
Perspectives towards End-of-Life Care in the Emergency Department of Tertiary Public Hospitals—A Qualitative Analysis
 , , ,
, , ,
Abstract
:1. Introduction
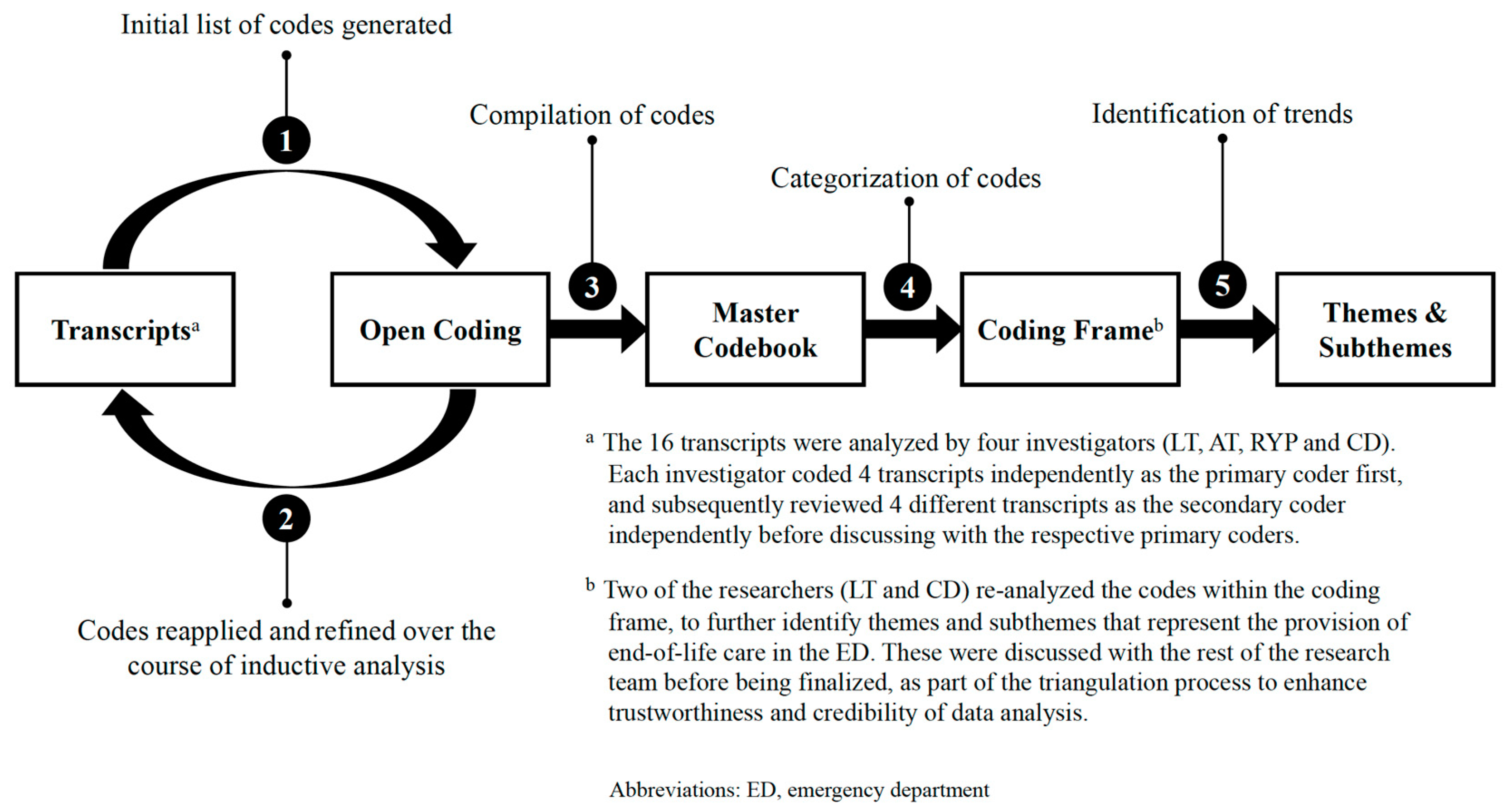
2. Materials and Methods
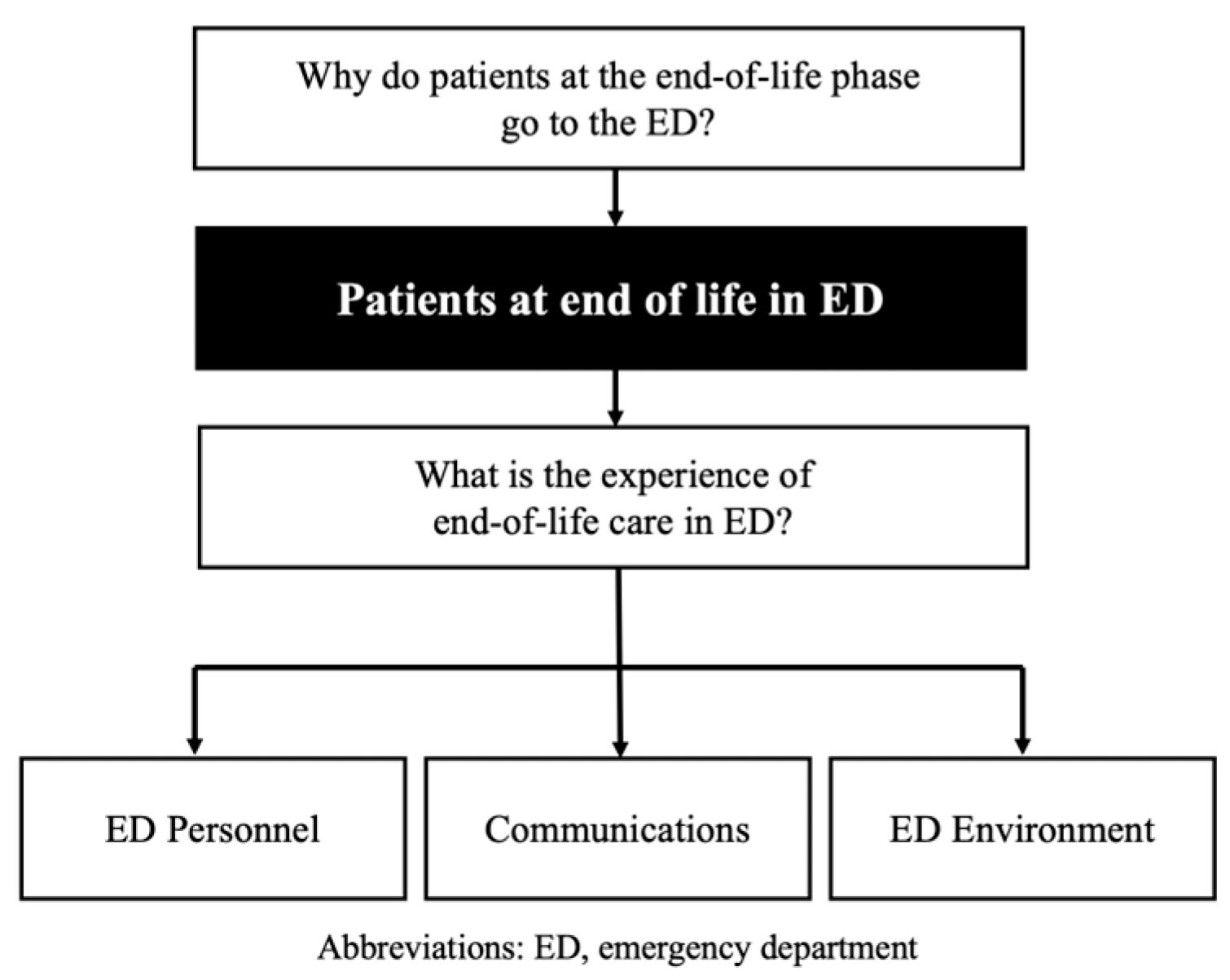
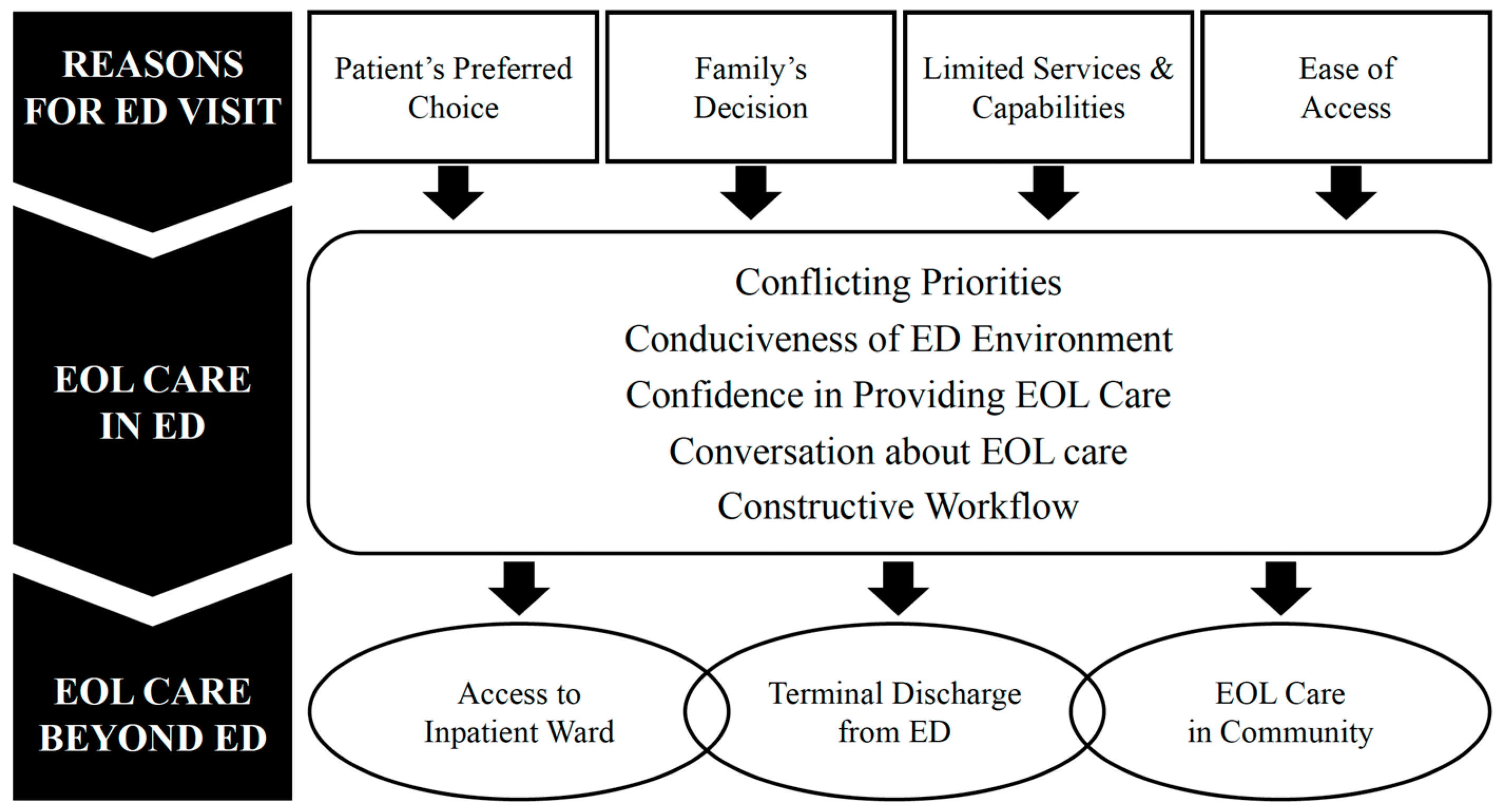
3. Results
3.1. Reasons for ED Visit
3.1.1. Patients’ Preferred Choice
“He (the patient) said that no, he is not going to go home …he said ‘I go home, I’m alone… here (there are) people (who) take care of me.’”(Next-of-kin, Session 4)
3.1.2. Family’s Decision
“The family is the one who would bring these patients to the ED, because they are very scared… they don’t know what to expect… how the real dying process (is like)...”(ED physician, Session 1)
“Family sometimes, because of emotional coping… may change their mind, so they say ‘Let’s give (the patient) another last chance.’”(Community healthcare professional, Session 7)
3.1.3. Limited Services and Capabilities
“More often than not, it would be a hypotension, desaturation, patients requiring antibiotics that need to be given in the restructured hospital, since the community hospitals have limited antibiotics… Those patients with fentanyl infusions—our nurses are not skilled yet for that.”(Community healthcare professional, Session 7)
3.1.4. Ease of Access
“In the community, I think the services (are) just not enough at the moment. Like home hospice, GPs (general practitioners), they are not available 24/7 and sometimes if you make a referral, it takes a few days...”(ED physician, Session 3)
3.2. End-of-Life Care in the ED
3.2.1. Conflicting Priorities
“It’s so busy.... It’s so chaotic. I feel the physicians are rushing and they have to attend to emergency cases. You (end-of-life patients) are not so urgent; they will leave you there for a while...”(Next-of-kin, Session 1)
3.2.2. Conduciveness of ED Environment
“ED—the space, the environment. It is TOO crowded. I think that is very important, at least give us space…it’s a SHOCK. PATIENT, PATIENT, PATIENT next to each other. And the relatives in between and… the (end-of-life) patient… they are in pain. It’s so painstaking looking at them...”(Next-of-kin, Session 6)
3.2.3. Confidence in Providing End-of-Life Care
“…my patient is gasping, my patient is in severe discomfort, SOB (shortness of breath) and pain, and we are advocating for subcut(aneous) fentanyl or morphine, and they (the physicians) are not comfortable. So, we need to wait for the inpatient (palliative team) to come.”(ED nurse, Session 6)
3.2.4. Conversations about End-of-Life Care in the ED
“It’s very hard to establish an end-of-life (care plan) at the first visit. In a few minutes, it’s very hard to tell the family members, ‘Your mum is going to die and then we are going through the comfort measures.’ Because they will think that we are not doing anything, we are giving up on hope…”(ED physician, Session 2)
“Sometimes their notes say ‘PALLIATIVE’. But when you go and talk to the patient, talk to the family, they are like ‘Huh? That was never communicated.’ So, it becomes very frustrating for us, and also very scary for the family, and very shocking…”(ED physician, Session 3)
“…it was a young ED physician. I was really impressed with him…While he conveyed it, I think the message (was) clear… I suppose it’s the empathy that comes with it. It’s the human factor—the empathy …”(Next-of-kin, Session 2)
3.2.5. Constructive Workflow
“So, in (Hospital X), there is close collaboration between ED and the palliative care department. During office hours, whenever the patient ends up in the ED who’s actually known to (Hospice X, Hospice Y) or any home care service, they (the ED) will give us a call and we’ll actually go down to see.”(Community healthcare professional, Session 8)
3.3. End-of-Life Care beyond the ED
3.3.1. Access to Inpatient Wards
“Recently we worked with (Hospital X) about direct admission… According to the consultant, they will eyeball, see the patient ‘Is he well?’ If he’s well enough, (he) will go direct to the pal(liative) ward in (the hospital) … I personally think it’s a very good way to go.”(Community healthcare professional, Session 8)
3.3.2. Terminal Discharge from the ED
“Because the time and amount of resources we spent into organizing ONE terminal discharge, we could have seen maybe five to ten other patients … And because we DON’T do it too frequently, we take EVEN longer...”(ED physician, Session 3)
3.3.3. End-of-Life Care in the Community
“Sometimes, we (nursing home) do transfer patients to the inpatient hospice and they pass away there, so we can actually avoid their admission to the ED. Yah. So we… don’t waste resources for a patient who’s able to have direct admission, provided all parties are agreeable...”(Community healthcare professional, Session 8)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Why do patients come to the Emergency Department at the end-of-life?
- How do you feel about the end-of-life care given at the Emergency Department?
- Do you think there are any areas that could be improved upon?
- Do you have any suggestions on how we can improve end-of-life care in the Emergency Department?
- Apart from coming to the Emergency Department, do patients have any other options at the end-of-life?
- Environment
- Staff (doctors, nurses, allied health, others)
- Investigations done
- Treatment given
- Communication/engagement regarding patient’s condition, symptoms, and treatment
- Overall care including spiritual needs and emotional support
- Can you talk about that more?
- Help me understand what you mean
- Can you give an example?
- Why do you need to send patients at end-of-life to the Emergency Department?
- How do you feel about the end-of-life care given at the Emergency Department?
- Do you think there are any areas that could be improved upon?
- Do you have any suggestions on how we can improve end-of-life care in the Emergency Department?
- Apart from coming to the Emergency Department, do patients have any other options at the end-of-life?
- Environment
- Staff (doctors, nurses, allied health, others)
- Investigations done
- Treatment given
- Communication/engagement regarding patient’s condition, symptoms, and treatment
- Overall care including spiritual needs and emotional support
- Can you talk about that more?
- Help me understand what you mean
- Can you give an example?
- Why did your family member need to come to the Emergency Department on (visit date)?
- How do you feel about the end-of-life care given at the Emergency Department?
- Do you think there are any areas that could be improved upon?
- Do you have any suggestions on how we can improve end-of-life care in the Emergency Department?
- Apart from coming to the Emergency Department, do patients have any other options at the end-of-life?
- Environment
- Staff (doctors, nurses, allied health, others)
- Investigations done
- Treatment given
- Communication/engagement regarding patient’s condition, symptoms, and treatment
- Overall care including spiritual needs and emotional support
- Can you talk about that more?
- Help me understand what you mean
- Can you give an example?
Appendix B

{kind=link}
{kind=link}
{kind=link}
| Theme | Subtheme | Quotes |
|---|---|---|
| Reasons for EOL visit | Patient’s choice: Prefer to die in a hospital | “I feel that when sent to hospital, … there’s somebody there for you—the doctors, the nurses, (there is) medicine, then you feel more secure.”—ED Nurse, Session 5 “I asked Dad, ‘At your last moments, can we have it in the hospital?’… He was very happy with the arrangement (to pass on in hospital) … ‘I can bring you home, but you must be aware that I will not be able to administer the pain relief, medication, oxygen …’ So, I think he might have a bit of a struggle … maybe I want to die at home but I know that I will be in pain and discomfort.”—NOK, Session 2 |
| Family’s decision: Emotional unpreparedness | “They (the family) have this book (“Spending the last days together”), everything was discussed, but when you talk to them, they feel very lost. Maybe it was explained, but they don’t digest it. So, I believe the reason why they still send patient to the hospital is because they know, they understand, but they don’t know how to do it. They need guidance; they need help.”—ED Nurse, Session 5 | |
| Family’s decision: Inability to cope with new or worse symptoms | “Uncontrolled pain, as in, for a patient who is a palliative or onco(logy) patient, could be like they were very acutely dyspneic, … the family members got anxious, and they didn’t know how to cope with that.”—ED Physician, Session 2 “… people can suddenly turn either septic, or they may suddenly turn breathless, or they get overloaded from the ESRF (end-stage renal failure) … things which they are not prepared for, and because things happen so fast and the goals of care have not even been discussed yet, and the family is understandably very worried, we’ll be forced to send them (to ED).”—Community HCP, Session 7 “Usually old people like [death] to be very peaceful and go at home. So, we actually decided to (keep) her at home. But at that moment, she’s struggling because she’s (mimics gasping for air). She’s struggling. So, do we want to see her struggle in this way to go? No. So that’s why.”—NOK, Session 7 | |
| Family’s decision: Delay death | “Maybe family, at the point of time when the patient suddenly deteriorated, they cannot handle the situation or they are not ready to let go, although they know it’s time to go.”—ED Nurse, Session 4 “I think they (family) think that at least they send to the hospital, the hospital can still assist them, can still treat (the patient). So that even though the patient is dying … by sending the patient to hospital, maybe their life can extend a bit longer.”—ED Nurse, Session 5 | |
| Limited services and capabilities: Unable to perform certain tests and treatment in community | “Sometimes, we also refer (to ED) when there is something acutely reversible that we can’t do at home, (like) blood tests and drips.”—Community HCP, Session 7 “In the community hospital, pain, breathlessness [are common], but we needed to send to ED because we needed some procedure to be done, say, for example, he had a symptomatic pleural effusion that suddenly accumulated, but he had otherwise good function.”—Community HCP, Session 7 | |
| Ease of access: More financial support in acute hospitals | “Technically, if they call the right person [general practitioner], there’s someone who will come down, BUT the cost will be exponentially high, so USUALLY they will end up in A&E (Accident & Emergency) still.”—Community HCP, Session 7 “I have a number of patients who due to insurance... so for the hospice, you can’t use insurance to pay, whereas in hospital, you can.”—Community HCP, Session 8 | |
| Ease of access: Round-the-clock services in ED | “The other reason why they go back to the A&E (Accident & Emergency) is sometimes it’s a cold call and (the patient) is actively dying and unfortunately, we (general practitioner) can’t go down ourselves, so the easiest way is to go back to A&E (Accident & Emergency).”—Community HCP, Session 7 “They cannot cope at home, and primary care cannot provide them with the service at such short notice—because to effect, to link up with a home hospice or anything, it will take time.”—Community HCP, Session 7 | |
| Ease of access: Respite and support for families | “I think I was so tired because I had been running non-stop. And prior to that, I was watching him round the clock. So I was just exhausted. I admittedly was just glad that the doctors were taking care of him for me because we were so tired …”—NOK, Session 2 “We help them to settle everything, from casket to the certificate. So, (there is) less hassle for the family actually.”—ED Nurse, Session 5 | |
| EOL care in ED | Conflicting priorities: Juggling between EOL and other critically ill patients | “And I feel like even if I couldn’t do more, I feel like I HAVE to do more. So, for me, I feel that personally it’s a bit difficult, and I think that it’s even worse when there’s no time, like we have to take care of the patient and, you know, that we have to tear ourselves between these things. But unfortunately, that’s just the way it is.”—ED Physician, Session 3 “Because in ED, there are so many cases and there are SO MANY things going on, so there’s only so much you can do in that … (trails off). Yes, you need to care for the patient, but there are so many patients that you need to divide (your time) up and there are only so many people (ED staff) there, so you have to do the best you can in the time that you have.”—ED Physician, Session 2 |
| Conflicting priorities: Time and manpower constraints | “I believe, on average, when I have had these conversations without specialist support, it takes me—just the discussion alone—about half an hour to forty-five minutes, just the initial initiation of the discussion. But that’s my own experience. So, actually, the time investment is very large.”—ED Physician, Session 1 “But if we are really very busy, we just let them (family members) stay with the patient … Sometimes it may be that you are also not able to provide them the emotional support that they need at that point of time. But sometimes, you can’t blame us, we have other emergencies, we have other patients also… for me, honestly, I don’t prioritize the emotional aspect.”—ED Nurse, Session 6 | |
| Conflicting priorities: Lack of updates | “Of course, I want to know but there is no nurse. Everybody is busy.”—NOK, Session 3 “There’s no nurse that comes by, and before that, there were a lot of people roaming around, but after that, they (the patient and family) are just left there. So, I think the presence of a nurse coming in to check in... I think it makes a difference as well. Of course, having that private space is important, but when it’s already put apart from the whole ED, it makes them feel like ‘Oh, we are abandoned now and there’s no one.’ ”—Community HCP, Session 8 | |
| Conduciveness of ED environment: Overcrowding in ED | “Well, I think for patients who are like her (the dying patient), it may be better that they are actually isolated somewhere else. Yeah, in a room whereby it’s not so hectic (and) to see all the things happening like physicians running around … during the time she was there (in the ED), she was quite stressed because she kept looking around, seeing the physicians doing this and that. And... I think there was a patient who was shouting a lot and she was stressed.”—NOK, Session 5 | |
| Conduciveness of ED environment: Need for privacy and adequate space | “Because if it is actually the last moments, most of our patients will want to be in the presence of their loved ones and a private space for them to mourn, to say what they need to say. (A private space) is actually important instead of the chaotic situation in the ED.”—Community HCP, Session 8 “The only thing about that room is I think it’s a bit small. I mean the room is okay, but we had so many of us. Almost 20 of us including my cousins … So (we) ended up standing along the corridor. So, it was inconvenient for the staff. We also felt that we are blocking (the passageway)—the patients are moving, the physicians are moving, the nurses are moving … it was very congested.” —NOK, Session 5 | |
| Confidence in providing EOL care: Unfamiliar with EOL care and medications | “I find it more difficult, not just clinically difficult to manage, but also (the) family (is) difficult to manage … I’m not … (sighs) I guess I AM equipped to talk to them, and this is my training, but I still … find them a challenge.”—ED Physician, Session 3 “I feel like sometimes the physicians themselves dare not do the, ordering of the medications for the management of the patients, because some think, ‘The patient is too ill. I cannot start fentanyl for the patient because the patient’s blood pressure is already so low. It will further deteriorate the patient.’ ”—ED Nurse, Session 6 | |
| Confidence in providing EOL care: More training necessary | “And the next thing is nursing skill. A lot of them tell me that they are not TRAINED or didn’t undergo a course to insert a subcut(aneous) needle. So, they are not qualified, because they need to get the paper qualification nowadays. So, training and all are also relevant in order to administer palliative treatment in ED.”—Community HCP, Session 8 | |
| Conversation about EOL care in ED: Challenging due to lack of rapport | “In an emergency setting, … the challenge is we are seeing this patient probably for the first time. We look through all the records, we don’t know what the prior discussions have been like and what the patient’s trajectory has been in the last few months. So, it’s a bit challenging for us to take on the role of exploring all these expectations, if they were not previously explored.”—ED Physician, Session 1 | |
| Conversation about EOL care in ED: Family not ready or did not understand prior discussion | “The hardest is (with) these cases, like (when the) patient doesn’t know the diagnosis or … the family doesn’t know and (only) the patient knows it. Yeah, so that’s the hardest.”—ED Nurse, Session 5 “The most difficult are the family who … at the last critical moment, break down and change their mind absolutely. Initially (they) say palliate all the way. Then, when the moment comes and the person is actively dying, all those discussions get thrown out of the window...”—Community HCP, Session 8 | |
| Conversation about EOL care in ED: Importance of empathy and effective communications | “Actually, the physicians were very good. They explained very clearly and they were very tactful. And especially (when) they knew it’s the end-of-life, they explained in a very nice way and gave us a brochure (“Spending the last days together”) … to get us prepared.”—NOK, Session 7 | |
| Conversation about EOL care in ED: Importance of aligning goals of care within ED team | “Actually, you feel lost, because you don’t know what has been conveyed and what has not been conveyed, who accepted it properly, who didn’t accept it properly, and what can I say next? … So you have to go back to your physician, ‘Physician, how? What happened? What are the things that you said?’… Even (for) that, we don’t have (clear) communication between each other.”—ED Nurse, Session 4 | |
| Constructive workflow: Protocols and guidelines for standardized care | “There are also suggestions on the protocol (on) what medications you can give for whatever symptoms that develop during the end-of-life process, and THAT helps us to cognitively offload quite a bit, so I don’t have to think, ‘Oh, what was this drug that I have to give? How much was the dose?’ And everything is written in already and the nurses know how to execute it.”—ED Physician, Session 3 “So, we have a workflow, the EOL pathway, so by referring to that pathway, it’s quite straight(forward)… Even though I’m trained, I do forget because we don’t have these kinds of cases frequently, so it’s good to just refer [to it] ‘Oh, these are the SOP (Standards of Practice) and this is the management.’ ”—ED Nurse, Session 4 | |
| Constructive workflow: Importance of multi-disciplinary collaborations | “Generally, during office hours, we tend to call the pal(liative) team, because they are most familiar with the patients and they do assist us a lot, in terms of, like, with the demands of both ED care, as well as having to care for a pal(liative) patient.”—ED Physician, Session 2 “They (the medical social workers) have come [to the ED] and done the appropriate things, helped us with the (EOL) journey, … they have done a very great job being that person that I needed to be, but I couldn’t be there.”—ED Physician, Session 3 | |
| Constructive workflow: Presence of advocates and champions | “I try to advocate. Like, for example, there’s a patient that I really identify as (being at the) end-of-life, I will advocate to my physicians … There should be nurses who (are) around every shift that can really advocate for them, because we have an end-of-life pathway, but not everyone is aware and not all physicians are aware.”—ED Nurse, Session 6 | |
| EOL care beyond ED | Access to inpatient wards: Importance of streamlining access | “When you want to transfer the EOL patient from ED to ward, can the ED doctor decide to send to the EOL room in the ward or not? You see, to me, I think it’s very important, because to send to (any bed in) the General Ward, there are (other) patients in the room and, you know, it defeats the whole purpose of what you are doing in the ED actually. There is no continuation on that.”—Community HCP, Session 8 “The one that I call is the palliative team in the hospital and tell them ‘This case is coming (from nursing home) just for palliation. He’s in the A&E (Accident & Emergency) right now. Can you quickly go and fish him out and just palliate him BEFORE anyone inserts an IV (intravenous) for him?’ But in order to do that, you need to put in that EXTRA effort to communicate with the hospital.”—Community HCP, Session 8 |
| Terminal discharge from ED: Coordinating logistics is challenging in ED | “It’s JUST a lot of work, you have to call a lot of people.”—ED Physician, Session 3 “I think for terminal discharge, the procedure is really very time-consuming, because it involves (caregiver) education on the medication, sourcing for resources and family education to look after the symptoms.”—ED Nurse, Session 4 | |
| Terminal discharge from ED: Increase in ED terminal discharges | “Some even discharge with morphine, with Paracet Sup (Paracetamol suppository), some of these basic things, and they get a generic list from the A&E (Accident & Emergency) about who to call in the event of demise, so it’s quite good now. And some of the A&E (Accident & Emergency) doctors have training in DipPal (Diploma in Palliative Medicine), so they may even give fentanyl (infusion) pumps.”—Community HCP, Session 7 “So, NOW, increasingly, we are seeing a lot of … discussion on end-of-life care from A&E (Accident & Emergency) … At least for me, I’m seeing a lot more willingness to allow the patient to quickly go back [home] to pass on.”—Community HCP, Session 7 | |
| Terminal discharge from ED: Robust palliative team support required | “Can we refer this kind of patient to the palliative care team? Because they know more about terminal discharges, education, and they recognize the symptoms and can give resource contacts to the patient or the NOK (next-of-kin) … I think it’s good to consider whether we can refer this group of patients or the NOK to the palliative (team), they have more knowledge or more resources. —ED Nurse, Session 4 “For terminal discharges, maybe a specialized group to come in to help us would be better given the ED environment.”—ED Nurse, Session 4 | |
| EOL care in community: Alternatives care arrangements need to be available to avoid ED attendances | “Our community hospital is connected with the restructured hospital. And we wanted to reduce the burden of sending (to ED), reduce the burden of patients. So, what we did was to liaise with the restructured hospital—the (project) group—to see the patients in the community hospital.”—Community HCP, Session 8 “A program done by (the hospital)—giving free phones to elderly who did not have a phone. There is an app on the phone that directly connects patient to the operator. Operators have records and are trained to direct patients according to their needs. For example, if (the) patient is facing a problem, the operator might say okay you have this problem now so I will send someone who is near you to go see you. I guess main point here is to allow patients to have a direct link to services in the community. Now that is lacking. People only know how to call 995 (public ambulance).”—Community HCP, Session 9 | |
| EOL care in community: Family education is important for successful EOL care at home | “I should think that the next leap forward is in family education and home hospice support, in order to deal with that (managing the dying patient at home), rather than providing this care in A&E (Accident & Emergency) … to keep all these people out of hospital.”—ED Physician, Session 1 “Help us (family) to understand the situation, what we can do … let the family know that ‘Anytime (soon) your mom will be going off.’ And what we can do for her.”—NOK, Session 3 |
References
- Chan, G.K. End-of-life Models and Emergency Department Care. Acad. Emerg. Med. 2004, 11, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Clarke, R. Improving end-of-life care in emergency departments. Emerg. Nurse 2008, 16, 34–37. [Google Scholar] [CrossRef] [PubMed]
- Solberg, L.M.; Hincapie-Echeverri, J. Palliative Care in the Emergency Department. Crit. Care Nurs. Clin. N. Am. 2015, 27, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Mierendorf, S.M.; Gidvani, V. Palliative Care in the Emergency Department. Perm. J. 2014, 18, 77–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqahtani, A.J.; Mitchell, G. End-of-Life Care Challenges from Staff Viewpoints in Emergency Departments: Systematic Review. Healthcare 2019, 7, 83. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.; Pang, W.S. Preferred place of death—A local study of cancer patients and their relatives. Singap. Med. J. 1998, 39, 447–450. [Google Scholar]
- Registry of Births and Deaths, Singapore Demographic Bulletin, July–September 2020; Immigration and Checkpoints Authority: Singapore, 2020. Available online: https://www.ica.gov.sg/news-and-publications/statistics (accessed on 8 February 2021).
- Lim, J. Sustainable Health Care Financing: The Singapore Experience. Glob. Policy 2017, 8, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Teo, J. Singapore Public Hospitals Raised A&E Fees This Year. The Straits Time. 2021. Available online: https://www.straitstimes.com/singapore/health/public-hospitals-raised-fees-for-emergency-services-this-year (accessed on 3 June 2022).
- Ouchi, K.; George, N.; Schuur, J.D.; Aaronson, E.L.; Lindvall, C.; Bernstein, E.; Sudore, R.L.; Schonberg, M.A.; Block, S.D.; Tulsky, J.A. Goals-of-Care Conversations for Older Adults with Serious Illness in the Emergency Department: Challenges and Opportunities. Ann. Emerg. Med. 2019, 74, 276–284. [Google Scholar] [CrossRef]
- Swenson, A.; Hyde, R. Understanding patients’ end-of-life goals of care in the emergency department. J. Am. Coll. Emerg. Physicians Open 2021, 2, e12388. [Google Scholar] [CrossRef]
- McCallum, K.J.; Jackson, D.; Walthall, H.; Aveyard, H. Exploring the quality of the dying and death experience in the Emergency Department: An integrative literature review. Int. J. Nurs. Stud. 2018, 85, 106–117. [Google Scholar] [CrossRef]
- Sopcheck, J.; Tappen, R.M. Nursing Home Resident, Family, and Staff Perspectives on Hospital Transfers for End-of-Life Care. Omega J. Death Dying 2021, 86, 1046–1068. [Google Scholar] [CrossRef]
- Trahan, L.M.; Spiers, J.A.; Cummings, G.G. Decisions to Transfer Nursing Home Residents to Emergency Departments: A Scoping Review of Contributing Factors and Staff Perspectives. J. Am. Med. Dir. Assoc. 2016, 17, 994–1005. [Google Scholar] [CrossRef] [PubMed]
- Allen, J.A. The Constructivist Paradigm. J. Teach. Soc. Work 1994, 8, 31–54. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall, Inc.: Upper Saddle River, NJ, USA, 1986. [Google Scholar]
- Attendances at Emergency Medicine Departments; Ministry of Health: Singapore, 2020. Available online: https://www.moh.gov.sg/resources-statistics/healthcare-institution-statistics/attendances-at-emergency-medicine-departments (accessed on 1 March 2021).
- Selman, L.; Robinson, V.; Klass, L.; Khan, S.; George, R.; Shepherd, K.; Burman, R.; Koffman, J. Improving confidence and competence of healthcare professionals in end-of-life care: An evaluation of the ‘Transforming End of Life Care’ course at an acute hospital trust: Table 1. BMJ Support. Palliat. Care 2016, 6, 231–236. [Google Scholar] [CrossRef] [Green Version]
- Weng, T.C.; Yang, Y.C.; Chen, P.J.; Kuo, W.F.; Wang, W.L.; Ke, Y.T.; Hsu, C.C.; Lin, K.C.; Huang, C.C.; Lin, H.J. Implementing a novel model for hospice and palliative care in the emergency department: An experience from a tertiary medical center in Taiwan. Medicine 2017, 96, e6943. [Google Scholar] [CrossRef]
- Di Leo, S.; Alquati, S.; Autelitano, C.; Costantini, M.; Martucci, G.; De Vincenzo, F.; Kuczynska, B.; Morini, A.; Trabucco, L.; Ursicelli, R.; et al. Palliative care in the emergency department as seen by providers and users: A qualitative study. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 88. [Google Scholar] [CrossRef]
- Marck, C.H.; Weil, J.; Lane, H.; Weiland, T.J.; Philip, J.; Boughey, M.; Jelinek, G.A. Care of the dying cancer patient in the emergency department: Findings from a National survey of Australian emergency department clinicians. Intern. Med. J. 2014, 44, 362–368. [Google Scholar] [CrossRef]
- Smith, A.K.; Fisher, J.; Schonberg, M.A.; Pallin, D.; Block, S.D.; Forrow, L.; Phillips, R.S.; McCarthy, E.P. Am I Doing the Right Thing? Provider Perspectives on Improving Palliative Care in the Emergency Department. Ann. Emerg. Med. 2009, 54, 86–93.e81. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.Y.; Kuan, W.S.; Koh, Y.; Venugopal, K.; Ibrahim, I. Death among elderly patients in the emergency department: A needs assessment for end-of-life care. Singap. Med J. 2017, 58, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Pal, R.Y.; Kuan, W.S.; Tiah, L.; Kumar, R.; Wong, Y.K.Y.; Shi, L.; Zheng, C.Q.; Lin, J.; Liang, S.; Segara, U.C.; et al. End-of-life management protocol offered within emergency room (EMPOWER): Study protocol for a multicentre study. BMJ Open 2020, 10, e036598. [Google Scholar] [CrossRef]
- Thomas, D.R. A general inductive approach for analyzing qualitative evaluation data. Am. J. Eval. 2006, 27, 237–246. [Google Scholar] [CrossRef]
- Glaser, B.G. The Constant Comparative Method of Qualitative Analysis. Soc. Probl. 2014, 12, 436–445. [Google Scholar] [CrossRef]
- Patrick, D.L.; Engelberg, R.A.; Curtis, J.R. Evaluating the Quality of Dying and Death. J. Pain Symptom Manag. 2001, 22, 717–726. [Google Scholar] [CrossRef] [PubMed]
- Hales, S.; Zimmermann, C.; Rodin, G. The Quality of Dying and Death. Arch. Intern. Med. 2008, 168, 912–918. [Google Scholar] [CrossRef] [PubMed]
- Keeley, M.P. Family Communication at the End of Life. Behav. Sci. 2017, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Tsubaki, M.; Fujimoto, M.; Sakaguchi, Y. Exploring the components of the quality of death in Japanese emergency departments: A qualitative study. Appl. Nurs. Res. 2020, 56, 151371. [Google Scholar] [CrossRef]
- Bailey, C.; Murphy, R.; Porock, D. Trajectories of End-of-Life Care in the Emergency Department. Ann. Emerg. Med. 2011, 57, 362–369. [Google Scholar] [CrossRef]
- Giles, T.M.; Hammad, K.; Breaden, K.; Drummond, C.; Bradley, S.L.; Gerace, A.; Muir-Cochrane, E. Nurses’ perceptions and experiences of caring for patients who die in the emergency department setting. Int. Emerg. Nurs. 2019, 47, 100789. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behaviour: Reactions and reflections. Psychol. Health 2011, 26, 1113–1127. [Google Scholar] [CrossRef]
- Icek, A. From Intentions to Actions: A Theory of Planned Behavior; SSSP Springer Series in Social, Psychology; Julius Kuhl, J.B., Ed.; Springer: Berlin/Heidelberg, Germany, 1985. [Google Scholar] [CrossRef]
- Bandura, A. Social Learning Theory. Group Organ. Stud. 1977, 2, 384–385. [Google Scholar] [CrossRef]
- Riekert, K.A.; Ockene, J.K.; Pbert, L. The Handbook of Health Behavior Change; Springer Publishing Company, Incorporated: New York, NY, USA, 2014. [Google Scholar]
- Harrison, A.W.; Rainer, R.K.; Hochwarter, W.A.; Thompson, K.R. Testing the Self-Efficacy—Performance Linkage of Social—Cognitive Theory. J. Soc. Psychol. 1997, 137, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Forero, R.; McDonnell, G.; Gallego, B.; McCarthy, S.; Mohsin, M.; Shanley, C.; Formby, F.; Hillman, K. A Literature Review on Care at the End-of-Life in the Emergency Department. Emerg. Med. Int. 2012, 2012, 486516. [Google Scholar] [CrossRef] [PubMed]
- Grudzen, C.R.; Richardson, L.D.; Hopper, S.S.; Ortiz, J.M.; Whang, C.; Morrison, R.S. Does Palliative Care Have a Future in the Emergency Department? Discussions with Attending Emergency Physicians. J. Pain Symptom Manag. 2011, 43, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Verhoef, M.-J.; De Nijs, E.J.M.; Ootjers, C.S.; Fiocco, M.; Fogteloo, A.J.; Heringhaus, C.; Marijnen, C.A.M.; Horeweg, N.; Van Der Linden, Y.M. End-of-Life Trajectories of Patients With Hematological Malignancies and Patients With Advanced Solid Tumors Visiting the Emergency Department: The Need for a Proactive Integrated Care Approach. Am. J. Hosp. Palliat. Med. 2019, 37, 692–700. [Google Scholar] [CrossRef] [Green Version]
- Stone, S.C.; Mohanty, S.; Grudzen, C.R.; Shoenberger, J.; Asch, S.; Kubricek, K.; Lorenz, K.A. Emergency Medicine Physicians’ Perspectives of Providing Palliative Care in an Emergency Department. J. Palliat. Med. 2011, 14, 1333–1338. [Google Scholar] [CrossRef]
- Meier, D.E.; Beresford, L. Fast Response is Key to Partnering with the Emergency Department. J. Palliat. Med. 2007, 10, 641–645. [Google Scholar] [CrossRef]
- Lamba, S.; Nagurka, R.; Zielinski, A.; Scott, S.R. Palliative Care Provision in the Emergency Department: Barriers Reported by Emergency Physicians. J. Palliat. Med. 2013, 16, 143–147. [Google Scholar] [CrossRef]
- Aldridge, M.D.; Hasselaar, J.; Garralda, E.; van der Eerden, M.; Stevenson, D.; McKendrick, K.; Centeno, C.; Meier, D.E. Education, implementation, and policy barriers to greater integration of palliative care: A literature review. Palliat. Med. 2015, 30, 224–239. [Google Scholar] [CrossRef]
- Rivera, M.R.; Torres, F.S. Lack of training and Comfort level with Provision of Palliative Care in Puerto Rican Emergency Departments. Bol. Asoc. Med. Puerto Rico 2015, 107, 92–96. [Google Scholar]
- Douplat, M.; Berthiller, J.; Schott, A.M.; Potinet, V.; Le Coz, P.; Tazarourte, K.; Jacquin, L. Difficulty of the decision-making process in emergency departments for end-of-life patients. J. Eval. Clin. Pract. 2019, 25, 1193–1199. [Google Scholar] [CrossRef]
- Bailey, C.J.; Murphy, R.; Porock, D. Dying cases in emergency places: Caring for the dying in emergency departments. Soc. Sci. Med. 2011, 73, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Koh, M.Y.H.; Lee, J.F.; Montalban, S.; Foo, C.L.; Hum, A.Y.M. ED-PALS: A Comprehensive Palliative Care Service for Oncology Patients in the Emergency Department. Am. J. Hosp. Palliat. Med. 2019, 36, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Cortés, M.D.M.; Granero-Molina, J.; Hernández-Padilla, J.M.; Rodríguez, R.P.; Casado, M.C.; Fernández-Sola, C. Promoting dignified end-of-life care in the emergency department: A qualitative study. Int. Emerg. Nurs. 2017, 37, 23–28. [Google Scholar] [CrossRef] [PubMed]
- George, N.R.; Kryworuchko, J.; Hunold, K.M.; Ouchi, K.; Berman, A.; Wright, R.; Grudzen, C.R.; Kovalerchik, O.; LeFebvre, E.M.; Lindor, R.A.; et al. Shared Decision Making to Support the Provision of Palliative and End-of-Life Care in the Emergency Department: A Consensus Statement and Research Agenda. Acad. Emerg. Med. 2016, 23, 1394–1402. [Google Scholar] [CrossRef] [PubMed]
- Reuter, Q.; Marshall, A.; Zaidi, H.; Sista, P.; Powell, E.S.; McCarthy, D.M.; Dresden, S.M. Emergency Department-Based Palliative Interventions: A Novel Approach to Palliative Care in the Emergency Department. J. Palliat. Med. 2019, 22, 649–655. [Google Scholar] [CrossRef] [PubMed]



| Group | Interview Method | Participants’ Role | Number Recruited (Total) | Age in Years, Median (Interquartile Range) |
|---|---|---|---|---|
| Physicians from emergency departments | FGD (Session 1) Institution 1 | EM physician | 6 | 32.5 (29–40) |
| Non-EM physician | 0 | |||
| FGD (Session 2) Institution 2 | EM physician | 6 | 40.5 (31–50) | |
| Non-EM physician | 0 | |||
| FGD (Session 3) Institution 3 | EM physician | 4 | 37.5 (36–40) | |
| Non-EM physician | 1 | |||
| Nurses from emergency departments | FGD (Session 4) Institution 1 | Nursing managers/clinicians | 5 | 35.0 (32–36) |
| Staff nurses | 1 | |||
| FGD (Session 5) Institution 2 | Nursing managers/clinicians | 2 | 33.0 (31–36) | |
| Staff nurses | 4 | |||
| FGD (Session 6) Institution 3 | Nursing managers/clinicians | 2 | 32.0 (30–39) | |
| Staff nurses | 5 | |||
| Healthcare professionals from community settings | FGD (Session 7) | Family physician in private practice | 2 | 35.0 (35–42) |
| Family physician in polyclinic | 1 | |||
| Physician in community hospital | 2 | |||
| FGD (Session 8) | Family physician in private practice | 1 | 40.5 (38–45) | |
| Physician in nursing home | 2 | |||
| Physician in hospice care | 1 | |||
| Nurse in hospice home care | 2 | |||
| FGD (Session 9) | Family physician in private practice | 2 | 46.5 (37–54) | |
| Physician in nursing home | 1 | |||
| Physician in hospice care | 1 | |||
| Nurse in hospice home care | 1 | |||
| Next-of-kin of patients at end of life | One-on-one semi-structured interviews | Children of patients at end of life | 5 | 57.0 (46–58) a |
| In-laws of patients at end of life | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tiah, L.; Chua, M.T.; Kuan, W.S.; Tan, A.; Tay, E.; Yash Pal, R.; Dong, C. Perspectives towards End-of-Life Care in the Emergency Department of Tertiary Public Hospitals—A Qualitative Analysis. Medicina 2023, 59, 456. https://doi.org/10.3390/medicina59030456
Tiah L, Chua MT, Kuan WS, Tan A, Tay E, Yash Pal R, Dong C. Perspectives towards End-of-Life Care in the Emergency Department of Tertiary Public Hospitals—A Qualitative Analysis. Medicina. 2023; 59(3):456. https://doi.org/10.3390/medicina59030456
Chicago/Turabian StyleTiah, Ling, Mui Teng Chua, Win Sen Kuan, Alina Tan, Eileen Tay, Rakhee Yash Pal, and Chaoyan Dong. 2023. "Perspectives towards End-of-Life Care in the Emergency Department of Tertiary Public Hospitals—A Qualitative Analysis" Medicina 59, no. 3: 456. https://doi.org/10.3390/medicina59030456