
Post-COVID-19 Spondylodiscitis: A Case Study and Review of the Literature

Abstract
:1. Introduction
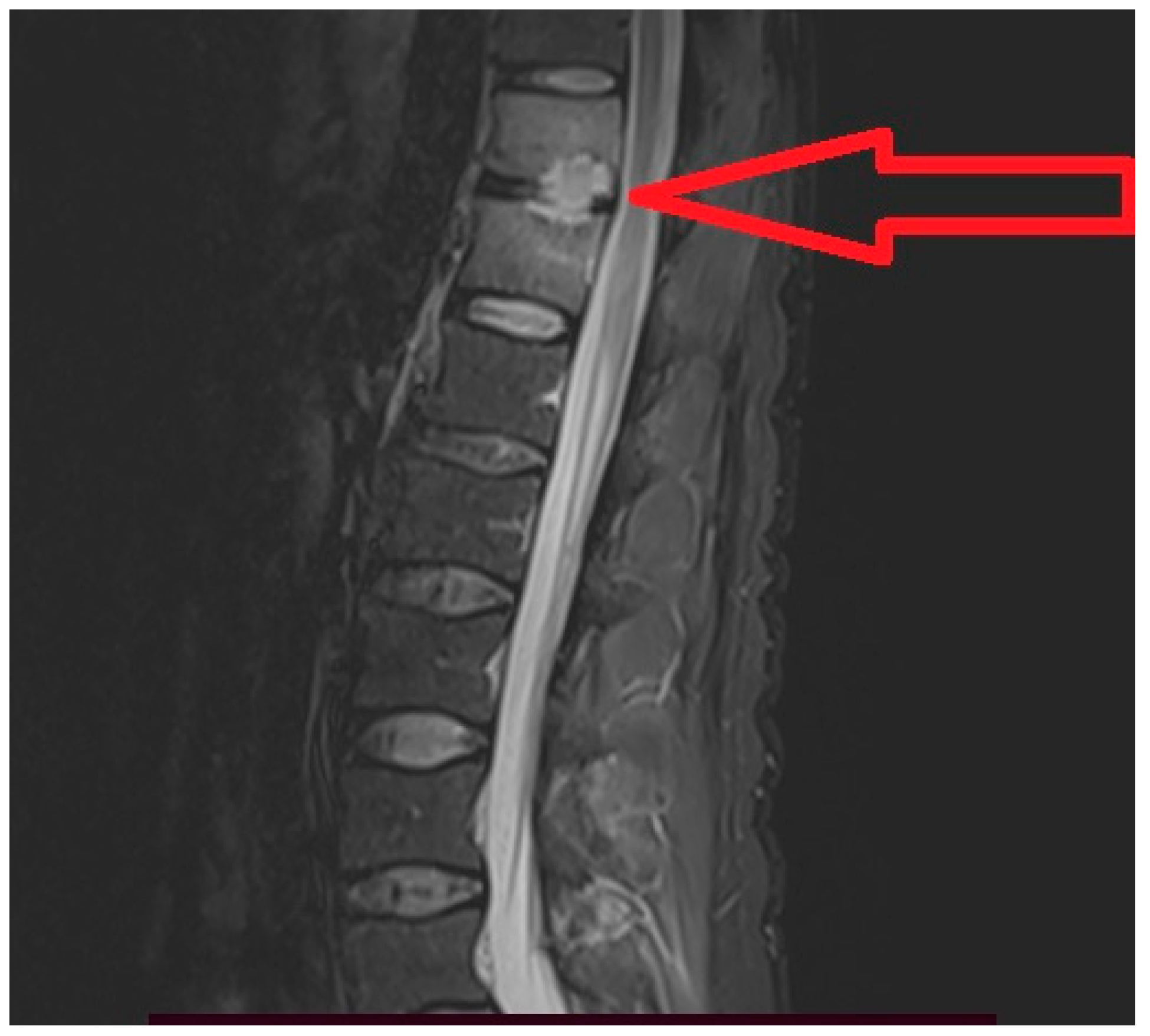
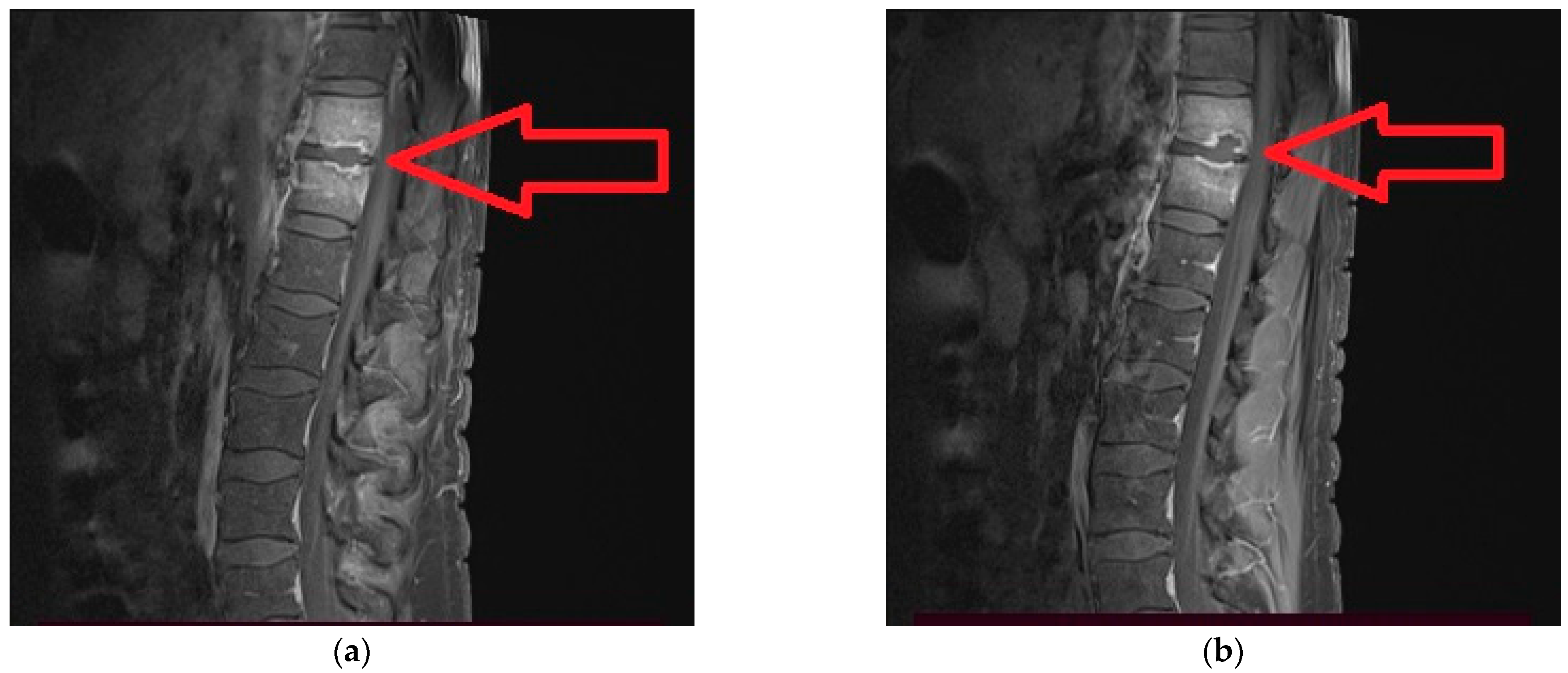
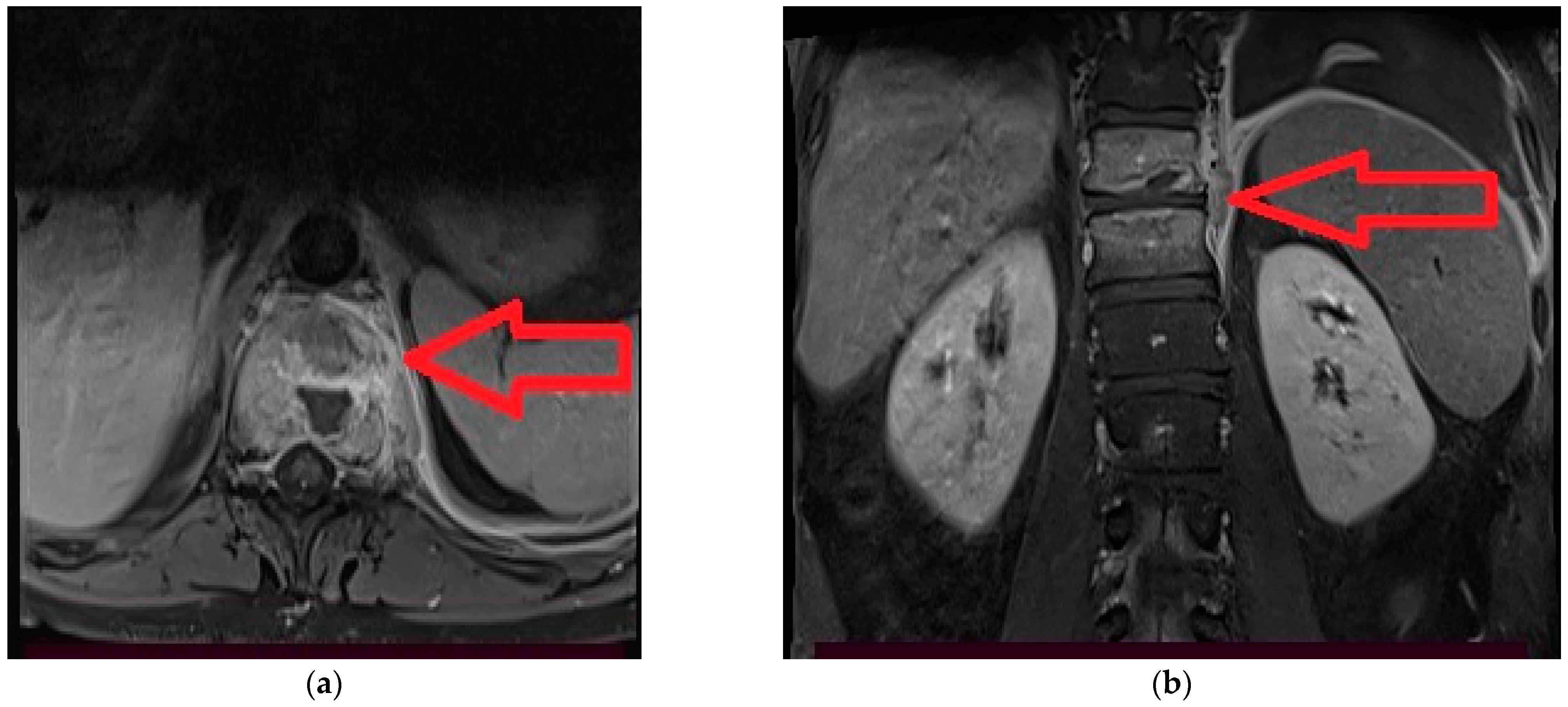
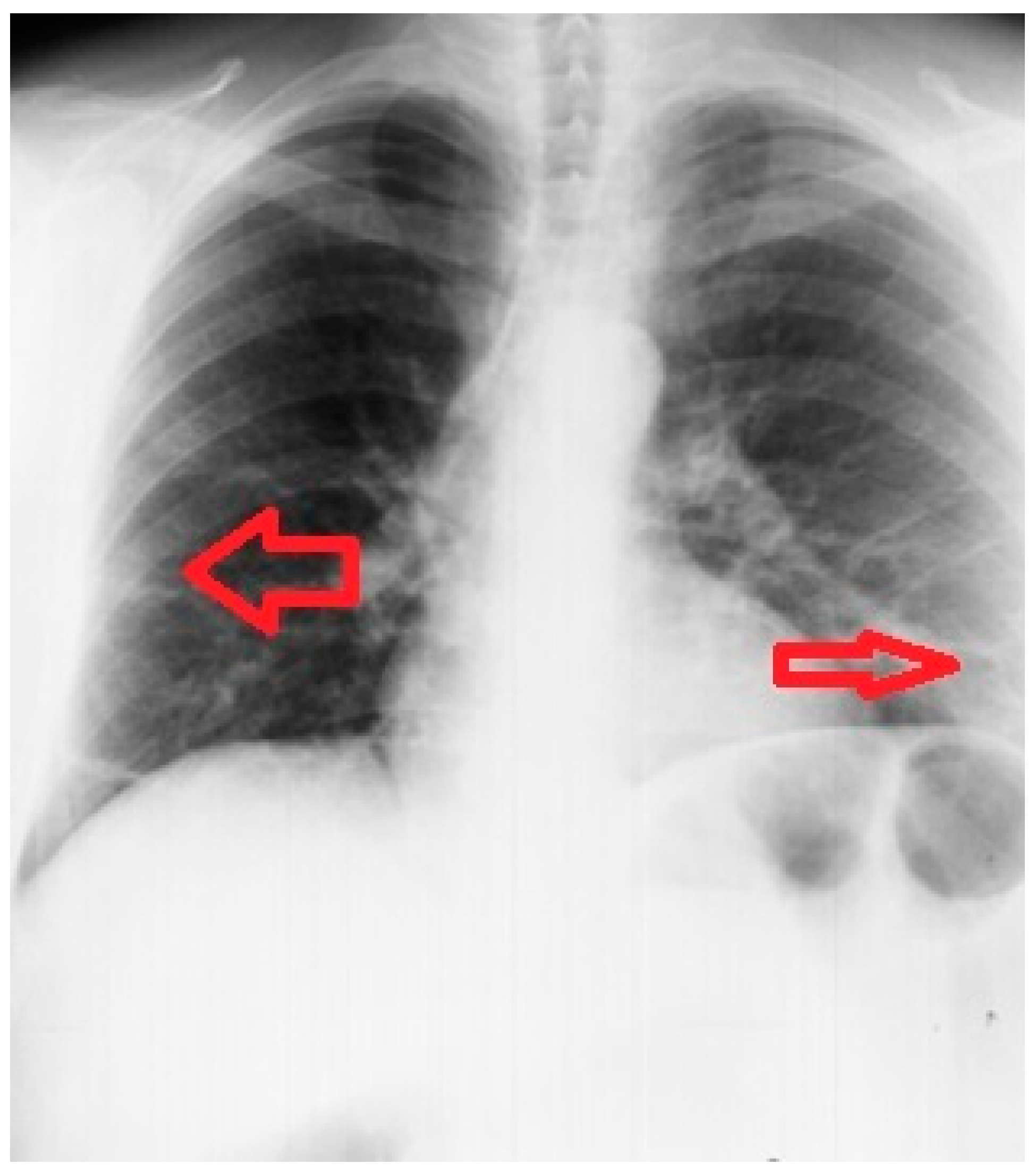
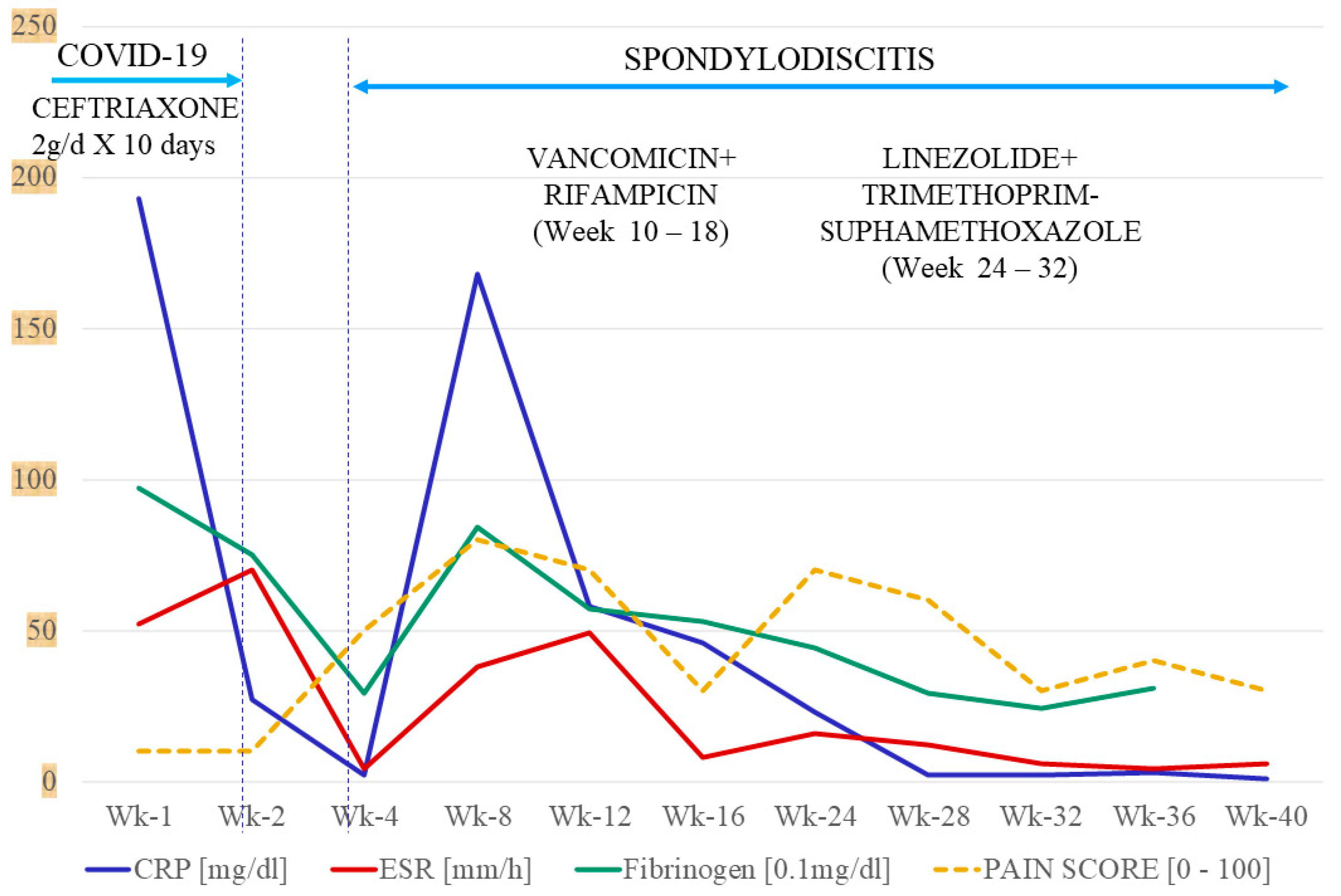
2. Case Report
3. Discussion
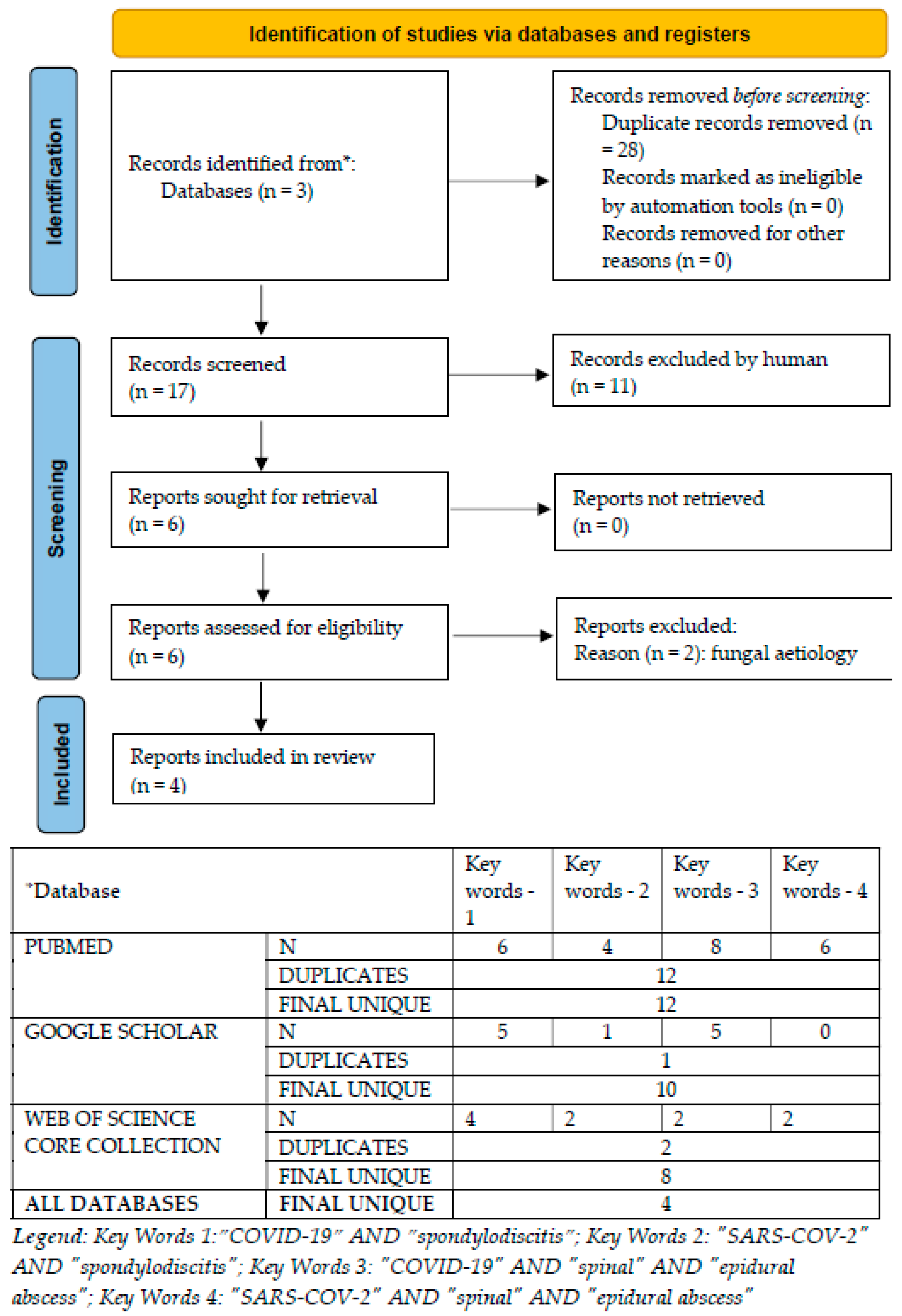
3.1. Systematic Review of Medical Databases
3.2. Particularities of the Reported Case
3.3. Hypothesis of the Linkage between COVID-19 and Spondylodiscitis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Tests | NRV | H-Day1 | H-Day2 | H-Day7 | H-Day 11 |
|---|---|---|---|---|---|
| ALT [U/L] | 0–50 | 119 | 95 | 289 | 307 |
| AST [U/L] | 14–59 | 98 | 48 | 151 | 72 |
| CK [U/L] | 30–170 | 43 | 27 | 29 | 24 |
| CREATININE [mg/dL] | 0.5–1.25 | 0.98 | 0.81 | 0.95 | 0.85 |
| UREA [mg/dL] | 15/42.9 | 43 | 33.3 | 39.2 | 39.6 |
| GLUCOSE [mg/dL] | 74/106 | 103 | 92 | 67 | 83 |
| LDH [U/L] | 313/618 U/L | 197 | 300 | 236 | |
| CRP [mg/dL] | 0–1 | 193 | 27 | 7 | |
| ESR [mm/h] | 2–10 | 52 | 70 | 18 | |
| Ferritin [ng/mL] | 17.9–464 | 1170 | |||
| FIBRINOGEN [mg/dL] | 200–400 | 967 | 753 | 461 | |
| LEUKOCYTES [/µL] | 4000–10,000 | 16,700 | 16,400 | 10,000 | 12,000 |
| NEUTROPHIL [/µL] | 2000–7000 | 15480.9 | 15793.2 | 8610 | 9180 |
| LYMPHOCYTE [/µL] | 700–5000 | 467.6 | 300.07 | 880 | 1200 |
| Ratio N/Ly | 1–3 | 33.10 | 52.63 | 9.78 | 7.65 |
| Blood Tests | NRV | Wk-4 | Wk-6 | Wk-8 | Wk-10 | Wk-12 | Wk-18 | Wk-24 | Wk-26 | Wk-28 | Wk-32 | Wk-36 | Wk-40 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ALT [U/L] | 0–50 | 419 | 91 | 45 | 157 | 31 | 19 | 17 | 110 | 31 | 29 | ||
| AST [U/L] | 14–59 | 118 | 34 | 27 | 45 | 17 | 15 | 15 | 39 | 22 | 20 | ||
| CK [U/L] | 30–170 | 48 | 29 | 53 | 97 | 142 | 86 | 149 | |||||
| CREATININE [mg/dL] | 0.5–1.25 | 1.05 | 0.88 | 0.82 | 0.98 | 0.92 | 1.15 | 0.92 | 0.99 | 1.02 | |||
| UREA [mg/dL] | 15/42.9 | 36 | 33 | 22 | 27 | 30 | 32 | 35 | 37 | 36 | |||
| GLUCOSE [mg/dL] | 74/106 | 103 | 89 | 92 | 92 | 107 | 99 | 86 | 96 | 102 | 92 | ||
| LDH [U/L] | 313/618 U/L | 482 | 326 | 551 | 236 | 220 | 349 | 310 | 323 | 388 | |||
| CRP [mg/dL] | 0–1 | 2 | 168 | 34 | 52 | 46 | 22 | 16.8 | 3.24 | 1.07 | |||
| ESR [mm/h] | 2–10 | 4 | 5 | 38 | 52 | 49 | 4 | 8 | 16 | 6 | 4 | 6 | |
| Ferritin [ng/mL] | 17.9–464 | 713 | 545 | 331 | 249 | 199 | 164 | 306 | 136 | 106 | |||
| FIBRINOGEN [mg/dL] | 200–400 | 287 | 967 | 842 | 720 | 562 | 264 | 532 | 436 | 290 | 235 | 308 | |
| LEUKOCYTES [/µL] | 4000–10,000 | 3900 | 10,540 | 20550 | 12,000 | 7300 | 4200 | 7800 | 6600 | 9800 | 6000 | 4600 | 5300 |
| NEUTROPHIL [/µL] | 2000–7000 | 2300 | 7910 | 17520 | 9180 | 5730 | 2580 | 6290 | 5030 | 7830 | 4770 | 3100 | 3500 |
| LYMPHOCYTE [/µL] | 700–5000 | 880 | 1460 | 1550 | 1200 | 1050 | 1140 | 1000 | 1010 | 1240 | 780 | 1110 | 1300 |
| Ratio N/Ly | 1–3 | 2.61 | 5.41 | 11.30 | 7.65 | 5.45 | 2.26 | 6.29 | 4.98 | 6.31 | 6.11 | 2.79 | 2.69 |

References
- World Health Organization. Clinical Management of COVID-19: Living Guideline, 15 September Geneva: World Health Organization; 2022 (WHO/2019-nCoV/Clinical/2022.2). Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2023.1 (accessed on 24 February 2023).
- Carsana, L.; Sonzogni, A.; Nasr, A.; Rossi, R.S.; Pellegrinelli, A.; Zerbi, P.; Rech, R.; Colombo, R.; Antinori, S.; Corbellino, M.; et al. Pulmonary post-mortem findings in a series of COVID-19 cases from northern Italy: A two-centre descriptive study. Lancet Infect. Dis. 2020, 20, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Geng, X.; Tan, Y.; Li, Q.; Xu, C.; Xu, J.; Hao, L.; Zeng, Z.; Luo, X.; Liu, F.; et al. New understanding of the damage of SARS-CoV-2 infection outside the respiratory system. Biomed. Pharmacother. 2020, 127, 110195. [Google Scholar] [CrossRef] [PubMed]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.-D.; Sacco, C.; Bertuzzi, A.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus disease 2019 in elderly patients: Characteristics and prognostic factors based on 4-week follow-up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef]
- Vasile, M.-C.; Arbune, A.-A.; Lupasteanu, G.; Vlase, C.-M.; Popovici, G.-C.; Arbune, M. Epidemiologic and Clinic Characteristics of the First Wave of the COVID-19 Pandemic in Hospitalized Patients from Galați County. J. Clin. Med. 2021, 10, 4210. [Google Scholar] [CrossRef]
- Centers for Diseases Control and Prevention. The novel coronavirus pneumonia emergency response epidemiology team: Vital Surveillances: The epidemiological characteristcs of an outbreak of 2019 Novel Coronavirus diseases (COVID-19)-China. China CDC Weekly 2020, 2, 113–122.u. [Google Scholar]
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospectve cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef] [PubMed]
- Yelin, D.; Moschopoulos, C.D.; Margalit, I.; Gkrania-Klotsas, E.; Landi, F.; Stahl, J.-P.; Yahav, D. ESCMID rapid guidelines for assessment and management of long COVID. Clin. Microbiol. Infect. 2022, 28, 955–972. [Google Scholar] [CrossRef]
- Sur, A.; Tsang, K.; Brown, M.; Tzerakis, N. Management of adult spontaneous spondylodiscitis and its rising incidence. Ind. Mark. Manag. 2015, 97, 451–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lener, S.; Hartmann, S.; Barbagallo, G.M.V.; Certo, F.; Thomé, C.; Tschugg, A. Management of spinal infection: A review of the literature. Acta Neurochir. 2018, 160, 487–496. [Google Scholar] [CrossRef] [Green Version]
- Mavrogenis, A.F.; Megaloikonomos, P.D.; Igoumenou, V.G.; Panagopoulos, G.N.; Giannitsioti, E.; Papadopoulos, A.; Papagelopoulos, P.J. Spondylodiscitis revisited. EFORT Open Rev. 2017, 2, 447–461. [Google Scholar] [CrossRef]
- Herren, C.; Jung, N.; Pishnamaz, M.; Breuninger, M.; Siewe, J.; Sobottke, R. Spondylodiscitis: Diagnosis and Treatment Options. Dtsch. Arztebl. Int. 2017, 114, 875–882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petkova, A.S.; Zhelyazkov, C.B.; Kitov, B.D. Spontaneous Spondylodiscitis—Epidemiology, Clinical Features, Diagnosis and Treatment. Folia Medica 2017, 59, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pojskić, M.; Carl, B.; Schmöckel, V.; Völlger, B.; Nimsky, C.; Saβ, B. Neurosurgical Management and Outcome Parameters in 237 Patients with Spondylodiscitis. Brain Sci. 2021, 11, 1019. [Google Scholar] [CrossRef] [PubMed]
- Homagk, L.; Marmelstein, D.; Homagk, N.; Hofmann, G.O. SponDT (Spondylodiscitis Diagnosis and Treatment): Spondylodiscitis scoring system. J. Orthop. Surg. Res. 2019, 14, 100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsantes, A.G.; Papadopoulos, D.V.; Vrioni, G.; Sioutis, S.; Sapkas, G.; Benzakour, A.; Benzakour, T.; Angelini, A.; Ruggieri, P.; Mavrogenis, A.F.; et al. Spinal Infections: An Update. Microorganisms 2020, 8, 476. [Google Scholar] [CrossRef] [Green Version]
- Başak, A.T.; Çakıcı, N.; Özbek, M.A.; Hekimoğlu, M.; Çerezci, Ç.; Ates, O.; Oktenoglu, T.; Sasani, M.; Özer, A.F. A Combined Diagnosis and Treatment Algorithm for Spine Infection Management: A Single-Center Experience. Cureus 2022, 14, e28251. [Google Scholar] [CrossRef] [PubMed]
- Algrmi, S.E.A.; Youssef, M.M.M.T.; Fattah, I.M.A.; Elsayed, E.M. Management of Patients with Spondylodiscitis: An Overview. Eur. J. Mol. Clin. Med. 2021, 8, 3023–3034. [Google Scholar]
- Lazzeri, E.; Bozzao, A.; Cataldo, M.A.; Petrosillo, N.; Manfrè, L.; Trampuz, A.; Signore, A.; Muto, M. Joint EANM/ESNR and ESCMID-endorsed consensus document for the diagnosis of spine infection (spondylodiscitis) in adults. Eur. J. Nucl. Med. 2019, 46, 2464–2487. [Google Scholar] [CrossRef]
- Van Gerven, C.; Eid, K.; Krüger, T.; Fell, M.; Kendoff, D.; Friedrich, M.; Kraft, C.N. Serum C-reactive protein and WBC count in conservatively and operatively managed bacterial spondylodiscitis. J. Orthop. Surg. 2021, 29, 1–8. [Google Scholar] [CrossRef]
- Sharfman, Z.T.; Gelfand, Y.; Shah, P.; Holtzman, A.J.; Mendelis, J.R.; Kinon, M.D.; Krystal, J.D.; Brook, A.; Yassari, R.; Kramer, D.C. Spinal Epidural Abscess: A Review of Presentation, Management, and Medicolegal Implications. Asian Spine J. 2020, 14, 742–759. [Google Scholar] [CrossRef]
- Kolinsky, D.C.; Liang, S.Y. Musculoskeletal Infections in the Emergency Department. Emerg. Med. Clin. North Am. 2018, 36, 751–766. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Prayag, P.S.; Purandare, B.D.; Patwardhan, S.A.; Pairaiturkar, P.P.; Rege, A.J.; Bhave, A.V.; Ramya, S.; Panchakshari, S.P.; Raja, P.T.; Melinkeri, A.S.; et al. COVID-19 Associated Vertebral Osteomyelitis Caused by Aspergillus Species—A Case Series. Indian J. Orthop. 2022, 56, 1268–1276. [Google Scholar] [CrossRef]
- Moreno-Gómez, L.M.; Esteban-Sinovas, O.; García-Pérez, D.; García-Posadas, G.; Delgado-Fernández, J.; Paredes, I. Case Report: SARS-CoV-2 Infection—Are We Redeemed? A Report of Candida Spondylodiscitis as a Late Complication. Front. Med. 2021, 8, 2223. [Google Scholar] [CrossRef] [PubMed]
- Talamonti, G.; Colistra, D.; Crisà, F.; Cenzato, M.; Giorgi, P.; D’Aliberti, G. Spinal epidural abscess in COVID-19 patients. J. Neurol. 2021, 268, 2320–2326. [Google Scholar] [CrossRef]
- Erok, B.; Kıbıcı, K. COVID-19 Infection Manifesting with Lumbar Spondylodiscitis Complicating with Psoas Abscess without Pneumonia. Indian J. Neurosurg. 2021. [Google Scholar] [CrossRef]
- Naderi, S. COVID-19 Infection Leading to Lethal Spondylodiscitis with Spinal Abscess. Iran. J. Neurosurg. 2020, 6, 151–154. [Google Scholar] [CrossRef]
- Ramlee, F.A.M.; Bin Harun, M.H.; Nagaretnam, V.; Lim, T.S.; Aris, H.F.; Tan, C.N. A Case Series of Spinal Infections Following COVID-19: A Delayed Complication. Cureus 2022, 14, e29272. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Point Prevalence Survey of Healthcareassociated Infections and Antimicrobial Use in European Acute Care Hospitals—Protocol Version 6; ECDC: Stockholm, Sweden, 2022. [Google Scholar] [CrossRef]
- Gautam, S.; Sharma, G.; Singla, S.; Garg, S. Case Report: Secondary Hemophagocytic Lymphohistiocytosis (sHLH) and Candida auris Fungemia in Post-acute COVID-19 Syndrome: A Clinical Challenge. Front. Med. 2022, 9, 835421. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef] [PubMed]
- Habib, G.; Mahmood, K.; Gul, H.; Tariq, M.; Ain, Q.U.; Hayat, A.; Rehman, M.U. Pathophysiology of Methicillin-Resistant Staphylococcus aureus Superinfection in COVID-19 Patients. Pathophysiology 2022, 29, 405–413. [Google Scholar] [CrossRef]
- Perez, M.E.; Fenoll, R.G.; Bayo, S.M.; Álvarez, R.M.M.; Millán, V.F.; Usón, M.C.V.; Ruiz, M.P.P.; Mainar, J.M.A.; Jiménez, M.C.M.; Paesa, C.R. Impact of Staphylococcus aureus bacteremia in COVID-19 patients. Rev. Esp. Quimioter. 2022, 35, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Stoop, N.; Zijlstra, H.; Ponds, N.H.; Wolterbeek, N.; Delawi, D.; Kempen, D.H. Long-term quality of life outcome after spondylodiscitis treatment. Spine J. 2021, 21, 1985–1992. [Google Scholar] [CrossRef] [PubMed]
- Scalia, G.; Umana, G.E.; Marrone, S.; Graziano, F.; Giuffrida, A.; Ponzo, G.; Giuffrida, M.; Furnari, M.; Galvano, G.; Nicoletti, G.F.; et al. Spontaneous anterior cervicothoracic spinal epidural hematoma extending to clivus in SARS-CoV-2 infection. Surg. Neurol. Int. 2021, 12, 181. [Google Scholar] [CrossRef]
- Schweizer, T.A.; Andreoni, F.; Acevedo, C.; Scheier, T.C.; Heggli, I.; Maggio, E.M.; Eberhard, N.; Brugger, S.D.; Dudli, S.; Zinkernagel, A.S. Intervertebral disc cell chondroptosis elicits neutrophil response in Staphylococcus aureus spondylodiscitis. Front. Immunol. 2022, 13, 908211. [Google Scholar] [CrossRef] [PubMed]
- McKenna, E.; Wubben, R.; Isaza-Correa, J.M.; Melo, A.M.; Mhaonaigh, A.U.; Conlon, N.; O’Donnell, J.S.; Cheallaigh, C.N.; Hurley, T.; Stevenson, N.J.; et al. Neutrophils in COVID-19: Not Innocent Bystanders. Front. Immunol. 2022, 13. [Google Scholar] [CrossRef]



| No | Gender | Age | Co-Morbidities | COVID-19 IST | Time Since COV | Fever | HC | Aetiology | Anatomic Site | Antibiotic | Surgery | Evolution | Dx Support | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 48 | AHT Obesity | Tocilizumab HC | Conc. (ICU) | yes | neg | MSSA | Ab T1-T7 | According ABG | Yes | Improve | MRI Ab + culture | Talamonti G, 2021 [27] |
| 2 | M | 47 | AHT Obesity | Tocilizumab Corticosteroid | Conc. (ICU) | no | poz | MSSA | Ab C4-C6 | According ABG | Yes | Improve | MRI Ab + culture | Talamonti G, 2021 [27] |
| 3 | M | 55 | Lymphoma AHT, MI | Tocilizumab | Conc. (ICU) | no | neg | MSSA | Ab C5-T1 | According ABG | Yes | Improve | MRI Ab + culture | Talamonti G, 2021 [27] |
| 4 | M | 56 | AHT, Venous Thrombosis | No | NA | no | neg | MSSA | Ab C1-2; Ab C7-T1 | According ABG | Yes | Pulmonary infarction; deteriorate | MRI Ab + culture | Talamonti G, 2021 [27] |
| 5 | F | 57 | Anaemia | No | NA | no | poz | MSSA | Ab T12-L5 | According ABG | Yes | Improve | MRI Ab + culture | Talamonti G, 2021 [27] |
| 6 | F | 78 | AHT, Obesity, Diabetes | No | NA | no | neg | MSSA | Ab T7-12 | According ABG | Yes | Improve | MRI Ab + culture | Talamonti G, 2021 [27] |
| 7 | F | 60 | No | No | 10 w | no | poz | MSSA | SD L4-5; Ab L3-2 | Pip/Taz; Cefazolin; Cloxacillin * | Yes | Improve | MRI | Ramlee M, 2022 [30] |
| 8 | M | 69 | IC, Bone metastases, prostate cancer | No | 12 w | no | neg | UN | SD L3-4-5 | Ceftriaxone | Yes | Improve | MRI | Ramlee M, 2022 [30] |
| 9 | F | 24 | No | No | 12 w | no | neg | TB | SD T2-7 | HRZE | Yes | Improve | MRI, HP exam | Ramlee M, 2022 [30] |
| 10 | M | 43 | No | No | Conc (ICU) | yes | neg | UN | SD L3-4 Psoas abscess | NA | Yes | Improve | MRI | Erok B, 2021 [28] |
| 11 | M | 71 | No | HC | Conc (ICU) | yes | neg | UN | Multiple SD and Ab | Meronem + Vancomycin | Yes | MSOF Death | MRI | Naderi S, 2020 [29] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Popovici, G.-C.; Georgescu, C.-V.; Arbune, A.-A.; Vasile, M.-C.; Olteanu, I.; Arbune, M. Post-COVID-19 Spondylodiscitis: A Case Study and Review of the Literature. Medicina 2023, 59, 616. https://doi.org/10.3390/medicina59030616
Popovici G-C, Georgescu C-V, Arbune A-A, Vasile M-C, Olteanu I, Arbune M. Post-COVID-19 Spondylodiscitis: A Case Study and Review of the Literature. Medicina. 2023; 59(3):616. https://doi.org/10.3390/medicina59030616
Chicago/Turabian StylePopovici, George-Cosmin, Costinela-Valerica Georgescu, Anca-Adriana Arbune, Mihaela-Camelia Vasile, Ionut Olteanu, and Manuela Arbune. 2023. "Post-COVID-19 Spondylodiscitis: A Case Study and Review of the Literature" Medicina 59, no. 3: 616. https://doi.org/10.3390/medicina59030616