
Relationship between Deep Marginal Elevation and Periodontal Parameters: A Systematic Review
 , and
, and
Abstract
:1. Introduction
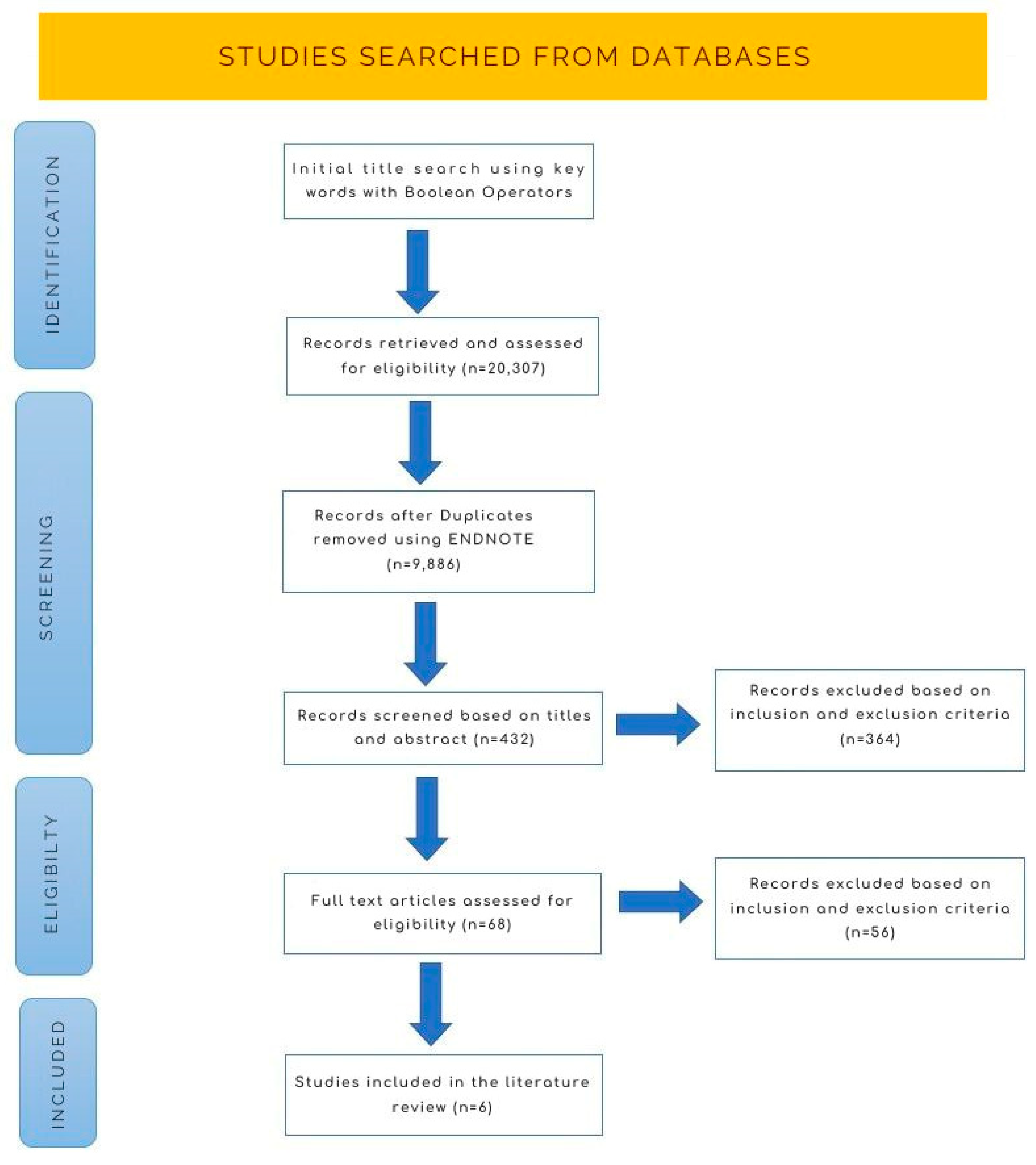
2. Materials and Methods
2.1. Eligibility Criteria
- Studies conducted between 2010 and 2023;
- Articles and books directly related to the research question and objectives;
- Studies indexed in Embase, The Cochrane Library, MEDLINE-PubMed and Google Scholar.
2.2. Exclusion Criteria
- Animal and in vitro studies;
- Conference abstracts and non-peer-reviewed sources;
- Studies not relevant to the research question;
- Studies with a high risk of bias or poor methodological quality.
2.3. Search Strategy
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Viswanath, D.R.A. Biomimetics in dentistry—A review. Indian J. Res. Pharm. Biotechnol. 2014, 2, 1384–1388. [Google Scholar]
- Chun, E.P.; de Andrade, G.S.; Grassi, E.D.A.; Garaicoa, J.; Garaicoa-Pazmino, C. Impact of Deep Margin Elevation Procedures Upon Periodontal Parameters: A Systematic Review. Eur. J. Prosthodont. Restor. Dent. 2023, 31, 10–21. [Google Scholar] [PubMed]
- Ayari, N.G.I.; Soua, S.N.; Moussa, A.B.; Nouira, Z.; Hadyaoui, D.; Harzallah, B.; Cherif, M. Deep margin elevation for indirect bonded restorations: A case report. Int. Dent. J. 2021, 71, 550. [Google Scholar] [CrossRef]
- Aldakheel, M.A.K.; Alnafissah, S.A.R.; Alqahtani, A.; Almuhtab, N. Deep Margin Elevation: Current Concepts and Clinical Considerations: A Review. Medicina 2022, 58, 1482. [Google Scholar] [CrossRef] [PubMed]
- Nugala, B.; Kumar, B.S.; Sahitya, S.; Krishna, P.M. Biologic width and its importance in periodontal and restorative dentistry. J. Conserv. Dent. 2012, 15, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Yamazaki, K. Periodontal manifestations of systemic diseases and developmental and acquired conditions: Consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S237–S248. [Google Scholar] [CrossRef]
- Gargiulo, A.W.W.F.; Orban, B. Dimensions and relations of the dentogingival junction in humans. J. Periodontol. 1961, 32, 261–267. [Google Scholar] [CrossRef]
- Eggmann, F.; Ayub, J.M.; Conejo, J.; Blatz, M.B. Deep margin elevation-Present status and future directions. J. Esthet. Restor. Dent. 2023, 35, 26–47. [Google Scholar] [CrossRef]
- Sarfati, A.; Tirlet, G. Deep Margin Elevation Versus Crown Lengthening: Biologic Width Revisited. Int. J. Esthet. Dent. 2018, 13, 334–356. [Google Scholar]
- Alghulikah, K.A.N.; Al Ibrahim, H.S.; AlYamany, R.M.; Alqahtani, N.H. Deep margin elevation for indirect restorations: A systematic review. J. Pharm. Res. Int. 2021, 33, 23–30. [Google Scholar] [CrossRef]
- Babkair, H.A. The Impact of Deep Marginal Elevation on the Periodontium: A Review Article. Sci. Arch. Dent. Sci. 2023, 6, 25–34. [Google Scholar]
- Magne, P.S.R. Deep margin elevation: A paradigm shift. Am. J. Esthet. Dent. 2012, 2, 86–96. [Google Scholar]
- Pasquale Venuti, D.D.E.M. Rethinking deep marginal extension (DME). Int. J. Cosmet. Dent. 2018, 7, 26–32. [Google Scholar]
- Ghezzi, C.; Brambilla, G.; Conti, A.; Dosoli, R.; Ceroni, F.; Ferrantino, L. Cervical margin relocation: Case series and new classification system. Int. J. Esthet. Dent. 2019, 14, 272–284. [Google Scholar] [PubMed]
- Khabadze IVB, Z.S.; Shilyaeva, E.S.; Kotelnikova, A.P.; Nazarova, D.A.; Bakayev, Y.A.; Abdulkerimova, S.M. Deep margin elevation: A systematic review. Endod. Today 2021, 19, 175–183. [Google Scholar] [CrossRef]
- Bresser, R.A.; Gerdolle, D.; van den Heijkant, I.A.; Sluiter-Pouwels, L.M.A.; Cune, M.S.; Gresnigt, M.M.M. Up to 12 years clinical evaluation of 197 partial indirect restorations with deep margin elevation in the posterior region. J. Dent. 2019, 91, 103227. [Google Scholar] [CrossRef] [PubMed]
- Dietschi, D.; Spreafico, R. Evidence-based concepts and procedures for bonded inlays and onlays. Part III. A case series with long-term clinical results and follow-up. Int. J. Esthet. Dent. 2019, 14, 118–133. [Google Scholar]
- Mugri, M.H.; Sayed, M.E.; Nedumgottil, B.M.; Bhandi, S.; Raj, A.T.; Testarelli, L.; Khurshid, Z.; Jain, S.; Patil, S. Treatment Prognosis of Restored Teeth with Crown Lengthening vs. Deep Margin Elevation: A Systematic Review. Materials 2021, 14, 6733. [Google Scholar] [CrossRef]
- Bertoldi, C.; Monari, E.; Cortellini, P.; Generali, L.; Lucchi, A.; Spinato, S.; Zaffe, D. Clinical and histological reaction of periodontal tissues to subgingival resin composite restorations. Clin. Oral. Investig. 2020, 24, 1001–1011. [Google Scholar] [CrossRef]
- Ferrari, M.; Koken, S.; Grandini, S.; Ferrari Cagidiaco, E.; Joda, T.; Discepoli, N. Influence of cervical margin relocation (CMR) on periodontal health: 12-month results of a controlled trial. J. Dent. 2018, 69, 70–76. [Google Scholar] [CrossRef]
- Muscholl, C.; Zamorska, N.; Schoilew, K.; Sekundo, C.; Meller, C.; Busch, C.; Wolff, D.; Frese, C. Retrospective Clinical Evaluation of Subgingival Composite Resin Restorations with Deep-Margin Elevation. J. Adhes. Dent. 2022, 24, 335–344. [Google Scholar]
- Vacek, J.S.; Gher, M.E.; Assad, D.A.; Richardson, A.C.; Giambarresi, L.I. The dimensions of the human dentogingival junction. Int. J. Periodontics Restor. Dent. 1994, 14, 154–165. [Google Scholar]
- Savadi, A.; Rangarajan, V.; Savadi, R.C.; Satheesh, P. Biologic perspectives in restorative treatment. J. Indian Prosthodont. Soc. 2011, 11, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Galler, K.M.; Weber, M.; Korkmaz, Y.; Widbiller, M.; Feuerer, M. Inflammatory Response Mechanisms of the Dentine-Pulp Complex and the Periapical Tissues. Int. J. Mol. Sci. 2021, 22, 1480. [Google Scholar] [CrossRef] [PubMed]
- Frese, C.; Wolff, D.; Staehle, H. Proximal Box Elevation with Resin Composite and the Dogma of Biological Width: Clinical R2-Technique and Critical Review. Oper. Dent. 2014, 39, 22–31. [Google Scholar] [CrossRef]
- Oppermann, R.V.; Gomes, S.C.; Cavagni, J.; Cayana, E.G.; Conceição, E.N. Response to Proximal Restorations Placed Either Subgingivally or Following Crown Lengthening in Patients with No History of Periodontal Disease. Int. J. Periodontics Restor. Dent. 2016, 36, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Bresser, R.A.; Cune, M.S.; Gresnigt, M.M.M. Deep Margin Elevation for adhesive indirect restorations. Ned. Tijdschr. Tandheelkd. 2023, 130, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Samartzi, T.K.; Papalexopoulos, D.; Ntovas, P.; Rahiotis, C.; Blatz, M.B. Deep Margin Elevation: A Literature Review. Dent. J. 2022, 10, 48. [Google Scholar] [CrossRef]
- Binalrimal, S.R.; Banjar, W.M.; Alyousef, S.H.; Alawad, M.I.; Alawad, G.I. Assessment of knowledge, attitude, and practice regarding Deep Margin Elevation (DME) among dental practitioners in Riyadh, Saudi Arabia. J. Fam. Med. Prim. Care 2021, 10, 1931–1937. [Google Scholar] [CrossRef]
- Bresser, R.A.; Naves, L.Z.; van der Made, S.A.M.; Cune, M.S.; Gresnigt, M.M.M. Deep margin elevation. Int. J. Esthet. Dent. 2023, 18, 142–160. [Google Scholar]
- Sirajuddin, S.; Narasappa, K.M.; Gundapaneni, V.; Chungkham, S.; Walikar, A.S. Iatrogenic Damage to Periodontium by Restorative Treatment Procedures: An Overview. Open Dent. J. 2015, 9, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Douglas de Oliveira, D.W.; Maravilha, M.N.; dos Anjos, T.N.; Goncalves, P.F.; Flecha, O.D.; Tavano, K. Clinical and Radiographic Evaluation of the Periodontium with Biologic Width Invasion by Overextending Restoration Margins—A Pilot Study. J. Int. Acad. Periodontol. 2015, 17, 116–122. [Google Scholar] [PubMed]
- Furtado, S.H.V.; Fanibunda, U. Deep margin elevation: Raising the bar in adhesive restorations—A case series. Int. J. Appl. Dent. Sci. 2021, 7, 387–392. [Google Scholar] [CrossRef]
- Gupta, S.K.; Saxena, P.; Pant, V.A.; Pant, A.B. Release and toxicity of dental resin composite. Toxicol. Int. 2012, 19, 225–234. [Google Scholar]


{kind=link}
| Classification of DME | |
|---|---|
| Venuti P et al. [13] | Ghezzi C et al. [14] |
| Class 1: soft tissue retraction through rubber dam, cord and teflon | Class 1: nonsurgical CMR |
| Class 2: soft tissue ablation through blade, diode laser, electrosurgery and soft tissue bur | Class 2a: surgical CMR (gingival approach) |
| Class 3: bone and soft tissue ablation through surgical crown lengthening | Class 2b: surgical CMR (osseous approach) |
| Class 4: Dental tissue elevation through orthodontic extrusion, the surgical extrusion technique and the partial exodontic technique | |
| Study | Study Design | Mean Follow Up | Material for Dme | Type of Restoration | Impact of Dme on Gingival Tissue | Recommendation |
|---|---|---|---|---|---|---|
| Mugri et al. [18] | Systematic review | N/a | Hybrid nanofiller composite, lithium disilicate | Indirect restoration | Better response compared to surgical crown lengthening | Inconclusive |
| Chun et al. [2] | Systematic review | N/a | Composites | Onlays and crowns | No change observed in clinical attachment loss, marginal bone level and recession; however, increased pocket depth and bleeding was seen upon probing | Negative |
| Bertoldi et al. [19] | Prospective cohort study | 3 months | Composite | Crowns | Gingival inflammation levels of DME were similar to the untreated natural root surfaces | Positive |
| Ferrari et al. [20] | Prospective cohort study | 12 months | Flow composite | Onlays | Frequent bleeding upon probing but no significant changes in plaque and gingival indices | Negative |
| Alghulikah et al. [10] | Systematic review | N/a | DME is well tolerated by the periodontium | Positive | ||
| Muscholl et al. [21] | Retrospective study | 3 years | Composite | - | No increased periodontal or gingival inflammation was observed | Positive |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Felemban, M.F.; Khattak, O.; Alsharari, T.; Alzahrani, A.H.; Ganji, K.K.; Iqbal, A. Relationship between Deep Marginal Elevation and Periodontal Parameters: A Systematic Review. Medicina 2023, 59, 1948. https://doi.org/10.3390/medicina59111948
Felemban MF, Khattak O, Alsharari T, Alzahrani AH, Ganji KK, Iqbal A. Relationship between Deep Marginal Elevation and Periodontal Parameters: A Systematic Review. Medicina. 2023; 59(11):1948. https://doi.org/10.3390/medicina59111948
Chicago/Turabian StyleFelemban, Mohammed Fareed, Osama Khattak, Thani Alsharari, Abdulrahman H. Alzahrani, Kiran Kumar Ganji, and Azhar Iqbal. 2023. "Relationship between Deep Marginal Elevation and Periodontal Parameters: A Systematic Review" Medicina 59, no. 11: 1948. https://doi.org/10.3390/medicina59111948