

Thyroid Disease and Systemic Lupus Erythematosus
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Clinical Thyroid Disease in the SLE and Control Groups
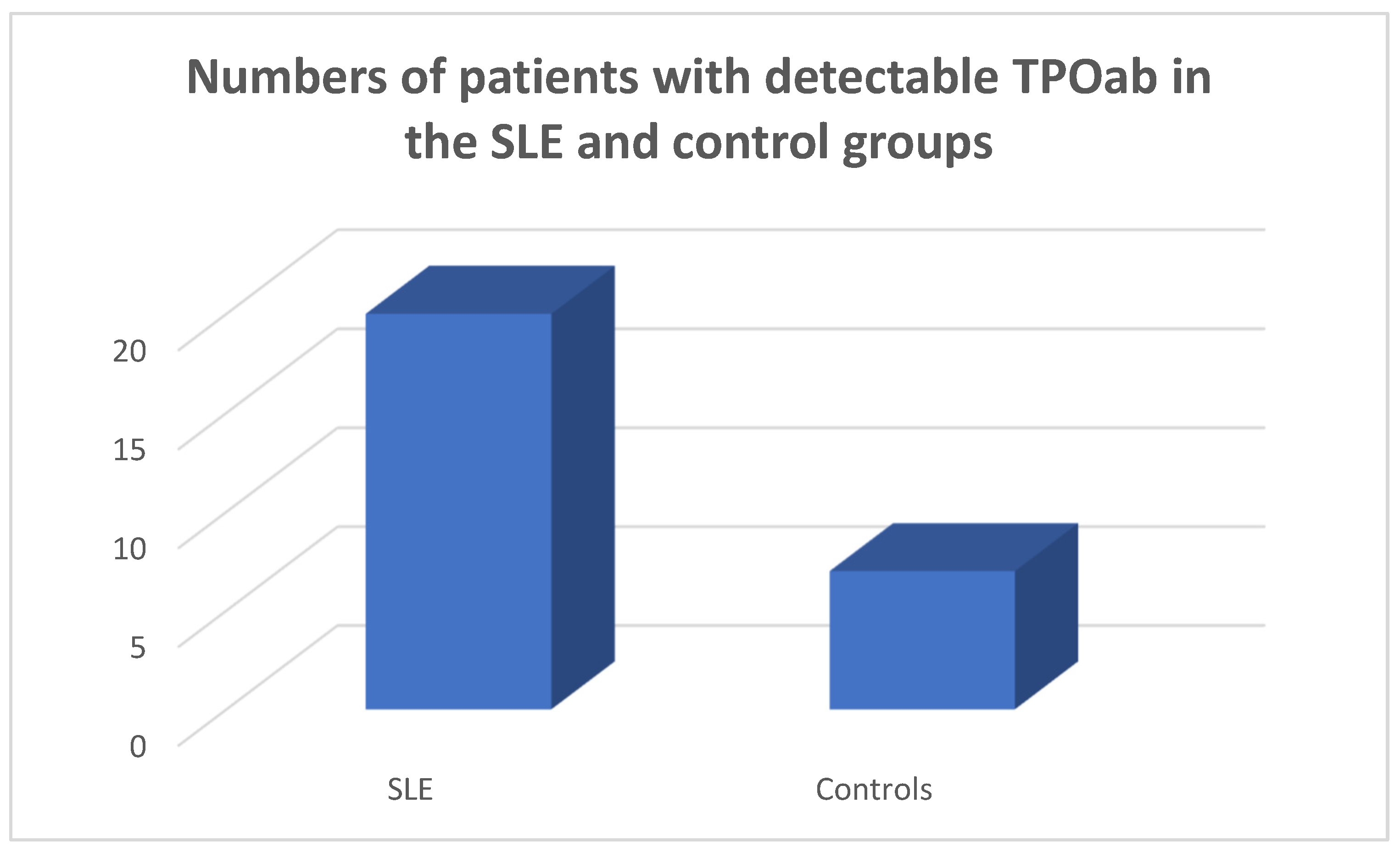
3.2. Antithytoid Antibodies in the SLE and Control Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tsokos, G.C. Systemic lupus erythematosus. N. Engl. J. Med. 2011, 365, 2110–2121. [Google Scholar] [CrossRef]
- Yu, H.; Nagafuchi, Y.; Fujio, K. Clinical and Immunological Biomarkers for Systemic Lupus Erythematosus. Biomolecules 2021, 11, 928. [Google Scholar] [CrossRef] [PubMed]
- Kiriakidou, M.; Ching, C.L. Systemic Lupus Erythematosus. Ann. Intern. Med. 2020, 172, itc81–itc96. [Google Scholar] [CrossRef] [PubMed]
- Prabhat, N.; Chakravarty, K.; Pattnaik, S.N.; Takkar, A.; Ray, S.; Lal, V. Systemic lupus erythematosus with autoimmune neurological manifestations in a carrier of chronic granulomatous disease—A rare presentation. J. Neuroimmunol. 2020, 343, 577229. [Google Scholar] [CrossRef]
- Fortuna, G.; Brennan, M.T. Systemic lupus erythematosus: Epidemiology, pathophysiology, manifestations, and management. Dent. Clin. N. Am. 2013, 57, 631–655. [Google Scholar] [CrossRef] [PubMed]
- Zucchi, D.; Elefante, E.; Schilirò, D.; Signorini, V.; Trentin, F.; Bortoluzzi, A.; Tani, C. One year in review 2022: Systemic lupus erythematosus. Clin. Exp. Rheumatol. 2022, 40, 4–14. [Google Scholar] [CrossRef]
- Posselt, R.T.; Coelho, V.N.; Skare, T.L. Hashimoto thyroiditis, anti-thyroid antibodies and systemic lupus erythematosus. Int. J. Rheum. Dis. 2018, 21, 186–193. [Google Scholar] [CrossRef]
- Garber, J.J.; Worthington, J.W.; Randall, R.V.; Kierland, R.R. Lupus erythematosus and hashimoto’s thyroiditis. Postgrad. Med. 1969, 46, 100–105. [Google Scholar] [CrossRef]
- Duan, L.; Shi, Y.; Feng, Y. Systemic lupus erythematosus and thyroid disease: A Mendelian randomization study. Clin. Rheumatol. 2023, 42, 2029–2035. [Google Scholar] [CrossRef]
- Saettini, F.; Cattoni, A.; Redaelli, M.; Silvestri, D.; Ferrari, G.M.; Biondi, A.; Jankovic, M.; Spinelli, M. Primary immunodeficiencies, autoimmune hyperthyroidism, coeliac disease and systemic lupus erythematosus in childhood immune thrombocytopenia. Acta Paediatr. 2021, 110, 643–651. [Google Scholar] [CrossRef]
- Boutzios, G.; Koukoulioti, E.; Goules, A.V.; Kalliakmanis, I.; Giovannopoulos, I.; Vlachoyiannopoulos, P.; Moutsopoulos, H.M.; Tzioufas, A.G. Hashimoto Thyroiditis, Anti-Parietal Cell Antibodies: Associations with Autoimmune Diseases and Malignancies. Front. Endocrinol. 2022, 13, 860880. [Google Scholar] [CrossRef] [PubMed]
- Conigliaro, P.; D’Antonio, A.; Pinto, S.; Chimenti, M.S.; Triggianese, P.; Rotondi, M.; Perricone, R. Autoimmune thyroid disorders and rheumatoid arthritis: A bidirectional interplay. Autoimmun. Rev. 2020, 19, 102529. [Google Scholar] [CrossRef] [PubMed]
- Andonopoulos, A.P.; Siambi, V.; Makri, M.; Christofidou, M.; Markou, C.; Vagenakis, A.G. Thyroid function and immune profile in rheumatoid arthritis. A controlled study. Clin. Rheumatol. 1996, 15, 599–603. [Google Scholar] [CrossRef] [PubMed]
- Meena, L.; Chejara, R.; Meena, P.D.; Nawal, C.L.; Vedwal, A. A Study to Evaluate the Thyroid Function in Sero Positive Rheumatoid Arthritis. J. Assoc. Physicians India 2022, 70, 11–12. [Google Scholar]
- Girón-Pïllado, M.; Cruz-Bautista, I.; Saavedra-González, V.; Atisha-Fregoso, Y.; Barraza, G.; Aguilar-Salinas, C.A.; Hernández-Molina, G. Autoimmune Thyroid Disease in Primary Sjögren’s Syndrome: Real-life Screening Practice and Clinical Outcomes. Curr. Rheumatol. Rev. 2022, 18, 272–277. [Google Scholar] [CrossRef]
- Anaya, J.M.; Restrepo-Jiménez, P.; Rodríguez, Y.; Rodríguez-Jiménez, M.; Acosta-Ampudia, Y.; Monsalve, D.M.; Pacheco, Y.; Ramirez-Santana, C.; Molano-Gonzalez, N.; Mantilla, R.D. Sjögren’s Syndrome and Autoimmune Thyroid Disease: Two Sides of the Same Coin. Clin. Rev. Allergy Immunol. 2019, 56, 362–374. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, P.; Ruffilli, I.; Giuggioli, D.; Colaci, M.; Ferrari, S.M.; Antonelli, A.; Ferri, C. Associations between Systemic Sclerosis and Thyroid Diseases. Front. Endocrinol. 2017, 8, 266. [Google Scholar] [CrossRef]
- Weetman, A.P. An update on the pathogenesis of Hashimoto’s thyroiditis. J. Endocrinol. Investig. 2021, 44, 883–890. [Google Scholar] [CrossRef]
- Kurimoto, C.; Inaba, H.; Ariyasu, H.; Iwakura, H.; Ueda, Y.; Uraki, S.; Takeshima, K.; Furukawa, Y.; Morita, S.; Yamamoto, S.; et al. Predictive and sensitive biomarkers for thyroid dysfunctions during treatment with immune-checkpoint inhibitors. Cancer Sci. 2020, 111, 1468–1477. [Google Scholar] [CrossRef]
- Zhang, Q.Y.; Ye, X.P.; Zhou, Z.; Zhu, C.F.; Li, R.; Fang, Y.; Zhang, R.-J.; Li, L.; Liu, W.; Wang, Z.; et al. Lymphocyte infiltration and thyrocyte destruction are driven by stromal and immune cell components in Hashimoto’s thyroiditis. Nat. Commun. 2022, 13, 775. [Google Scholar] [CrossRef]
- Katsuyama, T.; Tsokos, G.C.; Moulton, V.R. Aberrant T Cell Signaling and Subsets in Systemic Lupus Erythematosus. Front. Immunol. 2018, 9, 1088. [Google Scholar] [CrossRef] [PubMed]
- Tobón, G.J.; Izquierdo, J.H.; Cañas, C.A. B lymphocytes: Development, tolerance, and their role in autoimmunity-focus on systemic lupus erythematosus. Autoimmune Dis. 2013, 2013, 827254. [Google Scholar] [CrossRef]
- Kausman, D.; Isenberg, D.A. Thyroid autoimmunity in systemic lupus erythematosus: The clinical significance of a fluctuating course. Br. J. Rheumatol. 1995, 34, 361–364. [Google Scholar] [CrossRef]
- Hijmans, W.; Doniach, D.; Roitt, I.M.; Holborow, E.J. Serological overlap between lupus erythematosus, rheumatoid arthritis, and thyroid auto-immune disease. Br. Med. J. 1961, 2, 909–914. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.W.; Moore, G.F.; Weintraub, B.D.; Steinberg, A.D. Prevalence of thyroid disease and abnormal thyroid function test results in patients with systemic lupus erythematosus. Arthritis Rheum. 1987, 30, 1124–1131. [Google Scholar] [CrossRef]
- Boey, M.L.; Fong, P.H.; Lee, J.S.; Ng, W.Y.; Thai, A.C. Autoimmune thyroid disorders in SLE in Singapore. Lupus 1993, 2, 51–54. [Google Scholar] [CrossRef]
- Park, D.J.; Cho, C.S.; Lee, S.H.; Park, S.H.; Kim, H.Y. Thyroid disorders in Korean patients with systemic lupus erythematosus. Scand. J. Rheumatol. 1995, 24, 13–17. [Google Scholar] [CrossRef]
- Kohno, Y.; Naito, N.; Saito, K.; Hoshioka, A.; Niimi, H.; Nakajima, H.; Hosoya, T. Anti-thyroid peroxidase antibody activity in sera of patients with systemic lupus erythematosus. Clin. Exp. Immunol. 1989, 75, 217–221. [Google Scholar]
- Kumar, K.; Kole, A.K.; Karmakar, P.S.; Ghosh, A. The spectrum of thyroid disorders in systemic lupus erythematosus. Rheumatol. Int. 2012, 32, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Mulhern, L.M.; Masi, A.T.; Shulman, L.E. Hashimoto’s disease. A search for associated disorders in 170 clinically detected cases. Lancet 1966, 2, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Goh, K.L.; Wang, F. Thyroid disorders in systemic lupus erythematosus. Ann. Rheum. Dis. 1986, 45, 579–583. [Google Scholar] [CrossRef] [PubMed]
- Byron, M.A.; Mowat, A.G. Thyroid disorders in systemic lupus erythematosus. Ann. Rheum. Dis. 1987, 46, 174–175. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yuan, J.; Zhou, H.; Wang, Y.; Tian, G.; Liu, X.; Wang, X.; Tang, M.; Mang, X.; Kou, C.; et al. Association Between Systemic Lupus Erythematosus and Primary Hypothyroidism: Evidence from Complementary Genetic Methods. J. Clin. Endocrinol. Metab. 2023, 108, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Szanto, A.; Szodoray, P.; Kiss, E.; Kapitany, A.; Szegedi, G.; Zeher, M. Clinical, serologic, and genetic profiles of patients with associated Sjögren’s syndrome and systemic lupus erythematosus. Hum. Immunol. 2006, 67, 924–930. [Google Scholar] [CrossRef]
- Qin, Q.; Zhao, L.; Ren, A.; Li, W.; Ma, R.; Peng, Q.; Luo, S. Systemic lupus erythematosus is causally associated with hypothyroidism, but not hyperthyroidism: A Mendelian randomization study. Front. Immunol. 2023, 14, 1125415. [Google Scholar] [CrossRef]
- Lazúrová, I.; Benhatchi, K.; Rovenský, J.; Kozáková, D.; Wagnerová, H.; Tajtáková, M.; Shoenfeld, Y.; Macejova, Z. Autoimmune thyroid disease and autoimmune rheumatic disorders: A two-sided analysis. Ann. N. Y. Acad. Sci. 2009, 1173, 211–216. [Google Scholar] [CrossRef]
- Weetman, A.P. Diseases associated with thyroid autoimmunity: Explanations for the expanding spectrum. Clin. Endocrinol. 2011, 74, 411–418. [Google Scholar] [CrossRef]
- Odin, V.I.; Dvorovkin, A.E.; Inamova, O.V.; Tyrenko, V.V.; Gumilevskaya, O.P. Features of the ontogenetic forms of rheumatoid arthritis associated with autoimmune thyroiditis. Adv. Gerontol. 2018, 31, 125–131. [Google Scholar]
- Lazúrová, I.; Jochmanová, I.; Benhatchi, K.; Sotak, S. Autoimmune thyroid disease and rheumatoid arthritis: Relationship and the role of genetics. Immunol. Res. 2014, 60, 193–200. [Google Scholar] [CrossRef]
- Hart, F.D. Rheumatoid arthritis: Extra-articular manifestations. II. Br. Med. J. 1970, 2, 747–752. [Google Scholar] [CrossRef]
- Cárdenas Roldán, J.; Amaya-Amaya, J.; Castellanos-de la Hoz, J.; Giraldo-Villamil, J.; Montoya-Ortiz, G.; Cruz-Tapias, P.; Rojas-Villarraga, A.; Mantilla, R.D.; Anaya, J.M. Autoimmune thyroid disease in rheumatoid arthritis: A global perspective. Arthritis 2012, 2012, 864907. [Google Scholar] [CrossRef]
- El-Sherif, W.T.; El Gendi, S.S.; Ashmawy, M.M.; Ahmed, H.M.; Salama, M.M. Thyroid disorders and autoantibodies in systemic lupus erythematosus and rheumatoid arthritis patients. Egypt. J. Immunol. 2004, 11, 81–90. [Google Scholar]
- Nakamura, H.; Usa, T.; Motomura, M.; Ichikawa, T.; Nakao, K.; Kawasaki, E.; Tanaka, M.; Ishikawa, K.; Eguchi, K. Prevalence of interrelated autoantibodies in thyroid diseases and autoimmune disorders. J. Endocrinol. Investig. 2008, 31, 861–865. [Google Scholar] [CrossRef]
- Chen, Y.L.; Lin, J.Z.; Mo, Y.Q.; Liang, J.J.; Li, Q.H.; Zhou, C.J.; Wei, X.-N.; Ma, J.-D.; Yang, Z.-H.; Zheng, D.-H.; et al. Joint damage is amplified in rheumatoid arthritis patients with positive thyroid autoantibodies. PeerJ. 2018, 6, e4216. [Google Scholar] [CrossRef] [PubMed]
- Barsotti, S.; Stagnaro, C.; d’Ascanio, A.; Della Rossa, A. One year in review 2016: Systemic sclerosis. Clin. Exp. Rheumatol. 2016, 34 (Suppl. S100), 3–13. [Google Scholar] [PubMed]
- Wimmersberger, Y.; Zuercher, D. Graves’ disease associated with primary systemic sclerosis. Orbit 2009, 28, 262–263. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, S.M.; Rapoport, B. Breaking tolerance to thyroid antigens: Changing concepts in thyroid autoimmunity. Endocr. Rev. 2014, 35, 59–105. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Hegedüs, L. Graves’ Disease. N. Engl. J. Med. 2016, 375, 1552–1565. [Google Scholar] [CrossRef]
- Caturegli, P.; De Remigis, A.; Rose, N.R. Hashimoto thyroiditis: Clinical and diagnostic criteria. Autoimmun. Rev. 2014, 13, 391–397. [Google Scholar] [CrossRef]
- McLachlan, S.M.; Rapoport, B. Why measure thyroglobulin autoantibodies rather than thyroid peroxidase autoantibodies? Thyroid 2004, 14, 510–520. [Google Scholar] [CrossRef]
- Rose, N.R. Prediction and prevention of autoimmune disease: A personal perspective. Ann. N. Y. Acad. Sci. 2007, 1109, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Antonelli, A.; Fallahi, P.; Mosca, M.; Ferrari, S.M.; Ruffilli, I.; Corti, A.; Panicucci, E.; Neri, E.; Bombardieri, S. Prevalence of thyroid dysfunctions in systemic lupus erythematosus. Metabolism 2010, 59, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Annunziata, P.; Lore, F.; Venturini, E.; Morana, P.; Guarino, E.; Borghi, S.; Guazzi, G.C. Early synthesis and correlation of serum anti-thyroid antibodies with clinical parameters in multiple sclerosis. J. Neurol. Sci. 1999, 168, 32–36. [Google Scholar] [CrossRef]
- Scappaticcio, L.; Castellana, M.; Virili, C.; Bellastella, G.; Centanni, M.; Cannavò, S.; Campenni, A.; Ruggeri, R.M.; Giovanella, L.; Trimboli, P. Alemtuzumab-induced thyroid events in multiple sclerosis: A systematic review and meta-analysis. J. Endocrinol. Investig. 2020, 43, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Strieder, T.G.; Tijssen, J.G.; Wenzel, B.E.; Endert, E.; Wiersinga, W.M. Prediction of progression to overt hypothyroidism or hyperthyroidism in female relatives of patients with autoimmune thyroid disease using the Thyroid Events Amsterdam (THEA) score. Arch. Intern. Med. 2008, 168, 1657–1663. [Google Scholar] [CrossRef] [PubMed]
- Tsokos, G.C.; Lo, M.S.; Costa Reis, P.; Sullivan, K.E. New insights into the immunopathogenesis of systemic lupus erythematosus. Nat. Rev. Rheumatol. 2016, 12, 716–730. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, R.; Cheung, A.S.; Pang, K.; Saffery, R.; Novakovic, B. Sexual Dimorphism in Innate Immunity: The Role of Sex Hormones and Epigenetics. Front. Immunol. 2020, 11, 604000. [Google Scholar] [CrossRef] [PubMed]
- Shoenfeld, Y.; Tincani, A.; Gershwin, M.E. Sex gender and autoimmunity. J. Autoimmun. 2012, 38, J71–J73. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Elia, G.; Virili, C.; Centanni, M.; Antonelli, A.; Fallahi, P. Systemic Lupus Erythematosus and Thyroid Autoimmunity. Front. Endocrinol. 2017, 8, 138. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SLE Patients | |
|---|---|
| Age | 47.97 ± 2.17 |
| Sex | 41 F/4 M |
| SLE disease duration | 5.71 ± 0.49 |
| SLEDAI-2K | 9.24 ± 0.65 |
| Leucopenia | 35% |
| Cutaneous involvement | 32% |
| Renal involvement | 28.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Athanassiou, L.; Kostoglou-Athanassiou, I.; Kaiafa, G.; Tsakiridis, P.; Koukosias, N.; Mitsoulis, S.; Savopoulos, C.; Athanassiou, P. Thyroid Disease and Systemic Lupus Erythematosus. Medicina 2023, 59, 1911. https://doi.org/10.3390/medicina59111911
Athanassiou L, Kostoglou-Athanassiou I, Kaiafa G, Tsakiridis P, Koukosias N, Mitsoulis S, Savopoulos C, Athanassiou P. Thyroid Disease and Systemic Lupus Erythematosus. Medicina. 2023; 59(11):1911. https://doi.org/10.3390/medicina59111911
Chicago/Turabian StyleAthanassiou, Lambros, Ifigenia Kostoglou-Athanassiou, Georgia Kaiafa, Pavlos Tsakiridis, Nikolaos Koukosias, Spyridon Mitsoulis, Christos Savopoulos, and Panagiotis Athanassiou. 2023. "Thyroid Disease and Systemic Lupus Erythematosus" Medicina 59, no. 11: 1911. https://doi.org/10.3390/medicina59111911