
Effects of a Novel Proprioceptive Rehabilitation Device on Shoulder Joint Position Sense, Pain and Function
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Rehabilitation Programs
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
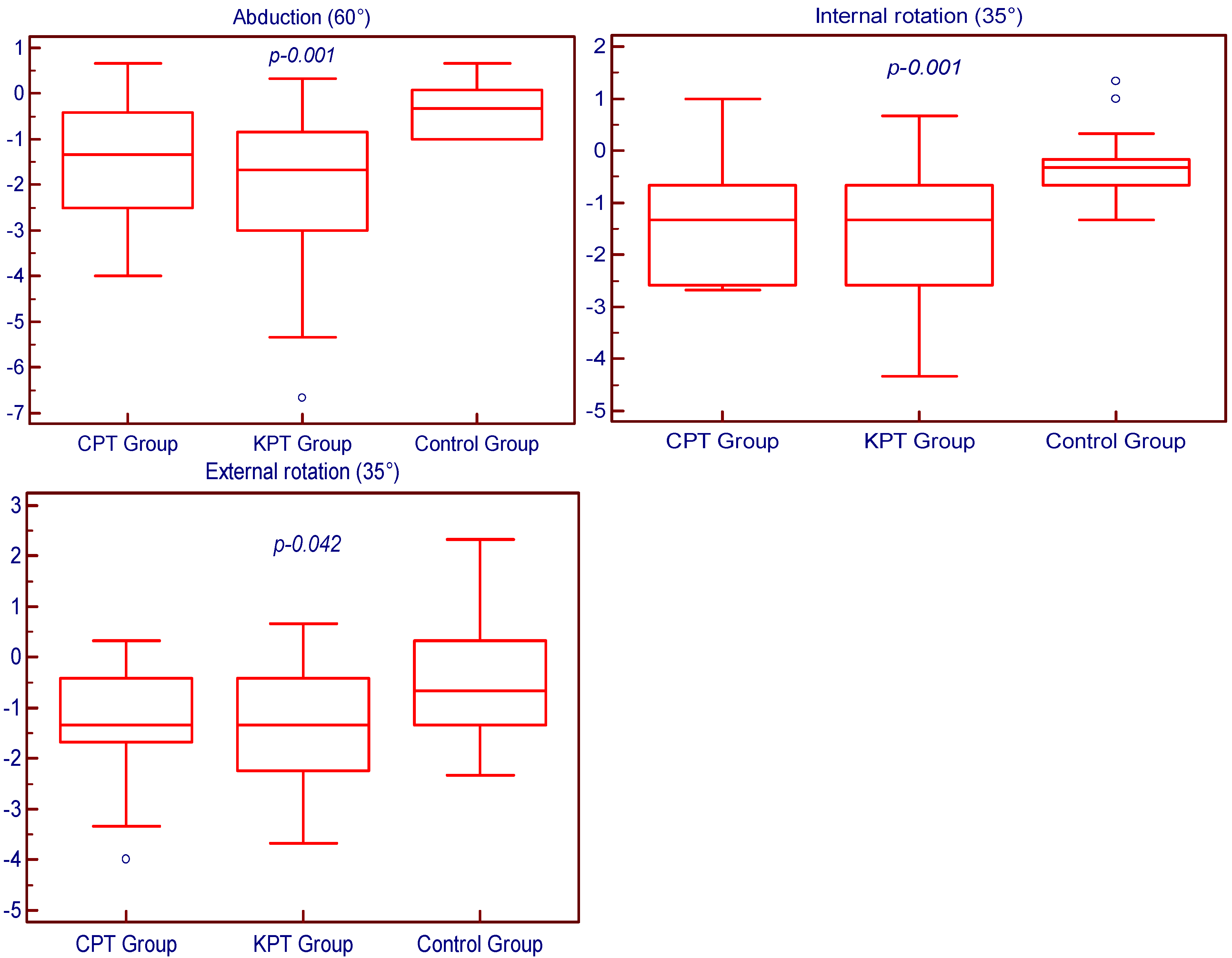
3.1. Joint Position Sense
3.2. DASH Outcome Questionnaire
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, Y.F.; Lin, D.H.; Jan, M.H.; Lin, C.H.J.; Cheng, C.K. Orthopedic Physical Therapy. In Comprehensive Biomedical Physics; Brahme, A., Ed.; Elsevier: Amsterdam, The Netherlands, 2014; Volume 10, pp. 379–400. [Google Scholar]
- Mendez-Rebolledo, G.; Ager, A.L.; Ledezma, D.; Montanez, J.; Guerrero-Henriquez, J.; Cruz-Montecinos, C. Role of active joint position sense on the upper extremity functional performance tests in college volleyball players. PeerJ 2022, 10, e13564. [Google Scholar] [CrossRef] [PubMed]
- Prescott, S.A.; Ratte, S. Somatosensation and Pain. In Conn’s Translational Neuroscience; Conn, P.M., Ed.; Academic Press: Amsterdam, The Netherlands, 2016; pp. 517–539. [Google Scholar]
- Miall, R.C.; Kitchen, N.M.; Nam, S.H.; Lefumat, H.; Renault, A.G.; Ørstavik, K.; Cole, J.D.; Sarlegna, F.R. Proprioceptive loss and the perception, control and learning of arm movements in humans: Evidence from sensory neuronopathy. Exp. Brain Res. 2018, 236, 2137–2155. [Google Scholar] [CrossRef] [PubMed]
- Kelso, J.A.S.; Holt, K.G.; Flatt, A.E. The role of proprioception in the perception and control of human movement: Toward a theoretical reassessment. Percept. Psychophys. 1980, 28, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Ji, Z.; Jiang, G.; Liu, W.; Jiao, X. Correlation among proprioception, muscle strength, and balance. J. Phys. Ther. Sci. 2016, 28, 3468–3472. [Google Scholar] [CrossRef]
- Marzetti, E.; Rabini, A.; Piccinini, G.; Piazzini, D.B.; Vulpiani, M.C.; Vetrano, M.; Specchia, A.; Ferriero, G.; Bertolini, C.; Saraceni, V.M. Neurocognitive therapeutic exercise improves pain and function in patients with shoulder impingement syndrome: A single-blind randomized controlled clinical trial. Eur. J. Phys. Rehabil. Med. 2014, 50, 255–264. [Google Scholar]
- Paolucci, T.; Zangrando, F.; Piccinini, G.; Sciarra, F.; Pallotta, R.; Mannocci, A.; la Torre, G.; Bini, F.; Marinozzi, F.; Gumina, S.; et al. A new neurocognitive interpretation of shoulder position sense during reaching: Unexpected competence in the measurement of extracorporeal space. BioMed Res. Int. 2016, 2016, 9065495. [Google Scholar] [CrossRef]
- Fyrh, C.; Gustavsson, L.; Wassinger, C.; Sole, G. The effect of shoulder injury on kinesthesia: A systematic review and meta-analysis. Man. Ther. 2015, 20, 28–37. [Google Scholar] [CrossRef]
- Matsui, K.; Tachibana, T.; Nobuhara, K.; Uchiyama, Y. Translational movement within the glenohumeral joint at different rotation velocities as seen by cine MRI. J. Exp. Orthop. 2018, 5, 7. [Google Scholar] [CrossRef]
- Ettinger, L.R.; Shapiro, M.; Karduna, A. Subacromial Anesthetics Increase Proprioceptive Deficit in the Shoulder and Elbow in Patients with Subacromial Impingement Syndrome. Clin. Med. Insights Arthritis Musculoskelet. Disord. 2017, 10, 1179544117713196. [Google Scholar] [CrossRef]
- Abechain, J.J.K.; Godinho, G.G.; Matsunaga, F.T.; Netto, N.A.; Daou, J.P.; Tamaoki, M.J.S. Functional outcomes of traumatic and non-traumatic rotator cuff tears after arthroscopic repair. World J. Orthop. 2017, 8, 631–637. [Google Scholar] [CrossRef]
- Oliva, F.; Piccirilli, E.; Bossa, M.; Via, A.G.; Colombo, A.; Chillemi, C.; Gasparre, G.; Pellicciari, L.; Franceschetti, E.; Rugiero, C.; et al. I.S.Mu.L.T—Rotator Cuff Tears Guidelines. Muscle Ligaments Tendons J. 2016, 5, 227–263. [Google Scholar] [CrossRef]
- Luke, A.; Ma, C.B. Sports Medicine & Outpatient Orthopedics. In Current Medical Diagnosis & Treatment; Papadakis, M.A., McPhee, S.J., Rabow, M.W., Eds.; McGraw-Hill Medical: New York, NY, USA, 2016; pp. 1664–1671. [Google Scholar]
- Bhattacharyya, R.; Edwards, K.; Wallace, A.W. Does arthroscopic sub-acromial decompression really work for sub-acromial impingement syndrome: A cohort study. BMC Musculoskelet. Disord. 2014, 15, 324. [Google Scholar] [CrossRef] [PubMed]
- Michener, L.A.; Walsworth, M.K.; Doukas, W.C.; Murphy, K.P. Reliability and diagnostic accuracy of 5 physical examination tests and combination of tests for subacromial impingement. Arch. Phys. Med. Rehabil. 2009, 90, 1898–1903. [Google Scholar] [CrossRef] [PubMed]
- Garving, C.; Jakob, S.; Bauer, I.; Nadjar, R.; Brunner, U.H. Impingement Syndrome of the Shoulder. Dtsch. Arztebl. Int. 2017, 114, 765–776. [Google Scholar] [CrossRef] [PubMed]
- Gunay Ucurum, S.; Kaya, D.O.; Kayali, Y.; Askin, A.; Tekindal, M.A. Comparison of different electrotherapy methods and exercise therapy in shoulder impingement syndrome: A prospective randomized controlled trial. Acta Orthop. Traumatol. Turc. 2018, 52, 249–255. [Google Scholar] [CrossRef]
- Novi, M.; Kumar, A.; Paladini, P.; Porcellini, G.; Merolla, G. Irreparable rotator cuff tears: Challenges and solutions. Orthop. Res. Rev. 2018, 10, 93–103. [Google Scholar] [CrossRef]
- Buckup, J.; Welsch, F.; Gramlich, Y.; Hoffmann, R.; Roessler, P.P.; Schüttler, K.F.; Stein, T. Back to Sports After Arthroscopic Revision Bankart Repair. Orthop. J. Sports Med. 2018, 6, 2325967118755452. [Google Scholar] [CrossRef]
- Kang, J.I.; Moon, Y.J.; Choi, H.; Jeong, D.K.; Kwon, H.M.; Park, J.S. The effect of exercise types for rotator cuff repair patients on activities of shoulder muscles and upper limb disability. J. Phys. Ther. Sci. 2016, 28, 2772–2777. [Google Scholar] [CrossRef]
- Moradi, M.; Hadadnezhad, M.; Letafatkar, A.; Khosrokiani, Z.; Baker, J.S. Efficacy of throwing exercise with TheraBand in male volleyball players with shoulder internal rotation deficit: A randomized controlled trial. BMC Musculoskelet. Disord. 2020, 21, 376. [Google Scholar] [CrossRef]
- Hanratty, C.E.; McVeigh, J.G.; Kerr, D.P.; Basford, J.R.; Finch, M.B.; Pendleton, A.; Sim, J. The effectiveness of physiotherapy exercises in subacromial impingement syndrome: A systematic review and meta-analysis. Semin. Arthritis. Rheum. 2012, 42, 297–316. [Google Scholar] [CrossRef]
- Sciascia, A.; Cromwell, R. Kinetic chain rehabilitation: A theoretical framework. Rehabil. Res. Pract. 2012, 2012, 853037. [Google Scholar] [CrossRef] [PubMed]
- Gliga, A.-C.; Neagu, N. Recuperarea Fizică și Reabilitarea Funcțională în Traumatologia Sportivă. Vademecum fizioterapeutic [Physical Recovery and Functional Rehabilitation in Sports Traumatology. A Physiotherapeutic Vademecum]; Discobolul Publishing House: Bucharest, Romania, 2021; Volume 2, pp. 23–30. [Google Scholar]
- Lombardi, I., Jr.; Magri, A.G.; Fleury, A.M.; Da Silva, A.C.; Natour, J. Progressive resistance training in patients with shoulder impingement syndrome: A randomized controlled trial. Arthritis. Rheum. 2008, 59, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Duzgun, I.; Turhan, E. Proprioception After Shoulder Injury, Surgery, and Rehabilitation. In Proprioception in Orthopaedics, Sports Medicine and Rehabilitation; Kaya, D., Yosmaoglu, B., Doral, M.N., Eds.; Springer: New York, NY, USA, 2018; pp. 35–45. [Google Scholar]
- Laut, J.; Porfiri, M.; Raghavan, P. The present and future of robotic technology in rehabilitation. Curr. Phys. Med. Rehabil. Rep. 2016, 4, 312–319. [Google Scholar] [CrossRef]
- Daunoraviciene, K.; Adomaviciene, A.; Grigonyte, A.; Griškevičius, J.; Juocevicius, A. Effects of robot-assisted training on upper limb functional recovery during the rehabilitation of poststroke patients. Technol. Health Care 2018, 26, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Dockx, K.; Bekkers, E.M.; Van den Bergh, V.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 12, CD010760. [Google Scholar] [CrossRef] [PubMed]
- Shoulder Plyometric Program. Available online: https://www.bostonsportsmedicine.com/rehabilitation-protocols/shoulder-plyometric-program/ (accessed on 3 March 2022).
- Gliga, A.-C.; Neagu, N.; Szabo, D.-A. Optimising the Validity of Shoulder Range of Motion Evaluation: A Comparative Study. Broad Res. Artif. Intell. Neurosci. 2020, 11, 101–112. [Google Scholar] [CrossRef]
- Gliga, A.-C.; Neagu, N.; Popoviciu, H.V.; Bățagă, T. Effects of adding aquatic-to-land-based physiotherapy programs for shoulder joint position sense rehabilitation. Healthcare 2022, 10, 332. [Google Scholar] [CrossRef]
- Springer, S.; Kelman, D.; Brand, M.; Gottlieb, U. Knee position sense: Does the time interval at the target angle affect position accuracy? J. Phys. Ther. Sci. 2017, 29, 1760–1765. [Google Scholar] [CrossRef]
- Lee, D.; Han, S. Validation of Joint Position Sense of Dorsi-Plantar Flexion of Ankle Measurements Using a Smartphone. Healthc. Inform. Res. 2017, 23, 183–188. [Google Scholar] [CrossRef]
- Darwish, M.H.; Ahmed, S.; Abdelalim, A.; Elsherif, A.A. Quantitative evaluation of shoulder proprioception 6 months following stroke. Egypt J. Neurol. Psychiatr. Neurosurg. 2018, 54, 31. [Google Scholar] [CrossRef]
- Hwang, M.; Lee, S.; Lim, C. Effects of the Proprioceptive Neuromuscular Facilitation Technique on Scapula Function in Office Workers with Scapula Dyskinesis. Medicina 2021, 57, 332. [Google Scholar] [CrossRef] [PubMed]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal clinically important difference of the disabilities of the arm, shoulder and hand outcome measure (DASH) and its shortened version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Li-Tsang, C.W.; Au, R.K. Robotic approaches for the rehabilitation of upper limb recovery after stroke: A systematic review and meta-analysis. Int. J. Rehabil. Res. 2017, 40, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef]
- Reis, S.B.; Bernardo, W.M.; Oshiro, C.A.; Krebs, H.I.; Conforto, A.B. Effects of Robotic Therapy Associated with Noninvasive Brain Stimulation on Upper-Limb Rehabilitation after Stroke: Systematic Review and Meta-analysis of Randomized Clinical Trials. Neurorehabil. Neural. Repair 2021, 35, 256–266. [Google Scholar] [CrossRef]
- Mazzoleni, S.; Duret, C.; Grosmaire, A.G.; Battini, E. Combining Upper Limb Robotic Rehabilitation with Other Therapeutic Approaches after Stroke: Current Status, Rationale, and Challenges. BioMed Res. Int. 2017, 2017, 8905637. [Google Scholar] [CrossRef]
- Kenzie, J.M.; Semrau, J.A.; Hill, M.D.; Scott, S.H.; Dukelow, S.P. A composite robotic-based measure of upper limb proprioception. J. Neuroeng. Rehabil. 2017, 14, 114. [Google Scholar] [CrossRef]
- Takasaki, H.; Okubo, Y.; Okuyama, S. The Effect of Proprioceptive Neuromuscular Facilitation on Joint Position Sense: A Systematic Review. J. Sport Rehabil. 2019, 29, 488–497. [Google Scholar] [CrossRef]
- Kline, A.E.; Leary, J.B.; Radabaugh, H.L.; Cheng, J.P.; Bondi, C.O. Combination therapies for neurobehavioral and cognitive recovery after experimental traumatic brain injury: Is more better? Prog. Neurobiol. 2016, 142, 45–67. [Google Scholar] [CrossRef]
- Reinkensmeyer, D.J.; Boninger, M.L. Technologies and combination therapies for enhancing movement training for people with a disability. J. Neuroeng. Rehabil. 2012, 9, 17. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants Characteristics | CPT Group Mean ± SD | KPT Group Mean ± SD | Control Group Mean ± SD | p Value |
|---|---|---|---|---|
| Age (years) | 56.32 ± 6.38 | 57.11 ± 6.94 | 55.41 ± 7.22 | 0.761 |
| Height (cm) | 171.32 ± 8.37 | 172.79 ± 7.26 | 169.24 ± 7.89 | 0.404 |
| Weight (kg) | 73.89 ± 14.70 | 75.68 ± 11.75 | 77.12 ± 11.02 | 0.746 |
| BMI (kg/m2) | 25.04 ± 3.47 | 25.27 ± 2.84 | 26.93 ± 3.47 | 0.181 |
| Participants Characteristics | CPT Group | KPT Group | Control Group | |||
|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |
| Sex (female/male) | 9/10 | 47.37/52.63 | 11/8 | 57.89/42.11 | 8/9 | 47.06/52.94 |
| Hand dominance (left/right) | 2/17 | 10.53/89.47 | 1/18 | 5.26/94.74 | 2/15 | 11.76/88.24 |
| SLAP tear | 4 | 21.05 | 5 | 26.32 | 3 | 17.65 |
| SIS | 9 | 47.37 | 6 | 31.58 | 7 | 41.18 |
| RC tear | 6 | 31.58 | 8 | 42.11 | 7 | 41.18 |
| CPT Group Mean ± SD | KPT Group Mean ± SD | Control Group Mean ± SD | ||
|---|---|---|---|---|
| Flexion (60°) | Initial assessment results | 5.93 ± 3.19 | 6.09 ± 3.73 | 5.53 ± 2.54 |
| Final assessment results | 4.51 ± 2.60 | 4.30 ± 3.21 | 5.06 ± 2.40 | |
| p Value | <0.001 | <0.001 | 0.047 | |
| Extension (25°) | Initial assessment results | 6.46 ± 3.30 | 6.79 ± 3.63 | 6.55 ± 3.36 |
| Final assessment results | 5.14 ± 2.45 | 5.21 ± 2.37 | 6.37 ± 3.00 | |
| p Value | <0.001 | <0.001 | 0.275 | |
| Abduction (60°) | Initial assessment results | 6.04 ± 3.34 | 6.35 ± 3.88 | 6.12 ± 3.10 |
| Final assessment results | 4.51 ± 2.31 | 4.12 ± 2.59 | 5.77 ± 2.95 | |
| p Value | <0.001 | <0.001 | 0.027 | |
| Internal rotation (35°) | Initial assessment results | 6.60 ± 3.58 | 6.98 ± 3.91 | 6.41 ± 2.77 |
| Final assessment results | 5.19 ± 3.08 | 5.33 ± 3.42 | 6.14 ± 2.99 | |
| p Value | <0.001 | <0.001 | 0.122 | |
| External rotation (35°) | Initial assessment results | 6.88 ± 3.32 | 6.81 ± 3.46 | 6.67 ± 3.20 |
| Final assessment results | 5.67 ± 2.50 | 5.44 ± 2.74 | 6.28 ± 2.92 | |
| p Value | <0.001 | <0.001 | 0.203 | |
| CPT Group Mean ± SD | KPT Group Mean ± SD | Control Group Mean ± SD | ||
|---|---|---|---|---|
| Pain and performing ability score | Initial assessment results | 29.52 ± 10.87 | 30.93 ± 7.62 | 27.15 ± 6.25 |
| Final assessment results | 21.60 ± 9.53 | 19.99 ± 7.82 | 24.94 ± 7.70 | |
| p Value | <0.001 | <0.001 | 0.014 | |
| Work ability score | Initial assessment results | 41.45 ± 16.03 | 45.07 ± 10.74 | 42.66 ± 19.69 |
| Final assessment results | 30.59 ± 17.90 | 29.28 ± 15.87 | 38.60 ± 19.04 | |
| p Value | <0.001 | <0.001 | 0.002 | |
| Sports and activities score | Initial assessment results | 47.04 ± 14.18 | 49.34 ± 10.60 | 50.00 ± 14.32 |
| Final assessment results | 34.87 ± 15.21 | 34.87 ± 14.78 | 44.12 ± 13.71 | |
| p Value | <0.001 | <0.001 | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gliga, A.C.; Neagu, N.E.; Voidazan, S.; Popoviciu, H.V.; Bataga, T. Effects of a Novel Proprioceptive Rehabilitation Device on Shoulder Joint Position Sense, Pain and Function. Medicina 2022, 58, 1248. https://doi.org/10.3390/medicina58091248
Gliga AC, Neagu NE, Voidazan S, Popoviciu HV, Bataga T. Effects of a Novel Proprioceptive Rehabilitation Device on Shoulder Joint Position Sense, Pain and Function. Medicina. 2022; 58(9):1248. https://doi.org/10.3390/medicina58091248
Chicago/Turabian StyleGliga, Alexandra Camelia, Nicolae Emilian Neagu, Septimiu Voidazan, Horatiu Valeriu Popoviciu, and Tiberiu Bataga. 2022. "Effects of a Novel Proprioceptive Rehabilitation Device on Shoulder Joint Position Sense, Pain and Function" Medicina 58, no. 9: 1248. https://doi.org/10.3390/medicina58091248