
Efficacy of Aceclofenac and Ilaprazole Combination Therapy versus Celecoxib Monotherapy for Treating NSAID-Induced Dyspepsia in Lumbar Spinal Stenosis Patients

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Particpants
2.3. Efficacy and Safety Evaluation
2.4. Sample Size Calculation
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Primary Efficacy Results
3.3. Secondary Efficacy Results
3.4. Safety Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, J.Y.; Song, K.S.; Cho, J.H.; Lee, J.H.; Kim, N.H. An Updated Overview of Low Back Pain Management. Asian Spine J. 2022, 16, 968–982. [Google Scholar] [CrossRef]
- Kwon, J.W.; Moon, S.H.; Park, S.Y.; Park, S.J.; Park, S.R.; Suk, K.S.; Kim, H.S.; Lee, B.H. Lumbar Spinal Stenosis: Review Update 2022. Asian Spine J. 2022, 16, 789–798. [Google Scholar] [CrossRef]
- Yap, P.R.Y.; Goh, K.L. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) Induced Dyspepsia. Curr. Pharm. Des. 2015, 21, 5073–5081. [Google Scholar] [CrossRef]
- Van Groenendael, J.H.; Markusse, H.M.; Dijkmans, B.A.; Breedveld, F.C. The effect of ranitidine on NSAID related dyspeptic symptoms with and without peptic ulcer disease of patients with rheumatoid arthritis and osteoarthritis. Clin. Rheumatol. 1996, 15, 450–456. [Google Scholar] [CrossRef]
- Bijlsma, J.W. Treatment of endoscopy-negative NSAID-induced upper gastrointestinal symptoms with cimetidine: An international multicentre collaborative study. Aliment. Pharmacol. Ther. 1988, 2 (Suppl. S1), 75–83. [Google Scholar] [CrossRef]
- Goldstein, J.L.; Eisen, G.M.; Burke, T.A.; Pena, B.M.; Lefkowith, J.; Geis, G.S. Dyspepsia tolerability from the patients’ perspective: A comparison of celecoxib with diclofenac. Aliment. Pharmacol. Ther. 2002, 16, 819–827. [Google Scholar] [CrossRef]
- McKenna, F.; Arguelles, L.; Burke, T.; Lefkowith, J.; Geis, G.S. Upper gastrointestinal tolerability of celecoxib compared with diclofenac in the treatment of osteoarthritis and rheumatoid arthritis. Clin. Exp. Rheumatol. 2002, 20, 35–43. [Google Scholar]
- Iolascon, G.; Gimenez, S.; Mogyorosi, D. A Review of Aceclofenac: Analgesic and Anti-Inflammatory Effects on Musculoskeletal Disorders. J. Pain Res. 2021, 14, 3651–3663. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, L.; Lin, S.; Hu, H.; Xia, J. A new PPI, ilaprazole compared with omeprazole in the treatment of duodenal ulcer: A randomized double-blind multicenter trial. J. Clin. Gastroenterol. 2011, 45, 322–329. [Google Scholar] [CrossRef]
- Savarino, E.; Ottonello, A.; Martinucci, I.; Dulbecco, P.; Savarino, V. Ilaprazole for the treatment of gastro-esophageal reflux. Expert Opin. Pharmacother. 2016, 17, 2107–2113. [Google Scholar] [CrossRef]
- Fraser, A.; Delaney, B.C.; Ford, A.C.; Qume, M.; Moayyedi, P. The Short-Form Leeds Dyspepsia Questionnaire validation study. Aliment. Pharm. Ther. 2007, 25, 477–486. [Google Scholar] [CrossRef]
- Ledlie, N.; Gudimetla, V. The use of Short Form 12 (SF-12) scores to assess the impact of a pre-habilitation programme. Anaesthesia 2021, 76, 151. [Google Scholar]
- Park, M.S.; Kang, C.N.; Lee, W.S.; Kim, H.J.; Lee, S.; Kim, J.H.; Shin, S.J.; Moon, S.H. A comparative study of the efficacy of NAXOZOL compared to celecoxib in patients with osteoarthritis. PLoS ONE 2020, 15, e0226184. [Google Scholar] [CrossRef] [Green Version]
- McAdam, B.F.; Catella-Lawson, F.; Mardini, I.A.; Kapoor, S.; Lawson, J.A.; FitzGerald, G.A. Systemic biosynthesis of prostacyclin by cyclooxygenase (COX)-2: The human pharmacology of a selective inhibitor of COX-2. Proc. Natl. Acad. Sci. USA 1999, 96, 272–277. [Google Scholar] [CrossRef]
- Bombardier, C.; Laine, L.; Reicin, A.; Shapiro, D.; Burgos-Vargas, R.; Davis, B.; Day, R.; Ferraz, M.B.; Hawkey, C.J.; Hochberg, M.C.; et al. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N. Engl. J. Med. 2000, 343, 1520–1528. [Google Scholar] [CrossRef]
- Silverstein, F.E.; Faich, G.; Goldstein, J.L.; Simon, L.S.; Pincus, T.; Whelton, A.; Makuch, R.; Eisen, G.; Agrawal, N.M.; Stenson, W.F.; et al. Gastrointestinal toxicity with celecoxib vs nonsteroidal anti-inflammatory drugs for osteoarthritis and rheumatoid arthritis: The CLASS study: A randomized controlled trial. Celecoxib Long-term Arthritis Safety Study. JAMA 2000, 284, 1247–1255. [Google Scholar] [CrossRef] [Green Version]
- Boers, M. NSAIDS and selective COX-2 inhibitors: Competition between gastroprotection and cardioprotection. Lancet 2001, 357, 1222–1223. [Google Scholar] [CrossRef]
- Cheng, Y.; Austin, S.C.; Rocca, B.; Koller, B.H.; Coffman, T.M.; Grosser, T.; Lawson, J.A.; FitzGerald, G.A. Role of prostacyclin in the cardiovascular response to thromboxane A2. Science 2002, 296, 539–541. [Google Scholar] [CrossRef]
- Solomon, S.D.; McMurray, J.J.; Pfeffer, M.A.; Wittes, J.; Fowler, R.; Finn, P.; Anderson, W.F.; Zauber, A.; Hawk, E.; Bertagnolli, M.; et al. Cardiovascular risk associated with celecoxib in a clinical trial for colorectal adenoma prevention. N. Engl. J. Med. 2005, 352, 1071–1080. [Google Scholar] [CrossRef] [Green Version]
- Ho, K.Y.; Kuan, A.; Zano, F.; Goh, K.L.; Mahachai, V.; Kim, D.Y.; Yoon, H.M. Randomized, parallel, double-blind comparison of the ulcer-healing effects of ilaprazole and omeprazole in the treatment of gastric and duodenal ulcers. J. Gastroenterol. 2009, 44, 697–707. [Google Scholar] [CrossRef]
- Wang, L.; Zhou, L.; Hu, H.; Lin, S.; Xia, J. Ilaprazole for the treatment of duodenal ulcer: A randomized, double-blind and controlled phase III trial. Curr. Med. Res. Opin. 2012, 28, 101–109. [Google Scholar] [CrossRef]
- Ji, X.Q.; Du, J.F.; Chen, G.; Chen, G.; Yu, B. Efficacy of ilaprazole in the treatment of duodenal ulcers: A meta-analysis. World J. Gastroenterol. 2014, 20, 5119–5123. [Google Scholar] [CrossRef]
- Shin, J.S.; Lee, J.Y.; Cho, K.H.; Park, H.L.; Kukulka, M.; Wu, J.T.; Kim, D.Y.; Park, S.H. The pharmacokinetics, pharmacodynamics and safety of oral doses of ilaprazole 10, 20 and 40 mg and esomeprazole 40 mg in healthy subjects: A randomised, open-label crossover study. Aliment. Pharmacol. Ther. 2014, 40, 548–561. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Aceclofenac + Ilaprazole n = 64 | Celecoxib n = 64 | p-Value | |
|---|---|---|---|
| Age (years) | 67.6 ± 8.4 | 67.2 ± 8.3 | 0.792 |
| Sex (No.) | 0.465 | ||
| Female | 42 (65.6%) | 38 (59.4%) | |
| Male | 22 (34.4%) | 26 (40.6%) | |
| Height, cm | 156.35 ± 8.35 | 158.01 ± 8.54 | 0.237 |
| Weight, kg | 61.97 ± 9.53 | 63.52 ± 9.75 | 0.410 |
| SF-LDQ a (initial) | 3.03 ± 4.57 | 2.91 ± 4.19 | 0.872 |
| SF-12 b (initial) | |||
| PCS c | 39.01 ± 7.34 | 38.54 ± 8.83 | 0.694 |
| MCS d | 46.89 ± 9.81 | 48.36 ± 10.70 | 0.421 |
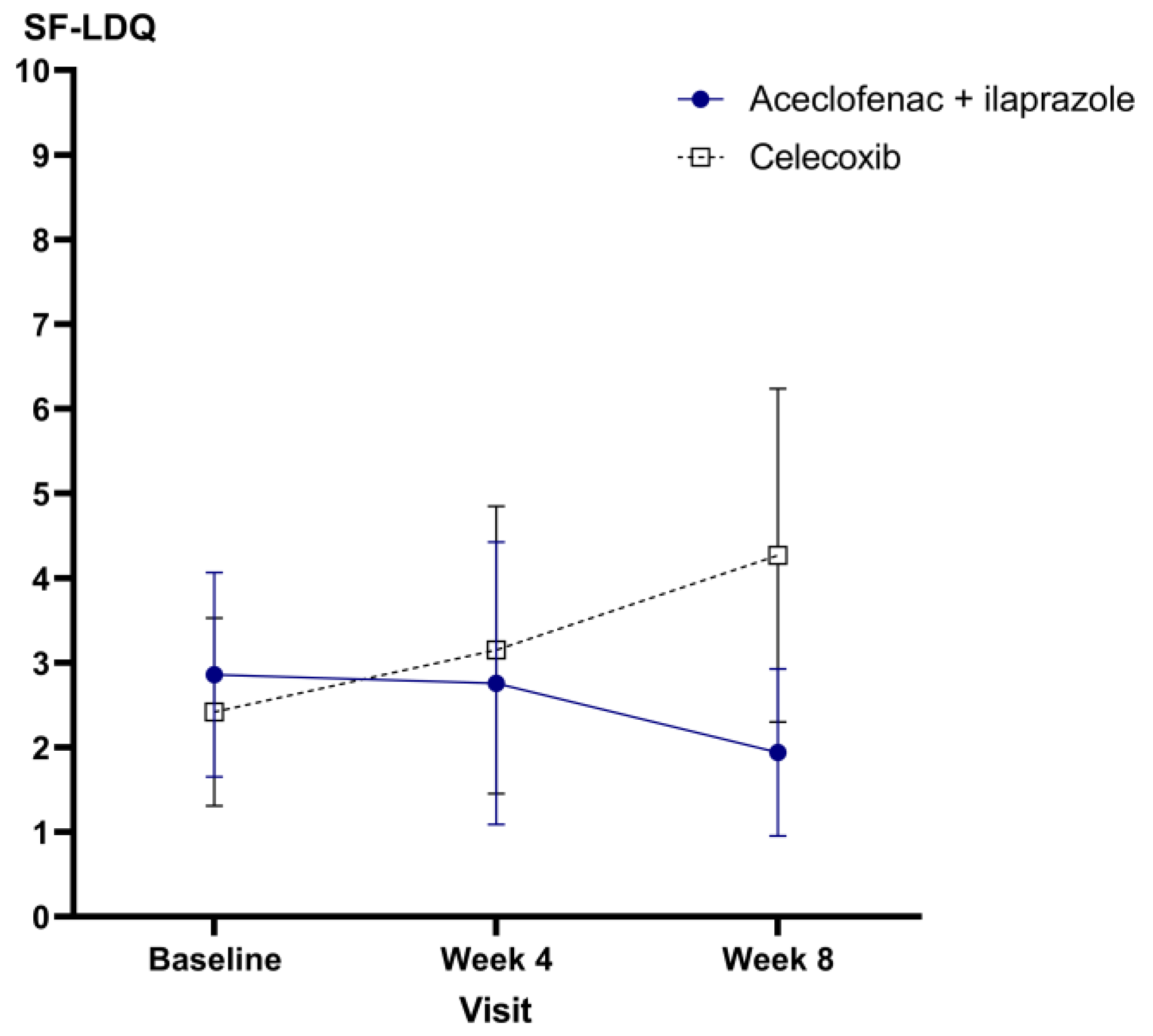
| Aceclofenac + Ilaprazole | Celecoxib | p-Value | |
|---|---|---|---|
| Full analysis set | |||
| Baseline | 2.76 ± 4.06 | 2.89 ± 4.21 | 0.866 |
| Week 4 | 2.84 ± 5.71 | 4.61 ± 8.06 | 0.162 |
| Week 8 | 2.88 ± 4.93 | 4.27 ± 7.07 | 0.234 |
| Difference (Week 8—Baseline) | 0.13 ± 5.30 | 1.85 ± 6.70 | 0.140 |
| Per protocol set | |||
| Baseline | 2.86 ± 4.29 | 2.42 ± 3.99 | 0.580 |
| Week 4 | 2.76 ± 5.93 | 3.15 ± 6.10 | 0.493 |
| Week 8 | 1.94 ± 3.51 | 4.27 ± 7.07 | 0.286 |
| Difference (Week 8—Baseline) | −0.51 ± 4.78 | 1.85 ± 6.70 | 0.054 |
| Aceclofenac + Ilaprazole | Celecoxib | p-Value | |
|---|---|---|---|
| Full analysis set | |||
| PCS a | |||
| Baseline | 39.01 ± 7.36 | 38.71 ± 8.91 | |
| Week 4 | 41.05 ± 7.78 | 41.13 ± 9.22 | |
| Week 8 | 41.13 ± 9.34 | 40.19 ± 9.39 | |
| Difference (Week 8—Baseline) | 2.54 ± 8.34 | 1.16 ± 10.78 | 0.457 |
| MCS b | |||
| Baseline | 47.04 ± 9.82 | 48.34 ± 10.84 | |
| Week 4 | 47.47 ± 10.08 | 48.57 ± 10.42 | |
| Week 8 | 48.81 ± 11.06 | 50.20 ± 10.32 | |
| Difference (Week 8—Baseline) | 1.51 ± 12.10 | 0.37 ± 9.55 | 0.589 |
| Per protocol set | |||
| PCS a | |||
| Baseline | 38.99 ± 7.08 | 39.03 ± 9.43 | |
| Week 4 | 41.36 ± 7.62 | 41.01 ± 9.65 | |
| Week 8 | 42.09 ± 9.21 | 40.19 ± 9.39 | |
| Difference (Week 8—Baseline) | 3.10 ± 8.38 | 1.16 ± 10.78 | 0.310 |
| MCS b | |||
| Baseline | 47.48 ± 9.73 | 49.83 ± 10.43 | |
| Week 4 | 48.35 ± 9.45 | 50.38 ± 9.50 | |
| Week 8 | 48.98 ± 11.08 | 50.20 ± 10.32 | |
| Difference (Week 8—Baseline) | 1.49 ± 11.92 | 0.37 ± 9.55 | 0.597 |
| Aceclofenac + Ilaprazole n = 64 | Celecoxib n = 64 | p-Value | |
|---|---|---|---|
| Incidence of adverse events | 7 (10.9%) | 6 (9.4%) | 0.770 |
| GI trouble | 3 | 4 | |
| Swelling | 3 | 0 | |
| Redness | 0 | 1 | |
| Dehydration | 1 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Kim, J.G.; Kim, H.-J. Efficacy of Aceclofenac and Ilaprazole Combination Therapy versus Celecoxib Monotherapy for Treating NSAID-Induced Dyspepsia in Lumbar Spinal Stenosis Patients. Medicina 2023, 59, 1307. https://doi.org/10.3390/medicina59071307
Lee S, Kim JG, Kim H-J. Efficacy of Aceclofenac and Ilaprazole Combination Therapy versus Celecoxib Monotherapy for Treating NSAID-Induced Dyspepsia in Lumbar Spinal Stenosis Patients. Medicina. 2023; 59(7):1307. https://doi.org/10.3390/medicina59071307
Chicago/Turabian StyleLee, Sanghoon, Jung Guel Kim, and Ho-Joong Kim. 2023. "Efficacy of Aceclofenac and Ilaprazole Combination Therapy versus Celecoxib Monotherapy for Treating NSAID-Induced Dyspepsia in Lumbar Spinal Stenosis Patients" Medicina 59, no. 7: 1307. https://doi.org/10.3390/medicina59071307