
A Fatal Case of Chlorfenapyr Poisoning and the Therapeutic Implications of Serum Chlorfenapyr and Tralopyril Levels
 , ,
, ,  and
and
Abstract
:1. Introduction
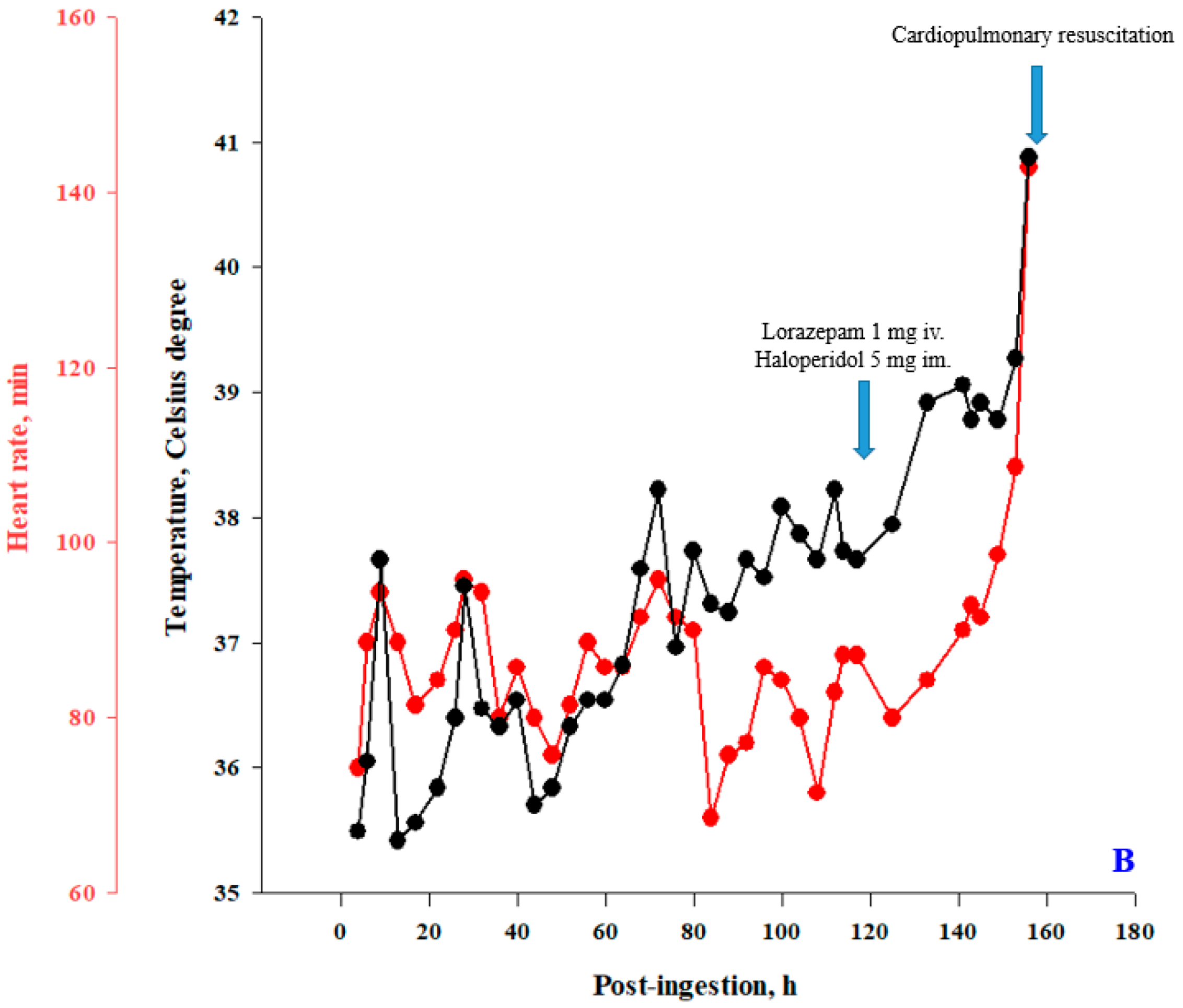
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chlorfenapyr. Pesticide Fact Sheet. Available online: https://www.epa.gov/pesticide-registration (accessed on 30 September 2022).
- Black, B.; Hollingworth, R.; Ahammadsahib, K.; Kukel, C.; Donovan, S. Insecticidal Action and Mitochondrial Uncoupling Activity of AC-303,630 and Related Halogenated Pyrroles. Pestic. Biochem. Physiol. 1994, 50, 115–128. [Google Scholar] [CrossRef]
- Hunt, D.A.; Treacy, M.F. Pyrrole insecticides: A new class of agriculturally important insecticides functioning as uncouplers of oxidative phosphorylation. In Insecticides with Novel Modes of Action: Merchanism and Application; Ishaaya, I., Degheele, D., Eds.; Springer: New York, NY, USA, 1998. [Google Scholar]
- Hollingworth, R.M.; Gadelhak, G.G. Mechanisms of action and toxicity of new pesticides that disrupt oxidative phosphorylation. Rev. Toxicol. 1998, 2, 253–266. [Google Scholar]
- Endo, Y.; Tachibana, S.; Hirano, J.; Kuroki, Y.; Ohashi, N.; Yoshioka, T.; Sugimoto, T. Acute chlorfenapyr poisoning. Chudoku Kenkyu Chudoku Kenkyukai Jun Kikanshi Jpn. J. Toxicol. 2004, 17, 89–93. [Google Scholar]
- Chien, S.-C.; Su, Y.-J. A fatal case of chlorfenapyr poisoning and a review of the literature. J. Int. Med. Res. 2022, 50, 03000605221121965. [Google Scholar] [CrossRef]
- Metruccio, F.; Boobis, A. Chlorfenapyr-JMPR 2012 Monograph Final. 2012. Available online: http://apps.who.int/pesticide-residues-jmpr-database/pesticide?name=CHLORFENAPYR (accessed on 30 September 2022).
- Lunn, D.; MacLachlan, D.; Shan, W. Pesticide Residues in Food 2012. Joint FAO/WHO Meeting on Pesticide Residues. 2012. Available online: https://wwwfaoorg/agriculture/crops/thematic-sitemap/theme/pests/jmpr/jmpr-rep/en/ (accessed on 30 June 2022).
- Periasamy, S.; Deng, J.-F.; Liu, M.-Y. Who is the real killer? Chlorfenapyr or detergent micelle-chlorfenapyr complex? Xenobiotica 2017, 47, 833–835. [Google Scholar] [CrossRef]
- Choi, J.T.; Kang, G.H.; Jang, Y.S.; Ahn, H.C.; Seo, J.Y.; Sohn, Y.D. Fatality from acute chlorfenapyr poisoning. Clin. Toxicol. 2010, 48, 458–459. [Google Scholar] [CrossRef]
- Kwon, J.S.; Kim, H.Y.; Han, H.J.; Kim, J.Y.; Park, J.H. A case of chlorfenapyr intoxication with central nervous system involvement. J. Clin. Toxicol. 2012, 2, 1–2. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.H.; Baek, J.M.; Lee, D.S.; Park, I.Y.; Won, J.M.; Sung, K.Y. Toxicity from intra-abdominal injection of chlorfenapyr. Case Rep. Emerg. Med. 2013, 2013, 425179. [Google Scholar] [CrossRef] [Green Version]
- Tharaknath, V.R.; Prabhakar, Y.V.S.; Kumar, K.S.; Babu, N.K. Clinical and radiological findings in chlorfenapyr poisoning. Ann. Indian Acad. Neurol. 2013, 16, 252–254. [Google Scholar] [CrossRef]
- Kim, D.H.; Kim, S.C.; Kim, D.S.; Kang, C. A patient fatality following the ingestion of a small amount of chlorfenapyr. J. Emergencies Trauma Shock 2014, 7, 239–241. [Google Scholar] [CrossRef]
- Ku, J.E.; Joo, Y.S.; You, J.S.; Chung, S.P.; Lee, H.S. A case of survival after chlorfenapyr intoxication with acute pancreatitis. Clin. Exp. Emerg. Med. 2015, 2, 63–66. [Google Scholar] [CrossRef]
- Baek, B.H.; Kim, S.K.; Yoon, W.; Heo, T.W.; Lee, Y.Y.; Kang, H.K. Chlorfenapyr-Induced Toxic Leukoencephalopathy with Radiologic Reversibility: A Case Report and Literature Review. Korean J. Radiol. 2016, 17, 277–280. [Google Scholar] [CrossRef]
- Furubeppu, H.; Yasuda, T.; Miyamoto, S.; Madokoro, Y.; Ito, T.; Kakihana, Y. Fatal chlorfenapyr poisoning: A case report. Poisoning Study 2017, 30, 379–382. [Google Scholar]
- Chomin, J.; Heuser, W.; Nogar, J.; Ramnarine, M.; Stripp, R.; Sud, P. Delayed hyperthermia from chlorfenapyr overdose. Am. J. Emerg. Med. 2018, 36, 2129.e1–2129.e2. [Google Scholar] [CrossRef]
- Han, S.-K.; Yeom, S.-R.; Lee, S.-H.; Park, S.-C.; Kim, H.-B.; Cho, Y.-M.; Park, S.-W. A fatal case of chlorfenapyr poisoning following dermal exposure. Hong Kong J. Emerg. Med. 2018, 26, 375–378. [Google Scholar] [CrossRef]
- Qiu, C.; Sun, H.; Xiao, H.; Cao, Y. Clinical and CT Manifestations of Delayed Toxic Encephalopathy caused by Low-Dose Chlorfenapyr Poisoning: A Case Report. J. Clin. Toxicol. 2020, 11, 464. [Google Scholar]
- Lee, J.Y. Delayed death after chlorfenapyr poisoning. J. Korean Soc. Clin. Toxicol. 2021, 19, 51–54. [Google Scholar]
- Kim, J.H.; Park, N.H.; Park, J.Y.; Kim, S.-J. Magnetic Resonance Imaging and Clinical Features of Chlorfenapyr-Induced Toxic Leukoencephalopathy: A Case Report. J. Korean Soc. Radiol. 2020, 81, 985–989. [Google Scholar] [CrossRef]
- Hoshiko, M.; Naito, S.; Koga, M.; Mori, M.; Hara, K.; Ishitake, T. Case report of acute death on the 7th day due to exposure to the vapor of the insecticide chlorfenapyr. Chudoku Kenkyu Chudoku Kenkyukai Jun Kikanshi Jpn. J. Toxicol. 2007, 20, 131–136. [Google Scholar]
- Watanabe, E.; Baba, K.; Eun, H.; Arao, T.; Ishii, Y.; Ueji, M.; Endo, S. Evaluation of a commercial immunoassay for the detection of chlorfenapyr in agricultural samples by comparison with gas chromatography and mass spectrometric detection. J. Chromatogr. A 2005, 1074, 145–153. [Google Scholar] [CrossRef]
- Tralopyril product type-21. Regulation (EU) No 528/2012 Concerning the Making Available on the Market and Use of Biocidal Products. Available online: https://echa.europa.eu/information-on-chemicals/biocidal-active-substances/-/disas/factsheet/1403/PT21 (accessed on 30 September 2022).
- Li, H.; Sun, F.; Hu, S.; Sun, Q.; Zou, N.; Li, B.; Mu, W.; Lin, J. Determination of Market, Field Samples, and Dietary Risk Assessment of Chlorfenapyr and Tralopyril in 16 Crops. Foods 2022, 11, 1246. [Google Scholar] [CrossRef]
- Oliveira, I.B.; Schönenberger, R.; Barroso, C.M.; Suter, M.J.-F. LC-MS/MS determination of tralopyril in water samples. Chemosphere 2016, 145, 445–449. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Post-Ingestion, h | 4 | 113 | 156 |
|---|---|---|---|
| White blood cell count, 3.9 × 109/L–10.6 × 109/L | 9.6 | 4.97 | 8.39 |
| Differential count (%) | |||
| Neutrophil | 84.9 | 63.6 | 89.5 |
| Lymphocyte | 9.6 | 27.4 | -- |
| Monocyte | 4.6 | 7.2 | -- |
| Hemoglobin, 12.3–18.3 g/dL | 14.7 | 15.3 | 14.5 |
| Platelet count, 150 × 109/L–400 × 109/L | 201 | 232 | -- |
| Sodium, mEq/L | 145 | 138 | 142 |
| Potassium, mEq/L | 3.9 | 3.7 | 4.1 |
| Calcium, 8.5–10.1 mg/dL | -- | 8.7 | -- |
| Chloride, mEq/L | 115 | -- | -- |
| Blood urea nitrogen, 5–25 mg/dL | 12 | 28 | -- |
| Creatinine, 0.7–1.4 mg/dL | 0.7 | 1 | 1.1 |
| Glucose, mg/dL | 89 | 159 | -- |
| Alanine transaminase, 10–50 U/L | 19 | 63 | -- |
| Alkaline phosphatase, 50–190 U/L | -- | 94 | -- |
| Total bilirubin, 0–1 mg/dL | -- | 0.58 | -- |
| Ammonia, 25–94 μg/dL | -- | 47 | -- |
| Prothrombin time, 9.8–14.2 s | -- | 11.9 | -- |
| Amylase, 20–140 U/L | 40 | -- | -- |
| C-reactive protein, <0.3 mg/dL | -- | 0.08 | 0.15 |
| Creatine kinase, 10–160 U/L | -- | 5843.4 | 8029.8 |
| Troponin-I, <0.2 ng/ml | -- | 0.02 | 0.03 |
| Osmolarity, 275–295 mOsm/Kg | 286 | -- | -- |
| Lactate, 3–12 mg/dL | 9.4 | -- | -- |
| Blood gas analysis | (Artery) | (Vein) | (Vein) |
| pH | 7.38 | 7.44 | 7.36 |
| O2 (mmHg) | 103 | 47.4 | 21.7 |
| CO2 (mmHg) | 40.3 | 44.3 | 46 |
| Bicarbonate (mmol/L) | 23.3 | 29.1 | 25.4 |
| Toxicological analysis, (serum; ng/mL) * | |||
| Chlorfenapyr | 77.4 | UQ | UQ |
| Tralopyril | 723.6 | 14,179 | 9654.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, M.-J.; Mao, Y.-C.; Hsu, C.-T.; Chung, M.-C.; Wang, T.-J.; Yu, T.-M.; Liu, P.-Y.; Fu, P.-K.; Hsieh, C.-M. A Fatal Case of Chlorfenapyr Poisoning and the Therapeutic Implications of Serum Chlorfenapyr and Tralopyril Levels. Medicina 2022, 58, 1630. https://doi.org/10.3390/medicina58111630
Chung M-J, Mao Y-C, Hsu C-T, Chung M-C, Wang T-J, Yu T-M, Liu P-Y, Fu P-K, Hsieh C-M. A Fatal Case of Chlorfenapyr Poisoning and the Therapeutic Implications of Serum Chlorfenapyr and Tralopyril Levels. Medicina. 2022; 58(11):1630. https://doi.org/10.3390/medicina58111630
Chicago/Turabian StyleChung, Ming-Jin, Yan-Chiao Mao, Chia-Tien Hsu, Mu-Chi Chung, Tsai-Jung Wang, Tung-Min Yu, Po-Yu Liu, Pin-Kuei Fu, and Chia-Ming Hsieh. 2022. "A Fatal Case of Chlorfenapyr Poisoning and the Therapeutic Implications of Serum Chlorfenapyr and Tralopyril Levels" Medicina 58, no. 11: 1630. https://doi.org/10.3390/medicina58111630