
Replacing Potassium in the Emergency Department May Not Decrease the Hospital Mortality in Mild Hypokalemia: A Propensity Score Matching Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
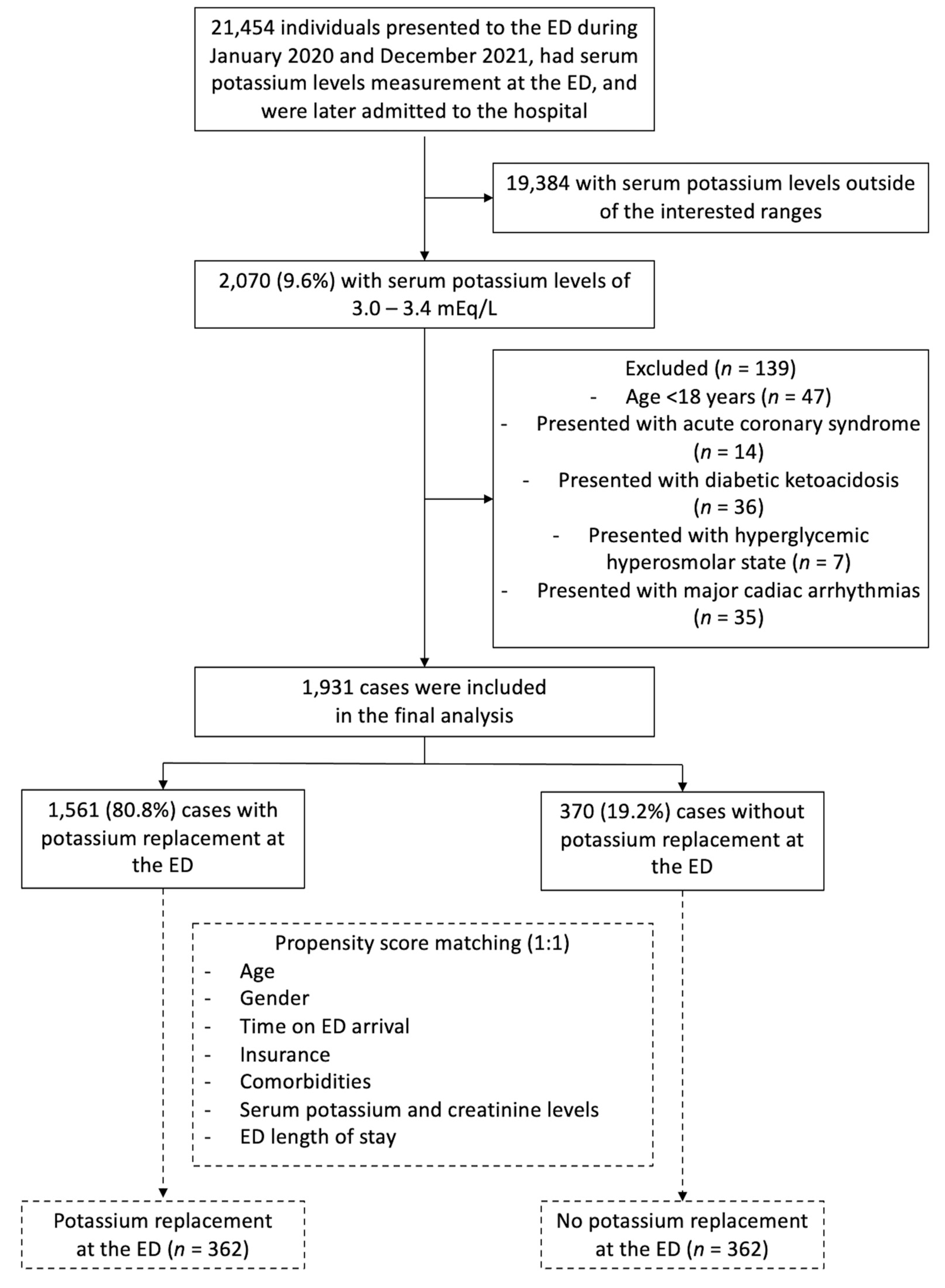
2.2. Study Participants
2.3. Data Collection and Outcome Measures
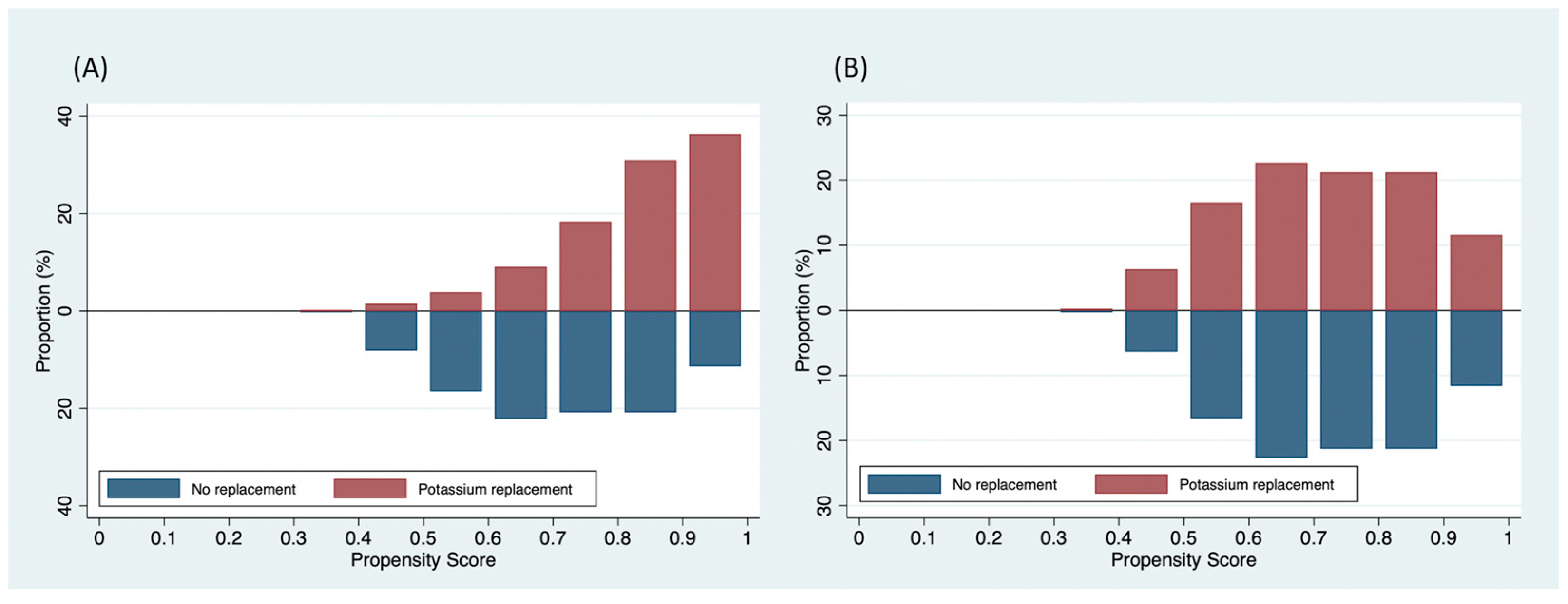
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ingram, T.C.; Olsson, J.M. In brief: Hypokalemia. Pediatr. Rev. 2008, 29, e50–e51. [Google Scholar] [CrossRef]
- Schaefer, T.J.; Wolford, R.W. Disorders of potassium. Emerg. Med. Clin. 2005, 23, 723–747. [Google Scholar] [CrossRef]
- Viera, A.J.; Wouk, N. Potassium Disorders: Hypokalemia and Hyperkalemia. Am. Fam. Physician 2015, 92, 487–495. [Google Scholar] [PubMed]
- Singer, A.J.; Thode, H.C., Jr.; Peacock, W.F. A retrospective study of emergency department potassium disturbances: Severity, treatment, and outcomes. Clin. Exp. Emerg. Med. 2017, 4, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Marti, G.; Schwarz, C.; Leichtle, A.B.; Fiedler, G.-M.; Arampatzis, S.; Exadaktylos, A.K.; Lindner, G. Etiology and symptoms of severe hypokalemia in emergency department patients. Eur. J. Emerg. Med. 2014, 21, 46–51. [Google Scholar] [CrossRef]
- Vuillaume, L.A.; Ferreira, J.P.; Asseray, N.; Trombert-Paviot, B.; Montassier, E.; Legrand, M.; Girerd, N.; Boivin, J.-M.; Chouihed, T.; Rossignol, P. Hypokalemia is frequent and has prognostic implications in stable patients attending the emergency department. PLoS ONE 2020, 15, e0236934. [Google Scholar]
- Harkness, W.; Watts, P.; Kopstein, M.; Dziadkowiec, O.; Hicks, G.; Scherbak, D. Correcting Hypokalemia in Hospitalized Patients Does Not Decrease Risk of Cardiac Arrhythmias. Adv. Med. 2019, 2019, 4919707. [Google Scholar] [CrossRef]
- Colombo, M.G.; Kirchberger, I.; Amann, U.; Dinser, L.; Meisinger, C. Association of serum potassium concentration with mortality and ventricular arrhythmias in patients with acute myocardial infarction: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2018, 25, 576–595. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Patel, R.B.; Tannenbaum, S.; Viana-Tejedor, A.; Guo, J.; Im, K.; Morrow, D.A.; Scirica, B.M. Serum potassium levels, cardiac arrhythmias, and mortality following non-ST-elevation myocardial infarction or unstable angina: Insights from MERLIN-TIMI 36. Eur. Heart J. Acute Cardiovasc. Care 2017, 6, 18–25. [Google Scholar] [CrossRef]
- Hoppe, L.K.; Muhlack, D.C.; Koenig, W.; Carr, P.R.; Brenner, H.; Schöttker, B. Association of Abnormal Serum Potassium Levels with Arrhythmias and Cardiovascular Mortality: A Systematic Review and Meta-Analysis of Observational Studies. Cardiovasc. Drugs Ther. 2018, 32, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Fayfman, M.; Pasquel, F.J.; Umpierrez, G.E. Management of Hyperglycemic Crises. Med. Clin. North Am. 2017, 101, 587–606. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat. Med. 2009, 28, 3083–3107. [Google Scholar] [CrossRef]
- Austin, P.C.; Stuart, E.A. Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Stat. Med. 2015, 34, 3661–3679. [Google Scholar] [CrossRef] [PubMed]
- Conway, R.; Creagh, D.; Byrne, D.G.; O’Riordan, D.; Silke, B. Serum potassium levels as an outcome determinant in acute medical admissions. Clin. Med. 2015, 15, 239–243. [Google Scholar] [CrossRef]
- Cohn, J.N.; Kowey, P.R.; Whelton, P.K.; Prisant, L.M. New Guidelines for Potassium Replacement in Clinical Practice: A Contemporary Review by the National Council on Potassium in Clinical Practice. Arch. Intern. Med. 2000, 160, 2429–2436. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Spertus, J.A.; Gosch, K.; Venkitachalam, L.; Jones, P.G.; Berghe, G.V.D.; Kosiborod, M. Serum potassium levels and mortality in acute myocardial infarction. JAMA 2012, 307, 157–164. [Google Scholar] [CrossRef]
- Madias, J.E.; Shah, B.; Chintalapally, G.; Chalavarya, G.; Madias, N.E. Admission serum potassium in patients with acute myocardial infarction: Its correlates and value as a determinant of in-hospital outcome. Chest 2000, 118, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Legrand, M.; Ludes, P.-O.; Massy, Z.; Rossignol, P.; Parenica, J.; Park, J.-J.; Ishihara, S.; AlHabib, K.F.; Maggioni, A.; Miróet, Ò.; et al. AssoSciation between hypo- and hyperkalemia and outcome in acute heart failure patients: The role of medications. Clin. Res. Cardiol. 2018, 107, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Speer, T.; Schunk, S.J.; Zewinger, S. Serum potassium and adverse outcomes across the range of kidney function: A CKD Prognosis Consortium meta-analysis. Eur. Heart J. 2018, 39, 1543–1545. [Google Scholar] [CrossRef]
- Krijthe, B.P.; Heeringa, J.; Kors, J.A.; Hofman, A.; Franco, O.H.; Witteman, J.C.M.; Stricker, B.H. Serum potassium levels and the risk of atrial fibrillation: The Rotterdam Study. Int. J. Cardiol. 2013, 168, 5411–5415. [Google Scholar] [CrossRef] [PubMed]
- Pucino, F.; Danielson, B.D.; Carlson, J.D.; Strommen, G.L.; Walker, P.R.; Beck, C.L.; Thiege, D.J.; Gill, D.S. Patient tolerance to intravenous potassium chloride with and without lidocaine. Drug Intell. Clin. Pharm. 1988, 22, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Stuebing, E.A. Surgical Vampires and Rising Health Care Expenditure. Arch. Surg. 2011, 146, 524. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Original Cohort | Propensity-Matched Cohort | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Replacement (n = 1561) | No Replacement (n = 370) | STD | Replacement (n = 362) | No Replacement (n = 362) | STD | |||||
| n | (%) | n | (%) | n | (%) | n | (%) | |||
| Baseline characteristics | ||||||||||
| Age (years), mean ± SD | 55.6 | ±20.0 | 46.0 | ±20.1 | +0.478 | 46.8 | ±20.1 | 46.3 | ±20.1 | +0.026 |
| Male gender | 899 | 57.6 | 228 | 61.6 | −0.082 | 223 | 61.6 | 226 | 62.4 | −0.017 |
| Time on ED arrival | −0.020 | +0.003 | ||||||||
| 08:01–16:00 | 348 | 22.3 | 122 | 33.0 | 112 | 30.9 | 117 | 32.3 | ||
| 16:01–24:00 | 597 | 38.2 | 122 | 33.0 | 129 | 35.6 | 120 | 33.2 | ||
| 00:01–08:00 | 616 | 39.5 | 126 | 34.0 | 121 | 33.4 | 125 | 34.5 | ||
| Insurance | −0.141 | −0.028 | ||||||||
| Universal coverage scheme | 673 | 43.1 | 163 | 44.1 | 170 | 47.0 | 158 | 43.7 | ||
| Government officer | 317 | 20.3 | 53 | 14.3 | 57 | 15.8 | 53 | 14.6 | ||
| Social security scheme | 144 | 9.2 | 41 | 11.1 | 42 | 11.6 | 39 | 10.8 | ||
| Cash payment | 368 | 23.6 | 94 | 25.4 | 67 | 18.5 | 94 | 26.0 | ||
| Stateless people | 59 | 3.8 | 19 | 5.1 | 26 | 7.2 | 18 | 5.0 | ||
| Comorbidities | ||||||||||
| Diabetes | 190 | 12.2 | 31 | 8.4 | +0.125 | 28 | 7.7 | 30 | 8.3 | −0.020 |
| Chronic heart failure | 10 | 0.6 | 5 | 1.4 | +0.476 | 8 | 2.2 | 4 | 1.1 | +0.087 |
| Chronic kidney disease | 144 | 9.2 | 25 | 6.8 | +0.091 | 28 | 7.7 | 24 | 6.6 | +0.043 |
| Route of potassium replacement | N/A | N/A | ||||||||
| Oral | 1253 | 80.3 | 0 | 0 | 257 | 71.0 | 0 | 0 | ||
| Intravenous | 738 | 47.3 | 0 | 0 | 180 | 49.7 | 0 | 0 | ||
| Serum potassium level (mmol/L), mean ± SD | 3.23 | ±0.14 | 3.31 | ±0.12 | −0.607 | 3.30 | ±0.11 | 3.31 | ±0.12 | −0.070 |
| Serum creatinine level (mg/L), median (IQR) | 0.86 | (0.68–1.16) | 0.87 | (0.69–1.09) | +0.027 | 0.85 | (0.68–1.11) | 0.87 | (0.68–1.09) | +0.011 |
| ED length of stay (hours), median (IQR) | 3.8 | (2.4–5.4) | 3.0 | (2.0–4.7) | +0.353 | 2.8 | (1.9–4.4) | 3.0 | (2.1–4.5) | −0.033 |
| Hospital Characteristics | ||||||||||
| Hospital length of stay (days), median (IQR) | 7 | (4–15) | 4 | (2–8) | +0.445 | 7 | (4–14) | 4 | (2–8) | +0.464 |
| Hospital length of stay | +0.118 | +0.186 | ||||||||
| <7 days | 875 | 56.1 | 225 | 60.8 | 192 | 53.0 | 220 | 60.8 | ||
| 7–30 days | 583 | 37.4 | 129 | 34.9 | 141 | 39.0 | 126 | 34.8 | ||
| >30 days | 103 | 6.6 | 16 | 4.3 | 29 | 8.0 | 16 | 4.4 | ||
| Acute comorbidities | ||||||||||
| Sepsis | 57 | 3.7 | 10 | 2.7 | +0.054 | 17 | 4.7 | 10 | 2.8 | +0.102 |
| Acute heart failure | 74 | 4.7 | 11 | 3.0 | +0.092 | 16 | 4.4 | 10 | 2.8 | +0.089 |
| Propensity score, mean ± SD | 0.83 | ±0.12 | 0.72 | ±0.15 | +0.872 | 0.72 | ±0.14 | 0.72 | ±0.14 | +0.041 |
| Equation Parameters | Coefficient | Standard Error | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| Age (year) | 0.022 | 0.003 | 0.015, 0.029 | <0.001 |
| Male gender | 0.079 | 0.130 | −0.175, 0.334 | 0.542 |
| Time on ED arrival | 0.207 | 0.078 | 0.055, 0.359 | 0.008 |
| Insurance | −0.049 | 0.034 | −0.117, −0.019 | 0.160 |
| Comorbidities | ||||
| Diabetes | 0.048 | 0.236 | −0.414, 0.509 | 0.840 |
| Chronic heart failure | −1.364 | 0.603 | −2.547, −0.182 | 0.024 |
| Chronic kidney disease | −0.016 | 0.312 | −0.628, 0.596 | 0.959 |
| Serum potassium level (mEq/L), mean ± SD | −0.525 | 0.053 | −0.630, −0.421 | <0.001 |
| Serum creatinine level (mg/L), median (IQR) | −0.080 | 0.061 | −0.199, 0.040 | 0.192 |
| ED length of stay (hours), median (IQR) | 0.135 | 0.320 | 0.073, 0.198 | <0.001 |
| Clinical Outcome | Replacement (n = 362) | No Replacement (n = 362) | Treatment Effect (Potassium Replacement vs. No Replacement at ED) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | Parameter | Unadjusted Analysis | Adjusted Analysis † | |||||
| Effect | 95% CI | p-Value | Effect | 95% CI | p-Value | ||||||
| All-cause hospital mortality | 12 | 3.3 | 14 | 3.9 | Odds ratio | 0.85 | 0.39, 1.87 | 0.69 | 0.81 | 0.36, 1.79 | 0.60 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wongtanasarasin, W.; Meelarp, N. Replacing Potassium in the Emergency Department May Not Decrease the Hospital Mortality in Mild Hypokalemia: A Propensity Score Matching Analysis. Medicina 2023, 59, 1912. https://doi.org/10.3390/medicina59111912
Wongtanasarasin W, Meelarp N. Replacing Potassium in the Emergency Department May Not Decrease the Hospital Mortality in Mild Hypokalemia: A Propensity Score Matching Analysis. Medicina. 2023; 59(11):1912. https://doi.org/10.3390/medicina59111912
Chicago/Turabian StyleWongtanasarasin, Wachira, and Nattikarn Meelarp. 2023. "Replacing Potassium in the Emergency Department May Not Decrease the Hospital Mortality in Mild Hypokalemia: A Propensity Score Matching Analysis" Medicina 59, no. 11: 1912. https://doi.org/10.3390/medicina59111912