
Does the Rechallenge with Another CDK 4/6 Inhibitor in Breast Cancer Work? A Case Report and Literature Review
 ,
,
Abstract
:1. Introduction
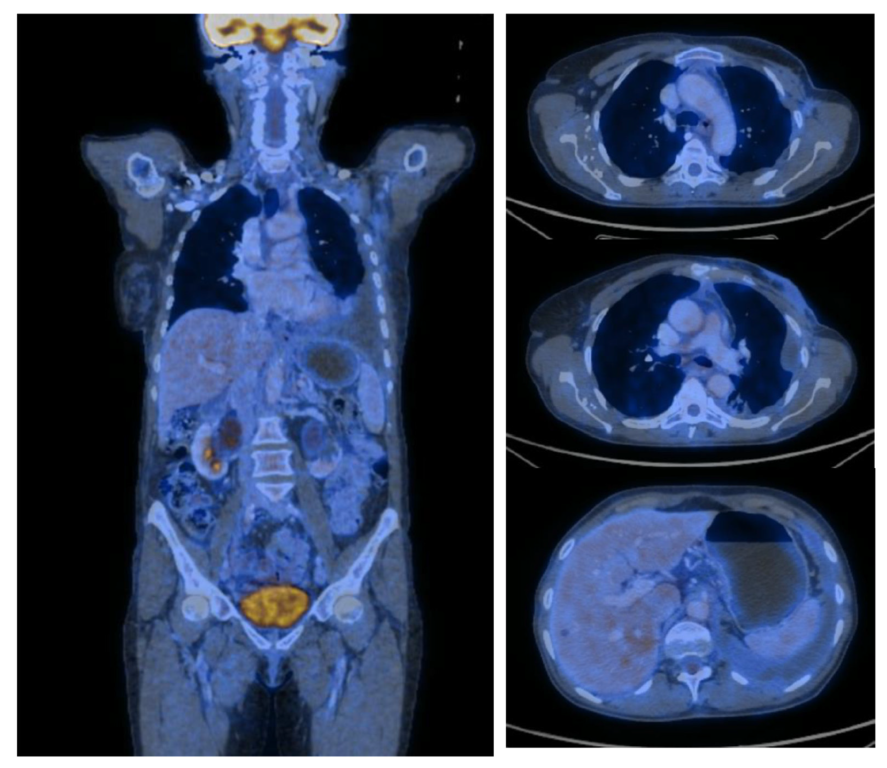
2. Case Report
3. Discussion
3.1. Rationale for CDK4/6 Inhibitors Choice
3.2. Elevation of Liver Enzymes
3.3. Gastrointestinal Toxicities
3.4. Neutropenia
3.5. Similar Cases of Rechallenge in the Literature
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ULN | Upper Limit of Normal |
| AI | Aromatase Inhibitor |
| HR | Hormone Receptor |
| HER2 | Human Epidermal Growth Factor 2 |
| Er | Estrogen receptor |
| PgR | Progesterone receptor |
| Ki67 | Nuclear antigen that is an excellent marker of active cell proliferation |
| PET-CT | Positron Emission Tomography |
| SUV | Standardized Uptake Values |
| M1HEP | Hepatic metastases |
| M1LYM | Lymphatic metastases |
| M1ADR | Adrenal metastases |
| G-CSF | Granulocyte Colony-Stimulating Factor |
| NCCN | National Comprehensive Cancer Network |
| IV | Intravenous |
| EKG | Electrocardiography |
| CBC | Complete Blood Count |
| PTV50 | Median Planning Target Volume |
| Gy | Gray |
| Fx | Fractions |
| IMRT-VMAT | Intensity Modulated Radiotherapy—Volumetric Modulated Arc Therapy |
| ALT | Alanine Aminotransferase |
| AST | Aspartate Aminotransferase |
| CT | Computed Tomography |
| PFS | Progression Free Survival |
| OS | Overall Survival |
References
- Stravodimou, A.; Voutsadakis, I.A. The future of ER+/HER2− metastatic breast cancer therapy: Beyond PI3K inhibitors. Anticancer Res. 2020, 40, 4829–4841. [Google Scholar] [CrossRef] [PubMed]
- Pernas, S.; Tolaney, S.M.; Winer, E.P.; Goel, S. CDK4/6 inhibition in breast cancer: Current practice and future directions. Ther. Adv. Med. Oncol. 2018, 10, 175883591878645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuentes-Antrás, J.; de Luna, A.; López de Sá, A.; Ocaña, A.; García-Sáenz, J.Á.; Moreno, F. Safety and efficacy of cyclin-dependent kinase inhibitor rechallenge following ribociclib-induced limiting hypertransaminasemia. Breast 2020, 54, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Raschi, E.; Fusaroli, M.; Ardizzoni, A.; Poluzzi, E.; De Ponti, F. Cyclin-dependent kinase 4/6 inhibitors and interstitial lung disease in the FDA adverse event reporting system: A pharmacovigilance assessment. Breast Cancer Res. Treat. 2021, 186, 219–227. [Google Scholar] [CrossRef] [PubMed]
- Gelbert, L.M.; Cai, S.; Lin, X.; Sanchez-Martinez, C.; del Prado, M.; Lallena, M.J.; Torres, R.; Ajamie, R.T.; Wishart, G.N.; Flack, R.S.; et al. Preclinical characterization of the CDK4/6 inhibitor LY2835219: In-vivo cell cycle-dependent/independent anti-tumor activities alone/in combination with gemcitabine. Investig. New Drugs 2014, 32, 825–837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malumbres, M.; Barbacid, M. Cell cycle, CDKs and cancer: A changing paradigm. Nat. Rev. Cancer 2009, 9, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Goetz, M.P.; Hamilton, E.P.; Campone, M.; Hurvitz, S.A.; Cortes, J.; Johnston, S.R.D.; Jerusalem, G.H.M.; Graham, H.; Wang, H.; Litchfield, L.; et al. Acquired genomic alterations in circulating tumor DNA from patients receiving abemaciclib alone or in combination with endocrine therapy. J. Clin. Oncol. 2020, 38, 3519. [Google Scholar] [CrossRef]
- Turner, N.C.; Slamon, D.J.; Ro, J.; Bondarenko, I.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Overall survival with palbociclib and fulvestrant in advanced breast cancer. N. Engl. J. Med. 2018, 379, 1926–1936. [Google Scholar] [CrossRef] [PubMed]
- Hortobagyi, G.N.; Stemmer, S.M.; Burris, H.A.; Yap, Y.S.; Sonke, G.S.; Paluch-Shimon, S.; Campone, M.; Petrakova, K.; Blackwell, K.L.; Winer, E.P.; et al. Updated results from MONALEESA-2, a phase III trial of first-line ribociclib plus letrozole versus placebo plus letrozole in hormone receptor-positive, HER2-negative advanced breast cancer. Ann. Oncol. 2018, 29, 1541–1547. [Google Scholar] [CrossRef] [PubMed]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.-A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dickler, M.N.; Tolaney, S.M.; Rugo, H.S.; Cortés, J.; Diéras, V.; Patt, D.; Wildiers, H.; Hudis, C.A.; O’Shaughnessy, J.; Zamora, E.; et al. MONARCH 1, a phase II study of abemaciclib, a CDK4 and CDK6 inhibitor, as a single agent, in patients with refractory HR+/HER2− metastatic breast cancer. Clin. Cancer Res. 2017, 23, 5218–5224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sledge, G.W.; Toi, M.; Neven, P.; Sohn, J.; Inoue, K.; Pivot, X.; Burdaeva, O.; Okera, M.; Masuda, N.; Kaufman, P.A.; et al. MONARCH 2: Abemaciclib in combination with fulvestrant in women with HR+/HER2− advanced breast cancer who had progressed while receiving endocrine therapy. J. Clin. Oncol. 2017, 35, 2875–2884. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.; Martin, M.; Di Leo, A.; Im, S.-A.; Awada, A.; Forrester, T.; Frenzel, M.; Hardebeck, M.C.; Cox, J.; Barriga, S.; et al. MONARCH 3 final PFS: A randomized study of abemaciclib as initial therapy for advanced breast cancer. Npj Breast Cancer 2019, 5, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thill, M.; Schmidt, M. Management of adverse events during cyclin-dependent kinase 4/6 (CDK4/6) inhibitor-based treatment in breast cancer. Ther. Adv. Med. Oncol. 2018, 10, 175883591879332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goetz, M.P.; Toi, M.; Campone, M.; Sohn, J.; Paluch-Shimon, S.; Huober, J.; Park, I.H.; Trédan, O.; Chen, S.-C.; Manso, L.; et al. MONARCH 3: Abemaciclib as initial therapy for advanced breast cancer. J. Clin. Oncol. 2017, 35, 3638–3646. [Google Scholar] [CrossRef] [PubMed]
- Im, S.-A.; Lu, Y.-S.; Bardia, A.; Harbeck, N.; Colleoni, M.; Franke, F.; Chow, L.; Sohn, J.; Lee, K.-S.; Campos-Gomez, S.; et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N. Engl. J. Med. 2019, 381, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Meynard, L.; Grellety, T. CDK 4/6 inhibitor successful rechallenge after limiting hepatic toxicity. Breast J. 2020, 26, 255–257. [Google Scholar] [CrossRef] [PubMed]
- Rechallenge with a different CDK 4/6 inhibitor after ribociclib induced hepatotoxicity, 2020. Available online: https://www.bib.irb.hr/1147359 (accessed on 16 March 2023).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Result | Normal Range |
|---|---|---|
| Hemoglobin | 13.8 | 11.7–15.9/g/dL |
| Hematocrit | 5.30 | 35.0–47.0/% |
| Platelets | 342 | 150–400/× 102/uL |
| White blood cells | 5.49 | 4.6–10.2/× 109/uL |
| Neutrophils | 3.36 | 1.5–6.9/× 103/uL |
| Lymphocytes | 1.56 | 0.6–3.4/× 103/uL |
| Monocytes | 0.47 | 0–0.9/× 103/uL |
| Eosinophils | 0.06 | 0–0.7/× 103/uL |
| AST | 41 | 14–36/U/L |
| ALT | 18 | 5–35/U/L |
| eGFR CKD-EPI | 89 | >90/L/min/1.73 m2 |
| Total Bilirubin | 0.8 | 0.2–1.3/mg/dL |
| Urea | 49 | 15–50/mg/dL |
| Creatinine | 0.7 | 0.7–1.2/mg/dL |
| Sodium | 142 | 137–145/mmol/L |
| Potassium | 4.9 | 3.6–5.1/mmol/L |
| LDH | 439 | 120–246/U/L |
| Glucose | 104 | 65–105/mg/dL |
| Erythrocyte sedimentation rate | 26 | 0–20/mm/1 h |
| Calcium | 1.91 | 2.0–2.5/mEg/L |
| Triglycerides | 153 | 35–150/mg/dL |
| Grade 1 (>3 × ULN) | Grade 2 (>3 to 5 × ULN) | Grade 3 (>5 to 20 × ULN) | Grade 4 (>20 × ULN) | |
|---|---|---|---|---|
| AST and/or ALT elevations from baseline **, without increase in total bilirubin above 2 × ULN | No dose adjustment is required. | Baseline grade <2: Dose interruption until recovery to ≤ baseline grade, then resumption of Kisqali at same dose level. If grade 2 recurs, resume Kisqali at next lower dose level. Baseline grade = 2: No dose interruption | Dose interruption of Kisqali until recovery to ≤ baseline grade, then resumption at next lower dose level. If grade 3 recurs, discontinue Kisqali. | Discontinue Kisqali. |
| Combined elevations in AST and/or ALT together with total bilirubin increase in the absence of cholestasis | If patients develop ALT and/or AST >3 × ULN along with total bilirubin >2 × ULN irrespective of baseline grade, discontinue Kisqali. | |||
| Toxicity | Management Recommendations |
|---|---|
| Grade 1 | No dose adjustment required. |
| Grade 2 | If toxicity does not resolve within 24 h to Grade 1 or less, suspend dose until resolution. Dose reduction is not required. |
| Grade 2 that persists or recurs after resuming the same dose despite maximal supportive measures | Suspend dose until toxicity resolves to Grade 1 or less. Resume at next lower dose. |
| Grade 3 or 4 or requires hospitalization |
| Toxicity | Management Recommendations |
|---|---|
| Grade 1 or 2 | No dose adjustment required. |
| Grade 3 | Suspend dose until toxicity resolves to Grade 2 or less. Dose reduction is not required. |
| Grade 3, recurrent; or Grade 4 | Suspend dose until toxicity resolves to Grade 2 or less. Resume at next lower dose. |
| Patient requires administration of blood cell growth factors | Suspend abemaciclib dose for at least 48 h after the last dose of blood cell growth factors was administered and until toxicity resolves to Grade 2 or less. Resume at next lower dose unless the dose was already reduced for the toxicity that led to the use of the growth factor. |
| AST | ALT | Diarrhea | Neutropenia | |||||
|---|---|---|---|---|---|---|---|---|
| Grade 1 + 2 % | Grade 3 + 4 % | Grade 1 + 2 % | Grade 3 + 4 % | Grade 1 + 2 % | Grade 3 + 4 % | Grade 1 + 2 % | Grade 3 + 4 % | |
| MONALEESA-2 (N = 334) | 44 | 7 | 46 | 10 | 33.8 | 1.2 | 33 | 60 |
| MONALEESA-7 (N = 248) | 37 | 4.8 | 33 | 6 | NA | NA | 29 | 63 |
| MONARCH-2 (N = 441) | 33.1 | 3.9 | 36.4 | 4.6 | 73 | 13 | 54.5 | 32.5 |
| MONARCH-3 (N = 327) | 33.2 | 3.8 | 41.4 | 6.6 | 72 | 9 | 58.1 | 21.9 |
| PALOMA-2 (N = 444) | 49 | 3 | 40 | 3 | 25 | 1 | 14 | 66 |
| PALOMA-3 (N = 345) | 39 | 4 | 34 | 2 | 24 | 0 | 17 | 66 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stanciu, I.-M.; Pirlog, C.F.; Anghel, A.-W.; Parosanu, A.I.; Olaru, C.M.; Orlov-Slavu, C.; Iaciu, I.C.; Popa, A.M.; Vrabie, R.C.; Nitipir, C. Does the Rechallenge with Another CDK 4/6 Inhibitor in Breast Cancer Work? A Case Report and Literature Review. Medicina 2023, 59, 696. https://doi.org/10.3390/medicina59040696
Stanciu I-M, Pirlog CF, Anghel A-W, Parosanu AI, Olaru CM, Orlov-Slavu C, Iaciu IC, Popa AM, Vrabie RC, Nitipir C. Does the Rechallenge with Another CDK 4/6 Inhibitor in Breast Cancer Work? A Case Report and Literature Review. Medicina. 2023; 59(4):696. https://doi.org/10.3390/medicina59040696
Chicago/Turabian StyleStanciu, Ioana-Miruna, Cristina Florina Pirlog, Andrei-Wilhelm Anghel, Andreea Ioana Parosanu, Cristina Mihaela Olaru, Cristina Orlov-Slavu, Ion Cristian Iaciu, Ana Maria Popa, Radu Constantin Vrabie, and Cornelia Nitipir. 2023. "Does the Rechallenge with Another CDK 4/6 Inhibitor in Breast Cancer Work? A Case Report and Literature Review" Medicina 59, no. 4: 696. https://doi.org/10.3390/medicina59040696