
The Assessment of Antimicrobial Resistance in Gram-Negative and Gram-Positive Infective Endocarditis: A Multicentric Retrospective Analysis

 , , , , , ,
, , , , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Considerations
2.2. Inclusion Criteria and Study Variables
2.3. Methods of Microbial Detection and Antibiotic Resistance
2.4. Statistical Analysis
3. Results
3.1. Patients’ Demographics and Background
3.2. Endocarditis Features
3.3. Microbial Identification and Antibacterial Management
3.4. Risk Analysis
4. Discussion
4.1. Important Findings
4.2. Study Limitations and Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogdan, I.; Citu, C.; Bratosin, F.; Malita, D.; Romosan, I.; Gurban, C.V.; Bota, A.V.; Turaiche, M.; Bratu, M.L.; Pilut, C.N.; et al. The Impact of Multiplex PCR in Diagnosing and Managing Bacterial Infections in COVID-19 Patients Self-Medicated with Antibiotics. Antibiotics 2022, 11, 437. [Google Scholar] [CrossRef] [PubMed]
- Karaman, R.; Jubeh, B.; Breijyeh, Z. Resistance of Gram-Positive Bacteria to Current Antibacterial Agents and Overcoming Approaches. Molecules 2020, 25, 2888. [Google Scholar] [CrossRef] [PubMed]
- Breijyeh, Z.; Jubeh, B.; Karaman, R. Resistance of Gram-Negative Bacteria to Current Antibacterial Agents and Approaches to Resolve It. Molecules 2020, 25, 1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeriu, E.; Borda, A.; Vulcanescu, D.D.; Sarbu, V.; Arghirescu, S.T.; Ciorica, O.; Bratosin, F.; Marincu, I.; Horhat, F.G. Diagnosis and Management of Febrile Neutropenia in Pediatric Oncology Patients—A Systematic Review. Diagnostics 2022, 12, 1800. [Google Scholar] [CrossRef]
- Reygaert, W.C. An overview of the antimicrobial resistance mechanisms of bacteria. AIMS Microbiol. 2018, 4, 482–501. [Google Scholar] [CrossRef]
- Zhu, Q.; Yue, Y.; Zhu, L.; Cui, J.; Zhu, M.; Chen, L.; Yang, Z.; Liang, Z. Epidemiology and microbiology of Gram-positive bloodstream infections in a tertiary-care hospital in Beijing, China: A 6-year retrospective study. Antimicrob. Resist. Infect. Control 2018, 7, 107. [Google Scholar] [CrossRef]
- Algammal, A.M.; Hetta, H.F.; Elkelish, A.; Alkhalifah, D.H.H.; Hozzein, W.N.; Batiha, G.E.; El Nahhas, N.; Mabrok, M.A. Methicillin-Resistant Staphylococcus aureus (MRSA): One Health Perspective Approach to the Bacterium Epidemiology, Virulence Factors, Antibiotic-Resistance, and Zoonotic Impact. Infect. Drug Resist. 2020, 13, 3255–3265. [Google Scholar] [CrossRef]
- O’Driscoll, T.; Crank, C.W. Vancomycin-resistant enterococcal infections: Epidemiology, clinical manifestations, and optimal management. Infect. Drug Resist. 2015, 8, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Aslan, G.; Tezcan, S.; Delialioğlu, N.; Aydın, F.E.; Kuyucu, N.; Emekdaş, G. Evaluation of penicillin-binding protein genotypes in penicillin susceptible and resistant Streptococcus pneumoniae isolates. Mikrobiyol Bul. 2012, 46, 190–201. (In Turkish) [Google Scholar]
- Munita, J.M.; Arias, C.A. Mechanisms of Antibiotic Resistance. Microbiol Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Budea, C.M.; Pricop, M.; Bratosin, F.; Bogdan, I.; Saenger, M.; Ciorica, O.; Braescu, L.; Domuta, E.M.; Grigoras, M.L.; Citu, C.; et al. Antibacterial and Antifungal Management in Relation to the Clinical Characteristics of Elderly Patients with Infective Endocarditis: A Retrospective Analysis. Antibiotics 2022, 11, 956. [Google Scholar] [CrossRef]
- Gopalakrishnan, P.P.; Shukla, S.K.; Tak, T. Infective endocarditis: Rationale for revised guidelines for antibiotic prophylaxis. Clin. Med. Res. 2009, 7, 63–68. [Google Scholar] [CrossRef] [Green Version]
- Liesenborghs, L.; Meyers, S.; Lox, M.; Criel, M.; Claes, J.; Peetermans, M.; Trenson, S.; Vande Velde, G.; Vanden Berghe, P.; Baatsen, P.; et al. Staphylococcus aureus endocarditis: Distinct mechanisms of bacterial adhesion to damaged and inflamed heart valves. Eur. Heart J. 2019, 40, 3248–3259. [Google Scholar] [CrossRef]
- Messika, J.; La Combe, B.; Ricard, J.D. Oropharyngeal colonization: Epidemiology, treatment and ventilator-associated pneumonia prevention. Ann. Transl. Med. 2018, 6, 426. [Google Scholar] [CrossRef]
- Bouza, E.; Muñoz, P.; Burillo, A. Gram-negative endocarditis: Disease presentation, diagnosis and treatment. Curr. Opin. Infect. Dis. 2021, 34, 672–680. [Google Scholar] [CrossRef]
- Siciliano, R.F.; Randi, B.A.; Gualandro, D.M.; Sampaio, R.O.; Bittencourt, M.S.; da Silva Pelaes, C.E.; Mansur, A.J.; Pomerantzeff, P.M.A.; Tarasoutchi, F.; Strabelli, T.M.V. Early-onset prosthetic valve endocarditis definition revisited: Prospective study and literature review. Int. J. Infect. Dis. 2018, 67, 3–6. [Google Scholar] [CrossRef] [Green Version]
- de Feiter, P.W.; Jacobs, J.A.; Jacobs, M.J.; Vink, C.; van der Geest, S. Successful treatment of Staphylococcus epidermidis prosthetic valve endocarditis with linezolid after failure of treatment with oxacillin, gentamicin, rifampicin, vancomycin, and fusidic acid regimens. Scand. J. Infect. Dis. 2005, 37, 173–176. [Google Scholar] [CrossRef]
- Ortega-Loubon, C.; Muñoz-Moreno, M.F.; Andrés-García, I.; Álvarez, F.J.; Gómez-Sánchez, E.; Bustamante-Munguira, J.; Lorenzo-López, M.; Tamayo-Velasco, Á.; Jorge-Monjas, P.; Resino, S.; et al. Nosocomial Vs. Community-Acquired Infective Endocarditis in Spain: Location, Trends, Clinical Presentation, Etiology, and Survival in the 21st Century. J. Clin. Med. 2019, 8, 1755. [Google Scholar] [CrossRef] [Green Version]
- Ji, Y.; Kujtan, L.; Kershner, D. Acute endocarditis in intravenous drug users: A case report and literature review. J Community Hosp Intern. Med. Perspect. 2012, 2, 11513. [Google Scholar] [CrossRef]
- Bumm, C.V.; Folwaczny, M. Infective endocarditis and oral health—A Narrative Review. Cardiovasc. Diagn. Ther. 2021, 11, 1403–1415. [Google Scholar] [CrossRef] [PubMed]
- Elkattawy, S.; Alyacoub, R.; El-Feki, I.; Fichadiya, H.; Appiah-Kubi, E.; Romero, J.; Guo, X.; Edward, W. Tricuspid Endocarditis: A Case Report and Comprehensive Literature Review. Cureus 2022, 14, e24027. [Google Scholar] [CrossRef] [PubMed]
- Desimone, D.C.; Tleyjeh, I.M.; Correa de Sa, D.D.; Anavekar, N.S.; Lahr, B.D.; Sohail, M.R.; Steckelberg, J.M.; Wilson, W.R.; Baddour, L.M. Mayo Cardiovascular Infections Study Group. Incidence of infective endocarditis caused by viridans group streptococci before and after publication of the 2007 American Heart Association’s endocarditis prevention guidelines. Circulation 2012, 126, 60–64. [Google Scholar] [CrossRef] [PubMed]
- Sitthicharoenchai, P.; Burrough, E.R.; Arruda, B.L.; Sahin, O.; Dos Santos, J.G.; Magstadt, D.R.; Piñeyro, P.E.; Schwartz, K.J.; Rahe, M.C. Streptococcus gallolyticus and Bacterial Endocarditis in Swine, United States, 2015–2020. Emerg. Infect. Dis. 2022, 28, 192–195. [Google Scholar] [CrossRef]
- Van Rossum, T.; Ferretti, P.; Maistrenko, O.M.; Bork, P. Diversity within species: Interpreting strains in microbiomes. Nat. Rev. Microbiol. 2020, 18, 491–506. [Google Scholar] [CrossRef]
- Coates, J.; Park, B.R.; Le, D.; Şimşek, E.; Chaudhry, W.; Kim, M. Antibiotic-induced population fluctuations and stochastic clearance of bacteria. eLife 2018, 7, e32976. [Google Scholar] [CrossRef]
- Steindel, S.J. International classification of diseases, 10th edition, clinical modification and procedure coding system: Descriptive overview of the next generation HIPAA code sets. J. Am. Med. Inform. Assoc. 2010, 17, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Pecoraro, A.J.K.; Herbst, P.G.; Pienaar, C.; Taljaard, J.; Prozesky, H.; Janson, J.; Doubell, A.F. Modified Duke/European Society of Cardiology 2015 clinical criteria for infective endocarditis: Time for an update? Open Heart 2022, 9, e001856. [Google Scholar] [CrossRef]
- Boujelben, I.; Gdoura, R.; Hammami, A. A broad-range PCR technique for the diagnosis of infective endocarditis. Braz. J. Microbiol. 2018, 49, 534–543. [Google Scholar] [CrossRef]
- Fihman, V.; Faury, H.; Moussafeur, A.; Huguet, R.; Galy, A.; Gal-lien, S.; Lim, P.; Lepeule, R.; Woerther, P.L. Blood Cultures for the Diagnosis of Infective Endocarditis: What Is the Benefit of Prolonged Incubation? J. Clin. Med. 2021, 10, 5824. [Google Scholar] [CrossRef]
- Hafner, S.; Albittar, M.; Abdel-Kahaar, E.; Zolk, O. Antibiotic prophylaxis of infective endocarditis in oral and maxillofacial surgery: Incomplete implementation of guidelines in everyday clinical practice. Int. J. Oral. Maxillofac. Surg. 2020, 49, 522–528. [Google Scholar] [CrossRef]
- Jayasuriya, S.; Movahed, M.R. Infectious endocarditis with systemic septic embolization as a rare complication of cardiac catheterization. Exp. Clin. Cardiol. 2009, 14, e17–e20. [Google Scholar]
- Durante-Mangoni, E.; Tripodi, M.F.; Albisinni, R.; Utili, R. Management of Gram-negative and fungal endocarditis. Int. J. Antimicrob. Agents. 2010, 36 (Suppl. 2), S40–S45. [Google Scholar] [CrossRef] [Green Version]
- Krcmery, V.; Demitrovicova, A.; Hricak, V.; Kisac, P. Endocarditis due to Gram-negative bacteria. Int. J. Infect. Dis. 2010, 14 (Suppl. 3), e359. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, N.; Sapra, A. Gram Staining. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Humphries, R.M.; Kircher, S.; Ferrell, A.; Krause, K.M.; Malherbe, R.; Hsiung, A.; Burnham, C.A. The Continued Value of Disk Diffusion for Assessing Antimicrobial Susceptibility in Clinical Laboratories: Report from the Clinical and Laboratory Standards Institute Methods Development and Standardization Working Group. J. Clin. Microbiol. 2018, 56, e00437-18. [Google Scholar] [CrossRef] [Green Version]
- Karah, N.; Rafei, R.; Elamin, W.; Ghazy, A.; Abbara, A.; Hamze, M.; Uhlin, B.E. Guideline for Urine Culture and Biochemical Identification of Bacterial Urinary Pathogens in Low-Resource Settings. Diagnostics 2020, 10, 832. [Google Scholar] [CrossRef]
- Rantakokko-Jalava, K.; Jalava, J. Optimal DNA isolation method for detection of bacteria in clinical specimens by broad-range PCR. J. Clin. Microbiol. 2002, 40, 4211–4217. [Google Scholar] [CrossRef] [Green Version]
- Bayot, M.L.; Bragg, B.N. Antimicrobial Susceptibility Testing. [Updated 2022 Oct 10]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK539714 (accessed on 7 December 2022).
- Bast, A.; Dohmen, P.M.; Podbielski, A.; Warnke, P. Rapid Microbiological Diagnostics from Explanted Heart Valves by a Multiplex PCR Assay. J. Clin. Microbiol. 2019, 57, e01575-18. [Google Scholar] [CrossRef] [Green Version]
- IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Manyi-Loh, C.; Mamphweli, S.; Meyer, E.; Okoh, A. Antibiotic Use in Agriculture and Its Consequential Resistance in Environmental Sources: Potential Public Health Implications. Molecules 2018, 23, 795. [Google Scholar] [CrossRef] [Green Version]
- Waluszewski, A.; Cinti, A.; Perna, A. Antibiotics in pig meat production: Restrictions as the odd case and overuse as normality? Experiences from Sweden and Italy. Humanit. Soc. Sci. Commun. 2021, 8, 172. [Google Scholar] [CrossRef]
- Kobayashi, T.; Ando, T.; Streit, J.; Sekar, P. Current Evidence on Oral Antibiotics for Infective Endocarditis: A Narrative Review. Cardiol. Ther. 2019, 8, 167–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gesser, R.M.; McCarroll, K.A.; Woods, G.L. Evaluation of outpatient treatment with ertapenem in a double blind controlled clinical trial of complicated skin/skin structure infections. J. Infect. 2004, 48, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Hale, A.J.; Snyder, G.M.; Ahern, J.W.; Eliopoulos, G.; Ricotta, D.; Alston, W.K. When are oral antibiotics a safe and effective choice for bacterial bloodstream infections? An evidence-based narrative review. J. Hosp. Med. 2018, 13, 328–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iversen, K.; Ihlemann, N.; Gill, S.U.; Madsen, T.; Elming, H.; Jensen, K.T.; Bruun, N.E.; Hofsten, D.E.; Fursted, K.; Christensen, J.J.; et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N. Engl. J. Med. 2019, 380, 415–424. [Google Scholar] [CrossRef]
- Fernández Guerrero, M.L.; González López, J.J.; Goyenechea, A.; Fraile, J.; de Górgolas, M. Endocarditis caused by Staphylococcus aureus: A reappraisal of the epidemiologic, clinical, and pathologic manifestations with analysis of factors determining outcome. Medicine 2009, 88, 1–22. [Google Scholar] [CrossRef]
- Fowler, V.G., Jr.; Miro, J.M.; Hoen, B.; Cabell, C.H.; Abrutyn, E.; Rubinstein, E.; Corey, G.R.; Spelman, D.; Bradley, S.F.; Barsic, B.; et al. Staphylococcus aureus Endocarditis A Consequence of Medical Progress. JAMA 2005, 293, 3012–3021. [Google Scholar] [CrossRef] [Green Version]
- Meidrops, K.; Burkhardt, F.J.; Osipovs, J.D.; Petrosina, E.; Groma, V.; Stradins, P. Etiology, Risk Factors and Clinical Outcomes in Infective Endocarditis Patients Requiring Cardiac Surgery. J. Clin. Med. 2022, 11, 1957. [Google Scholar] [CrossRef]
- Ma, L.; Ge, Y.; Ma, H.; Zhu, B.; Miao, Q. Infective endocarditis at a tertiary-care hospital in China. J. Cardiothorac. Surg. 2020, 15, 135. [Google Scholar] [CrossRef]
- Hase, R.; Otsuka, Y.; Yoshida, K.; Hosokawa, N. Profile of infective endocarditis at a tertiary–care hospital in Japan over a 14-year period: Characteristics, outcome and predictors for in-hospital mortality. Int. J. Infect. Dis. 2015, 33, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The international collaboration on endocarditis-prospective cohort study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Nakatani, S.; Mitsutake, K.; Ohara, T.; Kokubo, Y.; Yamamoto, H.; Hanai, S. CADRE investiga-tors. Recent picture of infective endocarditis in Japan–lessons from cardiac disease regis-tration (CADRE-IE). Circ. J. 2013, 77, 1558–1564. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Cai, S.; Dai, H. Characteristics of infective endocarditis in a tertiary hospital in East China. PLoS ONE 2016, 11, e0166764. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Gram-Negative (n= 29) | Gram-Positive (n = 142) | Significance |
|---|---|---|---|
| Age (mean ± SD) | 62.6 ± 8.1 | 60.9 ± 7.8 | 0.289 * |
| Sex (Men) | 17 (58.6%) | 86 (60.6%) | 0.845 |
| BMI | 0.042 | ||
| Underweight (<18.5 kg/m2) | 5 (17.2%) | 12 (8.5%) | |
| Normal weight (18.5–25.0 kg/m2) | 16 (55.2%) | 56 (39.4%) | |
| Overweight (>25.0 kg/m2) | 8 (27.6%) | 74 (52.1%) | |
| Place of origin (urban) | 17 (58.6%) | 82 (57.7%) | 0.930 |
| Occupation | 0.342 | ||
| Employed | 1 (51.3%) | 12 (8.5%) | |
| Unemployed | 10 (42.3%) | 33 (23.2%) | |
| Retired | 18 (42.3%) | 97 (68.3%) | |
| Living conditions | <0.001 | ||
| Independent living | 18 (62.1%) | 126 (88.7%) | |
| Institutional care | 11 (37.9%) | 16 (11.3%) | |
| Substance use behavior | |||
| Smoking | 5 (17.2%) | 52 (36.6%) | 0.043 |
| Frequent alcohol consumption | 2 (6.9%) | 29 (20.4%) | 0.084 |
| Injection drug use | 0 (0.0%) | 2 (1.4%) | 0.520 |
| Non-injection drug use | 0 (0.0%) | 11 (7.7%) | 0.121 |
| Comorbidities | |||
| Cardiovascular disease (non-valvular) | 13 (44.8%) | 59 (41.5%) | 0.744 |
| Valvulopathies | 5 (17.2%) | 34 (23.9%) | 0.433 |
| Diabetes mellitus | 5 (17.2%) | 47 (33.1%) | 0.091 |
| Cerebrovascular disease | 8 (27.6%) | 17 (12.0%) | 0.030 |
| Digestive and liver | 4 (13.8%) | 30 (21.1%) | 0.367 |
| Chronic kidney disease | 12 (41.4%) | 32 (22.5%) | 0.034 |
| Bad oral hygiene | 17 (58.6%) | 55 (38.7%) | 0.048 |
| Cancer | 1 (3.4%) | 8 (5.6%) | 0.631 |
| Immunosuppression | 3 (10.3%) | 11 (7.7%) | 0.641 |
| Others | 2 (6.9%) | 6 (4.2%) | 0.534 |
| Variables | Gram-Negative (n = 29) | Gram-Positive (n = 142) | Significance |
|---|---|---|---|
| Diagnostic delay, days (median, IQR) | 2.5 (2.0) | 3.5 (2.5) | 0.103 |
| Empiric treatment delay, days (median, IQR) | 1.5 (2.5) | 2.0 (2.0) | 0.322 |
| Presence of vegetations | 19 (65.5%) | 104 (73.2%) | 0.399 |
| Presence of cardiac abscess | 3 (10.3%) | 31 (21.8%) | 0.157 |
| Predisposing valvulopathy (n = 39) | (n = 5) | (n = 34) | 0.034 |
| Aortic | 4 (80.0%) | 8 (23.5%) | |
| Mitral | 1 (20.0%) | 22 (64.7%) | |
| Tricuspid | 0 (0.0%) | 4 (11.8%) | |
| Presence of a pacemaker device | 1 (3.4%) | 26 (18.3%) | 0.045 |
| Etiology | |||
| Peripheral/Central vein catheter | 9 (31.0%) | 18 (12.7%) | 0.013 |
| Hemodialysis | 1 (3.4%) | 11 (7.7%) | 0.408 |
| Cardiac surgery | 0 (0.0%) | 4 (2.8%) | 0.360 |
| Angiography | 2 (6.9%) | 31 (21.8%) | 0.063 |
| Vascular surgery | 2 (6.9%) | 10 (7.0%) | 0.977 |
| Gastrointestinal | 1 (3.4%) | 18 (12.7%) | 0.149 |
| Maxillo-Facial interventions | 5 (17.2%) | 14 (9.9%) | 0.249 |
| Dental/Ear-Nose-Throat interventions | 6 (15.5%) | 18 (12.7%) | 0.257 |
| Unknown | 3 (10.3%) | 20 (14.1%) | 0.590 |
| Variables | Gram-Negative (n = 29) | Gram-Positive (n = 142) | Significance |
|---|---|---|---|
| Signs and symptoms | |||
| Fever | 23 (79.3%) | 132 (93.0%) | 0.021 |
| Constitutional symptoms | 18 (62.1%) | 114 (80.3%) | 0.033 |
| Neurological involvement | 13 (44.8%) | 37 (26.1%) | 0.042 |
| Duke criteria | <0.001 | ||
| Two major criteria | 21 (72.4%) | 46 (32.4%) | |
| One major + three minor criteria | 5 (17.2%) | 74 (52.1%) | |
| Five minor criteria | 3 (10.3%) | 22 (15.5%) | |
| Cardiac signs | |||
| Heart failure | 14 (48.3%) | 45 (31.7%) | 0.044 |
| Murmur | 16 (55.2%) | 68 (47.9%) | 0.474 |
| EKG abnormalities | 18 (62.1%) | 75 (52.8%) | 0.138 |
| Embolic manifestations | 8 (27.6%) | 31 (21.8%) | 0.501 |
| Rheumatic signs | 9 (31.0%) | 74 (52.1%) | 0.038 |
| Skin findings | 3 (10.3%) | 29 (20.4%) | 0.204 |
| Renal involvement | 19 (65.5%) | 94 (59.2%) | 0.523 |
| Hematological abnormalities | 13 (44.8%) | 45 (31.7%) | 0.173 |
| The severity of valvular regurgitation | 0.036 | ||
| Mild | 6 (20.7%) | 54 (38.0%) | |
| Moderate | 14 (48.3%) | 69 (48.6%) | |
| Severe | 9 (31.0%) | 19 (13.4%) | |
| Outcomes | |||
| ICU admission | 19 (65.5%) | 63 (44.4%) | 0.037 |
| Days in the ICU (mean ± SD) | 5.6 ± 2.4 | 7.9 ± 3.1 | <0.001 |
| Days between symptom onset until death (mean ± SD) | 6.2 ± 3.0 | 7.4 ± 3.9 | <0.001 |
| Days between symptom onset until ICU admission (median, IQR) | 5.8 ± 4.1 | 3.0 ± 5.3 | <0.001 |
| Mortality | 17 (58.6%) | 49 (34.5%) | 0.015 |
| Days until discharge (mean ± SD) | 19.6 ± 5.3 | 14.4 ± 6.0 | <0.001 |
| Variables * | Gram-Negative (n = 29) | Gram-Positive (n = 142) | Significance |
|---|---|---|---|
| Tests performed for infection identification | |||
| Conventional culture | 24 (82.8%) | 130 (91.5%) | 0.149 |
| PCR | 5 (17.2%) | 12 (8.5%) | 0.149 |
| Culture and PCR | 7 (24.1%) | 36 (25.4%) | 0.890 |
| Testing | 0.435 | ||
| Positive samples | 17 (58.6%) | 94 (66.2.%) | |
| False negative result | 12 (41.4%) | 48 (33.8%) | |
| Antibiotic therapy | 0.619 | ||
| Intravenous | 25 (86.2%) | 111 (78.2%) | |
| Oral | 3 (10.3%) | 12 (16.2%) | |
| Combination | 1 (3.4%) | 36 (5.6%) | |
| Severe treatment complications | 7 (24.1%) | 21 (14.8%) | 0.215 |
| Treatment regimen type | 0.361 | ||
| Monotherapy | 11 (37.9%) | 67 (47.2%) | |
| Combined | 18 (62.1%) | 75 (52.8%) | |
| Change in antibiotics during hospitalization | 8 (27.6%) | 30 (21.1%) | 0.445 |
| Antibiotics side effects | |||
| Acute immune reactions | 2 (6.9%) | 7 (4.9%) | 0.665 |
| Delayed reactions | 1 (3.4%) | 6 (4.2%) | 0.847 |
| Nephrotoxicity | 9 (31.0%) | 29 (20.4%) | 0.210 |
| Neurotoxicity | 4 (13.8%) | 14 (9.9%) | 0.529 |
| Liver injury | 5 (17.2%) | 11 (7.7%) | 0.109 |
| Digestive side effects | 5 (17.2%) | 33 (23.2%) | 0.478 |
| Falls and delirium | 5 (17.2%) | 11 (7.7%) | 0.109 |
| Multidrug resistance | 0.368 | ||
| Yes | 25 (86.2%) | 130 (91.5%) | |
| No | 4 (13.8%) | 12 (8.5%) | |
| Distribution of antimicrobial resistance | (n = 29) | (n = 142) | 0.549 |
| 0 drug resistance (n = 46) | 5 (17.2%) | 41 (28.9%) | |
| 1 drug resistance (n = 33) | 5 (17.2%) | 28 (19.7%) | |
| 2 drug resistance (n = 41) | 8 (27.6%) | 33 (23.2%) | |
| ≥3 drug resistance (n = 51) | 11 (37.9%) | 40 (28.2%) |
| Variables | 0 Drug Resistance (n = 46) | 1 Drug Resistance (n = 33) | 2 Drug Resistance (n = 41) | ≥3 Drug Resistance (n = 51) | Significance |
|---|---|---|---|---|---|
| Gram-negative | (n = 6) | (n = 2) | (n = 10) | (n = 11) | 0.506 * |
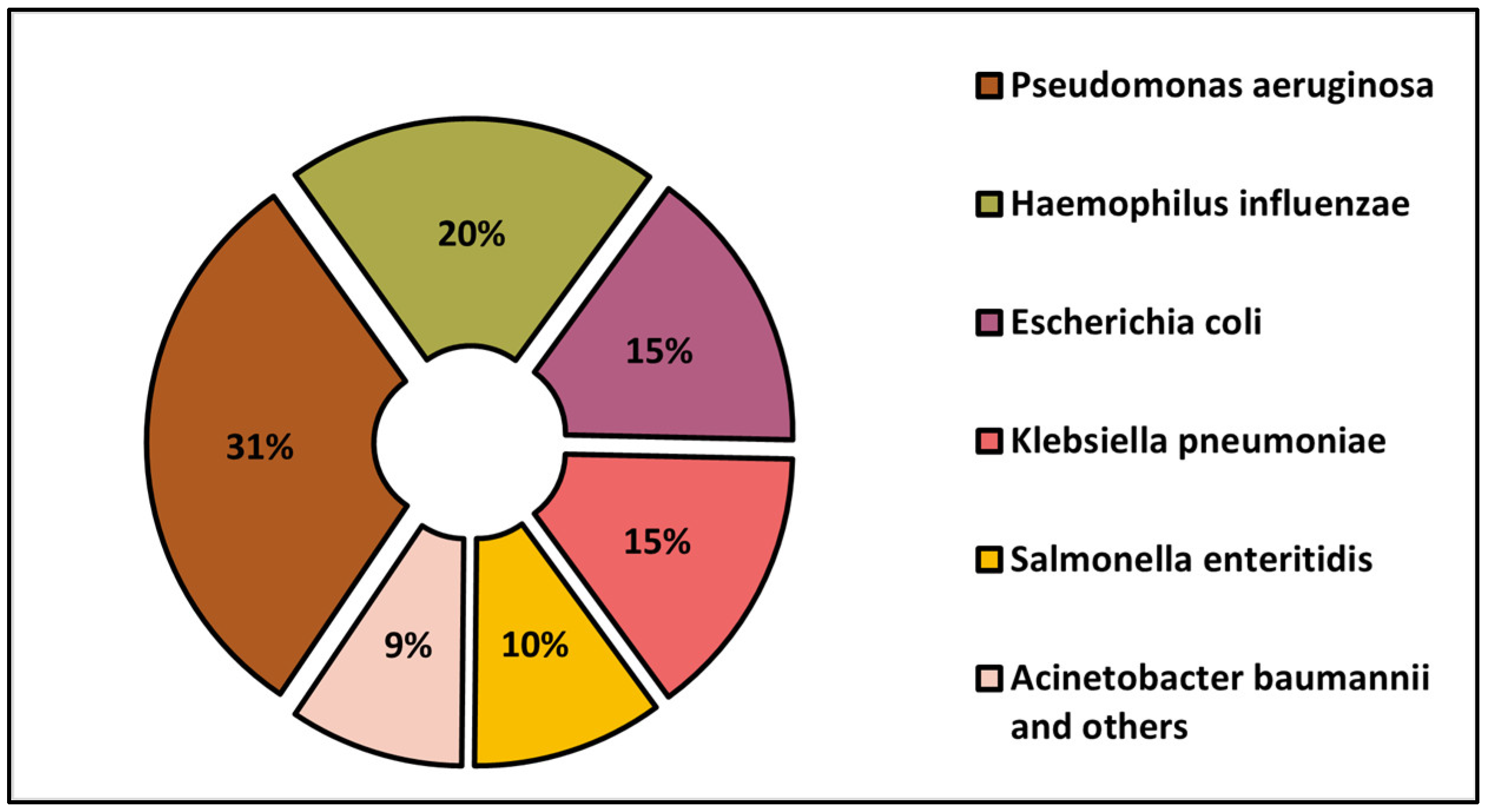
| Pseudomonas aeruginosa (n = 9) | 1 (16.7%) | 1 (34.3%) | 3 (30.0%) | 4 (36.4%) | |
| Haemophilus influenzae (n = 6) | 2 (33.3%) | 0 (34.3%) | 2 (20.0%) | 2 (18.2%) | |
| Escherichia coli (n = 4) | 1 (16.7%) | 1 (34.3%) | 1 (10.0%) | 1 (9.1%) | |
| Klebsiella pneumoniae (n = 4) | 2 (33.3%) | 0 (0.0%) | 2 (20.0%) | 0 (0.0%) | |
| Salmonella enteritidis (n = 3) | 0 (0.0%) | 0 (0.0%) | 2 (20.0%) | 1 (9.1%) | |
| Acinetobacter baumannii and others (n = 3) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 3 (27.3%) | |
| Gram-positive | (n = 40) | (n = 31) | (n = 31) | (n = 40) | 0.794 * |
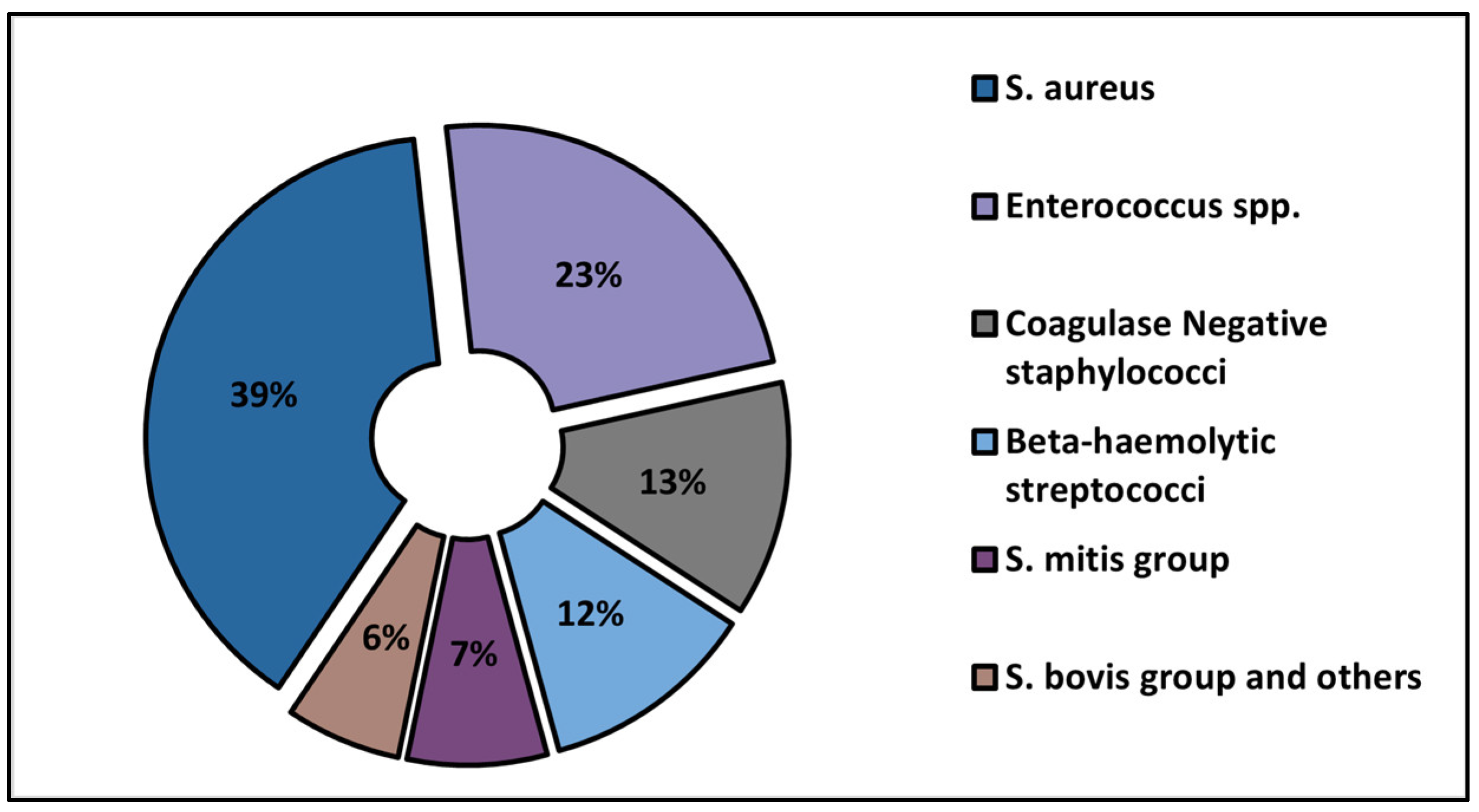
| S. aureus (n = 55) | 11 (32.4%) | 14 (42.4%) | 15 (40.5%) | 15 (34.9%) | |
| Enterococcus spp. (n = 32) | 6 (25.0%) | 8 (24.2%) | 8 (21.6%) | 10 (23.3%) | |
| Coagulase-negative staphylococci (n = 18) | 4 (8.3%) | 3 (9.1%) | 6 (16.2%) | 5 (11.6%) | |
| Beta-hemolytic streptococci (n = 17) | 5 (5.6%) | 2 (6.1%) | 4 (10.8%) | 6 (14.0%) | |
| S. mitis group (n = 10) | 2 (8.3%) | 3 (9.1%) | 1 (2.7%) | 4 (9.3%) | |
| S. bovis group and others (n = 10) | 3 (5.6%) | 1 (2.9%) | 3 (9.1%) | 3 (7.0%) | |
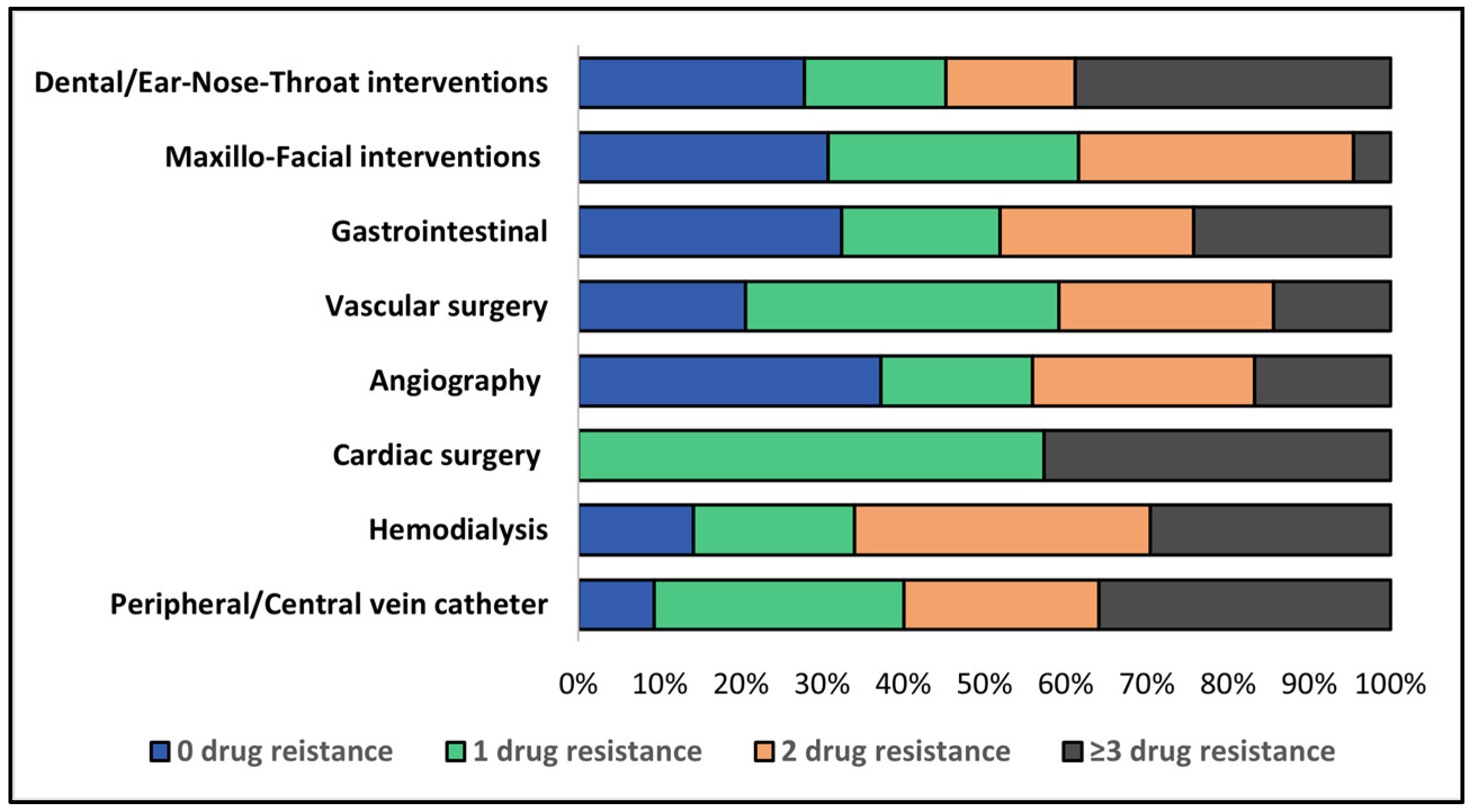
| Etiology | (n = 46) | (n = 33) | (n = 41) | (n = 51) | 0.328 * |
| Peripheral/Central vein catheter (n = 27) | 3 (6.7%) | 7 (21.9%) | 6 (17.1%) | 11 (25.6%) | |
| Hemodialysis (n = 12) | 2 (4.4%) | 2 (6.3%) | 4 (11.4%) | 4 (9.3%) | |
| Cardiac surgery (n = 4) | 0 (0.0%) | 2 (6.3%) | 0 (0.0%) | 2 (4.7%) | |
| Angiography (n = 33) | 14 (31.1%) | 5 (15.6%) | 8 (22.9%) | 6 (14.0%) | |
| Vascular surgery (n = 12) | 3 (6.7%) | 4 (12.5%) | 3 (8.6%) | 2 (4.7%) | |
| Gastrointestinal (n = 19) | 7 (15.6%) | 3 (9.4%) | 4 (11.4%) | 5 (11.6%) | |
| Maxillo-Facial interventions (n = 19) | 7 (15.6%) | 5 (15.6%) | 6 (17.1%) | 1 (2.3%) | |
| Dental/Ear-Nose-Throat interventions (n = 24) | 9 (20.0%) | 4 (12.5%) | 4 (11.4%) | 8 (27.9%) | |
| Unknown (n = 23) | – | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Budea, C.M.; Pricop, M.; Mot, I.C.; Horhat, F.G.; Hemaswini, K.; Akshay, R.; Negrean, R.A.; Oprisoni, A.L.; Citu, C.; Bumbu, B.A.; et al. The Assessment of Antimicrobial Resistance in Gram-Negative and Gram-Positive Infective Endocarditis: A Multicentric Retrospective Analysis. Medicina 2023, 59, 457. https://doi.org/10.3390/medicina59030457
Budea CM, Pricop M, Mot IC, Horhat FG, Hemaswini K, Akshay R, Negrean RA, Oprisoni AL, Citu C, Bumbu BA, et al. The Assessment of Antimicrobial Resistance in Gram-Negative and Gram-Positive Infective Endocarditis: A Multicentric Retrospective Analysis. Medicina. 2023; 59(3):457. https://doi.org/10.3390/medicina59030457
Chicago/Turabian StyleBudea, Camelia Melania, Marius Pricop, Ion Cristian Mot, Florin George Horhat, Kakarla Hemaswini, Raja Akshay, Rodica Anamaria Negrean, Andrada Licinia Oprisoni, Cosmin Citu, Bogdan Andrei Bumbu, and et al. 2023. "The Assessment of Antimicrobial Resistance in Gram-Negative and Gram-Positive Infective Endocarditis: A Multicentric Retrospective Analysis" Medicina 59, no. 3: 457. https://doi.org/10.3390/medicina59030457