
Marker Screw Utilization for Minimally Invasive Transforaminal Lumbar Interbody Fusion (MS-MIS TLIF): Promises and Advantages

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Measures
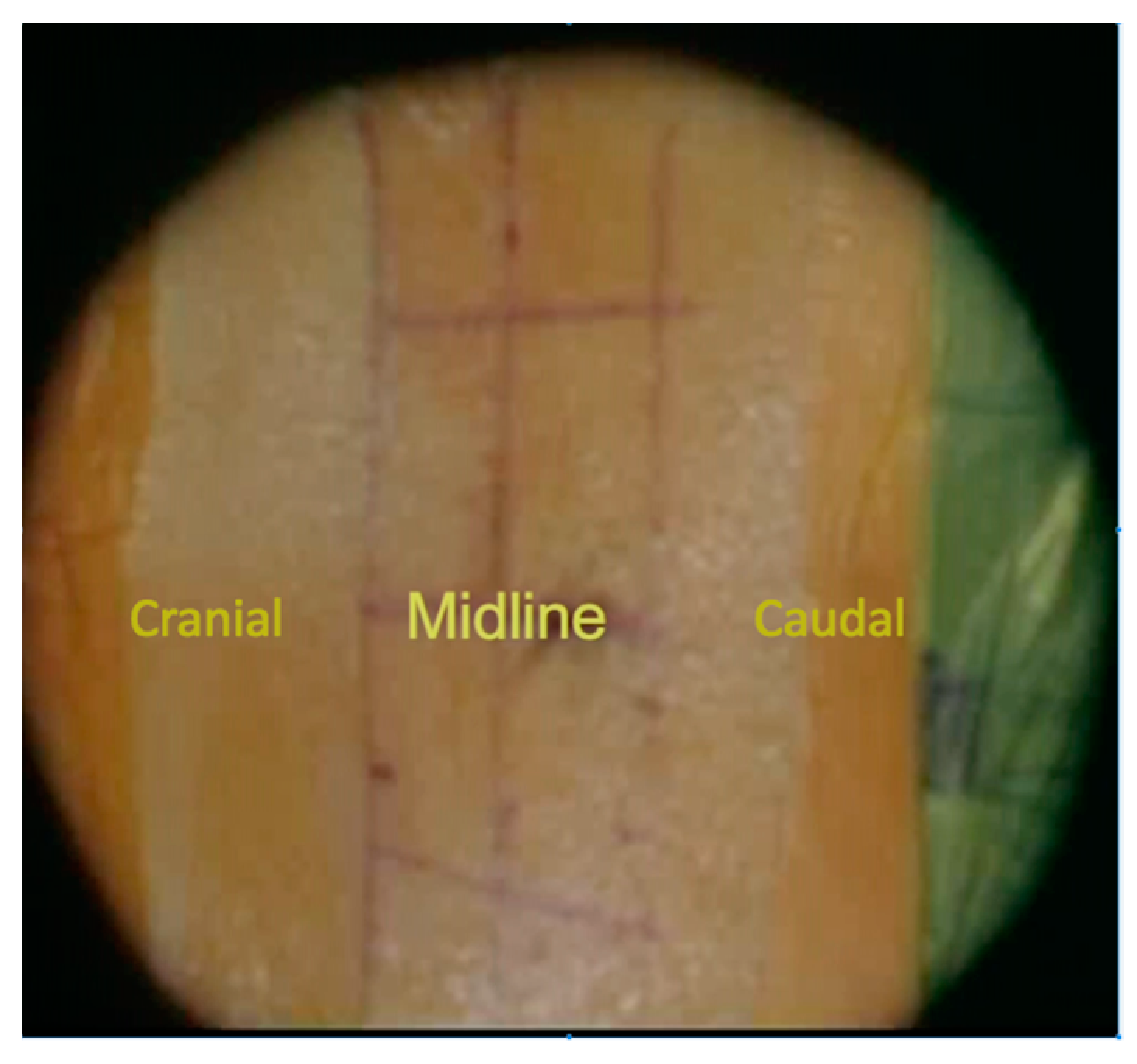
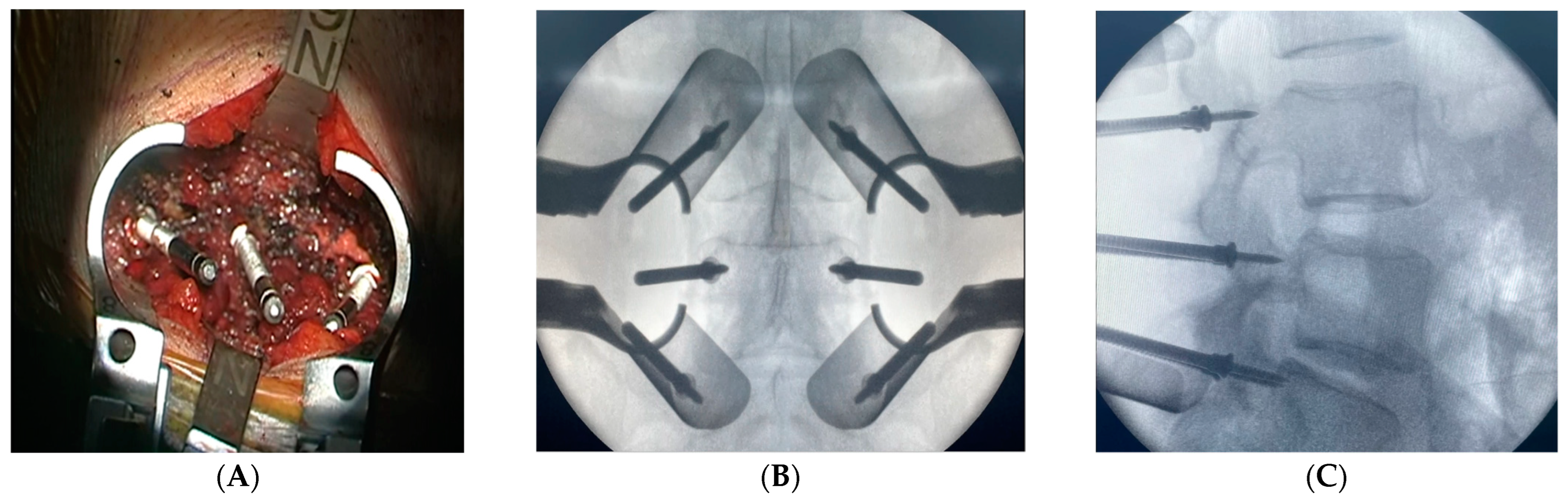
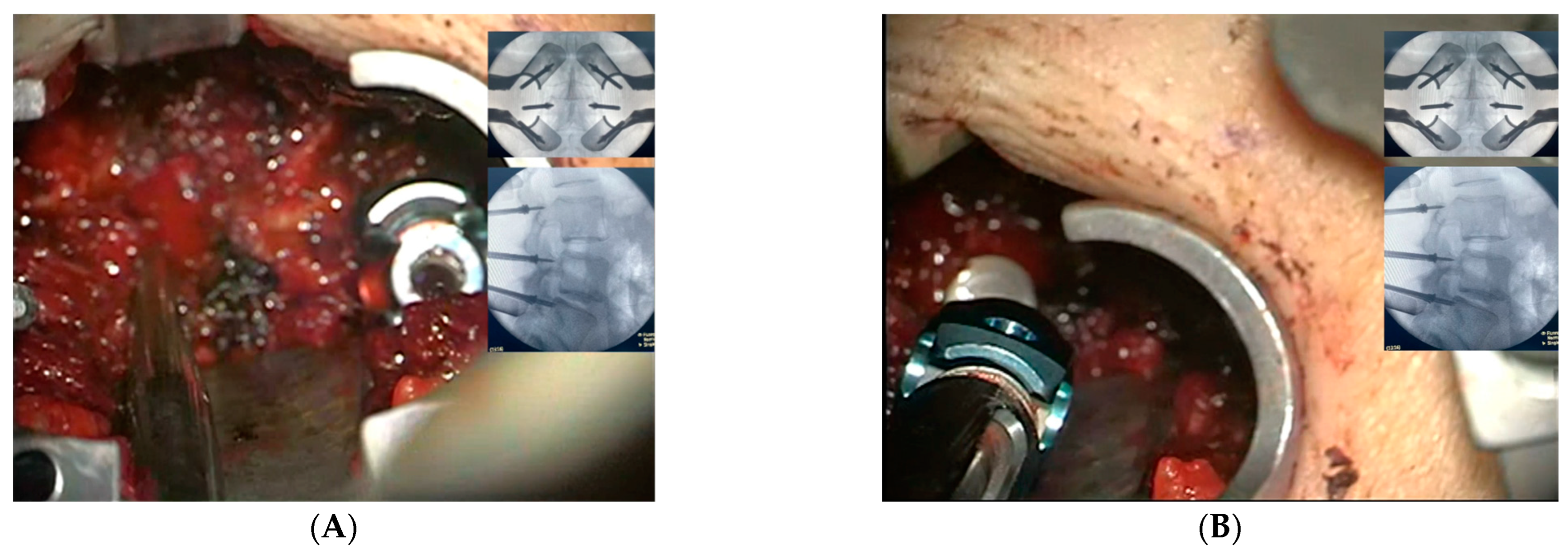
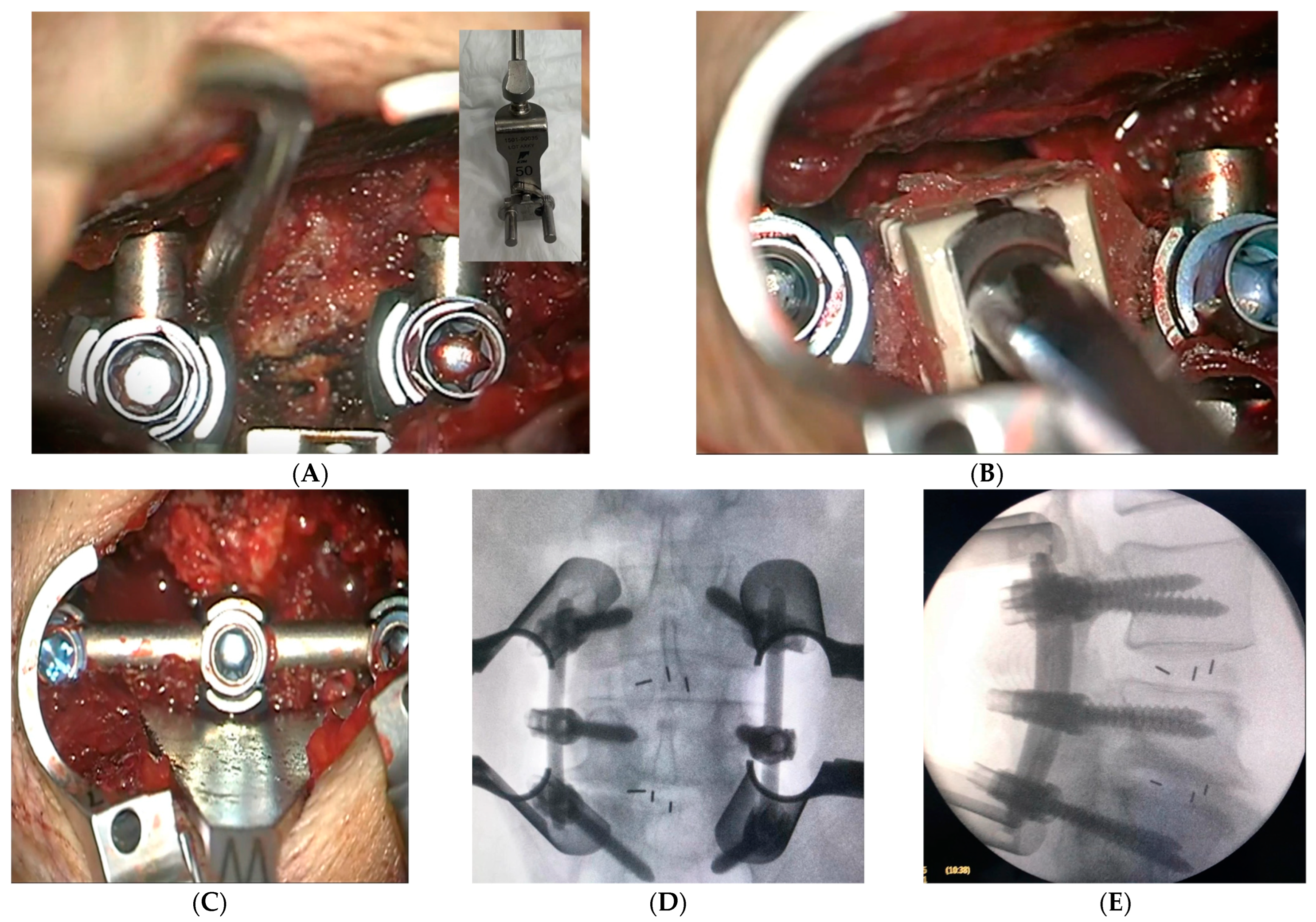
2.3. Surgical Intervention and Marker Screw Utilization
2.4. Statistical Analyses and Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [CrossRef] [PubMed]
- Khashab, M.A.M.; Alsofiani, B.; Algamedi, O.; Shulan, M. Open versus Minimally invasive transforaminal lumbar interbody fusion: Intermediate outcomes in overweight and obese patients. J. Musculoskelet. Surg. Res. 2020, 4, 82. [Google Scholar]
- Kim, H.J.; Park, E.S.; Lee, S.H.; Park, C.H.; Chung, S.W. Reduction of Radiation Exposure by Modifying Imaging Manner and Fluoroscopic Settings during Percutaneous Pedicle Screw Insertion. J. Korean Neurosurg. Soc. 2021, 64, 933–943. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Chang, H.K.; Wu, J.C.; Tu, T.H.; Cheng, H.; Huang, W.C. Comparison of Radiation Exposure Between O-Arm Navigated and C-Arm Guided Screw Placement in Minimally Invasive Transforaminal Lumbar Interbody Fusion. World Neurosurg. 2020, 139, e489–e495. [Google Scholar] [CrossRef] [PubMed]
- Lener, S.; Wipplinger, C.; Hernandez, R.N.; Hussain, I.; Kirnaz, S.; Navarro-Ramirez, R.; Schmidt, F.A.; Kim, E.; Härtl, R. Defining the MIS-TLIF: A Systematic Review of Techniques and Technologies Used by Surgeons Worldwide. Glob. Spine J. 2020, 10, 151s–167s. [Google Scholar] [CrossRef] [PubMed]
- Fujimori, T.; Le, H.; Schairer, W.W.; Berven, S.H.; Qamirani, E.; Hu, S.S. Does transforaminal lumbar interbody fusion have advantages over posterolateral lumbar fusion for degenerative spondylolisthesis? Glob. Spine J. 2015, 5, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.H.; Hwang, R.W.; Lee, G.H.; Joshi, R.; Baker, K.C.; Arnold, P.; Sasso, R.; Park, D.; Fischgrund, J. Comparing rates of early pedicle screw loosening in posterolateral lumbar fusion with and without transforaminal lumbar interbody fusion. Spine J. 2020, 20, 1438–1445. [Google Scholar] [CrossRef]
- Elmekaty, M.; Kotani, Y.; Mehy, E.E.; Robinson, Y.; Tantawy, A.E.; Sekiguchi, I.; Fujita, R. Clinical and Radiological Comparison between Three Different Minimally Invasive Surgical Fusion Techniques for Single-Level Lumbar Isthmic and Degenerative Spondylolisthesis: Minimally Invasive Surgical Posterolateral Fusion versus Minimally Invasive Surgical Transforaminal Lumbar Interbody Fusion versus Midline Lumbar Fusion. Asian Spine J. 2018, 12, 870–879. [Google Scholar] [CrossRef] [Green Version]
- Tovar, M.A.; Dowlati, E.; Zhao, D.Y.; Khan, Z.; Pasko, K.B.D.; Sandhu, F.A.; Voyadzis, J.M. Robot-assisted and augmented reality-assisted spinal instrumentation: A systematic review and meta-analysis of screw accuracy and outcomes over the last decade. J. Neurosurg. Spine 2022, 25, 1–16. [Google Scholar] [CrossRef]
- Parker, S.L.; McGirt, M.J.; Farber, S.H.; Amin, A.G.; Rick, A.M.; Suk, I.; Bydon, A.; Sciubba, D.M.; Wolinsky, J.P.; Gokaslan, Z.L.; et al. Accuracy of free-hand pedicle screws in the thoracic and lumbar spine:Analysis of 6816 consecutive screws. Neurosurgery 2011, 68, 170–178. [Google Scholar] [CrossRef]
- Guilfoyle, M.R.; Seeley, H.; Laing, R.J. The Short Form 36 health survey in spine disease--validation against condition-specific measures. Br. J. Neurosurg. 2009, 23, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Algarni, A.S.; Ghorbel, S.; Jones, J.G.; Guermazi, M. Validation of an Arabic version of the Oswestry index in Saudi Arabia. Ann. Phys. Rehabil. Med. 2014, 57, 653–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, K.A.; Yagoub, U.; Elsatouhy, M.; Al Sanosi, R.; Mohamud, S. Reliability and Validity of the Arabic Version of the SF-36 Health Survey Questionnaire in Population of Khat Chewers—Jazan Region-Kingdom of Saudi Arabia. Appl. Res. Qual. Life 2013, 10, 1–13. [Google Scholar] [CrossRef]
- Bin Abd Razak, H.R.; Dhoke, P.; Tay, K.S.; Yeo, W.; Yue, W.M. Single-Level Minimally Invasive Transforaminal Lumbar Interbody Fusion Provides Sustained Improvements in Clinical and Radiological Outcomes up to 5 Years Postoperatively in Patients with Neurogenic Symptoms Secondary to Spondylolisthesis. Asian Spine J. 2017, 11, 204–212. [Google Scholar] [CrossRef] [Green Version]
- Modi, H.N.; Shrestha, U. Comparison of Clinical Outcome and Radiologic Parameters in Open TLIF Versus MIS-TLIF in Single- or Double-Level Lumbar Surgeries. Int. J. Spine Surg. 2021, 15, 962–970. [Google Scholar] [CrossRef]
- Xie, L.; Wu, W.J.; Liang, Y. Comparison between Minimally Invasive Transforaminal Lumbar Interbody Fusion and Conventional Open Transforaminal Lumbar Interbody Fusion: An Updated Meta-analysis. Chin. Med. J. 2016, 129, 1969–1986. [Google Scholar] [CrossRef]
- Rampersaud, Y.R.; Foley, K.T.; Shen, A.C.; Williams, S.; Solomito, M. Radiation exposure to the spine surgeon during fluoroscopically assisted pedicle screw insertion. Spine 2000, 25, 2637–2645. [Google Scholar] [CrossRef]
- Funao, H.; Ishii, K.; Momoshima, S.; Iwanami, A.; Hosogane, N.; Watanabe, K.; Nakamura, M.; Toyama, Y.; Matsumoto, M. Surgeons’ exposure to radiation in single- and multi-level minimally invasive transforaminal lumbar interbody fusion; a prospective study. PLoS ONE 2014, 9, e95233. [Google Scholar] [CrossRef] [Green Version]
- Mariscalco, M.W.; Yamashita, T.; Steinmetz, M.P.; Krishnaney, A.A.; Lieberman, I.H.; Mroz, T.E. Radiation exposure to the surgeon during open lumbar microdiscectomy and minimally invasive microdiscectomy: A prospective, controlled trial. Spine 2011, 36, 255–260. [Google Scholar] [CrossRef]
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP publication 103. Ann. ICRP 2007, 37, 1–332. [Google Scholar] [CrossRef]
- Bindal, R.K.; Glaze, S.; Ognoskie, M.; Tunner, V.; Malone, R.; Ghosh, S. Surgeon and patient radiation exposure in minimally invasive transforaminal lumbar interbody fusion. J. Neurosurgery. Spine 2008, 9, 570–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kouyoumdjïan, P.; Gras-Combe, G.; Grelat, M.; Fuentes, S.; Blondel, B.; Tropiano, P.; Zairi, F.; Beaurain, J.; Charles, Y.P.; Dhenin, A.; et al. Surgeon’s and patient’s radiation exposure during percutaneous thoraco-lumbar pedicle screw fixation: A prospective multicenter study of 100 cases. Orthop. Traumatol. Surg. Res. OTSR 2018, 104, 597–602. [Google Scholar] [CrossRef] [PubMed]
- Marco, R.A.W.; Curry, M.C.; Mujezinovic, F.; Linton, J. Decreased radiation exposure using pulsed fluoroscopy and a detachable pedicle marker and probe to place pedicle screws: A comparison to current fluoroscopy techniques and CT navigation. Spine Deform. 2020, 8, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.B.; Wu, J.L.; Zuo, R.; Li, C.Q.; Zhang, C.; Zhou, Y. Does MIS-TLIF or TLIF result in better pedicle screw placement accuracy and clinical outcomes with navigation guidance? BMC Musculoskelet. Disord. 2022, 23, 153. [Google Scholar] [CrossRef] [PubMed]
- Alhabib, H.; Nataraj, A.; Khashab, M.; Mahood, J.; Kortbeek, F.; Fox, R. Pedicle screw insertion in the thoracolumbar spine: Comparison of 4 guidance techniques in the intact cadaveric spine. J. Neurosurg. Spine 2011, 14, 664–669. [Google Scholar] [CrossRef]
- Shin, M.H.; Ryu, K.S.; Park, C.K. Accuracy and Safety in Pedicle Screw Placement in the Thoracic and Lumbar Spines: Comparison Study between Conventional C-Arm Fluoroscopy and Navigation Coupled with O-Arm® Guided Methods. J. Korean Neurosurg. Soc. 2012, 52, 204–209. [Google Scholar] [CrossRef]
- Droeghaag, R.; Hermans, S.M.; Caelers, I.M.H.; Evers, S.A.; Van Hemert, W.W.; Van Santbrink, H. Cost-effectiveness of open transforaminal lumbar interbody fusion (OTLIF) versus minimally invasive transforaminal lumbar interbody fusion (MITLIF): A systematic review and meta-analysis. Spine J. 2021, 21, 945–954. [Google Scholar] [CrossRef]
- Yao, Y.C.; Lin, H.H.; Chou, P.H.; Wang, S.T.; Chang, M.C. Differences in the interbody bone graft area and fusion rate between minimally invasive and traditional open transforaminal lumbar interbody fusion: A retrospective short-term image analysis. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 2019, 28, 2095–2102. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean age (year) | 57.92 ± 14.2 |
| Gender (M/F) | 14/23 |
| Mean BMI (kg/m2) | 32.8 ± 4.2 |
| DM (%) | 29.7 |
| HTN (%) | 40.5 |
| CKD (%) | 5.4 |
| Dyslipidemia (%) | 18.9 |
| CAD (%) | 5.4 |
| The mean time since surgery (m) | 28.4 ± 5.6 |
| Indications (%) | |
| Degenerative disc disease | 35.1 |
| Spinal stenosis | 16.2 |
| Spondylolisthesis | 35.1 |
| Prolapsed intervertebral discs | 13.5 |
| Levels of surgery (%) | |
| L3–L4 | 5.4 |
| L4–L5 | 45.9 |
| L5–S1 | 16.2 |
| Two levels | 32.4 |
| Duration of surgery (hours ± SD) | 2.97 ± 0.7 |
| Estimated blood loss (mL ± SD) | 126.7 ± 72.1 |
| Decrease in hemoglobin (g/dL ± SD) | 1.3 ± 0.6 |
| Hospitalization time (days ± SD) | 2.68 ± 1.4 |
| Time before ambulation (days ± SD) | 1 ± 1.1 |
| Preoperative (Mean ± SD) | Six Months Postoperative (Mean ± SD) | Improvement in Score (Mean ± SD) | p-Value | |
|---|---|---|---|---|
| ODI | 60.3 ± 17.5 | 28.6 ± 18.9 | 29.1 ± 25.1 | 0.000 * |
| SF-36 | ||||
| Physical functioning | 25 ± 23.7 | 51.5 ± 29.1 | 27.4 ± 39.3 | 0.000 * |
| Role limitations due to physical health | 12.8 ± 32.8 | 52.1 ± 42.6 | 39.8 ± 41 | 0.000 * |
| Role limitations due to emotional problems | 20.9 ± 37.9 | 68.5 ± 40.3 | 47.7 ± 45.5 | 0.000 * |
| Energy and fatigue | 30 ± 18.6 | 58.4 ± 20.1 | 28.1 ± 25.9 | 0.000 * |
| Emotional well-being | 49.7.3 ± 14.7 | 67.6 ± 17.3 | 18.3 ± 21.5 | 0.000 * |
| Social functioning | 40.3 ± 28.1 | 74.2 ± 28.5 | 34.1 ± 37.9 | 0.000 * |
| Body pain | 26.3 ± 24.4 | 64.5 ± 25.8 | 37.3 ± 34.6 | 0.000 * |
| General health | 44.5 ± 19.8 | 65.2 ± 17 | 20.8 ± 21.8 | 0.000 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khashab, M.; Karami, M.; Alswat, M.; Elkhalifa, M. Marker Screw Utilization for Minimally Invasive Transforaminal Lumbar Interbody Fusion (MS-MIS TLIF): Promises and Advantages. Medicina 2023, 59, 585. https://doi.org/10.3390/medicina59030585
Khashab M, Karami M, Alswat M, Elkhalifa M. Marker Screw Utilization for Minimally Invasive Transforaminal Lumbar Interbody Fusion (MS-MIS TLIF): Promises and Advantages. Medicina. 2023; 59(3):585. https://doi.org/10.3390/medicina59030585
Chicago/Turabian StyleKhashab, Mohammed, Moyassar Karami, Muath Alswat, and Mohamed Elkhalifa. 2023. "Marker Screw Utilization for Minimally Invasive Transforaminal Lumbar Interbody Fusion (MS-MIS TLIF): Promises and Advantages" Medicina 59, no. 3: 585. https://doi.org/10.3390/medicina59030585