
Lower Platelet-to-Lymphocyte Ratio Was Associated with Poor Prognosis for Newborn Patients in NICU
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Selection
2.3. Data Extraction
2.4. Outcome Variables
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Association of Inflammatory Markers with Length of Hospital Stay and ICU Stay in Newborn Patients in the NICU
3.3. Association of Inflammatory Markers with Hospital Mortality in Newborn Patients in the NICU
3.4. Prognostic Significance of PLR in Newborn Patients in the NICU
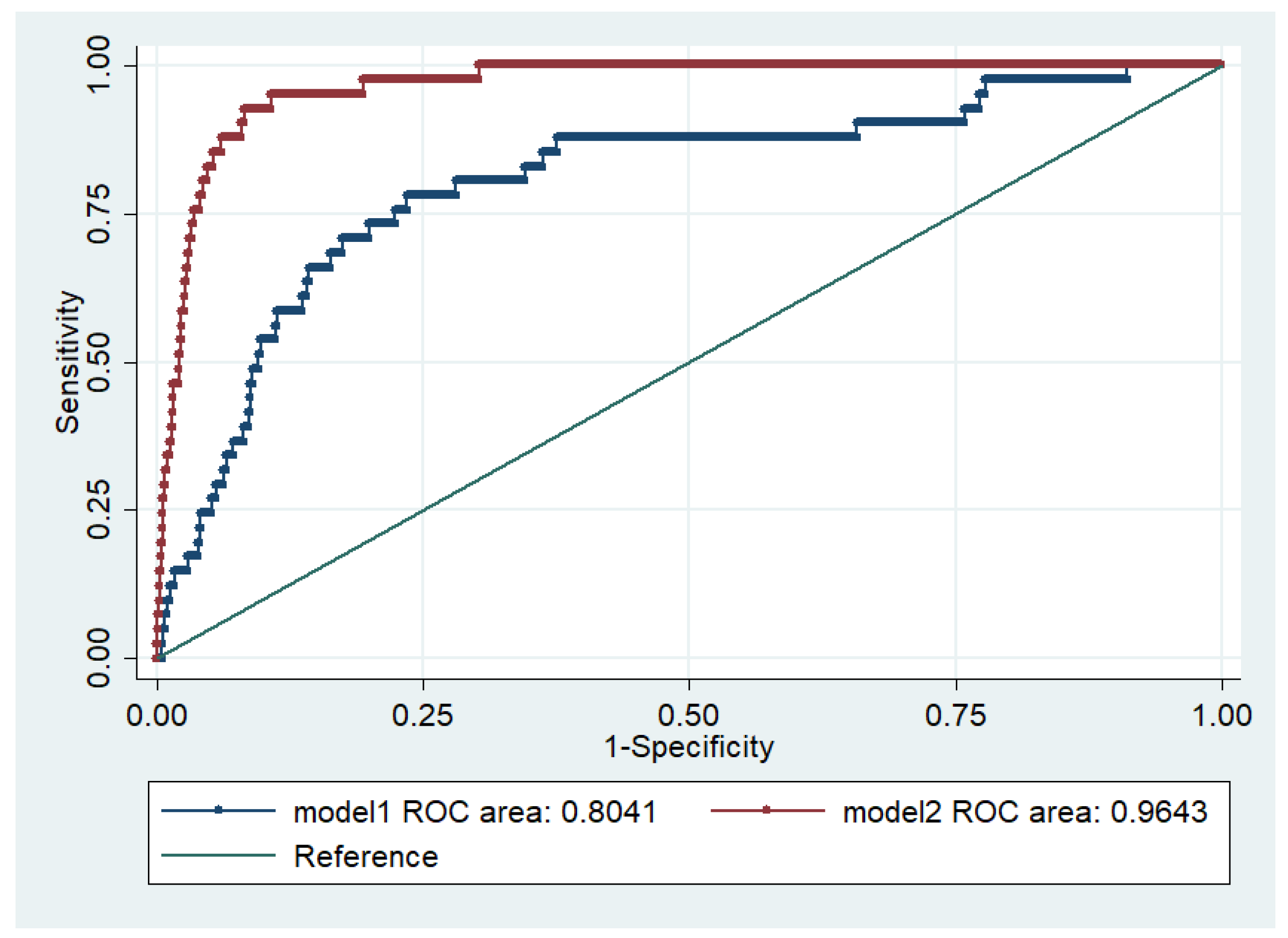
3.5. Prognostic Predictive Ability of Models Combining PLR with Other Variables for Hospital Mortality in Newborn Patients in the NICU
4. Discussion
5. Conclusions
6. Limitations of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Orsido, T.T.; Asseffa, N.A.; Berheto, T.M. Predictors of Neonatal mortality in Neonatal intensive care unit at referral Hospital in Southern Ethiopia: A retrospective cohort study. BMC Pregnancy Childbirth 2019, 19, 83. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Child Mortality Collaborators. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1725–1774. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Johnson, H.L.; Cousens, S.; Perin, J.; Scott, S.; Lawn, J.E.; Rudan, I.; Campbell, H.; Cibulskis, R.; Li, M.; et al. Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 2012, 379, 2151–2161. [Google Scholar] [CrossRef]
- Mekonnen, Y.; Tensou, B.; Telake, D.S.; Degefie, T.; Bekele, A. Neonatal mortality in Ethiopia: Trends and determinants. BMC Public Health 2013, 13, 483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teng, J.J.; Zhang, J.; Zhang, T.Y.; Zhang, S.; Li, B.S. Prognostic value of peripheral blood lymphocyte-to-monocyte ratio in patients with solid tumors: A meta-analysis. Onco Targets Ther. 2016, 9, 37–47. [Google Scholar]
- Chiriac, S.; Stanciu, C.; Singeap, A.M.; Sfarti, C.V.; Cuciureanu, T.; Trifan, A. Prognostic value of neutrophil-to-lymphocyte ratio in cirrhotic patients with acute-on-chronic liver failure. Turk. J. Gastroenterol. 2020, 31, 868–876. [Google Scholar] [CrossRef]
- Smith, R.A.; Bosonnet, L.; Raraty, M.; Sutton, R.; Neoptolemos, J.P.; Campbell, F.; Ghaneh, P. Preoperative platelet-lymphocyte ratio is an independent significant prognostic marker in resected pancreatic ductal adenocarcinoma. Am. J. Surg. 2009, 197, 466–472. [Google Scholar] [CrossRef]
- Wang, C.; He, W.; Yuan, Y.; Zhang, Y.; Li, K.; Zou, R.; Liao, Y.; Liu, W.; Yang, Z.; Zuo, D.; et al. Comparison of the prognostic value of inflammation-based scores in early recurrent hepatocellular carcinoma after hepatectomy. Liver Int. 2020, 40, 229–239. [Google Scholar] [CrossRef]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; Fletcher, C.D.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. A comparison of inflammation-based prognostic scores in patients with cancer. A Glasgow Inflammation Outcome Study. Eur. J. Cancer 2011, 47, 2633–2641. [Google Scholar] [CrossRef]
- Chen, T.; Song, C.; Liang, G.; Xu, X.; Wang, C.; Zhang, Z.; Tang, M. Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, and Their Variations as a Basis for a Prediction Model in Advanced NSCLC Patients Receiving Anlotinib. Dis. Markers 2022, 2022, 5879137. [Google Scholar] [CrossRef]
- Huang, L.; Shen, C.; Zhong, Y.; Ooi, J.D.; Eggenhuizen, P.J.; Zhou, Y.; Chen, J.; Wu, T.; Meng, T.; Xiao, Z.; et al. High levels of platelet-to-lymphocyte ratio may predict reduced risk of end stage of renal disease in Chinese patients with MPO-ANCA associated vasculitis. Zhong Nan Da Xue Xue Bao Yi Xue Ban = J. Cent. South Univ. Med. Sci. 2022, 47, 211–218. [Google Scholar]
- Liu, Y.; Zheng, J.; Zhang, D.; Jing, L. Neutrophil-lymphocyte ratio and plasma lactate predict 28-day mortality in patients with sepsis. J. Clin. Lab. Anal. 2019, 33, e22942. [Google Scholar] [CrossRef] [PubMed]
- Karagoz, I.; Yoldas, H. Platelet to lymphocyte and neutrophil to lymphocyte ratios as strong predictors of mortality in intensive care population. Rev. Assoc. Med. Bras. 2019, 65, 633–636. [Google Scholar] [CrossRef] [PubMed]
- Junare, P.R.; Debnath, P.; Nair, S.; Chandnani, S.; Udgirkar, S.; Thange, R.; Jain, S.; Deshmukh, R.; Debnath, P.; Rathi, P.; et al. Complete hemogram: Simple and cost-effective in staging and predicting outcome in acute pancreatitis. Wien. Klin. Wochenschr. 2021, 133, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Tian, T.; Wei, B.; Wang, J. Study of C-reactive protein, procalcitonin, and immunocyte ratios in 194 patients with sepsis. BMC Emerg. Med. 2021, 21, 81. [Google Scholar] [CrossRef]
- Zhang, S.; Luan, X.; Zhang, W.; Jin, Z. Platelet-to-Lymphocyte and Neutrophil-to-Lymphocyte Ratio as Predictive Biomarkers for Early-onset Neonatal Sepsis. J. Coll. Physicians Surg. Pak. 2021, 30, 821–824. [Google Scholar]
- Johnson, A.E.; Pollard, T.J.; Shen, L.; Lehman, L.W.; Feng, M.; Ghassemi, M.; Moody, B.; Szolovits, P.; Celi, L.A.; Mark, R.G. MIMIC-III, a freely accessible critical care database. Sci. Data 2016, 3, 160035. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Zhou, Y.; He, X.; Ma, J.; Guo, W.; Dong, B.; Liang, W.; Wu, Y.; Owusu-Agyeman, M.; Xue, R.; et al. Mean platelet volume/platelet count ratio predicts long-term mortality in patients with infective endocarditis. Biomark. Med. 2020, 14, 293–302. [Google Scholar] [CrossRef]
- Nording, H.M.; Seizer, P.; Langer, H.F. Platelets in inflammation and atherogenesis. Front. Immunol. 2015, 6, 98. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Kim, S.J.; Lee, M.J.; Kwon, Y.E.; Kim, Y.L.; Park, K.S.; Ryu, H.J.; Park, J.T.; Han, S.H.; Yoo, T.H.; et al. An increase in mean platelet volume from baseline is associated with mortality in patients with severe sepsis or septic shock. PLoS ONE 2015, 10, e0119437. [Google Scholar] [CrossRef]
- Manzoli, T.F.; Delgado, A.F.; Troster, E.J.; de Carvalho, W.B.; Antunes, A.C.; Marques, D.M.; Zamberlan, P. Lymphocyte count as a sign of immunoparalysis and its correlation with nutritional status in pediatric intensive care patients with sepsis: A pilot study. Clinics 2016, 71, 644–649. [Google Scholar] [CrossRef]
- Felmet, K.A.; Hall, M.W.; Clark, R.S.; Jaffe, R.; Carcillo, J.A. Prolonged lymphopenia, lymphoid depletion, and hypoprolactinemia in children with nosocomial sepsis and multiple organ failure. J. Immunol. 2005, 174, 3765–3772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miao, S.L.; Lin, T.T.; Chen, L.; Zheng, X.W.; Chen, F.F. Role of Platelet to Lymphocyte Ratio and Red Cell Distribution Width in Predicting Postoperative Complications in Patients with Acute Mesenteric Ischemia. Ann. Vasc. Surg. 2022, 84, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Akboga, M.K.; Canpolat, U.; Yayla, C.; Ozcan, F.; Ozeke, O.; Topaloglu, S.; Aras, D. Association of Platelet to Lymphocyte Ratio With Inflammation and Severity of Coronary Atherosclerosis in Patients With Stable Coronary Artery Disease. Angiology 2016, 67, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, C.; Yang, R.; Jin, J.; Liu, D.; Li, W. Prognostic value of the platelet-to-lymphocyte ratio in lung cancer patients receiving immunotherapy: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0268288. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.F.; Liu, W.Y.; Zeng, F.F.; Zheng, M.H.; Shi, H.Y.; Zhou, Y.; Pan, J.Y. Prognostic value of platelet-to-lymphocyte ratios among critically ill patients with acute kidney injury. Crit. Care 2017, 21, 238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akbas, E.M.; Hamur, H.; Demirtas, L.; Bakirci, E.M.; Ozcicek, A.; Ozcicek, F.; Kuyrukluyildiz, U.; Turkmen, K. Predictors of epicardial adipose tissue in patients with type 2 diabetes mellitus. Diabetol. Metab. Syndr. 2014, 6, 55. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Wang, X.; Wang, L.; Chen, W.; Liu, W.; Ye, T.; Hong, J.; Zhu, H.; Shen, F. Platelet-to-Lymphocyte Ratio Predicts the Presence of Diabetic Neurogenic Bladder. Diabetes Metab. Syndr. Obes. 2022, 15, 7–13. [Google Scholar] [CrossRef]
- Wang, Y.Q.; Zhi, Q.J.; Wang, X.Y.; Yue, D.S.; Li, K.; Jiang, R.C. Prognostic value of combined platelet, fibrinogen, neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in patients with lung adenosquamous cancer. Oncol. Lett. 2017, 14, 4331–4338. [Google Scholar] [CrossRef] [Green Version]
- Can, E.; Can, C. The value of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) parameters in analysis with fetal malnutrition neonates. J. Perinat. Med. 2019, 47, 775–779. [Google Scholar] [CrossRef]
- Akgun, N.; Namli Kalem, M.; Yuce, E.; Kalem, Z.; Aktas, H. Correlations of maternal neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) with birth weight. J. Matern.-Fetal Neonatal Med. 2017, 30, 2086–2091. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Survivors (n = 5197) | Nonsurvivors (n = 43) | p Value | |
|---|---|---|---|
| Demographics | |||
| Age (d) | 0.500 ± 0.004 | 0.548 ± 0.040 | 0.311 |
| Male, n (%) | 2823 (53.87%) | 26 (0.50%) | 0.420 |
| Female, n (%) | 2374 (45.31%) | 17 (0.32%) | |
| Birthweight (kg) | 1.63 (1.10–2.48) | 0.84 (0.62–1.59) | <0.0001 |
| Heart rate (bpm) | 152 (140–169) | 150 (140–168) | 0.001 |
| Laboratory events | |||
| RBC, 106/L | 4.14 (3.70–4.62) | 3.80 (3.45–4.23) | 0.001 |
| WBC, 109/L | 15.3 (10.9–19.8) | 8.8 (4.7–11.4) | <0.0001 |
| Lymphocytes, % | 29 (21–42) | 54.55 (33–67) | <0.0001 |
| Neutrophils, % | 57 (42.9–66) | 27 (19–46) | <0.0001 |
| Monocytes, % | 7 (4–9.2) | 7 (4–11) | 0.707 |
| Platelets, 109/L | 284 (232–338) | 212 (174–240) | <0.0001 |
| LMR | 4.33 (2.75–7.4) | 7.67 (4.17–13) | <0.0001 |
| NLR | 2 (1.02–3.13) | 0.55 (0.28–1.64) | 0.0008 |
| PLR | 9.77 (6.15–14.36) | 3.67 (2.73–5.72) | <0.0001 |
| Comorbidities | |||
| Hyaline membrane disease | 180 (3.56%) | 10 (23.81%) | <0.0001 |
| Sepsis | 180 (3.56%) | 10 (23.81%) | <0.0001 |
| Congestive heart failure | 14 (0.27%) | 0 (0.00%) | 0.736 |
| Cardiac arrhythmias | 19 (0.36%) | 0 (0.00%) | 0.694 |
| Valvular disease | 8 (0.15%) | 0 (0.00%) | 0.799 |
| Pulmonary circulation disorder | 5 (0.10%) | 0 (0.00%) | 0.840 |
| Hypertension | 10 (0.19%) | 0 (0.00%) | 0.773 |
| Liver disease | 2 (0.03%) | 1 (0.015%) | <0.0001 |
| Renal failure | 0 (0.00%) | 1 (0.015%) | <0.0001 |
| Scores | |||
| SAPS II | 18.86 ± 0.15 | 37.58 ± 0.81 | <0.0001 |
| SOFA | 2.75 ± 0.05 | 10.91 ± 0.41 | <0.0001 |
| MELD | 7.97 ± 0.05 | 11.64 ± 0.70 | <0.0001 |
| Length of Hospital Stay | Length of ICU Stay | |||
|---|---|---|---|---|
| Spearman’s Rho | p Value | Spearman’s Rho | p Value | |
| LMR | 0.228 | <0.0001 | 0.254 | <0.0001 |
| NLR | −0.427 | <0.0001 | −0.448 | <0.0001 |
| PLR | −0.416 | <0.0001 | −0.442 | <0.0001 |
| Q1 | Q2 | Q3 | Q4 | p Value | |
|---|---|---|---|---|---|
| LMR | |||||
| Survivors | 1364 (26.03%) | 1288 (24.58%) | 1288 (24.58%) | 1257 (23.99%) | <0.0001 |
| Nonsurvivors | 3 (0.06%) | 5 (0.10%) | 6 (0.11%) | 29 (0.55%) | |
| NLR | |||||
| Survivors | 1285 (24.52%) | 1277 (24.37%) | 1284 (24.50%) | 1351 (25.78%) | <0.0001 |
| Nonsurvivors | 31 (0.59%) | 4 (0.076%) | 4 (0.076%) | 4 (0.076%) | |
| PLR | |||||
| Survivors | 1258 (24.01%) | 1283 (24.48%) | 1288 (24.58%) | 1368 (26.11%) | <0.0001 |
| Nonsurvivors | 32 (0.61%) | 5 (0.10%) | 2 (0.038%) | 4 (0.076%) |
| Outcome | OR | 95% CI | p Value |
|---|---|---|---|
| Hospital mortality | |||
| PLR | 0.76 | 0.69–0.83 | <0.0001 |
| NLR | 0.50 | 0.37–0.69 | <0.0001 |
| LMR | 1.03 | 1.01–1.05 | <0.0001 |
| MELD | 1.19 | 1.12–1.25 | <0.0001 |
| SAPS II | 1.17 | 1.13–1.21 | <0.0001 |
| Liver disease | 63.18 | 5.62–710.58 | 0.001 |
| 90-day mortality | |||
| PLR | 0.76 | 0.69–0.84 | <0.0001 |
| NLR | 0.49 | 0.36–0.68 | <0.0001 |
| LMR | 1.04 | 1.02–1.05 | <0.0001 |
| MELD | 1.18 | 1.12–1.25 | <0.0001 |
| SAPS II | 1.17 | 1.13–1.22 | <0.0001 |
| Liver disease | 63.18 | 5.62–710.58 | 0.001 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Variable | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Hospital Mortality | ||||
| PLR | 0.84 (0.75–0.95) | 0.005 | 0.75 (0.67–0.84) | <0.0001 |
| NLR | 1.37 (0.98–1.90) | 0.063 | 1.18 (0.85–1.65) | 0.315 |
| LMR | 1.01 (0.99–1.03) | 0.253 | 1.01 (0.99–1.03) | 0.377 |
| MELD | 0.89 (0.80–0.99) | 0.028 | 1.11 (1.05–1.19) | <0.0001 |
| SAPS II | 1.19 (1.14–1.26) | <0.0001 | ||
| Liver disease | 11.39 (0.84–154.04) | 0.067 | ||
| 90-day Mortality | ||||
| PLR | 0.85 (0.76–0.96) | 0.010 | 0.79 (0.71–0.89) | <0.0001 |
| NLR | 1.32 (0.94–1.86) | 0.106 | 1.15 (0.82–1.63) | 0.417 |
| LMR | 1.01 (0.99–1.03) | 0.182 | 1.01 (0.99–1.03) | 0.232 |
| MELD | 0.88 (0.79–0.98) | 0.017 | 1.12 (1.04–1.19) | 0.001 |
| SAPS II | 1.20 (1.14–1.27) | <0.0001 | ||
| Liver disease | 11.53 (0.83–159.82) | 0.068 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tang, Y.; Teng, Y.; Xu, L.; Xu, G.; Chen, D.; Jin, X.; Li, W.; Jin, X.; Zhu, W.; Hu, B.; et al. Lower Platelet-to-Lymphocyte Ratio Was Associated with Poor Prognosis for Newborn Patients in NICU. Medicina 2022, 58, 1397. https://doi.org/10.3390/medicina58101397
Tang Y, Teng Y, Xu L, Xu G, Chen D, Jin X, Li W, Jin X, Zhu W, Hu B, et al. Lower Platelet-to-Lymphocyte Ratio Was Associated with Poor Prognosis for Newborn Patients in NICU. Medicina. 2022; 58(10):1397. https://doi.org/10.3390/medicina58101397
Chicago/Turabian StyleTang, Yanfei, Yiqun Teng, Lingyan Xu, Guangtao Xu, Deqing Chen, Xin Jin, Wanlu Li, Xiuhui Jin, Wen Zhu, Bo Hu, and et al. 2022. "Lower Platelet-to-Lymphocyte Ratio Was Associated with Poor Prognosis for Newborn Patients in NICU" Medicina 58, no. 10: 1397. https://doi.org/10.3390/medicina58101397