
An Evaluation of the Hitit Index in Differential Diagnosis of Crimean-Congo Hemorrhagic Fever in the Emergency Department
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spengler, J.R.; Bergeron, É.; Spiropoulou, C.F. Crimean-Congo hemorrhagic fever and expansion from endemic regions. Curr. Opin. Virol. 2019, 34, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Shahhosseini, N.; Wong, G.; Babuadze, G.; Camp, J.V.; Ergonul, O.; Kobinger, G.P.; Chinikar, S.; Nowotny, N. Crimean-Congo hemorrhagic fever virus in Asia, Africa and Europe. Microorganisms 2021, 9, 1907. [Google Scholar] [CrossRef] [PubMed]
- Raabe, V.N. Diagnostic testing for Crimean-Congo hemorrhagic fever. J. Clin. Microbiol. 2020, 58, e01580-19. [Google Scholar] [CrossRef] [PubMed]
- Fillâtre, P.; Revest, M.; Tattevin, P. Crimean-Congo hemorrhagic fever: An update. Med. Mal. Infect. 2019, 49, 574–585. [Google Scholar] [PubMed]
- Whitehouse, C.A. Crimean–Congo hemorrhagic fever. Antiviral Res. 2004, 64, 145–160. [Google Scholar] [CrossRef] [PubMed]
- Statistical Data for Crimean-Congo Hemorrhagic Fever. Available online: https://hsgmdestek.saglik.gov.tr/tr/zoonotikvektorel-kkka/zoonotikvektorel-kkka-istatistik (accessed on 1 April 2023).
- Kayadibi, H.; Yapar, D.; Akdogan, O.; Ulusu, N.N.; Baykam, N. Hitit Index to distinguish patients with and without Crimean-Congo hemorrhagic fever. Ticks Tick-Borne Dis. 2019, 10, 1035–1040. [Google Scholar] [CrossRef] [PubMed]
- Uyar, Y.; Carhan, A.; Albayrak, N.; Altaş, A.B. Evaluation of PCR and ELISA-IgM results in the laboratory diagnosis of Crimean-Congo haemorrhagic fever cases in 2008 in Turkey. Mikrobiyol. Bul. 2010, 44, 57–64. [Google Scholar] [PubMed]
- Statistical Data for Crimean-Congo Hemorrhagic Fever. Available online: https://hsgmdestek.saglik.gov.tr/tr/zoonotikvektorel-kkka/detay.html (accessed on 1 April 2023).
- Okely, M.; Anan, R.; Gad-Allah, S.; Samy, A.M. Mapping the environmental suitability of etiological agent and tick vectors of Crimean-Congo hemorrhagic fever. Acta Trop. 2020, 203, 105319. [Google Scholar] [CrossRef]
- Chinikar, S.; Shayesteh, M.; Khakifirouz, S.; Jalali, T.; Rasi Varaie, F.S.; Rafigh, M.; Mostafavi, E.; Shah-Hosseini, N. Nosocomial infection of Crimean–Congo haemorrhagic fever in eastern Iran: Case report. Travel Med. Infect. Dis. 2013, 11, 252–255. [Google Scholar] [CrossRef] [PubMed]
- Ergönül, Ö.; Çelikbaş, A.; Dokuzoğuz, B.; Eren, Ş.; Baykam, N.; Esener, H. Characteristics of patients with Crimean-Congo hemorrhagic fever in a recent outbreak in Turkey and impact of oral ribavirin therapy. Clin. Infect. Dis. 2004, 39, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Maupin, G.O.; Rollin, P.E.; Noor, A.M.; Shurie, H.H.; Shalabi, A.G.; Wasef, S.; Haddad, Y.M.; Sadek, R.; Ijaz, K.; et al. An outbreak of Crimean-Congo hemorrhagic fever in the United Arab Emirates, 1994–1995. Am. J. Trop. Med. Hyg. 1997, 57, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Bente, D.A.; Forrester, N.L.; Watts, D.M.; McAuley, A.J.; Whitehouse, C.A.; Bray, M. Crimean-Congo hemorrhagic fever: History, epidemiology, pathogenesis, clinical syndrome and genetic diversity. Antiviral Res. 2013, 100, 159–189. [Google Scholar] [PubMed]
- World Health Organization. Summary Report on the Meeting on Prevention and Control of Crimean–Congo Haemorrhagic Fever in the Eastern Mediterranean Region, Muscat, Oman, 7–9 December 2015; World Health Organization: Geneva, Switzerland; Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2016. [Google Scholar]
- Sidira, P.; Maltezou, H.; Haidich, A.B.; Papa, A. Seroepidemiological study of Crimean-Congo haemorrhagic fever in Greece, 2009–2010. Clin. Microbiol. Infect. 2012, 18, E16–E19. [Google Scholar] [CrossRef] [PubMed]
- Ceianu, C.S.; Panculescu-Gatej, R.I.; Coudrier, D.; Bouloy, M. First serologic evidence for the circulation of Crimean-Congo hemorrhagic fever virus in Romania. Vector Borne Zoonotic Dis. 2012, 12, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Bodur, H.; Akinci, E.; Ascioglu, S.; Öngürü, P.; Uyar, Y. Subclinical infections with Crimean-Congo hemorrhagic fever virus, Turkey. Emerg. Infect. Dis. 2012, 18, 640. [Google Scholar] [CrossRef] [PubMed]
- Ergönül, Ö. Crimean-Congo haemorrhagic fever. Lancet Infect. Dis. 2006, 6, 203–214. [Google Scholar] [PubMed]
- Komut, S.; Erenler, A.K.; Yapar, D.; Baykam, N. Use of Routine Laboratory Tests for Diagnosis of Crimean-Congo Hemorrhagic Fever Disease in Emergency Department. Exp. Appl. Med. Sci. 2022, 3, 312–317. [Google Scholar]
- Ardalan, M.R.; Shane, T.R.; Chinikar, S.; Shoja, M.M. Crimean–Congo haemorrhagic fever presenting as thrombotic microangiopathy and acute renal failure. Nephrol. Dial. Transplant. 2006, 21, 2304–2307. [Google Scholar] [CrossRef] [PubMed]
- Akinci, E.; Bodur, H.; Sunbul, M.; Leblebicioglu, H. Prognostic factors, pathophysiology and novel biomarkers in Crimean-Congo hemorrhagic fever. Antiviral Res. 2016, 132, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Kraus, A.A.; Mirazimi, A. Molecular biology and pathogenesis of Crimean–Congo hemorrhagic fever virus. Future Virol. 2010, 5, 469–479. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Definition |
| At least 2 of the following 4 clinical criteria: 1. At least 2 of the following complaints:
2. Findings of bleeding of the skin and mucosa 3. Thrombocytopenia and/or leukopenia which cannot be explained by another reason 4. Elevated ALT and AST which cannot be explained by another reason |
| Epidemiological Criteria |
| Within the 2 weeks prior to disease onset: 1. A history of tick contact or attachment 2. A history of contact with animal blood, tissue, or secretions 3. Living in a rural area or history of travel to a rural area 4. A history of close contact with a diagnosed case |
| Laboratory Criteria |
| 1. Virus isolation 2. Determination of virus-specific IgM antibody positivity 3. Determination of an increase of >4 fold in virus-specific IgG titer in the serum in the acute and convalescent periods 4. Determination of viral nucleic acid |
| Diagnostic Status for CCHF | ||||
|---|---|---|---|---|
| CCHF Excluded (n = 201) | Diagnosed with CCHF (n = 72) | p-Values | ||
| INR | 1.06 ± 0.10 1.04 (0.88–1.78) | 1.11 ± 0.22 1.07 (0.09–1.64) | 0.095 a | |
| Fibrinogen | 266.3 ± 119.2 256 (110–684) | 251.8 ± 78.12 234.5 (105–457) | 0.563 a | |
| Direct Bilirubin | 0.12 ± 0.10 0.11 (0.03–1.23) | 0.16 ± 0.10 0.13 (0.04–0.58) | <0.001 a | |
| AST | 33.83 ± 56.61 22 (10–544) | 206.8 ± 275.5 110.5 (1–1776) | <0.001 a | |
| CK | 244.5 ± 888.3 122 (0–12228) | 682.8 ± 1044 231 (21–4653) | <0.001 a | |
| CKDEPI | 92 ± 24.14 95 (6–156) | 92.35 ± 24.92 93 (28–145) | 0.764 | |
| Lymphocyte | 2.24 ± 1.04 2.20 (0.22–5.99) | 0.68 ± 0.39 0.56 (0.16–1.82) | <0.001 a | |
| HTC | 40.86 ± 4.80 41.3 (14.7–50.2) | 39.32 ± 6.07 39.65 (13.4–54.2) | 0.020 a | |
| Neutrophil | 4.68 ± 2.29 4.31 (1.27–20.97) | 2.17 ± 2.19 1.4 (0.34–11.91) | <0.001 a | |
| RBC | 4.79 ± 0.6 4.79 (1.02–7) | 4.77 ± 0.61 4.74 (3.22–6.70) | 0.601 a | |
| Conjunctival Hyperemia | No | 167 (83.1%) | 47 (65.3%) | 0.002 b |
| Yes | 34 (16.9%) | 25 (34.7%) | ||
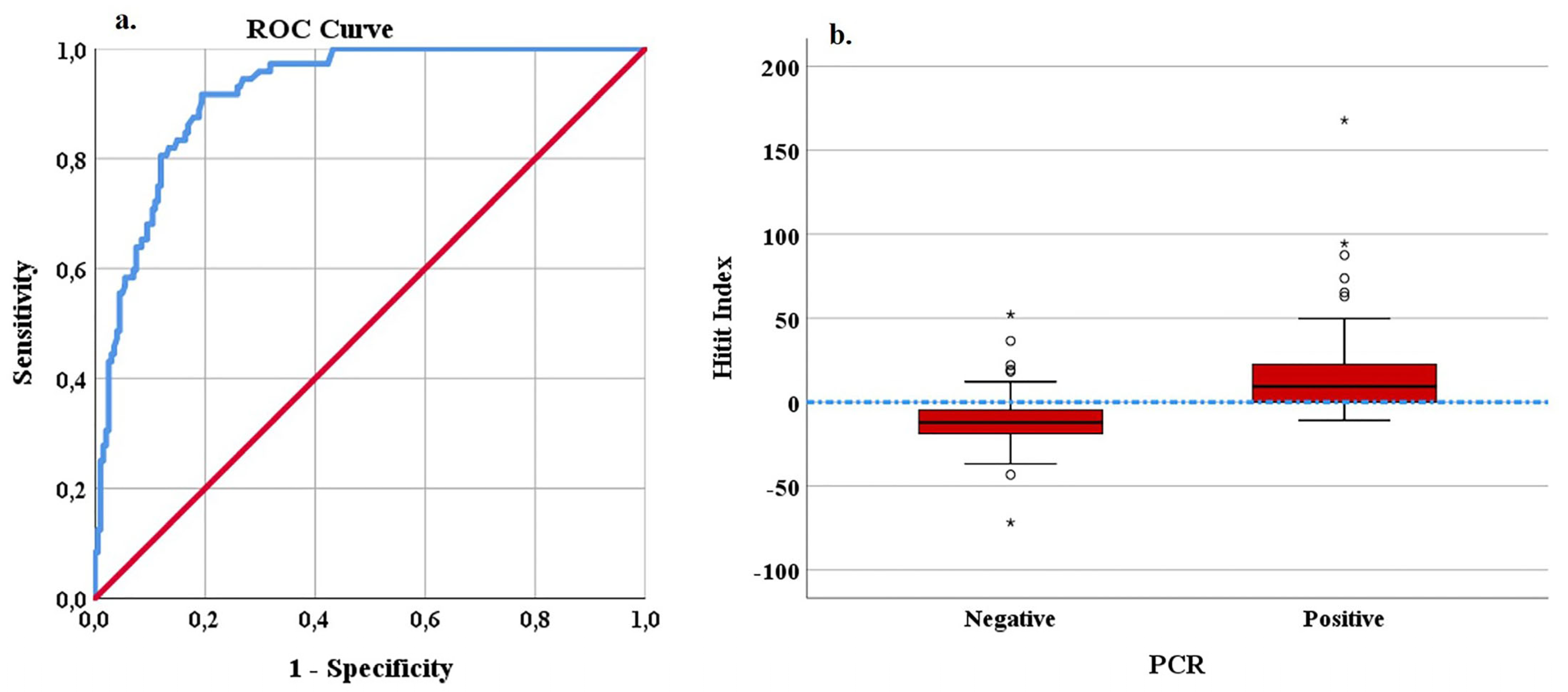
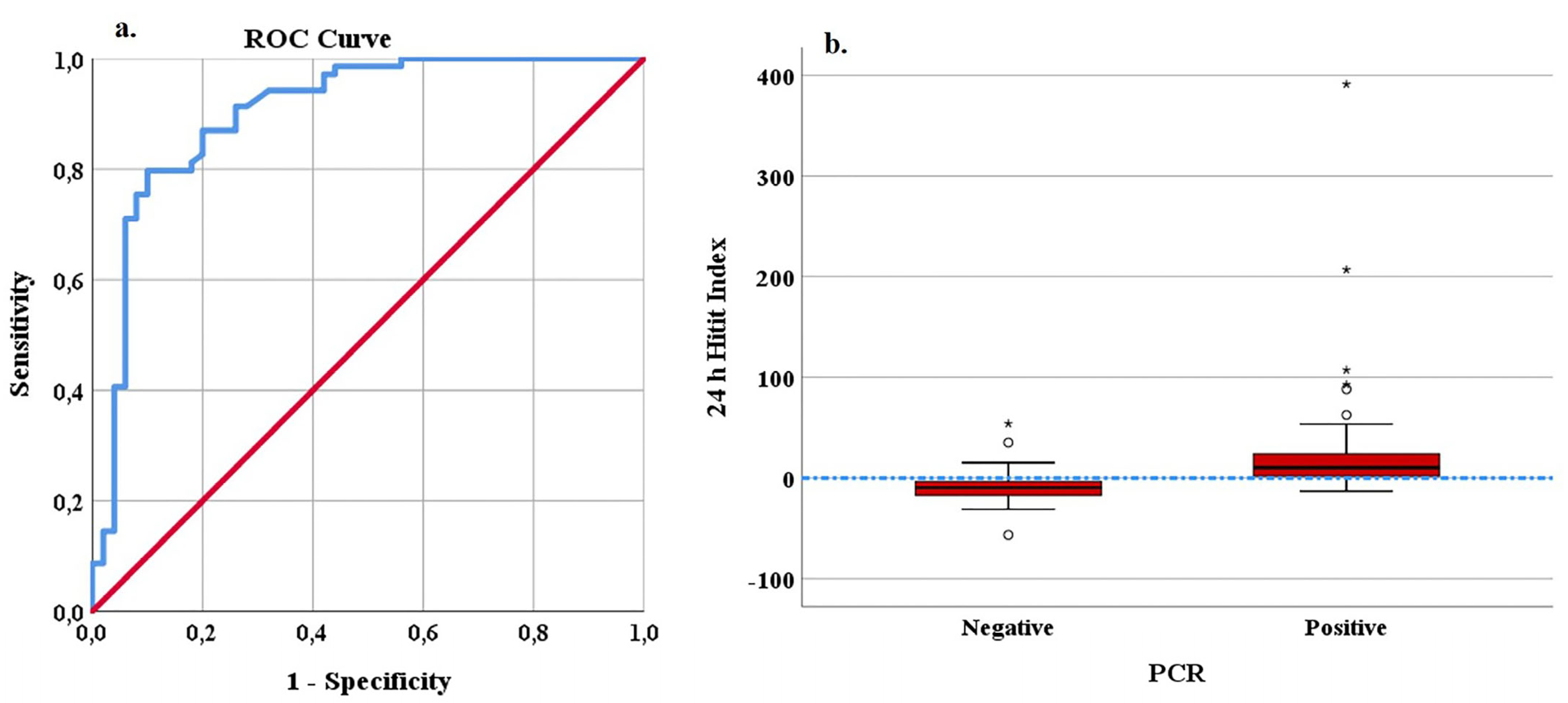
| Hitit Index (n = 273) | Hitit Index (n = 273) | 24 h Hitit Index (n = 119) | 24 h Hitit Index (n = 119) | |
|---|---|---|---|---|
| Cut off | ≥0 | ≥−3.55 | ≥0 | ≥0.85 |
| AUC | 0.919 (0.887–0.951) | 0.919 (0.887–0.951) | 0.902 (0.841–0.962) | 0.902 (0.841–0.962) |
| Sensitivity (95% CI) | 0.75 (0.631–0.841) | 0.916 (0.821–0.965) | 0.797 (0.679–0.880) | 0.797 (0.679–0.880) |
| Specificity (95% CI) | 0.880 (0.825–0.920) | 0.805 (0.743–0.856) | 0.84 (0.703–0.923) | 0.9 (0.774–0.962) |
| Accuracy | 0.846 | 0.835 | 0.815 | 0.840 |
| PPV (95% CI) | 0.692 (0.576–0.789) | 0.628 (0.528–0.719) | 0.873 (0.759–0.939) | 0.916 (0.808–0.968) |
| NPV (95% CI) | 0.907 (0.855–0.942) | 0.964 (0.920–0.985) | 0.75 (0.613–0.851) | 0.762 (0.631–0.859) |
| LR+ (95% CI) | 6.28 (4.21–9.35) | 4.72 (3.53–6.31) | 4.98 (2.61–9.50) | 7.97 (3.44–18.46) |
| Cut-Off | PCR | Total | ||
|---|---|---|---|---|
| Negative | Positive | |||
| Hitit Index | Negative (<0) | 177 | 18 | 195 |
| Positive (≥0) | 24 | 54 | 78 | |
| Hitit Index | Negative (<−3.55) | 162 | 6 | 168 |
| Positive (≥−3.55) | 39 | 66 | 105 | |
| Total | 201 | 72 | 273 | |
| 24 h Hitit Index | Negative (<0) | 42 | 14 | 56 |
| Positive (≥0) | 8 | 55 | 63 | |
| 24 h Hitit Index | Negative (<0.85) | 45 | 14 | 59 |
| Positive (≥0.85) | 5 | 55 | 60 | |
| Total | 50 | 69 | 119 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Komut, S.; Çorakyer, N.; Kaplan, G.; Baykam, N. An Evaluation of the Hitit Index in Differential Diagnosis of Crimean-Congo Hemorrhagic Fever in the Emergency Department. Medicina 2023, 59, 1796. https://doi.org/10.3390/medicina59101796
Komut S, Çorakyer N, Kaplan G, Baykam N. An Evaluation of the Hitit Index in Differential Diagnosis of Crimean-Congo Hemorrhagic Fever in the Emergency Department. Medicina. 2023; 59(10):1796. https://doi.org/10.3390/medicina59101796
Chicago/Turabian StyleKomut, Seval, Nurullah Çorakyer, Gülcan Kaplan, and Nurcan Baykam. 2023. "An Evaluation of the Hitit Index in Differential Diagnosis of Crimean-Congo Hemorrhagic Fever in the Emergency Department" Medicina 59, no. 10: 1796. https://doi.org/10.3390/medicina59101796