
Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Respiratory Support
2.4. Study Outcome
2.5. Statistical Analysis
3. Results
3.1. Demographic, Clinical, and Respiratory Characteristics According to Respiratory Support Allocation at Admission
3.2. Mortality and Admission to ICU Rates in HFNC and CPAP Groups
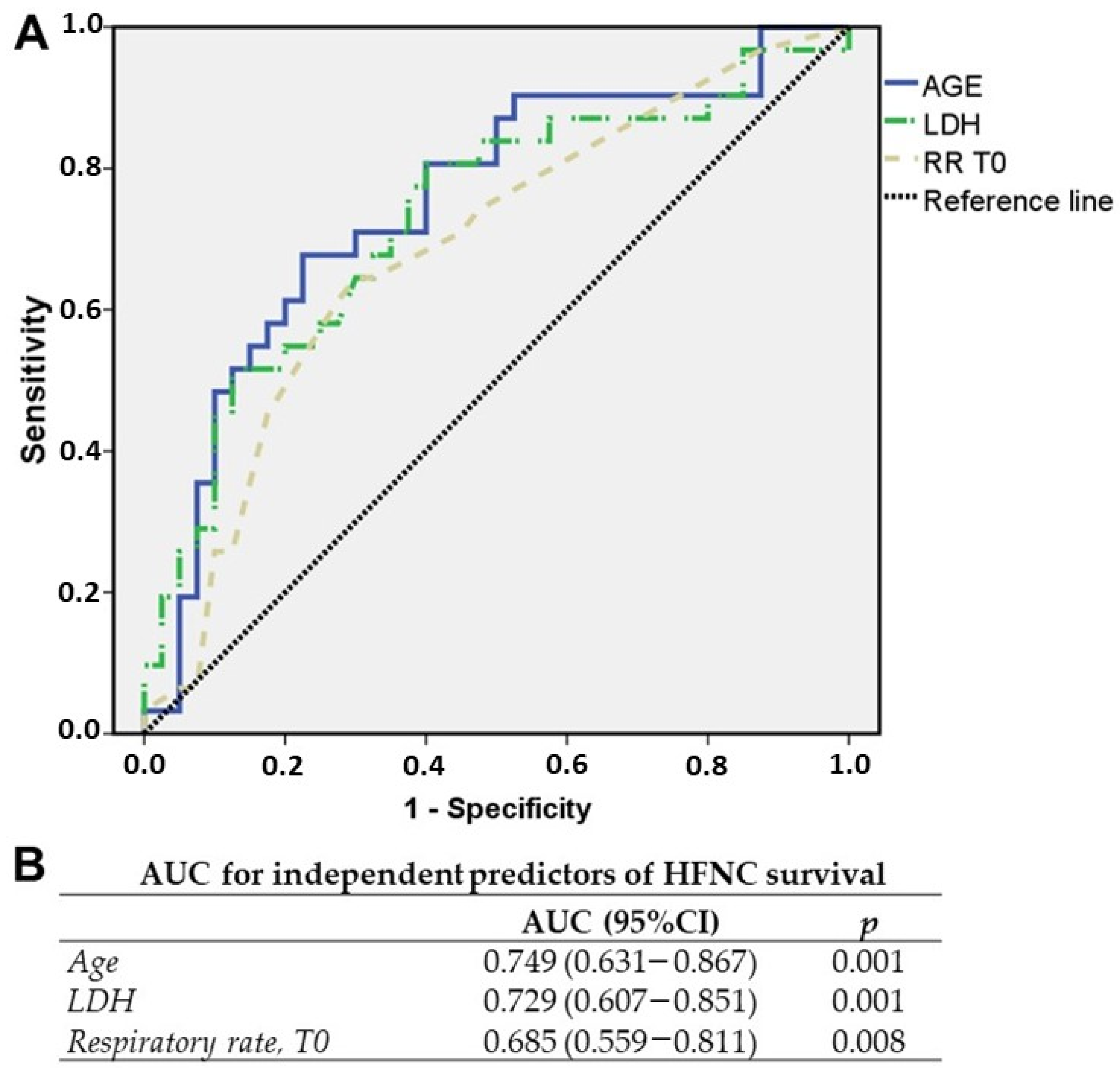
3.3. Predictors of Response to HFNC at Admission
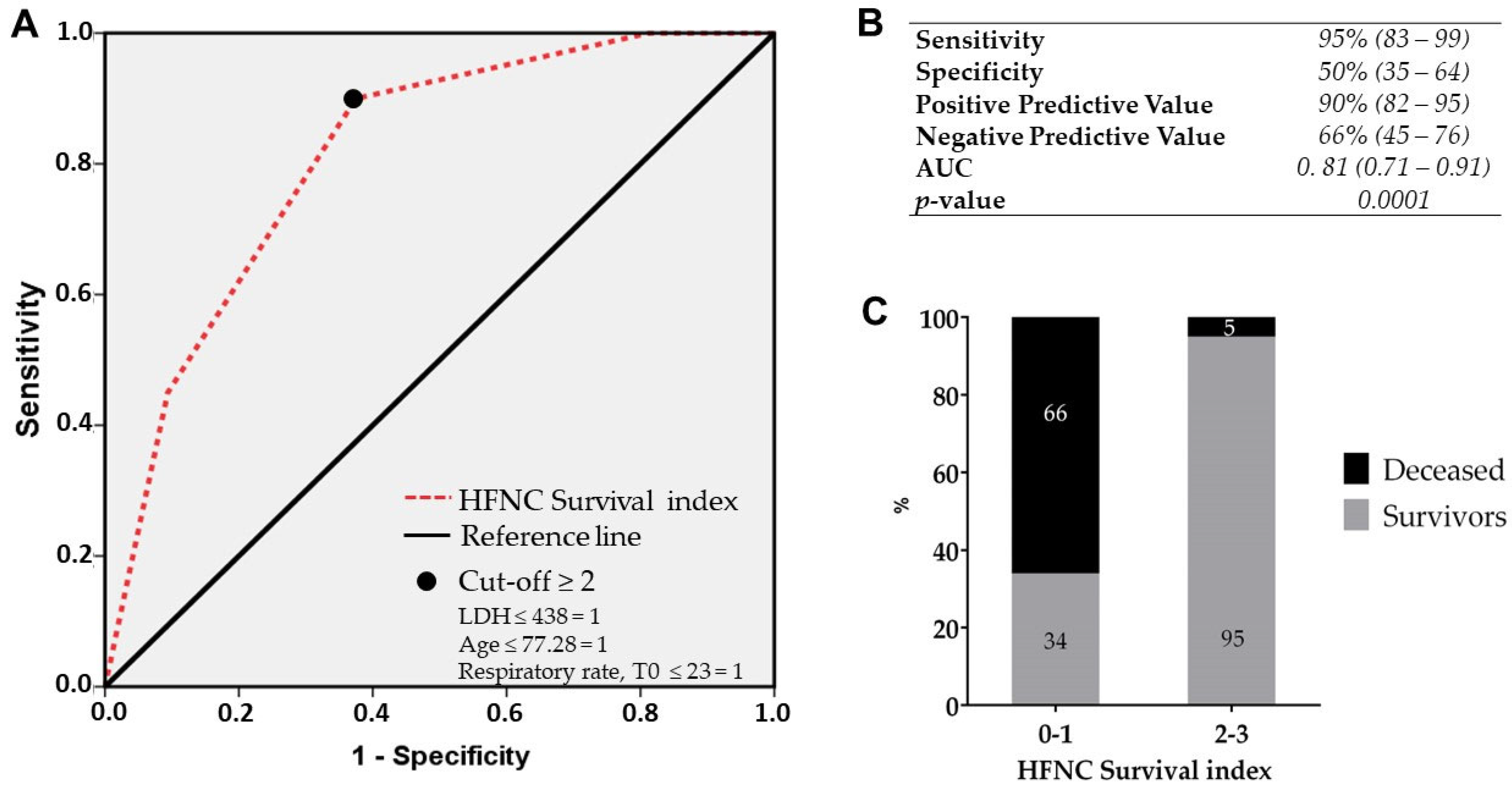
3.4. HFNC Survival Index at Admission
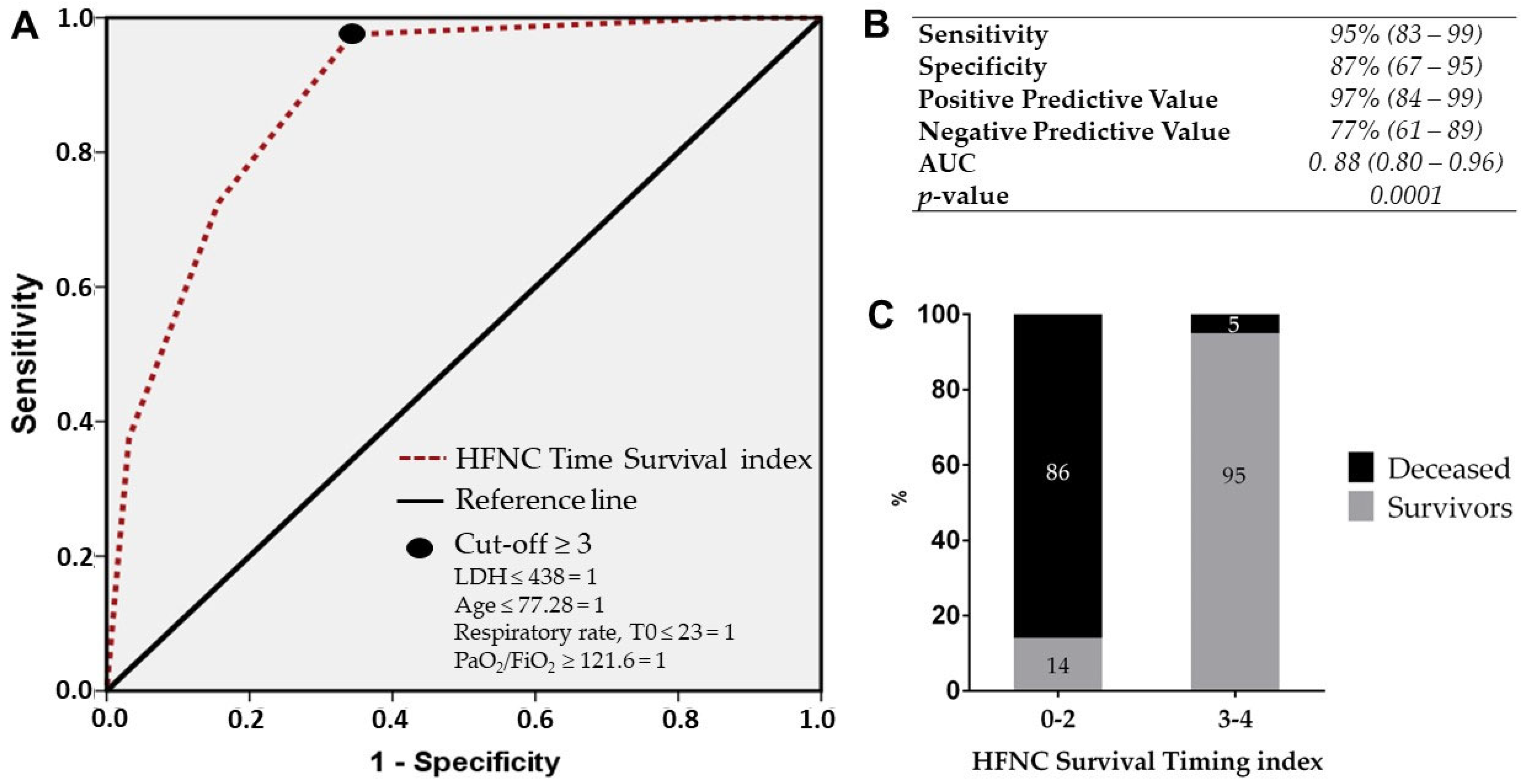
3.5. HFNC Survival Timing Index at 48 h
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections-More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef] [PubMed]
- Lieberum, J.N.; Kaiser, S.; Kalbhenn, J.; Burkle, H.; Schallner, N. Predictive markers related to local and systemic inflammation in severe COVID-19-associated ARDS: A prospective single-center analysis. BMC Infect. Dis. 2023, 23, 19. [Google Scholar] [CrossRef] [PubMed]
- Koch, V.; Gruenewald, L.D.; Albrecht, M.H.; Eichler, K.; Gruber-Rouh, T.; Yel, I.; Alizadeh, L.S.; Mahmoudi, S.; Scholtz, J.E.; Martin, S.S.; et al. Lung Opacity and Coronary Artery Calcium Score: A Combined Tool for Risk Stratification and Outcome Prediction in COVID-19 Patients. Acad. Radiol. 2022, 29, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]
- Bagnato, G.; Imbalzano, E.; Aragona, C.O.; Ioppolo, C.; Di Micco, P.; La Rosa, D.; Costa, F.; Micari, A.; Tomeo, S.; Zirilli, N.; et al. New-Onset Atrial Fibrillation and Early Mortality Rate in COVID-19 Patients: Association with IL-6 Serum Levels and Respiratory Distress. Medicina 2022, 58, 530. [Google Scholar] [CrossRef]
- Bonaccorsi, I.; Carrega, P.; Venanzi Rullo, E.; Ducatelli, R.; Falco, M.; Freni, J.; Miceli, M.; Cavaliere, R.; Fontana, V.; Versace, A.; et al. HLA-C*17 in COVID-19 patients: Hints for associations with severe clinical outcome and cardiovascular risk. Immunol. Lett. 2021, 234, 44–46. [Google Scholar] [CrossRef]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated With Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef]
- Duan, J.; Chen, B.; Liu, X.; Shu, W.; Zhao, W.; Li, J.; Li, Y.; Hong, Y.; Pan, L.; Wang, K. Use of high-flow nasal cannula and noninvasive ventilation in patients with COVID-19: A multicenter observational study. Am. J. Emerg. Med. 2021, 46, 276–281. [Google Scholar] [CrossRef]
- Fan, E.; Beitler, J.R.; Brochard, L.; Calfee, C.S.; Ferguson, N.D.; Slutsky, A.S.; Brodie, D. COVID-19-associated acute respiratory distress syndrome: Is a different approach to management warranted? Lancet Respir. Med. 2020, 8, 816–821. [Google Scholar] [CrossRef]
- Moisa, E.; Corneci, D.; Negutu, M.I.; Filimon, C.R.; Serbu, A.; Popescu, M.; Negoita, S.; Grintescu, I.M. Development and Internal Validation of a New Prognostic Model Powered to Predict 28-Day All-Cause Mortality in ICU COVID-19 Patients-The COVID-SOFA Score. J. Clin. Med. 2022, 11, 4160. [Google Scholar] [CrossRef] [PubMed]
- Elia, D.; Mozzanica, F.; Caminati, A.; Giana, I.; Carli, L.; Ambrogi, F.; Zompatori, M.; Harari, S. Prognostic value of radiological index and clinical data in patients with COVID-19 infection. Intern. Emerg. Med. 2022, 17, 1679–1687. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, R.; Mahajan, V.; Singla, K.; Konar, S.; Samra, T.; Sundaram, S.K.; Suri, V.; Garg, M.; Kalra, N.; Puri, G.D. Mortality Prediction of COVID-19 Patients at Intensive Care Unit Admission. Cureus 2021, 13, e19690. [Google Scholar] [CrossRef] [PubMed]
- Salbach, C.; Mueller-Hennessen, M.; Biener, M.; Stoyanov, K.M.; Vafaie, M.; Preusch, M.R.; Kihm, L.P.; Merle, U.; Schnitzler, P.; Katus, H.A.; et al. Validation of two severity scores as predictors for outcome in Coronavirus Disease 2019 (COVID-19). PLoS ONE 2021, 16, e0247488. [Google Scholar] [CrossRef] [PubMed]
- Bellani, G.; Grasselli, G.; Cecconi, M.; Antolini, L.; Borelli, M.; De Giacomi, F.; Bosio, G.; Latronico, N.; Filippini, M.; Gemma, M.; et al. Noninvasive Ventilatory Support of Patients with COVID-19 outside the Intensive Care Units (WARd-COVID). Ann. Am. Thorac. Soc. 2021, 18, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Malik, U.A.; Kumari, R.; Kumar, V.; Kumar, M.; Nasim, B. Effectiveness of non-invasive respiratory support strategies in patients with COVID-19: A systematic review and meta analysis. Ann. Med. Surg. 2022, 84, 104827. [Google Scholar] [CrossRef]
- Nair, P.R.; Haritha, D.; Behera, S.; Kayina, C.A.; Maitra, S.; Anand, R.K.; Ray, B.R.; Soneja, M.; Subramaniam, R.; Baidya, D.K. Comparison of High-Flow Nasal Cannula and Noninvasive Ventilation in Acute Hypoxemic Respiratory Failure Due to Severe COVID-19 Pneumonia. Respir. Care 2021, 66, 1824–1830. [Google Scholar] [CrossRef]
- Schifino, G.; Vega, M.L.; Pisani, L.; Prediletto, I.; Catalanotti, V.; Comellini, V.; Bassi, I.; Zompatori, M.; Ranieri, M.V.; Nava, S. Effects of non-invasive respiratory supports on inspiratory effort in moderate-severe COVID-19 patients. A randomized physiological study. Eur. J. Intern. Med. 2022, 100, 110–118. [Google Scholar] [CrossRef]
- Di Costanzo, D.; Mandal, M.; Mazza, M.; Esquinas, A. High-flow nasal oxygen decrease mortality in patients with severe SARS-CoV-2 pneumonia? Issues and controversies. Ann. Med. Surg. 2022, 77, 103543. [Google Scholar] [CrossRef]
- Alkouh, R.; El Rhalete, A.; Manal, M.; Ghizlane, E.A.; Samia, B.; Salma, T.; Aftiss, F.Z.; Houssam, B.; Naima, A.; Brahim, H. High-flow nasal oxygen therapy decrease the risk of mortality and the use of invasive mechanical ventilation in patients with severe SARS-CoV-2 pneumonia? A retrospective and comparative study of 265 cases. Ann. Med. Surg. 2022, 74, 103230. [Google Scholar] [CrossRef]
- Gorman, E.; Connolly, B.; Couper, K.; Perkins, G.D.; McAuley, D.F. Non-invasive respiratory support strategies in COVID-19. Lancet Respir. Med. 2021, 9, 553–556. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wang, Y.; Yang, Z.; Wu, H.; Liang, J.; Liang, H.; Lin, H.; Chen, R.; Ou, Y.; Wang, F.; et al. The use of non-invasive ventilation in COVID-19: A systematic review. Int. J. Infect. Dis. 2021, 106, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Cammarota, G.; Esposito, T.; Azzolina, D.; Cosentini, R.; Menzella, F.; Aliberti, S.; Coppadoro, A.; Bellani, G.; Foti, G.; Grasselli, G.; et al. Noninvasive respiratory support outside the intensive care unit for acute respiratory failure related to coronavirus-19 disease: A systematic review and meta-analysis. Crit. Care 2021, 25, 268. [Google Scholar] [CrossRef] [PubMed]
- Grieco, D.L.; Menga, L.S.; Cesarano, M.; Rosa, T.; Spadaro, S.; Bitondo, M.M.; Montomoli, J.; Falo, G.; Tonetti, T.; Cutuli, S.L.; et al. Effect of Helmet Noninvasive Ventilation vs High-Flow Nasal Oxygen on Days Free of Respiratory Support in Patients With COVID-19 and Moderate to Severe Hypoxemic Respiratory Failure: The HENIVOT Randomized Clinical Trial. JAMA 2021, 325, 1731–1743. [Google Scholar] [CrossRef] [PubMed]
- Perkins, G.D.; Ji, C.; Connolly, B.A.; Couper, K.; Lall, R.; Baillie, J.K.; Bradley, J.M.; Dark, P.; Dave, C.; De Soyza, A.; et al. Effect of Noninvasive Respiratory Strategies on Intubation or Mortality Among Patients With Acute Hypoxemic Respiratory Failure and COVID-19: The RECOVERY-RS Randomized Clinical Trial. JAMA 2022, 327, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Demoule, A.; Vieillard Baron, A.; Darmon, M.; Beurton, A.; Geri, G.; Voiriot, G.; Dupont, T.; Zafrani, L.; Girodias, L.; Labbe, V.; et al. High-Flow Nasal Cannula in Critically III Patients with Severe COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 1039–1042. [Google Scholar] [CrossRef]
- Ospina-Tascon, G.A.; Calderon-Tapia, L.E.; Garcia, A.F.; Zarama, V.; Gomez-Alvarez, F.; Alvarez-Saa, T.; Pardo-Otalvaro, S.; Bautista-Rincon, D.F.; Vargas, M.P.; Aldana-Diaz, J.L.; et al. Effect of High-Flow Oxygen Therapy vs Conventional Oxygen Therapy on Invasive Mechanical Ventilation and Clinical Recovery in Patients With Severe COVID-19: A Randomized Clinical Trial. JAMA 2021, 326, 2161–2171. [Google Scholar] [CrossRef]
- Marti, S.; Carsin, A.E.; Sampol, J.; Pallero, M.; Aldas, I.; Marin, T.; Lujan, M.; Lalmolda, C.; Sabater, G.; Bonnin-Vilaplana, M.; et al. Higher mortality and intubation rate in COVID-19 patients treated with noninvasive ventilation compared with high-flow oxygen or CPAP. Sci. Rep. 2022, 12, 6527. [Google Scholar] [CrossRef]
- Crimi, C.; Pierucci, P.; Renda, T.; Pisani, L.; Carlucci, A. High-Flow Nasal Cannula and COVID-19: A Clinical Review. Respir. Care 2022, 67, 227–240. [Google Scholar] [CrossRef]
- Force, A.D.T.; Ranieri, V.M.; Rubenfeld, G.D.; Thompson, B.T.; Ferguson, N.D.; Caldwell, E.; Fan, E.; Camporota, L.; Slutsky, A.S. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Attaway, A.H.; Scheraga, R.G.; Bhimraj, A.; Biehl, M.; Hatipoglu, U. Severe covid-19 pneumonia: Pathogenesis and clinical management. BMJ 2021, 372, n436. [Google Scholar] [CrossRef] [PubMed]
- Kofod, L.M.; Nielsen Jeschke, K.; Kristensen, M.T.; Krogh-Madsen, R.; Monefeldt Albek, C.; Hansen, E.F. COVID-19 and acute respiratory failure treated with CPAP. Eur. Clin. Respir. J. 2021, 8, 1910191. [Google Scholar] [CrossRef]
- Bagnato, G.; La Rosa, D.; Ioppolo, C.; De Gaetano, A.; Chiappalone, M.; Zirilli, N.; Viapiana, V.; Tringali, M.C.; Tomeo, S.; Aragona, C.O.; et al. The COVID-19 Assessment for Survival at Admission (CASA) Index: A 12 Months Observational Study. Front. Med. 2021, 8, 719976. [Google Scholar] [CrossRef] [PubMed]
- Richards, G.A.; Smith, O. Techniques for Oxygenation and Ventilation in Coronavirus Disease 2019. Semin. Respir. Crit. Care Med. 2023, 44, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Bonnesen, B.; Jensen, J.S.; Jeschke, K.N.; Mathioudakis, A.G.; Corlateanu, A.; Hansen, E.F.; Weinreich, U.M.; Hilberg, O.; Sivapalan, P. Management of COVID-19-Associated Acute Respiratory Failure with Alternatives to Invasive Mechanical Ventilation: High-Flow Oxygen, Continuous Positive Airway Pressure, and Noninvasive Ventilation. Diagnostics 2021, 11, 2259. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Dai, B.; Zhao, H.W.; Wang, W.; Kang, J.; Hou, H.J.; Tan, W. Comparison between high-flow nasal cannula and noninvasive ventilation in COVID-19 patients: A systematic review and meta-analysis. Ther. Adv. Respir. Dis. 2022, 16, 17534666221113663. [Google Scholar] [CrossRef] [PubMed]
- Smesseim, I.; Mooij-Kalverda, K.; Hessels, L.; Korevaar, D.A.; Atasever, B.; de Graaff, H.; Goorhuis, A.; Nossent, E.; Bos, L.; Bonta, P.; et al. High flow nasal cannula for acute respiratory failure due to COVID-19 in patients with a ‘do-not-intubate’ order: A survival analysis. Clin. Respir. J. 2022, 17, 115–119. [Google Scholar] [CrossRef]
- Tverring, J.; Akesson, A.; Nielsen, N. Helmet continuous positive airway pressure versus high-flow nasal cannula in COVID-19: A pragmatic randomised clinical trial (COVID HELMET). Trials 2020, 21, 994. [Google Scholar] [CrossRef]
- Singh, A.; Khanna, P.; Sarkar, S. High-Flow Nasal Cannula, a Boon or a Bane for COVID-19 Patients? An Evidence-Based Review. Curr. Anesthesiol. Rep. 2021, 11, 101–106. [Google Scholar] [CrossRef]
- Forrest, I.S.; Jaladanki, S.K.; Paranjpe, I.; Glicksberg, B.S.; Nadkarni, G.N.; Do, R. Non-invasive ventilation versus mechanical ventilation in hypoxemic patients with COVID-19. Infection 2021, 49, 989–997. [Google Scholar] [CrossRef] [PubMed]
- Nevola, R.; Russo, A.; Scuotto, S.; Imbriani, S.; Aprea, C.; Abitabile, M.; Beccia, D.; Brin, C.; Carusone, C.; Cinone, F.; et al. Non-invasive respiratory support in SARS-CoV-2 related acute respiratory distress syndrome: When is it most appropriate to start treatment? Respir. Res. 2022, 23, 327. [Google Scholar] [CrossRef] [PubMed]
- Coppadoro, A.; Benini, A.; Fruscio, R.; Verga, L.; Mazzola, P.; Bellelli, G.; Carbone, M.; Mulinacci, G.; Soria, A.; Noe, B.; et al. Helmet CPAP to treat hypoxic pneumonia outside the ICU: An observational study during the COVID-19 outbreak. Crit. Care 2021, 25, 80. [Google Scholar] [CrossRef] [PubMed]
- Menzella, F.; Barbieri, C.; Fontana, M.; Scelfo, C.; Castagnetti, C.; Ghidoni, G.; Ruggiero, P.; Livrieri, F.; Piro, R.; Ghidorsi, L.; et al. Effectiveness of noninvasive ventilation in COVID-19 related-acute respiratory distress syndrome. Clin. Respir. J. 2021, 15, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Ferreyro, B.L.; Angriman, F.; Munshi, L.; Del Sorbo, L.; Ferguson, N.D.; Rochwerg, B.; Ryu, M.J.; Saskin, R.; Wunsch, H.; da Costa, B.R.; et al. Association of Noninvasive Oxygenation Strategies With All-Cause Mortality in Adults With Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-analysis. JAMA 2020, 324, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Procopio, G.; Cancelliere, A.; Trecarichi, E.M.; Mazzitelli, M.; Arrighi, E.; Perri, G.; Serapide, F.; Pelaia, C.; Lio, E.; Busceti, M.T.; et al. Oxygen therapy via high flow nasal cannula in severe respiratory failure caused by Sars-Cov-2 infection: A real-life observational study. Ther. Adv. Respir. Dis. 2020, 14, 1753466620963016. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Tonetti, T.; Protti, A.; Langer, T.; Girardis, M.; Bellani, G.; Laffey, J.; Carrafiello, G.; Carsana, L.; Rizzuto, C.; et al. Pathophysiology of COVID-19-associated acute respiratory distress syndrome: A multicentre prospective observational study. Lancet Respir. Med. 2020, 8, 1201–1208. [Google Scholar] [CrossRef]
- Swenson, K.E.; Ruoss, S.J.; Swenson, E.R. The Pathophysiology and Dangers of Silent Hypoxemia in COVID-19 Lung Injury. Ann. Am. Thorac. Soc. 2021, 18, 1098–1105. [Google Scholar] [CrossRef]
- McFadden, R.G.; Oliphant, L.D. Serum lactate dehydrogenase in interstitial lung disease. Chest 1991, 100, 1182. [Google Scholar] [CrossRef]
- Poggiali, E.; Zaino, D.; Immovilli, P.; Rovero, L.; Losi, G.; Dacrema, A.; Nuccetelli, M.; Vadacca, G.B.; Guidetti, D.; Vercelli, A.; et al. Lactate dehydrogenase and C-reactive protein as predictors of respiratory failure in CoVID-19 patients. Clin. Chim. Acta 2020, 509, 135–138. [Google Scholar] [CrossRef]
- Romano, C.; Cozzolino, D.; Cuomo, G.; Abitabile, M.; Carusone, C.; Cinone, F.; Nappo, F.; Nevola, R.; Sellitto, A.; Auricchio, A.; et al. Prediction of SARS-CoV-2-Related Lung Inflammation Spreading by V:ERITAS (Vanvitelli Early Recognition of Inflamed Thoracic Areas Spreading). J. Clin. Med. 2022, 11, 2434. [Google Scholar] [CrossRef] [PubMed]
- Ait Hamou, Z.; Levy, N.; Charpentier, J.; Mira, J.P.; Jamme, M.; Jozwiak, M. Use of high-flow nasal cannula oxygen and risk factors for high-flow nasal cannula oxygen failure in critically-ill patients with COVID-19. Respir. Res. 2022, 23, 329. [Google Scholar] [CrossRef] [PubMed]
- Frat, J.P.; Thille, A.W.; Mercat, A.; Girault, C.; Ragot, S.; Perbet, S.; Prat, G.; Boulain, T.; Morawiec, E.; Cottereau, A.; et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N. Engl. J. Med. 2015, 372, 2185–2196. [Google Scholar] [CrossRef] [PubMed]
- Tobin, M.J.; Laghi, F.; Jubran, A. Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. Am. J. Respir. Crit. Care Med. 2020, 202, 356–360. [Google Scholar] [CrossRef]
- Mellado-Artigas, R.; Mujica, L.E.; Ruiz, M.L.; Ferreyro, B.L.; Angriman, F.; Arruti, E.; Torres, A.; Barbeta, E.; Villar, J.; Ferrando, C.; et al. Predictors of failure with high-flow nasal oxygen therapy in COVID-19 patients with acute respiratory failure: A multicenter observational study. J. Intensive Care 2021, 9, 23. [Google Scholar] [CrossRef]
- Cressoni, M.; Caironi, P.; Polli, F.; Carlesso, E.; Chiumello, D.; Cadringher, P.; Quintel, M.; Ranieri, V.M.; Bugedo, G.; Gattinoni, L. Anatomical and functional intrapulmonary shunt in acute respiratory distress syndrome. Crit. Care Med. 2008, 36, 669–675. [Google Scholar] [CrossRef]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota, L. COVID-19 pneumonia: Different respiratory treatments for different phenotypes? Intensive Care Med. 2020, 46, 1099–1102. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HFNC (n = 77) | CPAP (n = 82) | p | |
|---|---|---|---|
| Demographics | |||
| Age, years | 72 (63–78) | 73 (64–80) | 0.394 |
| BMI | 27.6 (24.4–29.4) | 27.3 (24.4–29.4) | 0.469 |
| Gender, male | 29 (37.6) | 34 (41.4) | 0.582 |
| Hospital stay (days) | 22.5 (16–29) | 14 (8–19.5) | 0.001 |
| Mortality (28 days) | 13 (16.8) | 41 (50) | 0.001 |
| ICU admission (28 days) | 10 (13) | 26 (32) | 0.003 |
| COVID-19 vaccination | 16 (20.7) | 12 (14.6) | 0.332 |
| Comorbidities | 2 (1–5) | 2 (1–4) | 0.408 |
| Charlson Comorbidity Index | 4 (2–6) | 4 (2.25–6) | 0.891 |
| Diabetes | 43 (55.8) | 38 (46.3) | 0.264 |
| Coronary artery disease | 25 (32.5) | 22 (26.8) | 0.459 |
| COPD | 16 (20.7) | 12 (14.6) | 0.332 |
| Heart failure | 23 (29.8) | 25 (30.4) | 0.891 |
| Hypertension | 43 (55.8) | 54 (65.8) | 0.164 |
| Chronic kidney disease | 12 (15.5) | 17 (20.7) | 0.381 |
| Atrial fibrillation | 11 (14.2) | 10 (12.9) | 0.725 |
| Cerebrovascular disease | 5 (6.4) | 8 (9.7) | 0.436 |
| Respiratory failure | 3 (3.8) | 2 (2.4) | 0.611 |
| Vital and clinical parameters | |||
| Heart rate | 80 (70–95) | 82 (76–92) | 0.777 |
| DBP mmHg | 80 (65–85) | 79 (70–85) | 0,689 |
| SBP mmHg | 135 (125–145) | 140 (130–150) | 0.114 |
| MBP mmHg | 96 (85–105) | 100 (93–104) | 0.193 |
| Fever (≥38 °C) | 31 (40.2) | 39 (47.5) | 0.319 |
| Glasgow Coma Scale | 15 (15–15) | 15 (15–15) | 0.665 |
| Therapy | |||
| Corticosteroids | 77 (100) | 82 (100) | 1 |
| Anti-IL6 | 8 (10.3) | 8 (9.7) | 0.917 |
| Remdesivir | 2 (2.5) | 2 (2.4) | 0.967 |
| Anti-SARS-CoV-2 antibody | 4 (5.1) | 4 (4.87) | 0.954 |
| HFNC (n = 77) | CPAP (n = 82) | p | |
|---|---|---|---|
| Laboratory findings | |||
| Albumin, g/dL | 3.13 (2.9–3.3) | 3.1 (2.7–3.4) | 0.582 |
| ALT, UI/L | 24.5 (15–42) | 29 (19–55) | 0.101 |
| AST, UI/L | 29 (20–40) | 31 (23–53) | 0.216 |
| CK, U/L | 100 (50–214) | 83.5 (44–241) | 0.950 |
| Creatinine, mg/dL | 0.9 (0.8–1.2) | 0.8 (0.7–1.4) | 0.147 |
| D-Dimer, mcg/mL | 3 (3–4) | 4 (4–4) | 0.953 |
| Fibrinogen, mg/dL | 464 (342–889) | 533 (360–636) | 0.595 |
| Hb, gr/dL | 14 (10–14.5) | 14 (11.5–15.5) | 0.620 |
| IL-6, pg/mL | 28 (9–63.9) | 70 (42.7–129) | 0.001 |
| LDH, U/L | 339 (276–432) | 425 (334–574) | 0.004 |
| Bilirubin, total, mg/dL | 0.63 (0.43–0.85) | 0.57 (0.45–0.93) | 0.895 |
| NT-proBNP, pg/mL | 504 (163–1712) | 574 (163–2071) | 0.703 |
| CRP, mg/dL | 6.3 (3.2–14.1) | 10.1 (5.9–14.6) | 0.119 |
| PCT, ng/mL | 0.15 (0.08–0.52) | 0.12 (0.08–0.3) | 0.920 |
| Ferritin, mg/dL | 642 (252–2235) | 905 (480–1621) | 0.519 |
| Platelet count, cells × 104 | 198 (106–244) | 205 (151–282) | 0.294 |
| Troponin, pg/mL | 32.5 (15.4–87) | 28 (11.7–63.9) | 0.238 |
| Urea, mg/dL | 77.5 (48.5–154.7) | 61 (40.5–114) | 0.772 |
| WBC, cells | 8600 (5150–15,175) | 9100 (6800–13,150) | 0.096 |
| Lymphocyte count, cells | 994 (657–1416) | 742 (551–1081) | 0.370 |
| Neutrophil count, cells | 6382 (3823–13,446) | 8010 (5731–11,614) | 0.126 |
| Neutrophil/lymphocyte ratio | 7.2 (3.8–11) | 9.5 (6.8–15.8) | 0.024 |
| HFNC (n = 77) | CPAP (n = 82) | p | |
|---|---|---|---|
| Arterial blood gas analysis | |||
| PaO2 | 62 (56–69) | 58 (54–63) | 0.039 |
| PaCO2 | 35 (33–37) | 34 (32–38) | 0.161 |
| SO2 | 94 (90–95) | 91 (88–93) | 0.004 |
| FiO2 | 60 (50–60) | 60 (60–60) | 0.564 |
| lactates | 1.45 (1–2.3) | 1.6 (1.1–2.5) | 0.485 |
| Respiratory Indexes | |||
| Respiratory Rate | 20 (20–25) | 25 (20–28) | 0.014 |
| SpO2 | 93 (90–95) | 92 (88–94) | 0.012 |
| PaO2/FiO2 ratio | 112 (97–125) | 101 (92–110) | 0.064 |
| SpO2/FiO2 ratio | 158 (152–179) | 155 (148–160) | 0.067 |
| ROX | 7.4 (6.8–8.1) | 6.6 (5.4–7.8) | 0.025 |
| Berlin criteria | |||
| PaO2/FiO2 ≤ 100 | 28 (36.4) | 35 (42.6) | 0.418 |
| >100 PaO2/FiO2 ≤ 200 | 49 (63.6) | 47 (57.3) | 0.418 |
| OR (95% CI) | Change in Risk (%) | p | |
|---|---|---|---|
| At admission | |||
| Age, years | 0.909 (0.856–0.965) | −9.1 | 0.002 |
| Albumin, g/dL | 0.285 | ||
| LDH, U/L | 0.995 (0.991–0.999) | −0.5 | 0.008 |
| Neutrophil-to-lymphocyte ratio | 0.914 (0.845–0.989) | −8.6 | 0.025 |
| IL-6, pg/mL | 0.981 (0.968–0.994) | −1.9 | 0.004 |
| Troponin, pg/mL | 0.703 | ||
| Respiratory rate | 0.859 (0.768–0.961) | −14.1 | 0.008 |
| 6 h | |||
| Respiratory rate | 0.801 (0.688–0.932) | −19.9 | 0.004 |
| SpO2/FiO2 | 1.21 (1.001–1.043) | 21 | 0.044 |
| ROX | 1.743 (1.226–2.478) | 74.3 | 0.002 |
| 24 h | |||
| Respiratory rate | 0.808 (0.688–0.95) | −19.2 | 0.010 |
| SpO2/FiO2 | 1.024 (1.007–1.04) | 2.4 | 0.005 |
| ROX | 1.436 (1.125–1.833) | 43.6 | 0.004 |
| PaO2/FiO2 | 1.013 (1.002–1.025) | 1.3 | 0.022 |
| 48 h | |||
| Respiratory rate | 0.819 | ||
| ROX | 1.37 (1.06–1.77) | 37 | 0.017 |
| PaO2/FiO2 | 1.032 (1.012–1.054) | 3.2 | 0.003 |
| OR (95% CI) | Change in Risk (%) | p | |
|---|---|---|---|
| At admission | |||
| Age, years | 0.922 (0.866–0.977) | −7.8 | 0.024 |
| CCI | 0.092 | ||
| LDH, U/L | 0.995 (0.992–0.999) | −0.5 | 0.013 |
| Respiratory rate | 0.864 (0.757–0.986) | −13.6 | 0.030 |
| Neutrophil-to-lymphocyte ratio | 0.088 | ||
| IL-6, pg/mL | 0.124 | ||
| 6 h | |||
| ROX | 1.743 (1.226–2.478) | 74.3 | 0.002 |
| SpO2/FiO2 | 0.423 | ||
| Respiratory rate | 0.374 | ||
| 24 h | |||
| ROX | 1.429 (1.116–1.830) | 42.9 | 0.005 |
| SpO2/FiO2 | 0.734 | ||
| Respiratory rate | 0.840 | ||
| PaO2/FiO2 | 0.582 | ||
| 48 h | |||
| PaO2/FiO2 | 1.041 (1.008–1.075) | 4.1 | 0.013 |
| ROX | 0.490 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagnato, G.; Imbalzano, E.; Ioppolo, C.; La Rosa, D.; Chiappalone, M.; De Gaetano, A.; Viapiana, V.; Irrera, N.; Nassisi, V.; Tringali, M.C.; et al. Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study. Medicina 2024, 60, 71. https://doi.org/10.3390/medicina60010071
Bagnato G, Imbalzano E, Ioppolo C, La Rosa D, Chiappalone M, De Gaetano A, Viapiana V, Irrera N, Nassisi V, Tringali MC, et al. Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study. Medicina. 2024; 60(1):71. https://doi.org/10.3390/medicina60010071
Chicago/Turabian StyleBagnato, Gianluca, Egidio Imbalzano, Carmelo Ioppolo, Daniela La Rosa, Marianna Chiappalone, Alberta De Gaetano, Valeria Viapiana, Natasha Irrera, Veronica Nassisi, Maria Concetta Tringali, and et al. 2024. "Stratification of COVID-19 Patients with Moderate-to-Severe Hypoxemic Respiratory Failure for Response to High-Flow Nasal Cannula: A Retrospective Observational Study" Medicina 60, no. 1: 71. https://doi.org/10.3390/medicina60010071