
The Management of Postoperative Cognitive Dysfunction in Cirrhotic Patients: An Overview of the Literature
 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
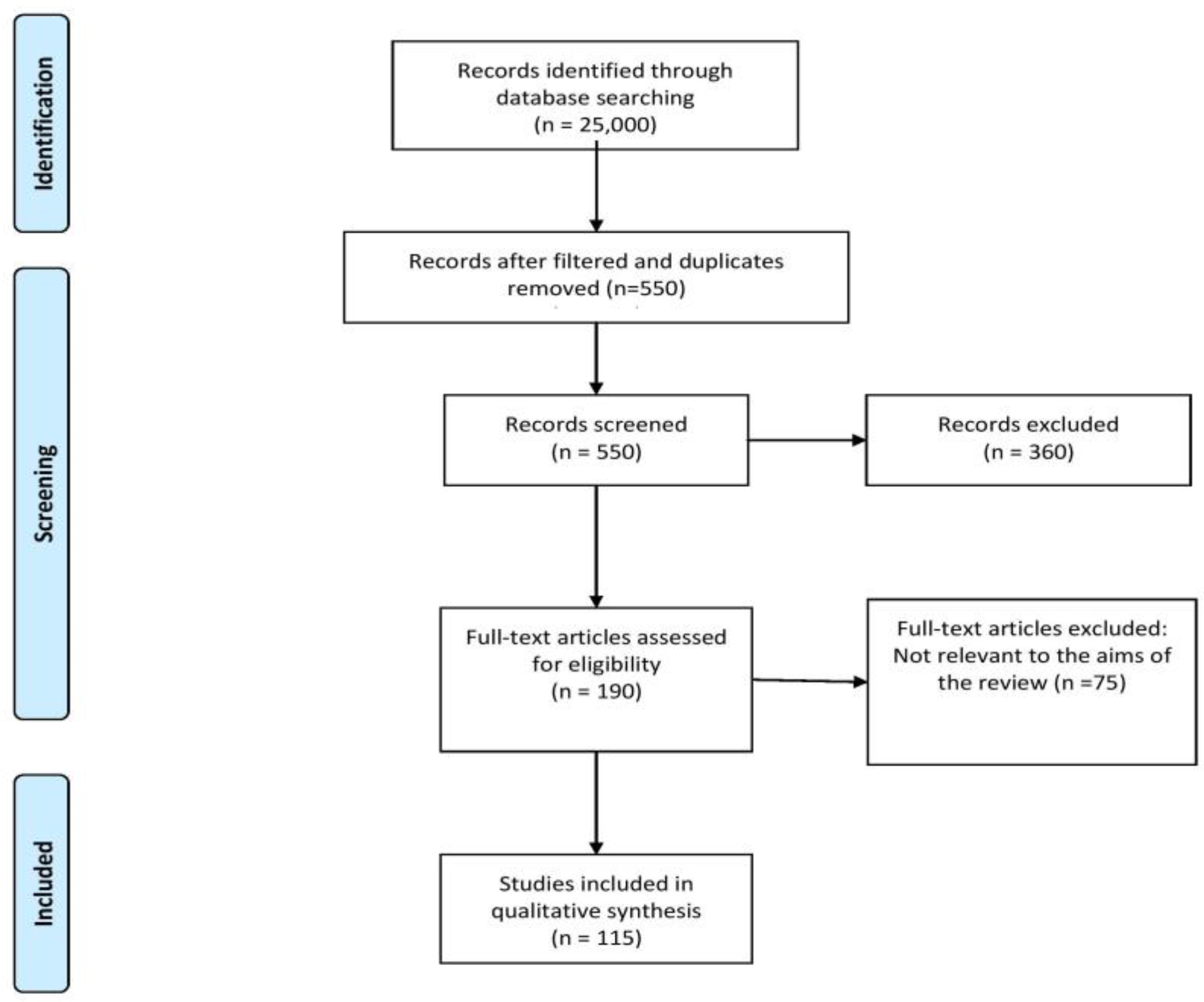
2. Methodology
3. Perioperative Cognitive Dysfunction Management in Cirrhotic Patients
3.1. Preoperative Management of Cognitive Dysfunction in Cirrhotic Patients
3.1.1. Pathophysiologic Mechanisms of Cognitive Impairment in Cirrhotic Patients
3.1.2. Preoperative Assessment of Cognitive Dysfunction in Cirrhotic Patients
3.2. Intraoperative Management of Cognitive Dysfunction in the Cirrhotic Patient
3.3. Postoperative Management of Cognitive Dysfunction in the Cirrhotic Patient
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kotekar, N.; Shenkar, A.; Nagaraj, R. Postoperative Cognitive Dysfunction—Current Preventive Strategies. Clin. Interv. Aging 2018, 13, 2267–2273. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, I.; Prabhakar, H.; Mahajan, C. Postoperative Cognitive Dysfunction. Indian J. Crit. Care Med. 2019, 23, S162–S164. [Google Scholar] [CrossRef]
- Moller, J.T.; Cluitmans, P.; Rasmussen, L.S.; Houx, P.; Rasmussen, H.; Canet, J.; Rabbitt, P.; Jolles, J.; Larsen, K.; Hanning, C.D.; et al. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet 1998, 351, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Silbert, B.S.; Evered, L.A.; Scott, D.A. Incidence of Postoperative Cognitive Dysfunction after General or Spinal Anaesthesia for Extracorporeal Shock Wave Lithotripsy. Br. J. Anaesth. 2014, 113, 784–791. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borozdina, A.; Porcella, L.; Bilotta, F. Postoperative Cognitive Dysfunction. In Essentials of Neuroanesthesia; Elsevier: Amsterdam, The Netherlands, 2017; pp. 661–667. [Google Scholar] [CrossRef]
- Aldridge, D.R.; Tranah, E.J.; Shawcross, D.L. Pathogenesis of hepatic encephalopathy: Role of ammonia and systemic inflammation. J. Clin. Exp. Hepatol. 2015, 5 (Suppl. 1), S7–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coltart, I.; Tranah, T.H.; Shawcross, D.L. Inflammation and Hepatic Encephalopathy. Arch. Biochem. Biophys. 2013, 536, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Bosoi, C.R.; Rose, C.F. Identifying the Direct Effects of Ammonia on the Brain. Metab. Brain Dis. 2009, 24, 95–102. [Google Scholar] [CrossRef] [Green Version]
- Shawcross, D.L.; Shabbir, S.S.; Taylor, N.J.; Hughes, R.D. Ammonia and the Neutrophil in the Pathogenesis of Hepatic Encephalopathy in Cirrhosis. Hepatology 2010, 51, 1062–1069. [Google Scholar] [CrossRef]
- Hadjihambi, A.; Arias, N.; Sheikh, M.; Jalan, R. Hepatic Encephalopathy: A Critical Current Review. Hepatol. Int. 2018, 12, 135–147. [Google Scholar] [CrossRef] [Green Version]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic Encephalopathy—Definition, Nomenclature, Diagnosis, and Quantification: Final Report of the Working Party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef]
- López-Franco, Ó.; Morin, J.-P.; Cortés-Sol, A.; Molina-Jiménez, T.; del Moral, D.I.; Flores-Muñoz, M.; Roldán-Roldán, G.; Juárez-Portilla, C.; Zepeda, R.C. Cognitive Impairment After Resolution of Hepatic Encephalopathy: A Systematic Review and Meta-Analysis. Front. Neurosci. 2021, 15, 579263. [Google Scholar] [CrossRef]
- Isac, T.; Isac, S.; Ioanitescu, S.; Mihaly, E.; Tanasescu, M.-D.; Balan, D.; Tulin, A.; Iliescu, L. Dynamics of Serum A-fetoprotein in Viral Hepatitis C without Hepatocellular Carcinoma. Exp. Ther. Med. 2021, 22, 749. [Google Scholar] [CrossRef] [PubMed]
- Isac, T.; Isac, S.; Rababoc, R.; Cotorogea, M.; Iliescu, L. Epigenetics in Inflammatory Liver Diseases: A Clinical Perspective (Review). Exp. Ther. Med. 2022, 23, 366. [Google Scholar] [CrossRef]
- Ahluwalia, V.; Wade, J.B.; Heuman, D.M.; Hammeke, T.A.; Sanyal, A.J.; Sterling, R.K.; Stravitz, R.T.; Luketic, V.; Siddiqui, M.S.; Puri, P.; et al. Enhancement of Functional Connectivity, Working Memory and Inhibitory Control on Multi-Modal Brain MR Imaging with Rifaximin in Cirrhosis: Implications for the Gut-Liver-Brain Axis. Metab. Brain Dis. 2014, 29, 1017–1025. [Google Scholar] [CrossRef] [PubMed]
- Rovira, A.; Córdoba, J.; Raguer, N.; Alonso, J. Magnetic Resonance Imaging Measurement of Brain Edema in Patients with Liver Disease: Resolution after Transplantation. Curr. Opin. Neurol. 2002, 15, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.J.; Zhong, J.; Lu, G.M. Multimodality MR imaging findings of low-grade brain edema in hepatic encephalopathy. Am. J. Neuroradiol. 2013, 34, 707–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teperman, L.W. Impact of Pretransplant Hepatic Encephalopathy on Liver Posttransplantation Outcomes. Int. J. Hepatol. 2013, 2013, 952828. [Google Scholar] [CrossRef] [Green Version]
- Ardizzone, G.; Arrigo, A.; Schellino, M.M.; Stratta, C.; Valzan, S.; Skurzak, S.; Andruetto, P.; Panio, A.; Ballaris, M.A.; Lavezzo, B.; et al. Neurological Complications of Liver Cirrhosis and Orthotopic Liver Transplant. Transplant. Proc. 2006, 38, 789–792. [Google Scholar] [CrossRef]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.P.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the Management of Patients with Decompensated Cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [Green Version]
- Bleszynski, M.S.; Bressan, A.K.; Joos, E.; Morad Hameed, S.; Ball, C.G. Acute care and emergency general surgery in patients with chronic liver disease: How can we optimize perioperative care? A review of the literature. World J. Emerg. Surg. 2018, 13, 32. [Google Scholar] [CrossRef]
- Rai, R.; Nagral, S.; Nagral, A. Surgery in a Patient with Liver Disease. J. Clin. Exp. Hepatol. 2012, 2, 238–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newman, K.L.; Johnson, K.M.; Cornia, P.B.; Wu, P.; Itani, K.; Ioannou, G.N. Perioperative Evaluation and Management of Patients with Cirrhosis: Risk Assessment, Surgical Outcomes, and Future Directions. Clin. Gastroenterol. Hepatol. 2020, 18, 2398–2414. [Google Scholar] [CrossRef] [PubMed]
- Bhangui, P.; Laurent, A.; Amathieu, R.; Azoulay, D. Assessment of Risk for Non-Hepatic Surgery in Cirrhotic Patients. J. Hepatol. 2012, 57, 874–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teh, S.H.; Nagorney, D.M.; Stevens, S.R.; Offord, K.P.; Therneau, T.M.; Plevak, D.J.; Talwalkar, J.A.; Kim, W.R.; Kamath, P.S. Risk Factors for Mortality After Surgery in Patients with Cirrhosis. Gastroenterology 2007, 132, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Csikesz, N.G.; Nguyen, L.N.; Tseng, J.F.; Shah, S.A. Nationwide Volume and Mortality after Elective Surgery in Cirrhotic Patients. J. Am. Coll. Surg. 2009, 208, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Abbas, N.; Makker, J.; Abbas, H.; Balar, B. Perioperative Care of Patients with Liver Cirrhosis: A Review. Health Serv. Insights 2017, 10, 1178632917691270. [Google Scholar] [CrossRef] [Green Version]
- Wetterkamp, M.; van Beekum, C.J.; Willis, M.A.; Glowka, T.R.; Manekeller, S.; Fimmers, R.; Praktiknjo, M.; Chang, J.; Kalff, J.C.; Vilz, T.O. Risk Factors for Postoperative Morbidity and Mortality after Small Bowel Surgery in Patients with Cirrhotic Liver Disease-A Retrospective Analysis of 76 Cases in a Tertiary Center. Biology 2020, 9, 349. [Google Scholar] [CrossRef]
- Andraus, W.; Pinheiro, R.S.; Lai, Q.; Haddad, L.B.P.; Nacif, L.S.; D’Albuquerque, L.A.C.; Lerut, J. Abdominal Wall Hernia in Cirrhotic Patients: Emergency Surgery Results in Higher Morbidity and Mortality Visceral and General Surgery. BMC Surg. 2015, 15, 65. [Google Scholar] [CrossRef]
- Ghaferi, A.A.; Mathur, A.K.; Sonnenday, C.J.; Dimick, J.B. Adverse Outcomes in Patients with Chronic Liver Disease Undergoing Colorectal Surgery. Ann. Surg. 2010, 252, 345–350. [Google Scholar] [CrossRef]
- Bell, C.L.; Rohan Jeyarajah, D. Management of the Cirrhotic Patient That Needs Surgery Opinion Statement. Curr. Treat. Options Gastroenterol. 2005, 8, 473–480. [Google Scholar] [CrossRef]
- Aminnejad, R.; Alemi, F.; Safari, S.; Hormati, A.; Ghadir, M.R.; Saeedi, M.; Afifian, M. Preoperative Considerations in Patients with Advanced Liver Disease. Middle East J. Dig. Dis. 2019, 11, 238–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Dong, Q.; Zhang, R.; Zhou, S.; Li, L.; Cheng, K.; Kong, R.; Yu, Q.; Xu, S.; Li, J.; et al. Cerebral Hemodynamics and Cognitive Function in Cirrhotic Patients with Hepatic Encephalopathy. Gastroenterol. Res. Pract. 2016, 2016, 8485032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feinkohl, I.; Winterer, G.; Spies, C.D.; Pischon, T. Cognitive Reserve and the Risk of Postoperative Cognitive Dysfunction—A Systematic Review and Meta-Analysis. Dtsch. Arztebl. Int. 2017, 114, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Møller, S.; Henriksen, J.H. Cirrhotic Cardiomyopathy. J. Hepatol. 2010, 53, 179–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjihambi, A.; Cudalbu, C.; Pierzchala, K.; Simicic, D.; Donnelly, C.; Konstantinou, C.; Davies, N.; Habtesion, A.; Gourine, A.V.; Jalan, R.; et al. Abnormal Brain Oxygen Homeostasis in an Animal Model of Liver Disease. JHEP Rep. 2022, 4, 100509. [Google Scholar] [CrossRef]
- Rodríguez-Roisin, R.; Krowka, M.J.; Hervé, P.; Fallon, M.B.; Barberá, J.A.; Cáneva, J.O.; García-Pagán, J.C.; García-Valdecasas, J.C.; Kawut, M.J.; Lebrec, D.; et al. Pulmonary-Hepatic Vascular Disorders (PHD). Eur. Respir. J. 2004, 24, 861–880. [Google Scholar] [CrossRef]
- Hay, J.E. Ascites, Hepatorenal Syndrome, and Encephalopathy. In Mayo Clinic Gastroenterology and Hepatology Board Review, 5th ed.; Hauser, S.C., Ed.; Mayo Clinic Scientific Press: New York, NY, USA, 2014; pp. 284–292. ISBN 9780190209728. [Google Scholar]
- Alessandria, C.; Elia, C.; Mezzabotta, L.; Risso, A.; Andrealli, A.; Spandre, M.; Morgando, A.; Marzano, A.; Rizzetto, M. Prevention of Paracentesis-Induced Circulatory Dysfunction in Cirrhosis: Standard vs Half Albumin Doses. A Prospective, Randomized, Unblinded Pilot Study. Dig. Liver Dis. 2011, 43, 881–886. [Google Scholar] [CrossRef]
- Zhu, S.H.; Ji, M.H.; Gao, D.P.; Li, W.Y.; Yang, J.J. Association between Perioperative Blood Transfusion and Early Postoperative Cognitive Dysfunction in Aged Patients Following Total Hip Replacement Surgery. Ups. J. Med. Sci. 2014, 119, 262–267. [Google Scholar] [CrossRef]
- Ciećko-Michalska, I.; Szczepanek, M.; Słowik, A.; MacH, T. Pathogenesis of Hepatic Encephalopathy. Gastroenterol. Res. Pract. 2012, 2012, 642108. [Google Scholar] [CrossRef]
- Androsova, G.; Krause, R.; Winterer, G.; Schneider, R. Biomarkers of Postoperative Delirium and Cognitive Dysfunction. Front. Aging Neurosci. 2015, 7, 112. [Google Scholar] [CrossRef]
- Merli, M.; Lucidi, C.; Pentassuglio, I.; Giannelli, V.; Giusto, M.; di Gregorio, V.; Pasquale, C.; Nardelli, S.; Lattanzi, B.; Venditti, M.; et al. Increased Risk of Cognitive Impairment in Cirrhotic Patients with Bacterial Infections. J. Hepatol. 2013, 59, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Millwala, F.; Nguyen, G.C.; Thuluvath, P.J. Outcomes of Patients with Cirrhosis Undergoing Non-Hepatic Surgery: Risk Assessment and Management. World J. Gastroenterol. 2007, 13, 4056–4063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiMartini, A.; Chopra, K. The Importance of Hepatic Encephalopathy: Pre-Transplant and Post-Transplant. Liver Transplant. 2009, 15, 121–123. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Schubert, C.M.; Heuman, D.M.; Wade, J.B.; Gibson, D.P.; Topaz, A.; Saeian, K.; Hafeezullah, M.; Bell, D.E.; Sterling, R.K.; et al. Persistence of Cognitive Impairment After Resolution of Overt Hepatic Encephalopathy. Gastroenterology 2010, 138, 2332–2340. [Google Scholar] [CrossRef] [Green Version]
- Riggio, O.; Ridola, L.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Moscucci, F.; Merli, M. Evidence of Persistent Cognitive Impairment After Resolution of Overt Hepatic Encephalopathy. Clin. Gastroenterol. Hepatol. 2011, 9, 181–183. [Google Scholar] [CrossRef]
- Telem, D.A.; Schiano, T.; Goldstone, R.; Han, D.K.; Buch, K.E.; Chin, E.H.; Nguyen, S.Q.; Divino, C.M. Factors That Predict Outcome of Abdominal Operations in Patients with Advanced Cirrhosis. Clin. Gastroenterol. Hepatol. 2010, 8, 451–457. [Google Scholar] [CrossRef]
- Perkins, L.; Jeffries, M.; Patel, T. Utility of Preoperative Scores for Predicting Morbidity After Cholecystectomy in Patients with Cirrhosis. Clin. Gastroenterol. Hepatol. 2004, 2, 1123–1128. [Google Scholar] [CrossRef]
- Northup, P.G.; Wanamaker, R.C.; Lee, V.D.; Adams, R.B.; Berg, C.L. Model for End-Stage Liver Disease (MELD) Predicts Nontransplant Surgical Mortality in Patients with Cirrhosis. Ann. Surg. 2005, 242, 244–251. [Google Scholar] [CrossRef]
- Befeler, A.S.; Palmer, D.E.; Hoffman, M.; Longo, W.; Solomon, H.; di Bisceglie, A.M. The Safety of Intra-Abdominal Surgery in Patients with Cirrhosis Model for End-Stage Liver Disease Score Is Superior to Child-Turcotte-Pugh Classification in Predicting Outcome. Arch. Surg. 2005, 140, 650–655. [Google Scholar] [CrossRef]
- Delis, S.; Bakoyiannis, A.; Madariaga, J.; Bramis, J.; Tassopoulos, N.; Dervenis, C. Laparoscopic Cholecystectomy in Cirrhotic Patients: The Value of MELD Score and ChildPugh Classification in Predicting Outcome. Surg. Endosc. 2010, 24, 407–412. [Google Scholar] [CrossRef]
- Pantiga, C.; Rodrigo, L.R.; Cuesta, M.; Lopez, L.; Arias, J.L. Cognitive Deficits in Patients with Hepatic Cirrhosis and in Liver Transplant Recipients. J. Neuropsychiatry Clin. Neurosci. 2003, 15, 84–89. [Google Scholar] [CrossRef]
- Campagna, F.; Montagnese, S.; Ridola, L.; Senzolo, M.; Schiff, S.; de Rui, M.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Merkel, C.; et al. The Animal Naming Test: An Easy Tool for the Assessment of Hepatic Encephalopathy. Hepatology 2017, 66, 198–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isac, S.; Pavel, B.; Dobre, M.; Milanesi, E.; Matache, I.-M.; Paun, R.-M.; Klimko, A.; Iesanu, M.I.; Droc, G.; Zagrean, A.-M. Does a Single Exposure to General Anesthesia Have a Cumulative Effect on the Developing Brain after Mild Perinatal Asphyxia? Life 2022, 12, 1568. [Google Scholar] [CrossRef]
- Liu, X.; Ji, J.; Zhao, G.Q. General Anesthesia Affecting on Developing Brain: Evidence from Animal to Clinical Research. J. Anesth. 2020, 34, 765–772. [Google Scholar] [CrossRef]
- Maze, M.; Bass, N.M. Anaesthesia and the Hepatobiliary System. In Anesthesia, 5th ed.; Miller, R.D., Ed.; Churchill Livingstone: London, UK, 2000; ISBN 9780443079788. [Google Scholar]
- Friedman, L.S. The Risk of Surgery in Patients with Liver Disease. Hepatology 1999, 29, 1617–1623. [Google Scholar] [CrossRef]
- Rahimzadeh, P.; Safari, S.; Reza Faiz, S.H.; Alavian, S.M. Anesthesia for Patients with Liver Disease. Hepat. Mon. 2014, 14, e19881. [Google Scholar] [CrossRef] [Green Version]
- Vaja, R.; McNicol, L.; Sisley, I. Anaesthesia for Patients with Liver Disease. Contin. Educ. Anaesth. Crit. Care Pain 2010, 10, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Lopez-Delgado, J.C.; Ballus, J.; Esteve, F.; Betancur-Zambrano, N.L.; Corral-Velez, V.; Mañez, R.; Betbese, A.J.; Roncal, J.A.; Javierre, C. Outcomes of Abdominal Surgery in Patients with Liver Cirrhosis. World J. Gastroenterol. 2016, 22, 2657–2667. [Google Scholar] [CrossRef] [PubMed]
- Mcclain, R.L.; Ramakrishna, H.; Iii, S.A.; Cartwright, J.A.; Phar, L.G.W.; Pai, S.-L.; Rodrigues, E.S.; Martin, A.K.; Shine, T.S. Anesthetic Pharmacology and Perioperative Considerations for the End Stage Liver Disease Patient. Curr. Clin. Pharmacol. 2015, 10, 35–46. [Google Scholar] [CrossRef]
- Jipa, M.; Isac, S.; Klimko, A.; Simion-Cotorogea, M.; Martac, C.; Cobilinschi, C.; Droc, G. Opioid-Sparing Analgesia Impacts the Perioperative Anesthetic Management in Major Abdominal Surgery. Medicina 2022, 58, 487. [Google Scholar] [CrossRef] [PubMed]
- Nimmo, S.M.; Harrington, L.S. What Is the Role of Epidural Analgesia in Abdominal Surgery? Contin. Educ. Anaesth. Crit. Care Pain 2014, 14, 224–229. [Google Scholar] [CrossRef]
- Brodier, E.A.; Cibelli, M. Postoperative Cognitive Dysfunction in Clinical Practice. BJA Educ. 2021, 21, 75. [Google Scholar] [CrossRef]
- Rasmussen, L.S.; Johnson, T.; Kuipers, H.M.; Kristensen, D.; Siersma, V.D.; Vila, P.; Jolles, J.; Papaioannou, A.; Abildstrom, H.; Silverstein, J.H.; et al. Does Anaesthesia Cause Postoperative Cognitive Dysfunction? A Randomised Study of Regional versus General Anaesthesia in 438 Elderly Patients. Acta Anaesthesiol. Scand. 2003, 47, 260–266. [Google Scholar] [CrossRef]
- Orhun, G.; Sungur, Z.; Koltka, K.; Karadeniz, M.S.; Yavru, H.A.; Gürvit, H.; Şentürk, M. Comparison of Epidural Analgesia Combined with General Anesthesia and General Anesthesia for Postoperative Cognitive Dysfunction in Elderly Patients. Ulus Travma Acil Cerrahi Derg. 2020, 26, 30–36. [Google Scholar] [CrossRef]
- Berger, M.; Schenning, K.J.; Brown, C.H., IV.; Deiner, S.G.; Whittington, R.A.; Eckenhoff, R.G.; Angst, M.S.; Avramescu, S.; Bekker, A.; Brzezinski, M.; et al. Best Practices for Postoperative Brain Health: Recommendations from the Fifth International Perioperative Neurotoxicity Working Group. Anesth. Analg. 2018, 127, 1406–1413. [Google Scholar] [CrossRef]
- Ologunde, R.; Ma, D. Do Inhalational Anesthetics Cause Cognitive Dysfunction? Acta Anaesthesiol. Taiwan. 2011, 49, 149–153. [Google Scholar] [CrossRef]
- Adembri, C.; Venturi, L.; Tani, A.; Chiarugi, A.; Gramigni, E.; Cozzi, A.; Pancani, T.; de Gaudio, R.A.; Pellegrini-Giampietro, D.E. Neuroprotective Effects of Propofol in Models of Cerebral Ischemia: Inhibition of Mitochondrial Swelling as a Possible Mechanism. Anesthesiology 2006, 104, 80–89. [Google Scholar] [CrossRef] [Green Version]
- Oh, S.K.; Lim, B.G.; Kim, Y.S.; Kim, S.S. Comparison of the Postoperative Liver Function Between Total Intravenous Anesthesia and Inhalation Anesthesia in Patients with Preoperatively Elevated Liver Transaminase Levels: A Retrospective Cohort Study. Ther. Clin. Risk Manag. 2020, 16, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.; Yang, W.; Zhao, G. Effect of Propofol and Inhalation Anesthesia on Postoperative Cognitive Dysfunction in the Elderly: A Meta-Analysis. Nan Fang Yi Ke Da Xue Xue Bao 2012, 32, 1623–1627. [Google Scholar]
- Miller, D.; Lewis, S.R.; Pritchard, M.W.; Schofield-Robinson, O.J.; Shelton, C.L.; Alderson, P.; Smith, A.F. Intravenous versus Inhalational Maintenance of Anaesthesia for Postoperative Cognitive Outcomes in Elderly People Undergoing Non-Cardiac Surgery. Cochrane Database Syst. Rev. 2018, 8, CD012317. [Google Scholar] [CrossRef]
- Qiao, Y.; Feng, H.; Zhao, T.; Yan, H.; Zhang, H.; Zhao, X. Postoperative Cognitive Dysfunction after Inhalational Anesthesia in Elderly Patients Undergoing Major Surgery: The Influence of Anesthetic Technique, Cerebral Injury and Systemic Inflammation. BMC Anesthesiol. 2015, 15, 154. [Google Scholar] [CrossRef] [Green Version]
- Li, W.X.; Luo, R.Y.; Chen, C.; Li, X.; Ao, J.S.; Liu, Y.; Yin, Y.Q. Effects of Propofol, Dexmedetomidine, and Midazolam on Postoperative Cognitive Dysfunction in Elderly Patients: A Randomized Controlled Preliminary Trial. Chin. Med. J. 2019, 132, 437–445. [Google Scholar] [CrossRef]
- Yang, W.; Kong, L.S.; Zhu, X.X.; Wang, R.X.; Liu, Y.; Chen, L.R. Effect of Dexmedetomidine on Postoperative Cognitive Dysfunction and Inflammation in Patients after General Anaesthesia: A PRISMA-Compliant Systematic Review and Meta-Analysis. Medicine 2019, 98, e15383. [Google Scholar] [CrossRef]
- Djaiani, G.; Silverton, N.; Fedorko, L.; Carroll, J.; Styra, R.; Rao, V.; Katznelson, R. Dexmedetomidine versus Propofol Sedation Reduces Delirium after Cardiac Surgery: A Randomized Controlled Trial. Anesthesiology 2016, 124, 362–368. [Google Scholar] [CrossRef]
- Deiner, S.; Luo, X.; Lin, H.M.; Sessler, D.I.; Saager, L.; Sieber, F.E.; Lee, H.B.; Sano, M. Intraoperative Infusion of Dexmedetomidine for Prevention of Postoperative Delirium and Cognitive Dysfunction in Elderly Patients Undergoing Major Elective Noncardiac Surgery: A Randomized Clinical Trial. JAMA Surg. 2017, 152, e171505. [Google Scholar] [CrossRef]
- Soleimanpour, H.; Nia, K.S.; Sanaie, S.; Ghojazadeh, M.; Alavian, S.M. Use of Dexmedetomidine in Liver Disease: A Systematic Review and Meta-Analysis. Hepat. Mon. 2019, 19, 98530. [Google Scholar] [CrossRef] [Green Version]
- Hovaguimian, F.; Tschopp, C.; Beck-Schimmer, B.; Puhan, M. Intraoperative Ketamine Administration to Prevent Delirium or Postoperative Cognitive Dysfunction: A Systematic Review and Meta-Analysis. Acta Anaesthesiol. Scand. 2018, 62, 1182–1193. [Google Scholar] [CrossRef] [Green Version]
- Avidan, M.S.; Maybrier, H.R.; ben Abdallah, A.; Jacobsohn, E.; Vlisides, P.E.; Pryor, K.O.; Veselis, R.A.; Grocott, H.P.; Emmert, D.A.; Rogers, E.M.; et al. Intraoperative Ketamine for Prevention of Postoperative Delirium or Pain after Major Surgery in Older Adults: An International, Multicentre, Double-Blind, Randomised Clinical Trial. Lancet 2017, 390, 267–275. [Google Scholar] [CrossRef]
- Lavand’homme, P.; Estebe, J.P. Opioid-Free Anesthesia: A Different Regard to Anesthesia Practice. Curr. Opin. Anaesthesiol. 2018, 31, 556–561. [Google Scholar] [CrossRef]
- Batistaki, C.; Riga, M.; Zafeiropoulou, F.; Lyrakos, G.; Kostopanagiotou, G.; Matsota, P. Effect of Sugammadex versus Neostigmine/Atropine Combination on Postoperative Cognitive Dysfunction after Elective Surgery. Anaesth. Intensive Care 2017, 45, 581–588. [Google Scholar] [CrossRef] [Green Version]
- Chan, M.T.V.; Cheng, B.C.P.; Lee, T.M.C.; Gin, T. BIS-Guided Anesthesia Decreases Postoperative Delirium and Cognitive Decline. J. Neurosurg. Anesthesiol. 2013, 25, 33–42. [Google Scholar] [CrossRef]
- Quan, C.; Chen, J.; Luo, Y.; Zhou, L.; He, X.; Liao, Y.; Chou, J.; Guo, Q.; Chen, A.F.; Wen, O. BIS-Guided Deep Anesthesia Decreases Short-Term Postoperative Cognitive Dysfunction and Peripheral Inflammation in Elderly Patients Undergoing Abdominal Surgery. Brain Behav. 2019, 9, e01238. [Google Scholar] [CrossRef] [Green Version]
- Wang, C.H.; Chen, C.L.; Cheng, K.W.; Huang, C.J.; Chen, K.H.; Wang, C.C.; Concejero, A.M.; Cheng, Y.F.; Huang, T.L.; Chiu, K.W.; et al. Bispectral Index Monitoring in Healthy, Cirrhotic, and End-Stage Liver Disease Patients Undergoing Hepatic Operation. Transplant Proc. 2008, 40, 2489–2491. [Google Scholar] [CrossRef]
- Li, L.Q.; Wang, C.; Fang, M.D.; Xu, H.Y.; Lu, H.L.; Zhang, H.Z. Effects of Dexamethasone on Post-Operative Cognitive Dysfunction and Delirium in Adults Following General Anaesthesia: A Meta-Analysis of Randomised Controlled Trials. BMC Anesthesiol. 2019, 19, 113. [Google Scholar] [CrossRef] [Green Version]
- Espitalier, F.; Idrissi, M.; Fortier, A.; Bélanger, M.È.; Carrara, L.; Dakhlallah, S.; Rivard, C.; Brulotte, V.; Zaphiratos, V.; Loubert, C.; et al. Impact of Nociception Level (NOL) Index Intraoperative Guidance of Fentanyl Administration on Opioid Consumption, Postoperative Pain Scores and Recovery in Patients Undergoing Gynecological Laparoscopic Surgery. A Randomized Controlled Trial. J. Clin. Anesth. 2021, 75, 110497. [Google Scholar] [CrossRef]
- Meijer, F.; Honing, M.; Roor, T.; Toet, S.; Calis, P.; Olofsen, E.; Martini, C.; van Velzen, M.; Aarts, L.; Niesters, M.; et al. Reduced Postoperative Pain Using Nociception Level-Guided Fentanyl Dosing during Sevoflurane Anaesthesia: A Randomised Controlled Trial. Br. J. Anaesth. 2020, 125, 1070–1078. [Google Scholar] [CrossRef]
- Plourde, G. Auditory Evoked Potentials. Best Pract. Res. Clin. Anaesthesiol. 2006, 20, 129–139. [Google Scholar] [CrossRef]
- Jildenstal, P.K.; Hallén, J.L.; Rawal, N.; Gupta, A.; Berggren, L. Effect of Auditory Evoked Potential-Guided Anaesthesia on Consumption of Anaesthetics and Early Postoperative Cognitive Dysfunction: A Randomised Controlled Trial. Eur. J. Anaesthesiol. 2011, 28, 213–219. [Google Scholar] [CrossRef]
- Murkin, J.M.; Arango, M. Near-Infrared Spectroscopy as an Index of Brain and Tissue Oxygenation. Br. J. Anaesth. 2009, 103 (Suppl. 1), i3–i13. [Google Scholar] [CrossRef] [Green Version]
- Jing, Z.; Wu, D. Application of Regional Cerebral Oxygen Saturation Monitoring with Near-Infrared Spectroscopy in Peri-Anesthesia Management of Elderly Hypertensive Patients Undergoing Shoulder Arthroscopic Surgery. Am. J. Transl. Res. 2021, 13, 5568–5574. [Google Scholar]
- Chatzizacharias, N.A.; Bradley, J.A.; Harper, S.; Butler, A.; Jah, A.; Huguet, E.; Praseedom, R.K.; Allison, M.; Gibbs, P. Successful Surgical Management of Ruptured Umbilical Hernias in Cirrhotic Patients. World J. Gastroenterol. 2015, 21, 3109–3113. [Google Scholar] [CrossRef]
- Harmouch, M.A.; Hobeika, M.J. Perioperative Management of the Cirrhotic Patient. In Common Problems in Acute Care Surgery; Moore, L.J., Turner, K.L., Todd, S.R., Eds.; Springer International Publishing: New York, NY, USA, 2017; ISBN 978-3-319-42790-4. [Google Scholar]
- Umapathy, S.; Dhiman, R.K.; Grover, S.; Duseja, A.; Chawla, Y.K. Persistence of Cognitive Impairment after Resolution of Overt Hepatic Encephalopathy. Am. J. Gastroenterol. 2014, 109, 1011–1019. [Google Scholar] [CrossRef]
- Saleh, Z.M.; Solano, Q.P.; Louissaint, J.; Jepsen, P.; Tapper, E.B. The Incidence and Outcome of Postoperative Hepatic Encephalopathy in Patients with Cirrhosis. United Eur. Gastroenterol. J. 2021, 9, 672. [Google Scholar] [CrossRef]
- You, D.D.; Choi, G.S.; Kim, J.M.; Kwon, C.H.D.; Joh, J.W.; Lee, S.K. Long-Term Outcomes for Liver Transplant Recipients in Terms of Hepatic Encephalopathy. Transplant. Proc. 2017, 49, 1425–1429. [Google Scholar] [CrossRef]
- Moore, K.A.; McL Jones, R.; Burrows, G.D. Quality of Life and Cognitive Function of Liver Transplant Patients: A Prospective Study. Liver Transplant. 2000, 6, 633–642. [Google Scholar] [CrossRef]
- Riether, A.M.; Smith, S.L.; Lewison, B.J.; Cotsonis, G.A.; Epstein, C.M. Quality-of-Life Changes and Psychiatric and Neurocognitive Outcome after Heart and Liver Transplantation. Transplantation 1992, 54, 444–450. [Google Scholar] [CrossRef]
- Hopp, A.E.; Dirks, M.; Petrusch, C.; Goldbecker, A.; Tryc, A.B.; Barg-Hock, H.; Strassburg, C.; Klempnauer, J.; Weissenborn, K.; Pflugrad, H. Hepatic Encephalopathy Is Reversible in the Long Term After Liver Transplantation. Liver Transpl. 2019, 25, 1661–1672. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Wang, L.; Wu, F.; Rong, W.; Liu, Y.; Zhang, K.; Wu, J. Enhanced Recovery after Surgery Strategy for Cirrhosis Patients Undergoing Hepatectomy: Experience in a Single Research Center. Ann. Surg. Treat. Res. 2020, 98, 224. [Google Scholar] [CrossRef]
- Hirota, K. Preoperative Management and Postoperative Delirium: The Possibility of Neuroprehabilitation Using Virtual Reality. J. Anesth. 2020, 34, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Cacau, L.d.A.P.; Oliveira, G.U.; Maynard, L.G.; de Araújo Filho, A.A.; da Silva Junior, W.M.; CerqueriaNeto, M.L.; Antoniolli, A.R.; Santana-Filho, V.J. The Use of the Virtual Reality as Intervention Tool in the Postoperative of Cardiac Surgery. Rev. Bras. Cir. Cardiovasc. 2013, 28, 281–289. [Google Scholar] [CrossRef] [Green Version]
- Heyer, E.J.; Sharma, R.; Winfree, C.J.; Mocco, J.; McMahon, D.J.; McCormick, P.A.; Quest, D.O.; McMurtry, J.G.; Riedel, C.J.; Lazar, R.M.; et al. Severe Pain Confounds Neuropsychological Test Performance. J. Clin. Exp. Neuropsychol. 2000, 22, 633. [Google Scholar] [CrossRef]
- Zywiel, M.G.; Prabhu, A.; Perruccio, A.V.; Gandhi, R. The Influence of Anesthesia and Pain Management on Cognitive Dysfunction after Joint Arthroplasty: A Systematic Review. Clin. Orthop. Relat. Res. 2014, 472, 1453–1466. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Wang, Y.; Wu, H.; Lei, L.; Xu, S.; Shen, X.; Guo, X.; Shen, R.; Xia, X.; Liu, Y.; et al. Postoperative Cognitive Dysfunction: Current Developments in Mechanism and Prevention. Med. Sci. Monit. 2014, 20, 1908–1912. [Google Scholar] [CrossRef] [Green Version]
- Fong, H.K.; Sands, L.P.; Leung, J.M. The Role of Postoperative Analgesia in Delirium and Cognitive Decline in Elderly Patients: A Systematic Review. Anesth. Analg. 2006, 102, 1255–1266. [Google Scholar] [CrossRef]
- Evered, L.A.; Silbert, B.S. Postoperative Cognitive Dysfunction and Noncardiac Surgery. Anesth. Analg. 2018, 127, 496–505. [Google Scholar] [CrossRef]
- He, H.; Wen, L.-J.; Cui, C.; Li, D.-R.; Teng, J.-F. S100β Protein Affects POCD in Patients Who Underwent Single Valve Replacement Surgery. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 2192–2198. [Google Scholar]
- Huang, S.; Hu, H.; Cai, Y.H.; Hua, F. Effect of Parecoxib in the Treatment of Postoperative Cognitive Dysfunction: A Systematic Review and Meta-Analysis. Medicine 2019, 98, e13812. [Google Scholar] [CrossRef]
- Liu, X.; Yu, Y.; Zhu, S. Inflammatory Markers in Postoperative Delirium (POD) and Cognitive Dysfunction (POCD): A Meta-Analysis of Observational Studies. PLoS ONE 2018, 13, e0195659. [Google Scholar] [CrossRef] [Green Version]
- Leung, J.M.; Sands, L.P.; Chen, N.; Ames, C.; Berven, S.; Bozic, K.; Burch, S.; Chou, D.; Covinsky, K.; Deviren, V.; et al. Perioperative Gabapentin Does Not Reduce Postoperative Delirium in Older Surgical Patients: A Randomized Clinical Trial. Anesthesiology 2017, 127, 633–644. [Google Scholar] [CrossRef]
- Peskind, E.R.; Potkin, S.G.; Pomara, N.; Ott, B.R.; Graham, S.M.; Olin, J.T.; McDonald, S. Memantine Treatment in Mild to Moderate Alzheimer Disease: A 24-Week Randomized, Controlled Trial. Am. J. Geriatr. Psychiatry 2006, 14, 704–715. [Google Scholar] [CrossRef]
- Hagsten, B.; Svensson, O.; Gardulf, A. Early Individualized Postoperative Occupational Therapy Training in 100 Patients Improves ADL after Hip Fracture: A Randomized Trial. Acta Orthop. Scand. 2004, 75, 177–183. [Google Scholar] [CrossRef] [Green Version]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ingustu, D.-G.; Pavel, B.; Paltineanu, S.-I.; Mihai, D.-I.; Cotorogea-Simion, M.; Martac, C.; Florescu, M.-M.; Cobilinschi, C.; Isac, S.; Droc, G. The Management of Postoperative Cognitive Dysfunction in Cirrhotic Patients: An Overview of the Literature. Medicina 2023, 59, 465. https://doi.org/10.3390/medicina59030465
Ingustu D-G, Pavel B, Paltineanu S-I, Mihai D-I, Cotorogea-Simion M, Martac C, Florescu M-M, Cobilinschi C, Isac S, Droc G. The Management of Postoperative Cognitive Dysfunction in Cirrhotic Patients: An Overview of the Literature. Medicina. 2023; 59(3):465. https://doi.org/10.3390/medicina59030465
Chicago/Turabian StyleIngustu, Daiana-Georgiana, Bogdan Pavel, Silvia-Ioana Paltineanu, Diana-Irene Mihai, Mihail Cotorogea-Simion, Cristina Martac, Madalina-Marieta Florescu, Cristian Cobilinschi, Sebastian Isac, and Gabriela Droc. 2023. "The Management of Postoperative Cognitive Dysfunction in Cirrhotic Patients: An Overview of the Literature" Medicina 59, no. 3: 465. https://doi.org/10.3390/medicina59030465