, A.R.; Oner, C.; Kepler, C.K.; Dvorak, M.; Schnake, K.; Bellabarba, C.; Reinhold, M.; Aarabi, B.; Kandziora, F.; Chapman, J.; et al. AOSpine thoracolumbar spine injury classification system: Fracture description, neurological status, and key modifiers. Spine 2013, 38, 2028–2037. [Google Scholar] [CrossRef]
- Petersilge, C.A.; Emery, S.E. Thoracolumbar burst fracture: Evaluating stability. Semin. Ultrasound CT MRI 1996, 17, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Pehlivanoglu, T.; Akgul, T.; Bayram, S.; Meric, E.; Ozdemir, M.; Korkmaz, M.; Sar, C. Conservative Versus Operative Treatment of Stable Thoracolumbar Burst Fractures in Neurologically Intact Patients: Is There Any Difference Regarding the Clinical and Radiographic Outcomes? Spine 2020, 45, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Daniaux, H.; Wagner, M.; Kathrein, A.; Lang, T. Fractures of the thoraco-lumbar junction. Conservative management. Orthopade 1999, 28, 682–691. [Google Scholar]
- Ye, B.; Yan, M.; Zhu, H.; Duan, W.; Hu, X.; Ye, Z.; Luo, Z. A Novel Screw Head Design of Pedicle Screw for Reducing The Correction Loss in Patients with Thoracolumbar Vertebral Fractures: A Biomechanical Study. J. Orthop. Transl. 2016, 7, 84–85. [Google Scholar] [CrossRef] [Green Version]
- Siebenga, J.; Leferink, V.J.M.; Segers, M.J.M.; Elzinga, M.J.; Bakker, F.C.; Haarman, H.J.T.M.; Rommens, P.M.; Duis, H.-J.T.; Patka, P. Treatment of traumatic thoracolumbar spine fractures: A multicenter prospective randomized study of operative versus nonsurgical treatment. Spine 2006, 31, 2881–2890. [Google Scholar] [CrossRef]
- Been, H.D.; Poolman, R.W.; Ubags, L.H. Clinical outcome and radiographic results after surgical treatment of post-traumatic thoracolumbar kyphosis following simple type A fractures. Eur. Spine J. 2004, 13, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Defino, H.L.A.; Canto, F.R. Low thoracic and lumbar burst fractures: Radiographic and functional outcomes. Eur. Spine J. 2007, 16, 1934–1943. [Google Scholar] [CrossRef] [Green Version]
- Tropiano, P.; Huang, R.C.; Louis, C.A.; Poitout, D.G.; Louis, R.P. Functional and radiographic outcome of thoracolumbar and lumbar burst fractures managed by closed orthopaedic reduction and casting. Spine 2003, 28, 2459–2465. [Google Scholar] [CrossRef] [PubMed]
- Verlaan, J.J.; Diekerhof, C.H.; Buskens, E.; Van der Tweel, I.; Verbout, A.J.; Dhert, W.J.A.; Oner, F.C. Surgical treatment of traumatic fractures of the thoracic and lumbar spine: A systematic review of the literature on techniques, complications, and outcome. Spine 2004, 29, 803–814. [Google Scholar] [CrossRef] [PubMed]
- Wood, K.; Butterman, G.; Mehbod, A.; Garvey, T.; Jhanjee, R.; Sechriest, V. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study. J. Bone Jt. Surg. 2003, 85, 773–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Roer, N.; De Lange, E.S.; Bakker, F.C.; Vet, H.C.D.; Van Tulder, M.W. Management of traumatic thoracolumbar fractures: A systematic review of the literature. Eur. Spine J. 2005, 14, 527–534. [Google Scholar] [CrossRef]
- Leferink, V.J.M.; Keizer, H.J.E.; Oosterhuis, J.K.; van der Sluis, C.K.; Duis, H.J.T. Functional outcome in patients with thoracolumbar burst fractures treated with dorsal instrumentation and transpedicular cancellous bone grafting. Eur. Spine J. 2003, 12, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulmar, B.; Gühring, M.; Schmälzle, T.; Weise, K.; Badke, A.; Brunner, A. Inter- and intra-observer reliability of the Cobb angle in the measurement of vertebral, local and segmental kyphosis of traumatic lumbar spine fractures in the lateral X-ray. Arch. Orthop. Trauma Surg. 2010, 130, 1533–1538. [Google Scholar] [CrossRef] [PubMed]
- Page, P.S.; Parmar, V.K.; Bond, E.; Josiah, D.T. Radiographic Outcomes of Thoracolumbar AOSpine A3 and A4 Fractures Treated With External Bracing. Cureus 2022, 14, e22490. [Google Scholar] [CrossRef]
- Seo, D.K.; Kim, C.H.; Jung, S.K.; Kim, M.K.; Choi, S.J.; Park, J.H. Analysis of the Risk Factors for Unfavorable Radiologic Outcomes after Fusion Surgery in Thoracolumbar Burst Fracture: What Amount of Postoperative Thoracolumbar Kyphosis Correction is Reasonable? J. Korean Neurosurg. Soc. 2019, 62, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daly, R.M.; Via, J.D.; Duckham, R.L.; Fraser, S.F.; Helge, E.W. Exercise for the prevention of osteoporosis in postmenopausal women: An evidence-based guide to the optimal prescription. Braz. J. Phys. Ther. 2019, 23, 170–180. [Google Scholar] [CrossRef]
- Patel, D.; Worley, J.R.; Volgas, D.A.; Crist, B.D. The Effectiveness of Osteoporosis Screening and Treatment in the Midwest. Geriatr. Orthop. Surg. Rehabil. 2018, 9, 2151459318765844. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Curtis, E.M.; Cooper, C.; Harvey, N.C. State of the art in osteoporosis risk assessment and treatment. J. Endocrinol. Investig. 2019, 42, 1149–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cosman, F.; De Beur, S.J.; LeBoff, M.S.; Lewiecki, E.M.; Tanner, B.; Randall, S.; Lindsay, R. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Osteoporos. Int. 2014, 25, 2359–2381. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Young | Elderly | Operative | Conservative | |
|---|---|---|---|---|
| Number of patients | 78 | 153 | 33 | 198 |
| Sex | ||||
| Female, n (%) | 37 (47.4) | 100 (65.4) | 21 (63.6) | 120 (60.6) |
| Male, n (%) | 41 (52.6) | 53 (34.6) | 12 (36.4) | 78 (39.4) |
| Age (mean ± SD) | 41.4 ± 13.5 | 79 ± 8.8 | 52.8 ± 19.7 | 67.0 ± 19.4 |
| Mechanism of injury | ||||
| Fall from stand | 29 (37.2) | 136 (88.8) | 23 (69.7) | 142 (71.7) |
| Fall from height | 8 (10.3) | 2 (1.3) | 8 (24.2) | 2 (1.0) |
| Traffic accidents | 21 (26.9) | 7 (4.6) | 9 (27.3) | 19 (9.6) |
| Sport injuries | 19 (24.4) | 0 | 2 (6.0) | 17 (8.6) |
| AO-Classification | ||||
| A1 | 60 (76.9) | 140 (91.5) | 21 (63.6) | 179 (90.4) |
| A2 | 0 | 1 (0.7) | 0 | 1 (0.5) |
| A3 | 15 (19.2) | 10 (6.5) | 18 (54.5) | 7 (3.5) |
| A4 | 2 (2.6) | 1 (0.7) | 3 (9.1) | 0 |
| B2 | 1 (1.3) | 0 | 1 (3.0) | 0 |
| B3 | 0 | 1 (0.7) | 1 (3.0) | 0 |
| Risk factors | ||||
| Osteoporosis | 6 (7.7) | 44 (28.8) | 11 (33.3) | 38 (19.2) |
| Diabetes | 6 (7.7) | 17 (12.7) | 4 (12.1) | 19 (9.6) |
| Mb. Ankylosing spondylitis | 2 (2.6) | 3 (2.0) | 3 (9.1) | 2 (1.0) |
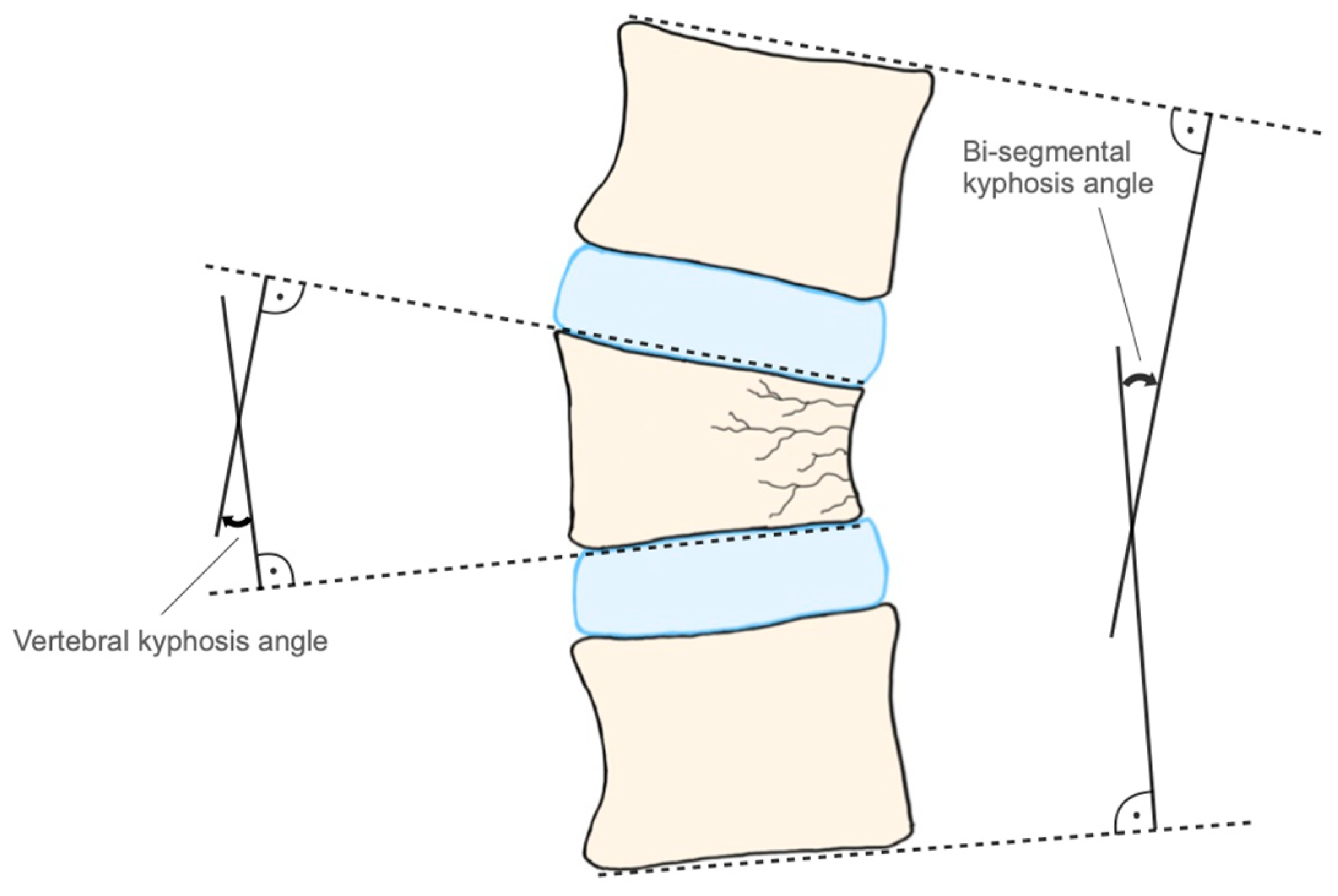
| Vert. Pre-Op | Vert. Post-Op | p-Value | Bi-Seg. Pre-Op | Bi-seg. Post-Op | p-Value | |
|---|---|---|---|---|---|---|
| Conservative young (mean ± SD) | 6.73 ± 4.07 | 9.65 ± 4.54 | 0.007 | 6.06 ± 5.43 | 7.81 ± 5.86 | 0.044 |
| Conservative old (mean ± SD) | 7.37 ± 5.21 | 10.19 ± 5.64 | 0.0001 | 7.99 ± 6.36 | 10.34 ± 6.91 | 0.0001 |
| Operative young (mean ± SD) | 9.59 ± 4.95 | 3.27 ± 2.84 | 0.003 | 10.00 ± 5.87 | 5.72 ± 4.14 | 0.07 |
| Operative old (mean ± SD) | 7.69 ± 4.0 | 3.52 ± 3.39 | 0.007 | 6.45 ± 5.11 | 6.24 ± 5.06 | 1.0 |
| Young | Old | |
|---|---|---|
| Conservative (n = 198) | 1 (0.5%) | 16 (8%) |
| Operative (n = 33) | 4 (12%) | 6 (18%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuller, A.; Payr, S.; Pichler, L.; Sator, T.; Ploetzl, A.; Chocholka, B.; Tiefenboeck, T.M.; Sarahrudi, K. Radiographic Outcomes of Conservative and Operative Treatment in Isolated L1 Fractures. Medicina 2023, 59, 695. https://doi.org/10.3390/medicina59040695
Schuller A, Payr S, Pichler L, Sator T, Ploetzl A, Chocholka B, Tiefenboeck TM, Sarahrudi K. Radiographic Outcomes of Conservative and Operative Treatment in Isolated L1 Fractures. Medicina. 2023; 59(4):695. https://doi.org/10.3390/medicina59040695
Chicago/Turabian StyleSchuller, Andrea, Stephan Payr, Lorenz Pichler, Thomas Sator, Anna Ploetzl, Britta Chocholka, Thomas M. Tiefenboeck, and Kambiz Sarahrudi. 2023. "Radiographic Outcomes of Conservative and Operative Treatment in Isolated L1 Fractures" Medicina 59, no. 4: 695. https://doi.org/10.3390/medicina59040695