
Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
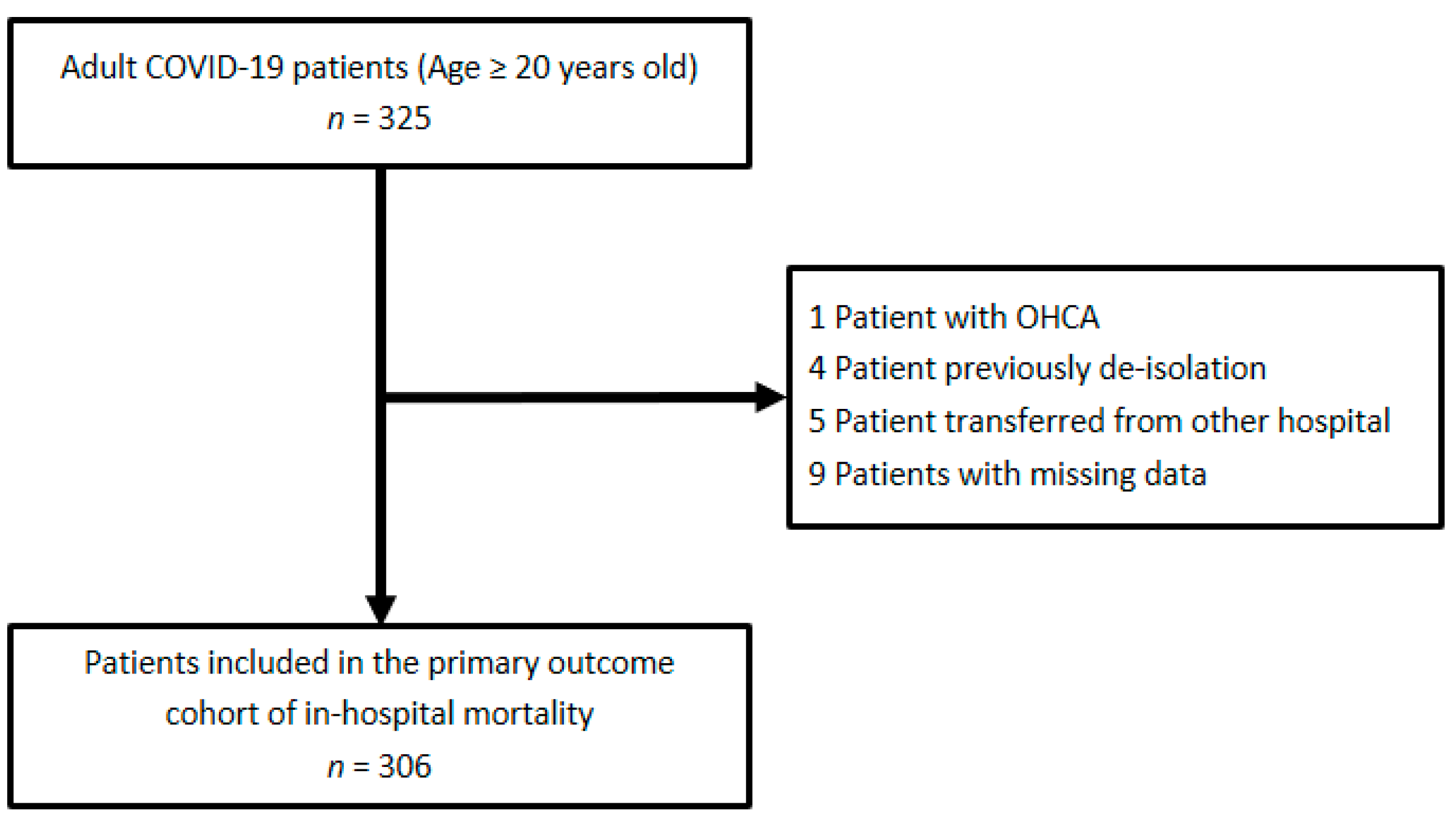
2.2. Study Population
2.3. Variables
2.4. Outcomes
2.5. Statistical Analyses
2.6. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Kramer, A.A.; Sebat, F.; Lissauer, M. A review of early warning systems for prompt detection of patients at risk for clinical decline. J. Trauma Acute Care Surg. 2019, 87, S67–S73. [Google Scholar] [CrossRef]
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.B.; Prytherch, D.R.; Meredith, P.; Schmidt, P.E.; Featherstone, P.I. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013, 84, 465–470. [Google Scholar] [CrossRef]
- Olsson, T.; Terent, A.; Lind, L. Rapid Emergency Medicine score: A new prognostic tool for in-hospital mortality in nonsurgical emergency department patients. J. Intern. Med. 2004, 255, 579–587. [Google Scholar] [CrossRef]
- Chen, T.-H.; Chi, W.-Y.; Yang, S.-Y.; Liao, C.-H.; Tsai, Y.-L.; Chang, W.-H.; Tsai, W. The role of quarantine ward in the COVID-era: A Taiwan medical center experience. Health Technol. 2021, 5, 9. [Google Scholar] [CrossRef]
- Liao, C.-H.; Tsai, Y.-L.; Chen, T.-H.; Chi, W.-Y.; Yang, S.-Y.; Chang, W.-H.; Tsai, W. Staying connected in the COVID-19 pandemic: A medical center’s experience to synchronize information across two branches of emergency department to enhance communication. Health Technol. 2021, 5, 16. [Google Scholar] [CrossRef]
- Tsai, Y.-L.; Chen, T.-H.; Chi, W.-Y.; Yang, S.-Y.; Liao, C.-H.; Chang, W.-H.; Tsai, W. Screening unit during coronavirus disease 2019 pandemic: A review of current evidence and experience of a medical center in Taiwan. Health Technol. 2021, 5, 7. [Google Scholar] [CrossRef]
- Chen, T.-H.; Chen, C.; Jo, S.-Y.; Hsiao, C.-H.; Tsai, W.; Chang, W.-H.; Chien, D.-K. Discriminant Ability of In-Hospital Mortality Based on Prognostic Scores of Elderly Patients with COVID-19: A Taiwan Medical Center Study. Int. J. Gerontol. 2022, 16, 202–206. [Google Scholar] [CrossRef]
- Chen, T.H.; Huang, M.Y.; Hsiao, C.H.; Chien, D.K.; Tsai, W. Performance evaluation of Panbio(TM) COVID-19 rapid antigen test for SARS-CoV-2 detection in a low prevalence cohort. Infect. Dis. 2022, 54, 944–946. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): Explanation and elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Hu, H.; Yao, N.; Qiu, Y. Comparing Rapid Scoring Systems in Mortality Prediction of Critically Ill Patients with Novel Coronavirus Disease. Acad. Emerg. Med. 2020, 27, 461–468. [Google Scholar] [CrossRef] [Green Version]
- Bourn, S.S.; Crowe, R.P.; Fernandez, A.R.; Matt, S.E.; Brown, A.L.; Hawthorn, A.B.; Myers, J.B. Initial prehospital Rapid Emergency Medicine Score (REMS) to predict outcomes for COVID-19 patients. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12483. [Google Scholar] [CrossRef] [PubMed]
- Pokeerbux, M.R.; Yelnik, C.M.; Faure, E.; Drumez, E.; Bruandet, A.; Labreuche, J.; Assaf, A.; Goffard, A.; Garabedian, C.; Poissy, J.; et al. National early warning score to predict intensive care unit transfer and mortality in COVID-19 in a French cohort. Int. J. Clin. Pract. 2021, 75, e14121. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir, S.; Algin, A.; Akca, H.S.; Altunok, I.; Kokulu, K.; Eroglu, S.E.; Aksel, G. Predictive Ability of the MEWS, REMS, and RAPS in Geriatric Patients With SARS-CoV-2 Infection in the Emergency Department. Disaster Med. Public Health Prep. 2023, 17, e174. [Google Scholar] [CrossRef]
- Wang, L.; Lv, Q.; Zhang, X.; Jiang, B.; Liu, E.; Xiao, C.; Yu, X.; Yang, C.; Chen, L. The utility of MEWS for predicting the mortality in the elderly adults with COVID-19: A retrospective cohort study with comparison to other predictive clinical scores. PeerJ 2020, 8, e10018. [Google Scholar] [CrossRef]
- Aygun, H.; Eraybar, S. The role of emergency department triage early warning score (TREWS) and modified early warning score (MEWS) to predict in-hospital mortality in COVID-19 patients. Ir. J. Med. Sci. 2022, 191, 997–1003. [Google Scholar] [CrossRef]
- Croft, C.A.; Moore, F.A.; Efron, P.A.; Marker, P.S.; Gabrielli, A.; Westhoff, L.S.; Lottenberg, L.; Jordan, J.; Klink, V.; Sailors, R.M.; et al. Computer versus paper system for recognition and management of sepsis in surgical intensive care. J. Trauma Acute Care Surg. 2014, 76, 311–317; discussion 318–319. [Google Scholar] [CrossRef]
- Wibisono, E.; Hadi, U.; Bramantono; Arfijanto, M.V.; Rusli, M.; Rahman, B.E.; Asmarawati, T.P.; Choirunnisa, M.L.; Rahayu, D.R.P. National early warning score (NEWS) 2 predicts hospital mortality from COVID-19 patients. Ann. Med. Surg. 2022, 76, 103462. [Google Scholar] [CrossRef]
- Chen, Y.; Klein, S.L.; Garibaldi, B.T.; Li, H.; Wu, C.; Osevala, N.M.; Li, T.; Margolick, J.B.; Pawelec, G.; Leng, S.X. Aging in COVID-19: Vulnerability, immunity and intervention. Ageing Res. Rev. 2021, 65, 101205. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 4 | 3 | 2 | 1 | 0 | 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Modified Early Warning Score (MEWS) | |||||||||||
| SBP (mmHg) | ≤70 | 71–80 | 81–100 | 101–199 | ≥200 | ||||||
| HR (bpm) | <40 | 41–50 | 51–100 | 101–110 | 111–129 | ≥130 | |||||
| RR (bpm) | <9 | 9–14 | 15–20 | 21–29 | ≥30 | ||||||
| BT (‘C) | <35 | 35–38.4 | ≥38.5 | ||||||||
| AVPU | A | V | P | U | |||||||
| National Early Warning Score (NEWS) | |||||||||||
| RR (bpm) | ≤8 | 9–11 | 12–20 | 21–24 | ≥25 | ||||||
| SpO2 (%) | ≤91 | 92–93 | 94–95 | ≥96 | |||||||
| Oxygen supple | No | Yes | |||||||||
| BT (°C) | ≤35 | 35.1–36 | 36.1–38 | 38.1–39 | ≥39.1 | ||||||
| SBP (mmHg) | ≤90 | 91–100 | 101–110 | 111–219 | ≥220 | ||||||
| HR (bpm) | ≤40 | 41–50 | 51–90 | 91–110 | 111–130 | ≥131 | |||||
| AVPU | A | V, P, U | |||||||||
| Rapid Emergency Medicine Score (REMS) | |||||||||||
| Age | <45 | 45–54 | 55–64 | 65–74 | >74 | ||||||
| MAP (mmHg) | ≤ 49 | 50–69 | 70–109 | 110–129 | 130–159 | >159 | |||||
| HR (bpm) | ≤ 39 | 40–54 | 55–69 | 70–109 | 110–139 | 140–179 | >179 | ||||
| RR (bpm) | ≤ 5 | 6–9 | 10–11 | 12–24 | 25–34 | 35–49 | >49 | ||||
| SpO2 (%) | <75 | 75–85 | 86–89 | >89 | |||||||
| GCS | <5 | 5–7 | 8–10 | 11–13 | >13 | ||||||
| All Patients (n = 306) | Non-Survivors (n = 35) | Survivors (n = 271) | p Value | |
|---|---|---|---|---|
| Basic characteristics | ||||
| Age | 61.07 ± 15.12 | 69.74 ± 10.18 | 59.87 ± 15.23 | <0.05 |
| Sex | 52.90% | 65.71% | 51.15% | <0.05 |
| Medical history | ||||
| HTN | 34% | 60% | 31% | <0.05 |
| DM | 26% | 43% | 23% | <0.05 |
| CAD | 10% | 26% | 8% | <0.05 |
| HF | 3% | 11% | 2% | <0.05 |
| CKD | 9% | 40% | 5% | <0.05 |
| Vital signs (mean ± SD) | ||||
| GCS | 14.57 ± 1.82 | 13.83 ± 2.99 | 14.65 ± 1.63 | <0.05 |
| BT | 37.38 ± 1.77 | 37.70 ± 1.06 | 37.33 ± 1.86 | 0.25 |
| HR | 93.17 ± 20.65 | 103.23 ± 21.70 | 92.09 ± 19.98 | <0.05 |
| RR | 20.16 ± 7.14 | 21.86 ± 5.17 | 19.59 ± 4.48 | <0.05 |
| SBP | 129.99 ± 24.78 | 139.46 ± 30.64 | 128.79 ± 23.62 | <0.05 |
| DBP | 75.25 ± 13.33 | 75.94 ± 15.17 | 75.30 ± 13.03 | 0.789 |
| MAP | 93.50 ± 15.32 | 93.13 ± 14.69 | 97.11 ± 18.98 | 0.148 |
| SpO2 | 94.64 ± 7.99 | 88.60 ± 13.78 | 95.42 ± 6.40 | <0.05 |
| Emergency warning scores (mean ± SD) | ||||
| REMS | 5.32 ± 3.67 | 8.46 ± 3.97 | 4.87 ± 3.32 | <0.05 |
| NEWS | 3.56 ± 3.11 | 6.06 ± 3.79 | 3.25 ± 2.81 | <0.05 |
| MEWS | 2.51 ± 1.91 | 3.49 ± 1.98 | 2.22 ± 1.47 | <0.05 |
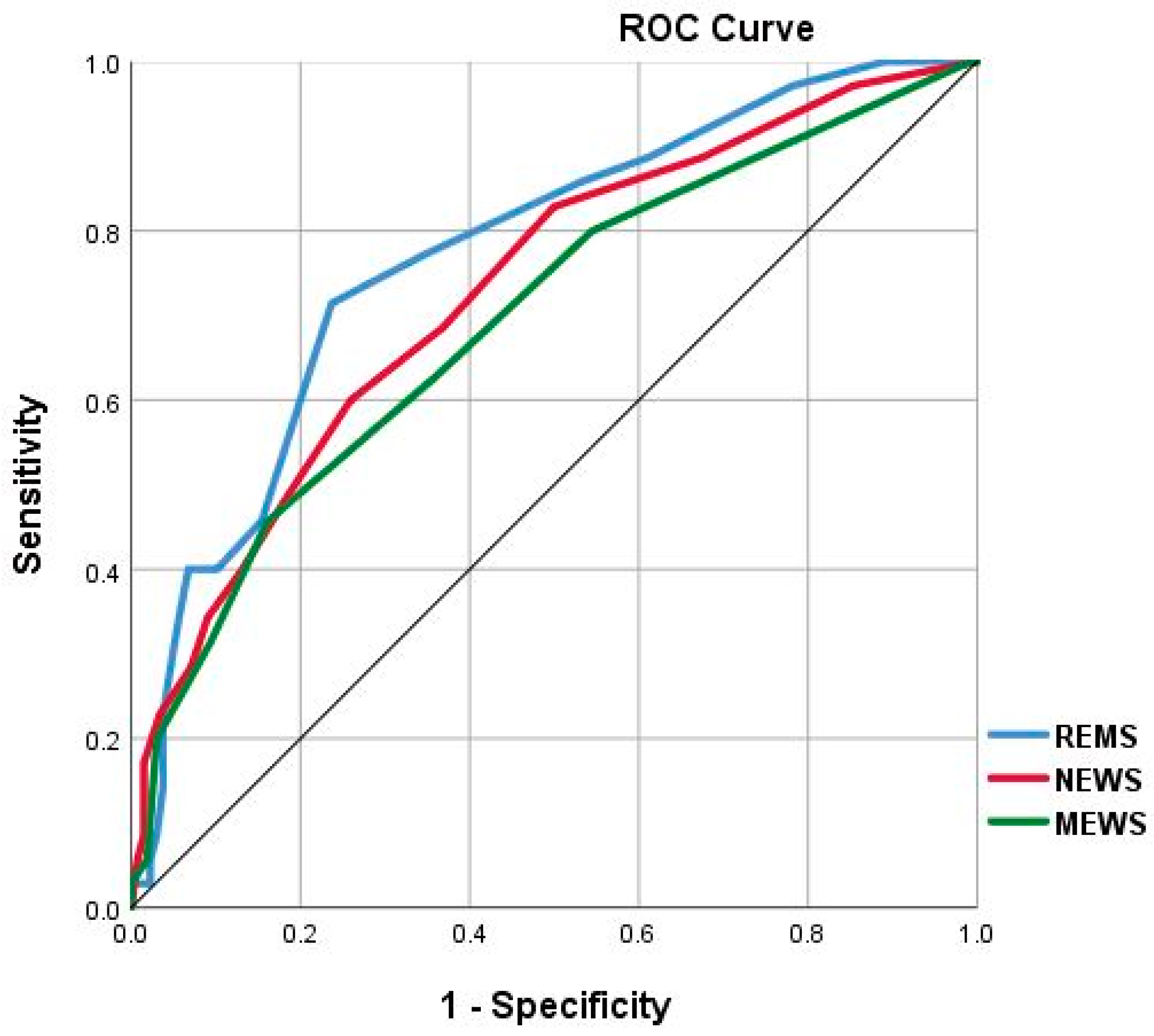
| Score | AUC | 95% CI | p Value | Cutoff Value | Sensitivity | Specificity | PPV | NPV | PLR | NLR |
|---|---|---|---|---|---|---|---|---|---|---|
| REMS | 0.773 | 0.692–0.854 | <0.05 | > 6.5 | 71.4% | 76.3% | 27.9% | 95.4% | 3.01 | 0.37 |
| NEWS | 0.730 | 0.639–0.820 | <0.05 | > 4.5 | 60.0% | 74.1% | 23.0% | 93.5% | 2.32 | 0.54 |
| MEWS | 0.695 | 0.597–0.792 | <0.05 | > 3.5 | 45.7% | 83.8% | 26.6% | 92.3% | 2.82 | 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, W.; Chen, C.; Jo, S.-Y.; Hsiao, C.-H.; Chien, D.-K.; Chang, W.-H.; Chen, T.-H. Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan. Medicina 2023, 59, 464. https://doi.org/10.3390/medicina59030464
Tsai W, Chen C, Jo S-Y, Hsiao C-H, Chien D-K, Chang W-H, Chen T-H. Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan. Medicina. 2023; 59(3):464. https://doi.org/10.3390/medicina59030464
Chicago/Turabian StyleTsai, Weide, Chun Chen, Szu-Yang Jo, Chien-Han Hsiao, Ding-Kuo Chien, Wen-Han Chang, and Tse-Hao Chen. 2023. "Evaluation of Early Warning Scores on In-Hospital Mortality in COVID-19 Patients: A Tertiary Hospital Study from Taiwan" Medicina 59, no. 3: 464. https://doi.org/10.3390/medicina59030464