
Assessing the Impact of the COVID-19 Pandemic on Pediatric Emergency Department Visits in Taiwan
 , and
, and
Abstract
:1. Introduction
2. Methods
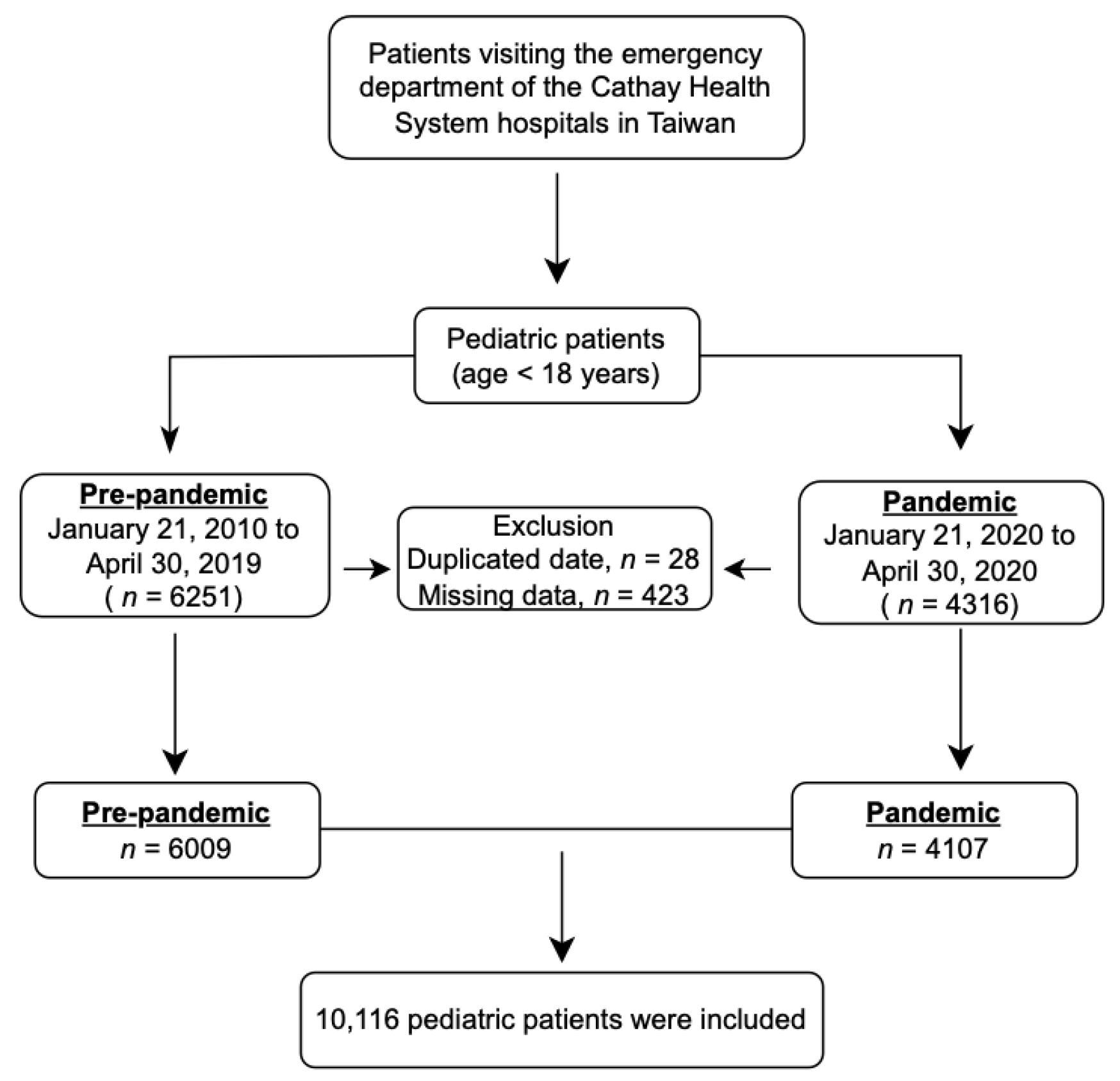
2.1. Study Setting
2.2. Study Design
2.3. Variables
2.4. Ethical Statement
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitation
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COVID-19 | coronavirus disease 2019 |
| ED | emergency department |
| IRR | incidence rate ratio |
| EMR | electronic medical record |
| CTAS | Canadian Triage and Acuity Scale |
| SD | standard deviation |
| URI | upper respiratory infection |
| AGE | acute gastroenteritis |
| GI | gastrointestinal |
| PED | pediatric emergency department |
| ESIs | emergency severity indexes |
| EMS | emergency medical service |
References
- Taiwan Centers for Disease Control. Introduction of COVID-19. (27 April 2020). Available online: https://www.cdc.gov.tw/Category/Page/vleOMKqwuEbIMgqaTeXG8A (accessed on 10 March 2023).
- Lai, C.-C.; Lee, P.-I.; Hsueh, P.-R. How Taiwan has responded to COVID-19 and how COVID-19 has affected Taiwan, 2020–2022. J. Microbiol. Immunol. Infect. 2023, 56, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.-T.; Lin, C.-Y.; Tsai, M.-J.; Hung, C.-T.; Hsu, C.-W.; Lu, P.-L.; Hou, M.-F. Infection control measures of a Taiwanese hospital to confront the COVID-19 pandemic. Kaohsiung J. Med. Sci. 2020, 36, 296–304. [Google Scholar] [CrossRef]
- DeLaroche, A.M.; Rodean, J.; Aronson, P.L.; Fleegler, E.W.; Florin, T.A.; Goyal, M.; Hirsch, A.W.; Jain, S.; Kornblith, A.E.; Sills, M.R.; et al. Pediatric Emergency Department Visits at US Children’s Hospitals During the COVID-19 Pandemic. Pediatrics 2021, 147, e2020039628. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.-Y.; Chaou, C.-H.; Chang, Y.-C.; Ng, C.-J.; Chen, S.-Y. Prediction of emergency department volume and severity during a novel virus pandemic: Experience from the COVID-19 pandemic. Am. J. Emerg. Med. 2020, 46, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Baugh, J.J.; White, B.A.; McEvoy, D.; Yun, B.J.; Brown, D.F.M.; Raja, A.S.; Dutta, S. The cases not seen: Patterns of emergency department visits and procedures in the era of COVID-19. Am. J. Emerg. Med. 2021, 46, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.-W.; Huang, Y.-B.; Chao, H.-Y.; Ng, C.-J.; Chen, S.-Y. Impact of the COVID-19 Pandemic on Pediatric Emergency Medicine: A Systematic Review. Medicina 2022, 58, 1112. [Google Scholar] [CrossRef] [PubMed]
- Kostopoulou, E.; Gkentzi, D.; Papasotiriou, M.; Fouzas, S.; Tagalaki, A.; Varvarigou, A.; Dimitriou, G. The impact of COVID-19 on paediatric emergency department visits. A one-year retrospective study. Pediatr. Res. 2022, 91, 1257–1262. [Google Scholar] [CrossRef]
- Dubé, J.P.; Smith, M.M.; Sherry, S.B.; Hewitt, P.L.; Stewart, S.H. Suicide behaviors during the COVID-19 pandemic: A meta-analysis of 54 studies. Psychiatry Res. 2021, 301, 113998. [Google Scholar] [CrossRef]
- Ghaderi, H.; Stowell, J.R.; Akhter, M.; Norquist, C.; Pugsley, P.; Subbian, V. Impact of COVID-19 Pandemic on Emergency Department Visits: A Regional Case Study of Informatics Challenges and Opportunities. AMIA Annu. Symp. Proc. 2021, 2021, 496–505. [Google Scholar]
- Lai, Y.-W.; Hsu, C.-T.; Lee, Y.-T.; Chen, W.-L.; Chen, J.-H.; Huang, C.-C.; Chung, J.-Y. Analysis of COVID-19 pandemic impact on the presenting complaints of the emergency department visits. Medicine 2021, 100, e28406. [Google Scholar] [CrossRef]
- Rivera-Sepulveda, A.; Maul, T.; Dong, K.; Crate, K.; Helman, T.; Bria, C.; Martin, L.; Bogers, K.; Pearce, J.W.; Glass, T.F. Effect of the COVID-19 Pandemic on the Pediatric Emergency Department Flow. Disaster Med. Public Health Prep. 2021, 20, e83. [Google Scholar]
- Laukkanen, L.; Lahtinen, S.; Liisanantti, J.; Kaakinen, T.; Ehrola, A.; Raatiniemi, L. Early impact of the COVID-19 pandemic and social restrictions on ambulance missions. Eur. J. Public Health 2021, 31, 1090–1095. [Google Scholar] [CrossRef] [PubMed]
- Sanford, E.L.; Zagory, J.; Blackwell, J.-M.; Szmuk, P.; Ryan, M.; Ambardekar, A. Changes in pediatric trauma during COVID-19 stay-at-home epoch at a tertiary pediatric hospital. J. Pediatr. Surg. 2021, 56, 918–922. [Google Scholar] [CrossRef] [PubMed]
- Sethuraman, U.; Kannikeswaran, N.; Singer, A.; Krouse, C.B.; Cloutier, D.; Farooqi, A.; Donoghue, L.; Stankovic, C. Trauma Visits to a Pediatric Emergency Department During the COVID-19 Quarantine and “Stay at Home” Period. Am. Surg. 2021, 89, 4262–4270. [Google Scholar] [CrossRef] [PubMed]
- Nabian, M.H.; Vosoughi, F.; Najafi, F.; Khabiri, S.S.; Nafisi, M.; Veisi, J.; Rastgou, V.; Ghamari, S.; Aakhashi, A.; Bahrami, N.; et al. Epidemiological pattern of pediatric trauma in COVID-19 outbreak: Data from a tertiary trauma center in Iran. Injury 2020, 51, 2811–2815. [Google Scholar] [CrossRef] [PubMed]
- Bessoff, K.E.; Han, R.W.; Cho, M.; Stroud, M.; Urrechaga, E.M.; Thorson, C.M.; Russell, K.W.; Rohan, A.; Acker, S.N.; Swain, S.; et al. Epidemiology of pediatric trauma during the COVID-19 pandemic shelter in place. Surg. Open Sci. 2021, 6, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Fothergill, R.T.; Smith, A.L.; Wrigley, F.; Perkins, G.D. Out-of-Hospital Cardiac Arrest in London during the COVID-19 pandemic. Resusc. Plus 2020, 5, 100066. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.L.; Shahidah, N.; Saffari, S.E.; Ng, Q.X.; Ho, A.F.W.; Leong, B.S.-H.; Arulanandam, S.; Siddiqui, F.J.; Ong, M.E.H. Impact of COVID-19 on Out-of-Hospital Cardiac Arrest in Singapore. Int. J. Environ. Res. Public Health 2021, 18, 3646. [Google Scholar] [CrossRef]
- Uysal, B.; Akça, T.; Akacı, O.; Uysal, F. The Prevalence of Post-COVID-19 Hypertension in Children. Clin. Pediatr. 2022, 61, 453–460. [Google Scholar] [CrossRef]
- Verma, A.; Rajput, R.; Verma, S.; Balania, V.K.; Jangra, B. Impact of lockdown in COVID 19 on glycemic control in patients with type 1 Diabetes Mellitus. Diabetes Metab. Syndr. 2020, 14, 1213–1216. [Google Scholar] [CrossRef]
- Sharifi, H.; Ghanei, M.; Jamaati, H.; Masjedi, M.R.; Najafimehr, H.; Fakharian, A.; Eslaminejad, A. Prevalence of Asthma and Asthma-like Symptoms: A Study in Five Provinces of Iran. Tanaffos 2019, 18, 321–328. [Google Scholar] [PubMed]
- Adhikari, S.; Sathian, B.; Koirala, D.P.; Rao, K.S. Profile of children admitted with seizures in a tertiary care hospital of Western Nepal. BMC Pediatr. 2013, 13, 43. [Google Scholar] [CrossRef] [PubMed]
- Bamaga, A.K.; Alharbi, O.; Bajuaifer, M.; Batarfi, A.; Althobaiti, K.H.; AlQusaibi, B. The Effect of the COVID-19 Pandemic on Emergency Department Visits for Neurological Diseases in Saudi Arabia. Cureus 2020, 12, e12200. [Google Scholar] [CrossRef]
- Sokoloff, W.C.; Krief, W.I.; Giusto, K.A.; Mohaimin, T.; Murphy-Hockett, C.; Rocker, J.; Williamson, K.A. Pediatric emergency department utilization during the COVID-19 pandemic in New York City. Am. J. Emerg. Med. 2021, 45, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.D.; Wood, E.G.; Cohen, D.M. Reduced Emergency Department Utilization by Patients with Epilepsy Using QI Methodology. Pediatrics 2017, 139, e20152358. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Park, S. The Effect of COVID-19 on Domestic Violence and Assaults. Crim. Justice Rev. 2022, 47, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Kourti, A.; Stavridou, A.; Panagouli, E.; Psaltopoulou, T.; Spiliopoulou, C.; Tsolia, M.; Sergentanis, T.N.; Tsitsika, A. Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Trauma Violence Abus. 2021, 24, 719–745. [Google Scholar] [CrossRef] [PubMed]
- Piquero, A.R.; Jennings, W.G.; Jemison, E.; Kaukinen, C.; Knaul, F.M. Domestic violence during the COVID-19 pandemic-Evidence from a systematic review and meta-analysis. J. Crim. Justice 2021, 74, 101806. [Google Scholar] [CrossRef]
- Leeb, R.T.; Price, S.; Sliwa, S.; Kimball, A.; Szucs, L.; Caruso, E.; Godfred-Cato, S.; Lozier, M. COVID-19 Trends Among School-Aged Children—United States, March 1-September 19, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1410–1415. [Google Scholar] [CrossRef]
- Dalabih, A.; Bennett, E.; Javier, J.R.; Pediatric Policy Council. The COVID-19 pandemic and pediatric mental health: Advocating for improved access and recognition. Pediatr. Res. 2022, 91, 1018–1020. [Google Scholar] [CrossRef]
- Hill, R.M.; Rufino, K.; Kurian, S.; Saxena, J.; Saxena, K.; Williams, L. Suicide Ideation and Attempts in a Pediatric Emergency Department Before and during COVID-19. Pediatrics 2021, 147, e2020029280. [Google Scholar] [CrossRef]
- Sher, L. The impact of the COVID-19 pandemic on suicide rates. QJM Int. J. Med. 2020, 113, 707–712. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Before Epidemic (January 2019~April 2019) (n = 6009) | During Epidemic (January 2020~April 2020) (n = 4107) | Difference (%) | p-Value |
|---|---|---|---|---|
| Total visits/day— (mean ± SD) | 60.09 ± 20.5 | 40.66 ± 23.6 | −31.65 | <0.01 |
| Age—n. (%) | ||||
| 12 ≤ Age < 18 | 1388 (23.10) | 1462 (35.60) | +5.33 | 0.57 |
| Age < 12 | 4621 (76.90) | 2645 (64.40) | −42.76 | <0.01 |
| Sex—no. (%) | ||||
| Male | 3417 (56.86) | 2325 (56.61) | −31.96 | <0.01 |
| Female | 2592 (43.14) | 1782 (43.39) | −31.25 | <0.01 |
| Mode of arrival—n. (%) | ||||
| Walk-in | 3939 (65.56) | 2796 (68.08) | −29.02 | <0.01 |
| Carried | 1511 (25.14) | 675 (16.44) | −55.33 | <0.01 |
| Ambulance | 205 (3.41) | 245 (5.97) | +19.51 | <0.01 |
| Others | 354 (5.89) | 391 (9.52) | −9.46 | 0.31 |
| Triage—n. (%) | ||||
| Triage 1 | 42 (0.70) | 26 (0.63) | −38.10 | 0.04 |
| Triage 2 | 655 (10.90) | 418 (10.18) | −36.18 | <0.01 |
| Triage 3 | 4899 (81.53) | 3371 (82.08) | −31.19 | <0.01 |
| Triage 4 | 370 (6.17) | 271 (6.60) | −26.76 | <0.01 |
| Triage 5 | 43 (0.70) | 21 (0.51) | −51.16 | <0.01 |
| Disposition—n. (%) | ||||
| Admission | 640 (10.65) | 406 (9.89) | −36.56 | <0.01 |
| Discharge | 5308 (88.33) | 3670 (89.36) | −30.86 | <0.01 |
| AMA | 47 (0.78) | 18 (0.44) | −61.70 | <0.01 |
| Transfer | 12 (0.20) | 10 (0.24) | −16.67 | 0.69 |
| Mortality | 2 (0.04) | 3 (0.07) | +50.00 | 0.65 |
| Chief Complaints | Before Pandemic (January 2019~March 2019) | During Pandemic (January 2020~March 2020) | Difference (%) | Incidence Rate Ratio | p-Value | ||
|---|---|---|---|---|---|---|---|
| n | Incidence (%) | n | Incidence (%) | ||||
| Infection-related complaints | |||||||
| Fever | 2033 | 33.83 | 1254 | 30.53 | −38.32% | 0.90 | <0.01 |
| URI | 1148 | 19.10 | 697 | 16.97 | −39.29% | 0.89 | <0.01 |
| Cellulitis | 75 | 1.25 | 64 | 1.56 | −14.67% | 1.25 | 0.28 |
| Gastrointestinal-related complaints | |||||||
| Abdominal pain | 689 | 11.47 | 445 | 10.84 | −35.41% | 0.95 | <0.01 |
| AGE symptoms | 489 | 8.14 | 264 | 6.43 | −46.01% | 0.79 | <0.01 |
| Constipation | 20 | 0.33 | 11 | 0.27 | −45.00% | 0.82 | 0.09 |
| GI bleeding symptoms | 11 | 0.18 | 15 | 0.37 | 36.36% | 2.06 | 0.55 |
| Cardiovascular-related complaints | |||||||
| Chest pain | 52 | 0.87 | 98 | 2.39 | 88.46% | 2.75 | 0.01 |
| Hypertension | 2 | 0.03 | 20 | 0.49 | 900.00% | 16.33 | <0.01 |
| Neurology-related complaints | |||||||
| Dizziness | 107 | 1.78 | 96 | 2.34 | −10.28% | 1.32 | 0.46 |
| Headache | 118 | 1.96 | 52 | 1.27 | −55.93% | 0.65 | <0.01 |
| Convulsion | 50 | 0.83 | 29 | 0.71 | −42.00% | 0.35 | <0.01 |
| Altered mental status | 7 | 0.12 | 15 | 0.37 | 114.29% | 3.08 | 0.10 |
| Malaise | 12 | 0.20 | 11 | 0.27 | −8.33% | 1.35 | 0.83 |
| Myalgia | 65 | 0.01 | 83 | 2.02 | 27.69% | 202.00 | 0.65 |
| Shortness of breath | 155 | 2.58 | 135 | 3.29 | −12.90% | 1.26 | 0.28 |
| Glycemic problems | 3 | 0.05 | 11 | 0.27 | 266.67% | 5.40 | 0.07 |
| Urological symptoms | 78 | 1.30 | 58 | 1.41 | −25.64% | 1.09 | 0.12 |
| Trauma | 1401 | 23.31 | 970 | 23.62 | −30.76% | 1.01 | <0.01 |
| Facial feature problems + | 217 | 3.61 | 106 | 2.58 | −51.15% | 0.72 | <0.01 |
| Cardiac arrest | 2 | 0.03 | 6 | 0.15 | 200% | 5.00 | 0.31 |
| Psychological problems | 6 | 0.10 | 19 | 0.46 | 216.67% | 4.60 | 0.03 |
| Social problems * | 13 | 0.22 | 13 | 0.32 | 0% | 1.46 | 0.71 |
| Others | 49 | 0.82 | 18 | 0.44 | −63.27% | 0.54 | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-T.; Lai, Y.-W.; Chen, J.-H.; Chen, W.-L.; Wu, M.-Y.; Chung, J.-Y. Assessing the Impact of the COVID-19 Pandemic on Pediatric Emergency Department Visits in Taiwan. Medicina 2024, 60, 288. https://doi.org/10.3390/medicina60020288
Lee Y-T, Lai Y-W, Chen J-H, Chen W-L, Wu M-Y, Chung J-Y. Assessing the Impact of the COVID-19 Pandemic on Pediatric Emergency Department Visits in Taiwan. Medicina. 2024; 60(2):288. https://doi.org/10.3390/medicina60020288
Chicago/Turabian StyleLee, Yu-Ting, Yen-Wen Lai, Jiann-Hwa Chen, Wei-Lung Chen, Meng-Yu Wu, and Jui-Yuan Chung. 2024. "Assessing the Impact of the COVID-19 Pandemic on Pediatric Emergency Department Visits in Taiwan" Medicina 60, no. 2: 288. https://doi.org/10.3390/medicina60020288