
Innovative Use of Biodex Balance System to Improve Dynamic Stabilization and Function of Upper Quarter in Recreational Weightlifters: A Randomized Controlled Trial
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
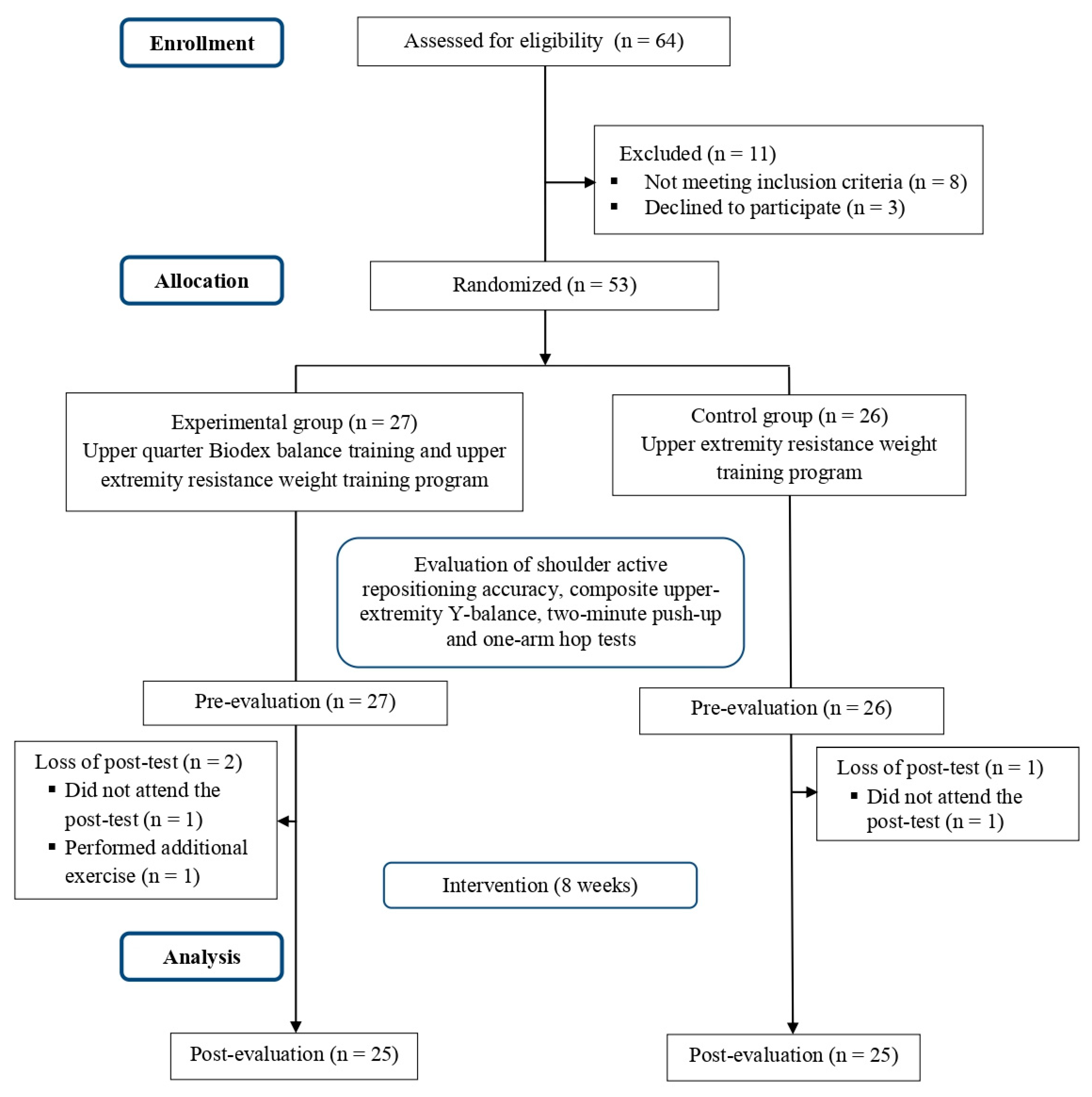
2.1. Participants
2.2. Testing Procedures
2.3. Upper-Quarter Y-Balance Test
2.4. Shoulder Active Repositioning Accuracy Using Isokinetic Dynamometer
2.5. Two-Minute (2 Min) 90° Push-Up Test
2.6. One-Arm Hop Test
2.7. Training Procedure
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wasiluk, A.; Saczuk, J. Changes in the somatic build and physical fitness of physical education students in the years 2004 and 2014. Trends Sport Sci. 2020, 27, 29–34. [Google Scholar] [CrossRef]
- Alves, A.R.; Marinho, D.A.; Pecêgo, M.; Ferraz, R.; Marques, M.C.; Neiva, H.P. Strength training combined with high-intensity interval aerobic training in young adults’ body composition. Trends Sport Sci. 2021, 28, 187–193. [Google Scholar] [CrossRef]
- Keogh, J.W.L.; Winwood, P.W. The epidemiology of injuries across the weight-training sports. Sport. Med. 2017, 47, 479–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grenier, S.G.; McGill, S.M. Quantification of lumbar stability by using 2 different abdominal activation strategies. Arch. Phys. Med. Rehabil. 2007, 88, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Harman, E.A.; Frykman, P.N.; Clagett, E.R.; Kraemer, W.J. Intra-abdominal and intra-thoracic pressures during lifting and jumping. Med. Sci. Sports Exerc. 1988, 20, 195–201. [Google Scholar] [CrossRef]
- Kerr, Z.Y.; Collins, C.L.; Comstock, R.D. Epidemiology of Weight Training-Related Injuries Presenting to United States Emergency Departments, 1990 to 2007. Am. J. Sports Med. 2010, 38, 765–771. [Google Scholar] [CrossRef]
- Abdelraouf, O.R.; Abdel-Aziem, A.A. The relationship between core endurance and back dysfunction in collegiate male athletes with and without nonspecific low back pain. Int. J. Sports Phys. Ther. 2016, 11, 337–344. [Google Scholar]
- Golshani, K.; Cinque, M.E.; O’Halloran, P.; Softness, K.; Keeling, L.; Macdonell, J.R. Upper extremity weightlifting injuries: Diagnosis and management. J. Orthop. 2018, 15, 24–27. [Google Scholar] [CrossRef]
- Ellenbecker, T.S.; Manske, R.; Davies, G.J. Closed kinetic chain testing techniques of the upper extremities. Orthop. Phys. Ther. Clin. N. Am. 2000, 9, 219–229. [Google Scholar]
- Mayer, F.; Schlumberger, A.; Van Cingel, R.; Henrotin, Y.; Laube, W.; Schmidtbleicher, D. Training and testing in open versus closed kinetic chain. Isokinet. Exerc. Sci. 2003, 11, 181–187. [Google Scholar] [CrossRef]
- Tucci, H.T.; Martins, J.S.G.C. Closed Kinetic Chain Upper Extremity Stability test (CKCUES test): A reliability study in persons with and without shoulder impingement syndrome. BMC Musculoskelet. Disord. 2014, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, R.J.B.; Pirauá, A.L.T.; Nascimento, V.Y.S.; dos Santos, P.S.; Beltrão, N.B.; de Oliveira, V.M.A.; Pitangui, A.C.R.; de Araújo, R.C. Shoulder muscle activation levels during the push-up-plus exercise on stable and unstable surfaces. J. Sport Rehabil. 2017, 26, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Phan, K. Functional testing in human performance. Athl. Train. Sport. Health Care 2010, 5, 244–250. [Google Scholar] [CrossRef]
- Westrick, R.B.; Miller, J.M.; Carow, S.D.; Gerber, J.P. Exploration of the y-balance test for assessment of upper quarter closed kinetic chain performance. Int. J. Sports Phys. Ther. 2012, 7, 139–147. [Google Scholar] [PubMed]
- Ruffe, N.J.; Sorce, S.R.; Rosenthal, M.D.; Rauh, M.J. Lower quarter- and upper quarter Y balance tests as predictors of running-related injuries in high school cross-country runners. Int. J. Sports Phys. Ther. 2019, 14, 695–706. [Google Scholar] [CrossRef] [PubMed]
- Gorman, P.P.; Butler, R.J.; Plisky, P.J.; Kiesel, K.B. Upper quarter y balance test: Reliability and performance comparison between genders in active adults. J. Strength Cond. Res. 2012, 26, 3043–3048. [Google Scholar] [CrossRef]
- Falsone, S.A.; Gross, M.T.; Guskiewicz, K.M.; Schneider, R.A. One-arm hop test: Reliability and effects of arm dominance. J. Orthop. Sports Phys. Ther. 2002, 32, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Seo, S.H.; Jeon, I.H.; Cho, Y.H.; Lee, H.G.; Hwang, Y.T.; Jang, J.H. Surface EMG during the push-up plus exercise on a stable support or Swiss ball: Scapular stabilizer muscle exercise. J. Phys. Ther. Sci. 2013, 25, 833–837. [Google Scholar] [CrossRef] [Green Version]
- ACSM. ACSM’s Health-Related Physical Fitness Assessment Manual; ACSM: Michigan, IN, USA, 2008. [Google Scholar]
- Zech, A.; Hübscher, M.; Vogt, L.; Banzer, W.; Hänsel, F.; Pfeifer, K. Balance training for neuromuscular control and performance enhancement: A systematic review. J. Athl. Train. 2010, 45, 392–403. [Google Scholar] [CrossRef] [Green Version]
- Behm, D.; Colado, J.C. The effectiveness of resistance training using unstable surfaces and devices for rehabilitation. Int. J. Sports Phys. Ther. 2012, 7, 226–241. [Google Scholar]
- Dawson, N.; Dzurino, D.; Karleskint, M.; Tucker, J. Examining the reliability, correlation, and validity of commonly used assessment tools to measure balance. Health Sci. Reports 2018, 1, e98. [Google Scholar] [CrossRef] [PubMed]
- Eftekharsadat, B.; Babaei-Ghazani, A.; Mohammadzadeh, M.; Talebi, M.; Eslamian, F.; Azari, E. Effect of virtual reality-based balance training in multiple sclerosis. Neurol Res. 2015, 37, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Ramos, G.S.; Silva-Batista, C.; Palma, B.P.; Ugrinowitsch, C.; da Cunha, T.F. Risk of falls using the Biodex Balance System in non-faller patients with Parkinson Disease. Somat. Mot. Res. 2021, 21, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Parsa, M.; Rahimi, A.; Dehkordi, S.N. Studying the correlation between balance assessment by Biodex Stability System and Berg Scale in stroke individuals. J. Bodyw. Mov. Ther. 2019, 4, 850–854. [Google Scholar] [CrossRef] [PubMed]
- Sah, D.; Mu, R.; Arsh, A.; Junaid, M. Effect of balance training with Biodex Balance System to improve balance in patients with diabetic neuropathy: A quasi experimental study. Pak. J. Med. Sci. 2021, 37, 389–392. [Google Scholar] [CrossRef]
- Siddiqi, F.A.; Masood, T. Training on Biodex balance system improves balance and mobility in the elderly. J. Pak. Med. Assoc. 2018, 68, 1655–1659. [Google Scholar] [PubMed]
- Jagim, A.R.; Dominy, T.A.; Camic, C.L.; Wright, G.; Doberstein, S.; Jones, M.T.; Oliver, J.M. Acute effects of the elevation training mask on strength performance in recreational weight lifters. J. Strength Cond. Res. 2018, 32, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J.; Plisky, P. Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. J. Athl. Train. 2012, 47, 339–357. [Google Scholar] [CrossRef] [Green Version]
- Ager, A.; Roy, J.; Roos, M.; Belley, A.; Cools, A.; Hébert, L. Shoulder proprioception: How is it measured and is it reliable? A systematic review. J. Hand Ther. 2017, 30, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Anwar, E.A.; Karkousha, R.N.; Amen, F.S. Effect of forward head posture on shoulder proprioception in young adults. Int. J. Ther. Rehabil. Res. 2017, 6, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Safran, M.; Borsa, P.; Lephart, S.; Fu, F.; Warner, J. Shoulder proprioception in baseball pitchers. J. Shoulder Elb. Surg 2001, 10, 438–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fielitz, L.; Coelho, J.; Horne, T.; Brechue, W. Inter-rater reliability and intra-rater reliability of assessing the 2-minute push-up test. Mil. Med. 2016, 181, 167–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G.A.V. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.C.; Jones, P.W. Long-term reproducibility of Borg scale estimates of breathlessness during exercise. Clin. Sci. 1991, 80, 309–312. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.S.; Mattar, A.G.; Elhafez, S.M. Efficacy of virtual reality-based balance training versus the biodex balance system training on the body balance of adults. J. Phys. Ther. Sci. 2016, 26, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eftekhar-Sadat, B.; Azizi, R.; Aliasgharzadeh, A.; Toopchizadeh, V.; Ghojazadeh, M. Effect of balance training with biodex stability system on balance in diabetic neuropathy. Ther. Adv. Endocrinol. Metab. 2015, 6, 233–240. [Google Scholar] [CrossRef] [Green Version]
- Kibele, A.; Behm, D.G. Seven weeks of instability and traditional resistance training effects on strength, balance and functional performance. J. Strength Cond. Res. 2009, 23, 2443–2450. [Google Scholar] [CrossRef] [PubMed]
- Behm, D.G.; Drinkwater, E.J.; Willardson, J.M.; Cowley, P.M. Canadian society for exercise physiology position stand: The use of instability to train the core in athletic and nonathletic conditioning. Appl. Physiol. Nutr. Metab. 2010, 35, 109–112. [Google Scholar] [CrossRef] [Green Version]
- Behm, D.G.; Muehlbauer, T.; Kibele, A.; Granacher, U. Effects of strength training using unstable surfaces on strength, power and balance performance across the lifespan: A systematic review and meta-analysis. Sport. Med. 2015, 45, 1645–1669. [Google Scholar] [CrossRef] [Green Version]
- Anderson, K.; Behm, D.G. Trunk muscle activity increases with unstable squat movements. Can. J. Appl. Physiol. 2005, 30, 33–45. [Google Scholar] [CrossRef] [Green Version]
- Sparkes, R.; Behm, D.G. Training adaptations associated with an 8-week instability resistance training program with recreationally active individuals. J. Strength Cond. Res. 2010, 24, 1931–1941. [Google Scholar] [CrossRef] [PubMed]
- Maté-Muñoz, J.L.; Antón, A.J.M.; Jiménez, P.J.; Garnacho-Castaño, M.V. Effects of instability versus traditional resistance training on strength, power and velocity in untrained men. J. Sport. Sci. Med. 2014, 13, 460–468. [Google Scholar]
- Willardson, J.M. The effectiveness of resistance exercises performed on unstable equipment. Strength Cond. J. 2004, 26, 5. [Google Scholar] [CrossRef]
- van Vliet, P.; Wulf, G. Extrinsic feedback for motor learning after stroke: What is the evidence? Disabil. Rehabil. 2006, 28, 831–840. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Gao, F.; Chen, H.; Al, E. Correlation analysis of factors affecting human Gait balance. Control Eng. 2017, 24, 140–141. [Google Scholar]
- Zhao, W.; You, H.; Jiang, S.; Zhang, H.; Yang, Y.; Zhang, M. Effect of Pro-kin visual feedback balance training system on gait stability in patients with cerebral small vessel disease. Medicine 2019, 98, e14503. [Google Scholar] [CrossRef]
- Cug, M.; Wikstrom, E.A. Learning effects associated with the least stable level of the Biodex® stability system during dual and single limb stance. J. Sport. Sci. Med. 2014, 13, 387–392. [Google Scholar]
- Padnjarethil, H. Sport specific movements on the biodex balance system as a measure of dynamic balance. J. Sport. Med. Doping Stud. 2018, 52, 08–09. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Group Mean ± SD | Control Group Mean ± SD | p Value | |
|---|---|---|---|
| Age, year | 22.24 ± 2.15 | 22.80 ± 2.25 | 0.373 |
| Height, cm | 174.56 ± 4.54 | 172.92 ± 4.37 | 0.234 |
| Weight, kg | 79.32 ± 8.10 | 77.36 ± 7.49 | 0.379 |
| BMI, kg/m2 | 26.06 ± 2.00 | 25.82 ± 1.59 | 0.635 |
| Upper-extremity length, cm | 72.12 ± 4.59 | 71.36 ± 3.56 | 0.516 |
| Experimental Group Mean ± SD | Control Group Mean ± SD | p Value | ||
|---|---|---|---|---|
| Shoulder active repositioning accuracy test (degree) | pre | 5.23 ± 2.52 | 5.98 ± 2.83 | 0.333 |
| post | 3.21 ± 1.97 | 4.06 ± 2.04 | 0.019 * | |
| p value | 0.001 * | 0.001 * | ||
| Composite right upper-extremity Y-balance test score (cm) | pre | 82.47 ± 10.68 | 79.24 ± 9.47 | 0.302 |
| post | 91.57 ± 10.20 | 84.92 ± 10.20 | 0.025 * | |
| p value | 0.001 * | 0.001 * | ||
| Composite left upper-extremity Y-balance test score (cm) | pre | 80.46 ± 9.97 | 77.52 ± 7.57 | 0.201 |
| post | 90.90 ± 10.47 | 83.27 ± 6.57 | 0.003 * | |
| p value | 0.001 * | 0.001 * | ||
| Two-minute push-up test (no. of repetitions) | pre | 53.96 ± 4.49 | 55.52 ± 4.87 | 0.245 |
| post | 67.24 ± 5.75 | 70.16 ± 5.68 | 0.077 | |
| p value | 0.001 * | 0.001 * | ||
| Right one-arm hop test (seconds) | pre | 6.78 ± 1.25 | 6.60 ± 1.38 | 0.632 |
| post | 4.26 ± 1.18 | 5.36 ± 1.22 | 0.002 | |
| p value | 0.001 * | 0.001 * | ||
| Left one-arm hop test (seconds) | pre | 6.18 ± 1.07 | 6.10 ± 1.35 | 0.818 |
| post | 4.08 ± 1.07 | 5.02 ± 1.26 | 0.007 | |
| p value | 0.001 * | 0.001 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdelraouf, O.R.; Abdel-aziem, A.A.; Ghally, S.A.; Osama, L.A.; Dawood, R.S.; Yehia, A.M.; Eed, E.M.; EI-Gendy, A.M.; Radwan, R.E. Innovative Use of Biodex Balance System to Improve Dynamic Stabilization and Function of Upper Quarter in Recreational Weightlifters: A Randomized Controlled Trial. Medicina 2022, 58, 1631. https://doi.org/10.3390/medicina58111631
Abdelraouf OR, Abdel-aziem AA, Ghally SA, Osama LA, Dawood RS, Yehia AM, Eed EM, EI-Gendy AM, Radwan RE. Innovative Use of Biodex Balance System to Improve Dynamic Stabilization and Function of Upper Quarter in Recreational Weightlifters: A Randomized Controlled Trial. Medicina. 2022; 58(11):1631. https://doi.org/10.3390/medicina58111631
Chicago/Turabian StyleAbdelraouf, Osama R., Amr A. Abdel-aziem, Shahesta A. Ghally, Lamis A. Osama, Reem S. Dawood, Amr M. Yehia, Emad M. Eed, Amira M. EI-Gendy, and Rafik E. Radwan. 2022. "Innovative Use of Biodex Balance System to Improve Dynamic Stabilization and Function of Upper Quarter in Recreational Weightlifters: A Randomized Controlled Trial" Medicina 58, no. 11: 1631. https://doi.org/10.3390/medicina58111631