
Emergency General Surgery and COVID-19 Pandemic: Are There Any Changes? A Scoping Review
 ,
,  , ,
, , 
Abstract
:1. Introduction
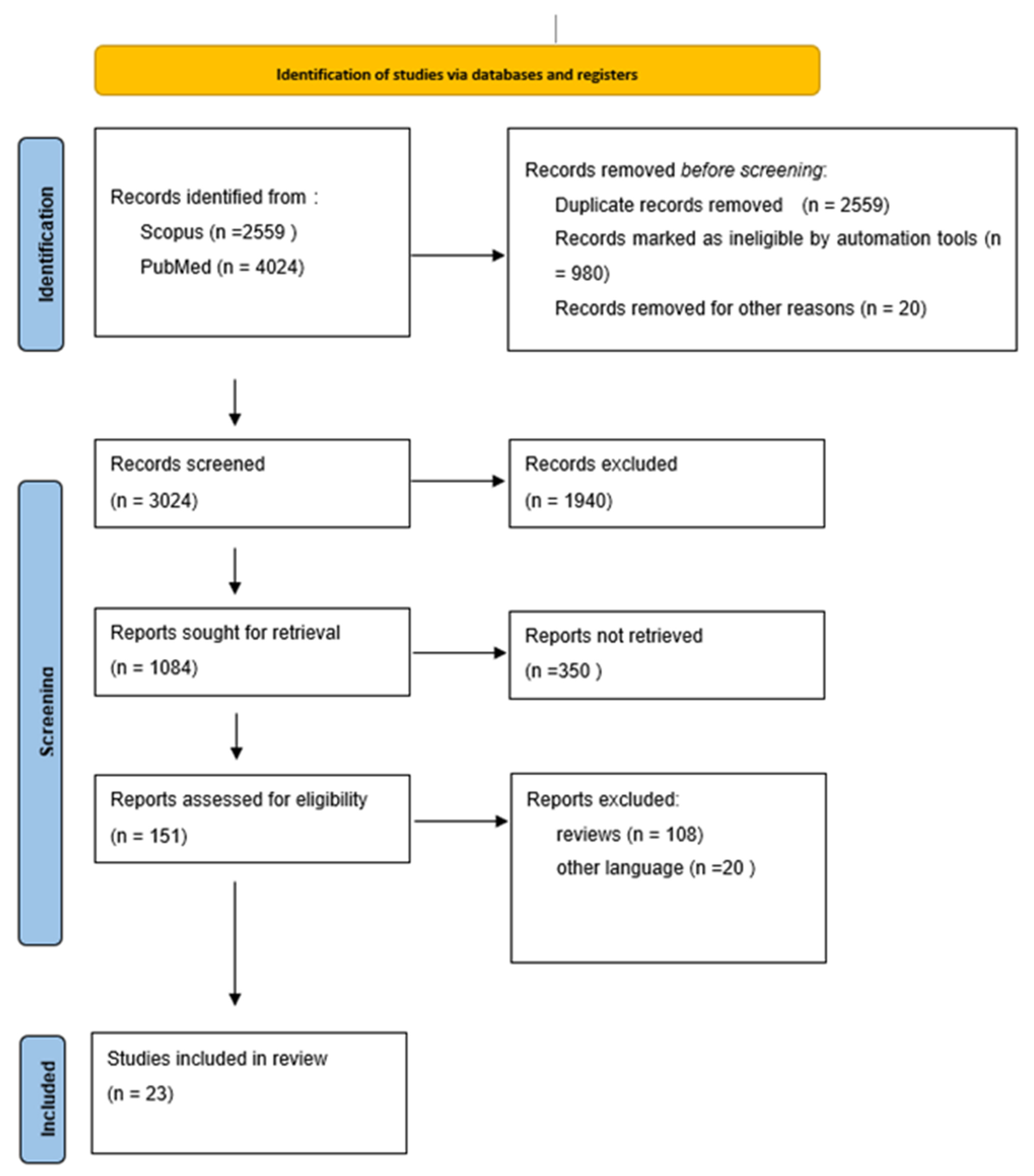
2. Methods
3. Results
3.1. Characteristics of Studies
3.2. Differences in Presented Cases in Emergency Operation Rooms
3.3. Patient’s Characteristics—Comorbidities
3.4. Length of Hospitalization
3.5. Type of Surgeries According to Pathological Status and Surgical Approach
3.6. Complications
3.7. Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Study ID | Diagnoses | Results | |
|---|---|---|---|
| Pre | Pan | ||
| Balla et al. | Bowel ischemia (0%), Bowel occlusion (12%), Bowel perforation (12%), Abdominal trauma (4%), Appendectomy (16%), Cholecystectomy (12%), Abdominal wall (4%), Pneumothorax (16%), Urology (12%), Other (12%) | Bowel ischemia (11.8%), Bowel occlusion (11.8%), Bowel perforation (17.6%), Abdominal trauma (5.8%), Appendectomy (11.8%), Cholecystectomy (11.8%), Abdominal wall (11.8%), Pneumothorax (5.8%), Urology (11.8%), Other (0%) | There were no differences in emergency general surgeries. |
| Cano-Valderrama et al. | Acute appendicitis (30.9%), Perianal abscess (12.6%), Acute cholocystitis (12.3%), Complication of an elective procedure (14.4%), Complication of an elective procedure (14.4%), Bowel obstruction (6.7%), Abdominal wall hernia (5.6%), Other (17.5%) | Acute appendicitis (34.2%), Perianal abscess (14.5%), Acute cholocystitis (2.6%), Complication of an elective prosedure (6.8%), Bowel obstruction (12.8%), Abdominal wall hernia (9.4%), Other (19.7%) | There was a change in the gender (M > F) during pandemic period. Avarage duration of symptoms prior to presenting in the emergency department was increased (p < 0.001). |
| Carpio Colmenares et al. | Acute appendicitis (55.5%), Acute lithiasic cholecystitis (37.7%), Hernias (6.7%), Gastric perforation (0%), Intestinal obstruction (0%) | Acute appendicitis (50.8%), Acute lithiasic cholecystitis (42.4%), Hernias (3.4%), Gastric perforation (1.7%), Intestinal obstruction (1.7%) | In this study there was an increase in length of stay. The degree of severity of emergency abdominal surgical pathology in pandemic has not increased, except for post operative complications. |
| Casella et al. | Appendicectomy (17%), Gastrointenstinal or Colorectal resections (18.2%) | Gastrointenstinal or Colorectal resections (25%), Abscess drainage (18.8%), Adhesiolesis (18.8%) | The time elapsed between hospital admission and surgery was increased. The percentage of patients who experience post operative complications was increased, p = 0.019. The mortality was increased (p < 0.0001) |
| D’Urbano et al. | Cholecystectomy (21.7%), Appendectomy (19.7%), Hemothorax/Pneumothorax/Pleural effusion (8.6%), GI perforation (10.9%), Bowel obstruction (15.2%), Bowel infraction (6.5%), Hemoperitoneum evacuation (6.5%), GI bleeding (2.2%), Fasciotomy/Abcess drainage/Hematoma drainage (6.5%), Other (2.2%) | Cholecystectomy (22.2%), Appendectomy (0%), Hemothorax/Pneumothorax/Pleural effusion (14.9%), GI perforation (11.1%), Bowel obstruction (33.3%), Bowel infraction (3.7%), Hemoperitoneum evacuation (0%), GI bleeding (3.7%), Fasciotomy/Abcess drainage/Hematoma drainage (11.1%), Other (0%) | D’Urbano et al. found a reduction in the number of patients who were hospitalized and underwent emergency surgery. Mean age was higher in the pre-pandemic period. The complications were increased in the pandemic era in 2020. The fatality rate after surgery decreased. |
| Drysdale et al. | Laparoscopic appendicectomy (50%), Soft tissue infection (41%), Laparoscopic cholecystectomy (26%), Laparotomy (22%), Hernia repair (8%), Gastroscopy (16%), Colonoscopy (7%), ERCP (7%) | Laparoscopic appendicectomy (48%), Soft tissue infection (46%), Laparoscopic cholecystectomy (40%), Laparotomy (21%), Hernia repair (7%), Gastroscopy (5%), Colonoscopy (13%), ERCP (6%) | Drysdale et al. reported a 13.9% rise in emergency laparoscopic cholecystectomies and emergency colonoscopies; this study did not found any other differences between the two periods. |
| Fallani et al. | Secondary peritonitis | Secondary peritonitis | Patients who underwent surgery during pandemic had a higher rate of severe peritonitis. The surgery lasted longer in the pandemic period. The mean time elapsed between hospital admission and surgery was greater in the pandemic period. In the pandemic era there was a bigger proportion of secondary peritonitis caused by appendicitis and a smaller proportion caused by perforated peptic ulcer. Complications and length of stay were increased in the pandemic group. |
| Fowler et al. | - | - | A decline was seen in the proportion of emergency procedures in general surgery; this study says the total number of procedures did not significantly decreased in emergency general. surgery. |
| Hossain et al. | Acute diverculitis | Acute diverculitis | There was a decrease in the cases of Acute diverculitis. The proportion of patients who underwent emergency surgery was significantly higher during the pandemic period (p = 0.04). |
| Kamil et al. | Cholecystitis, Appendicitis, Diverculitis | Cholecystitis, Appendicitis, Diverculitis | Hospital admissions decreased in March and increased in April and May. The treatment method was primarily conservative in 2020. |
| Karlafti et al. | Digestive system surgeries (19.7%), Hernia repair (22.6%), Soft tissue infection surgeries (28.3%), Hepatobiliary surgeries (21.7%) | Digestive system surgeries (16.6%), Hernia repair (18.4%), Soft tissue infection surgeries (26%), Hepatobiliary surgeries (30.5%) | During the pandemic period, mortality rates nearly doubled (2.2% vs. 4%), although the total number was significantly lower than during the control period. |
| Kumaira Fonseca et al. | Acute appendicitis | Acute appendicitis | The cases were lower in the pandemic period. The average time of symptom onset to arrival at the emergency department was higher in the pandemic. There was a higher proportion of complicated cases during the pandemic. |
| Madzaro et al. | Complexity: Minor (749)/Moderate (1311)/Major (848)/Major+ (82) | Complexity: Minor (508)/Moderate (1081)/Major (712)/Major+ (57) | There were differences in complications in the lenght of stay and in post-operative mortality; this study finds post-operative mortality of COVID-19 positive patients was greater for Minor, Moderate, Major and Major+ procedures. |
| Malik et al. | Hernia repair | Hernia repair | There was an 18% increase in the number of surgeries for Hernia reparation in the pandemic era. The duration of symptoms prior to presenting in the ER was slightly increased in 2020. In this study is mentioned that the pandemic resulted to cancellations of non-urgent elective procedures for hernias and that is why emergency hernia operations were increased in the pandemic era, considering the acute presentation of symptomatic hernias. |
| Osorio et al. | - | - | This multi-centered study concluded no differences in the results between the two periods, but points out that patients infected with SARS-CoV-19 had worse outcomes after the surgery. |
| Rashdan et al. | Acute appendicitis, Acute cholecystitis, Acute pancreatitis, Intestinal obtruction, Complicated hernia, For observation, Perianal pain, Soft tissue infection, Burn, Trauma, Others | Acute appendicitis, Acute cholecystitis, Acute pancreatitis, Intestinal obtruction, Complicated hernia, For observation, Perianal pain, Soft tissue infection, Burn, Trauma, Others | Admissions decreased. There were more male patients in the pandemic group. Duration of symptoms before the ER visit was longer in the pandemic. |
| Rausei et al. | Appendicitis, Cholecystitis, Bowel obstruction, Bowel perforation, GI bleeding, Proctologic diseases, Abdominal trauma | Appendicitis, Cholecystitis, Bowel obstruction, Bowel perforation, GI bleeding, Proctologic diseases, Abdominal trauma | Emergency surgical admissions and surgical operations significantly decreased from March 2019 to March 2020, no other changes found. |
| Salgaonkar et al. | Acute appendicitis | Acute appendicitis | The only differences on appendicectomy was that percentage of surgical site infections was increased in the pandemic period. |
| Surek et al. | Trauma (11), GI bleeding (9), Acute mesenteric ischemia (2), Perforations (14), Acute mechanical intestinal obstruction (25), Incarcerated hernia (25), Acute cholecystitis (55), Acute appendicitis (155) | Trauma (12), GI bleeding (7), Acute mesenteric ischemia (2), Perforations (18), Acute mechanical intestinal obstruction (24), Incarcerated hernia (2), Acute cholecystitis (29), Acute appendicitis (42) | There was a 59.1% reduction in the number of emergency surgeries and 50% decrease in the number of non-operatively followed patients in the pandemic group. There was a 47.3% and a 73% reduction in the number of patients who had surgery for acute cholecystitis and for acute appendicitis, respectivly. |
| van Aert et al. | Minor trauma (2.5%), Major trauma (17.9%), Polytrauma (5.6%), Neck of Femur (53.7%), Soft tissue trauma (3.7%), Pediatric trauma (16.7%) | Minor trauma (8.1%), Major trauma (21.4%), Polytrauma (4.6%), Neck of Femur (50.3%), Soft tissue trauma (5.8%), Pediatric trauma (9.8%) | There was an overall decrease in trauma-related admissions. The age was significantly higher in 2020 with fewer adolecents and more senior patients. In 2020, more patients underwent minor surgery. Comparingly in 2020 there was a bigger proportion of patients falling from standing high than 2019; furthermore, trauma-related surgeries were increased in 2020. There was a reduction of the number of car and motorcycle accidents. |
| Wade et al. | - | - | - |
| Wilms et al. | Appendicitis | Appendicitis | The overall number of patients decreased. Avarage duration of symptoms prior to presenting in the emergency department was increased. |
| Yasunori Nishida et al. | Acute appendicitis (45%), Acute cholecystitis (12%), Strangulated small bowel obstruction (5%), Colon perforation (10%), GI perforation (11%), Malignant bowel obstruction (4%), Others (8%) | Acute appendicitis (41%), Acute cholecystitis (18%), Strangulated small bowel obstruction (14%), Colon perforation (1%), GI perforation (5%), Malignant bowel obstruction (6%), Others (4%) | This study found not statistically significant differences of the involved parameters of our study. |
| Age (Years) | Gender | BMI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Study ID | Pre | Pan | p | Pre | Pan | p | Pre | Pan | p |
| Cano-Valderrama et al. | 55 | 52.6 | 0.276 | F (50.88%) | F (33.8%) | 0.001 | |||
| D’Urbano et al. | 65 | 63.5 | M (54.3%) | M (55.5%) | |||||
| Fallani et al. | 44 | 49 | 0.223 | M (53%) | M (63.1%) | 0.065 | 25.2 ± 2.4 | 25.3 ± 2.1 | 0.675 |
| Hossain et al. | 63.3 | 62.6 | 0.762 | M (47.7%) | M (46.2%) | 0.867 | |||
| Karlafti et al. | 51.2 ± 17.6 | 49.3 ± 17.1 | M (53.9%) | M (58.2%) | 0.284 | ||||
| Kumaira Fonseca et al. | 34.3 ± 5.8 | 38.2 ± 18.1 | ns | F (62.2%) | F (55.6%) | Ns | |||
| Osorio et al. | 57 | 56 | M (58.6%) | M (59.8%) | 27.3 | 27.3 | ns | ||
| Surek et al. | 46.1 ± 17.9 | 46.6 ± 18.9 | 0.890 | M (63.5%) | M (65%) | 0.928 | |||
| Wilms et al. | 35 ± 19 | 36 ± 20 | 0.24 | M (N:510) | M (N:468) | 0.18 | |||
| F (N:517) | F (N:420) | ||||||||
| van Aert et al. | 42 | 48 | >0.001 | F (47.8%) | F (52%) | 0.088 | |||
| Study ID | Country | Publication Year | Study Period | Patients Included | Number of Surgeries | Average Duration of Symptoms Prior to Presenting in Emergency | Time (Hours) Elapsed between Hospital Admission and Surgery | Length of Stay (Days) | Complications % of pts Experiencing Complications | Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Pan | Pre | Pan | Pre | Pan | Pre | Pan | Pre | Pan | Pre | Pan | Pre | Pan | ||||
| Balla et al. | Italy | Junuary 2021 | 8/3–4/5/2019–8/3–4/5/2020 | 99 | 41 | 25 | 17 | ||||||||||
| Cano-Valderrama et al. | Spain | July 2020 | 11/3–21/4/2019–11/3–21/4/2020 | 285 | 117 | 285 | 117 | 44.6 h | 71 h | 12.4 (N: 285) | 12.3 (N: 117) | 12.2 | 8.5 | 4.27% | 6.67% | ||
| Carpio Colmenares et al. | Peru | 2021 | 11/3–8/6/2019–11/3–8/6/2020 | 45 | 59 | 45 | 59 | 1.73 ± 1.07 | 2.74 ± 2.80 | ||||||||
| Casella et al. | Italy | February 2022 | 9/3–9/5/2019–9/3–9/5/2020 | 476 | 79 | 88 | 16 | 16.73 ± 1.76 (N: 88) | 22.56 ± 11.12 (N:16) | 0% | 31.3% | ||||||
| D’Urbano et al. | Italy | September 2020 | 9/3–9/4/2019–9/3–9/4/2020 | 46 | 27 | 46 | 27 | 36.9% | 55.5% | 19.6% | 11.1% | ||||||
| Drysdale et al. | Australia | July 2020 | 1/4–19/5/2019–30/3–17/5/2020 | 506 | 475 | 180 | 205 | 1 pt | 1 pt | ||||||||
| Fallani et al. | Italy | December 2020 | 23/3–4/5/2019–23/3–4/5/2020 | 183 | 149 | 183 | 149 | 18% | 35.6% | 4.9% | 6% | ||||||
| Fowler et al. | Australia | December 2020 | 1/3–24/4/2019–1/3–24/4/2020 | 1574 | 1240 | 694 | 596 | ||||||||||
| Hossain et al. | UK | 2020 | 1/3–30/6/2019–1/3–30/6/2020 | 107 | 52 | 1 | 4 | ||||||||||
| Kamil et al. | Ireland | June 2021 | 1/3–31/5/2019–1/3–31/5/2020 | 138 | 94 | 84 | 33 | 2.70 ± 2.86 days | 3.13 ± 2.67 days | ||||||||
| Karlafti et al. | Greece | November 2021 | 3/2019–2/2020–3/2020–2/2021 | 456 | 223 | 456 | 223 | 4 ± 8.6 | 4.6 ± 10.3 | 2.2% | 4% | ||||||
| Kumaira Fonseca et al. | Brazil | 2020 | March–April 2019–March–April 2020 | 82 | 36 | 82 | 36 | 13.4% | 11.1% | ||||||||
| Madzaro et al. | Spain | November 2021 | 1/3–30/6/2019 1/3-30/6/2020 | 2800 | 2188 | 2800 | 2188 | <0.001 | |||||||||
| Malik et al. | UK | June 2021 | 1/1–31/12/2019–1/1–31/12/2020 | 32 | 39 | 32 | 39 | ||||||||||
| Osorio et al. | Spain | September 2021 | 1/3–30/6/2019–1/3–30/6/2020 | 2992 | 2315 | 2992 | 2315 | 4 | 4 | 3.2% | 5.2% | ||||||
| Rashdan et al. | Jordan | May 2021 | March–June 2019–March–June 2020 | 201 | 143 | 154 | 60 | 57 ± 64.4 min | 95.32 ± 148.62 min | ||||||||
| Rausei et al. | USA | August 2020 | 3/2019–3/2020 | 869 | 475 | 515 | 302 | ||||||||||
| Salgaonkar et al. | UK | March 2021 | 1/3–5/6/2019–1/3–5/6/2020 | 206 | 132 | 206 | 132 | 0% | 0.7% | ||||||||
| Surek et al. | Germany | November 2020 | 14/3–15/5/2019–14/3–15/5/2020 | 453 (total in both) | 453 | 252 | 103 | 17.06% | 24.27% | 1.19% | 4.85% | ||||||
| van Aert et al. | The Netherlands | February 2021 | 11/3–10/5/2019–11/3–10/5/2020 | 1717 | 1182 | 162 | 173 | (N:162) | (N:173) | ||||||||
| Wade et al. | England | June 2020 | 23/3–10/5/2019–23/3–10/5/2020 | 193 | 64 | - | - | ||||||||||
| Wilms et al. | Germany | Janruary 2021 | February–March/2019–February–March/2020 | 1027 | 888 | 1027 | 888 | 37.5 ± 45.8 h | 41.1 ± 55.9 h | 4.5 ± 4.1 | 4.6 ± 4.0 | ||||||
| Yasunori Nishida et al. | Japan | December 2020 | 1/3–30/6/2019–1/3–30/6/2020 | 90 | 89 | 90 | 89 | ||||||||||
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Rothan, H.A.; Byrareddy, S.N. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J. Autoimmun. 2020, 109, 102433. [Google Scholar] [CrossRef] [PubMed]
- Baccini, M.; Cereda, G.; Viscardi, C. The first wave of the SARS-CoV-2 epidemic in Tuscany (Italy): A SI2R2D compartmental model with uncertainty evaluation. PLoS ONE 2021, 16, e0250029. [Google Scholar] [CrossRef] [PubMed]
- Pedziwiatr, M.; Lasek, A.; Wysocki, M.; Mavrikis, J.; Mysliwiec, P.; Bobowicz, M.; Karcz, W.; Michalik, M.; Makarewicz, W.; Major, P.; et al. Complicated appendicitis: Risk factors and outcomes of laparoscopic appendectomy–results from Pol-LA (Polish Laparoscopic Appendectomy) multicenter large cohort study. Ulus. Travma Ve Acil Cerrahi Derg. = Turk. J. Trauma Emerg. Surg. TJTES 2018, 25, 129–136. [Google Scholar] [CrossRef]
- Casella, G.; Castagneto-Gissey, L.; Lattina, I.; Ferrari, P.; Iodice, A.; Tesori, C.; Catani, M.; Assenza, M.; Mingoli, A.; LA Torre, F. Repercussions of covid-19-related national lockdown on emergency surgery department: A longitudinal cohort monocentric study. Minerva Surg. 2022, 71, 22–29. [Google Scholar] [CrossRef]
- Wade, S.; Nair, G.; Ayeni, H.A.; Pawa, A. A Cohort Study of Emergency Surgery Caseload and Regional Anesthesia Provision at a Tertiary UK Hospital During the Initial COVID-19 Pandemic. Cureus 2020, 12, e8781. [Google Scholar] [CrossRef]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.J.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J.M.; et al. Acute Care Surgery during the COVID-19 pandemic in Spain: Changes in volume, causes and complications. A multicentre retrospective cohort study. Int. J. Surg. 2020, 80, 157–161. [Google Scholar] [CrossRef]
- Osorio, J.; Madrazo, Z.; Videla, S.; Sainz, B.; Rodríguez-González, A.; Campos, A.; Santamaría, M.; Pelegrina, A.; González-Serrano, C.; Aldeano, A.; et al. Analysis of outcomes of emergency general and gastrointestinal surgery during the COVID-19 pandemic. Br. J. Surg. 2021, 108, 1438–1447. [Google Scholar] [CrossRef]
- Willms, A.G.; CAMIN Study Group; Oldhafer, K.J.; Conze, S.; Thasler, W.E.; von Schassen, C.; Hauer, T.; Huber, T.; Germer, C.-T.; Günster, S.; et al. Appendicitis during the COVID-19 lockdown: Results of a multicenter analysis in Germany. Langenbeck’s Arch. Surg. 2021, 406, 367–375. [Google Scholar] [CrossRef]
- Drysdale, H.R.E.; Ooi, S.; Nagra, S.; Watters, D.A.; Guest, G.D. Clinical activity and outcomes during Geelong’s general surgery response to the coronavirus disease 2019 pandemic. ANZ J. Surg. 2020, 90, 1573–1579. [Google Scholar] [CrossRef]
- Karlafti, E.; Benioudakis, E.S.; Paramythiotis, D.; Sapalidis, K.; Kaiafa, G.; Didangelos, T.; Michalopoulos, A.; Kesisoglou, I.; Savopoulos, C. Does the COVID-19 Pandemic Affect Morbidity and Mortality Rates of Emergency General Surgery? A Retrospective Study from a Single-Center Tertiary Greek Hospital. Medicina 2021, 57, 1185. [Google Scholar] [CrossRef] [PubMed]
- Rausei, S.; Ferrara, F.; Zurleni, T.; Frattini, F.; Chiara, O.; Pietrabissa, A.; Sarro, G. Dramatic decrease of surgical emergencies during COVID-19 outbreak. J. Trauma Acute Care Surg. 2020, 89, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Van Aert, G.J.; van der Laan, L.; Winter, L.J.B.-D.; Berende, C.A.; de Groot, H.G.; van Hensbroek, P.B.; Schormans, P.M.; Winkes, M.B.; Vos, D.I. Effect of the COVID-19 pandemic during the first lockdown in The Netherlands on the number of trauma-related admissions, trauma severity and treatment: The results of a retrospective cohort study in a level 2 trauma centre. BMJ Open 2021, 11, e045015. [Google Scholar] [CrossRef] [PubMed]
- Fowler, S.; Zahir, S.F.; Manning, W.; Kearney, A.; Sturgess, D. Effect of the COVID-19 pandemic first wave and public policy on elective and emergency surgery provision in Southern Queensland. ANZ J. Surg. 2021, 91, 249–254. [Google Scholar] [CrossRef]
- Surek, A.; Ferahman, S.; Gemici, E.; Dural, A.C.; Donmez, T.; Karabulut, M. Effects of COVID-19 pandemic on general surgical emergencies: Are some emergencies really urgent? Level 1 trauma center experience. Eur. J. Trauma Emerg. Surg. 2021, 47, 647–652. [Google Scholar] [CrossRef]
- Colmenares, Y.T.C.; de Castilla, D.C.R.; Barrionuevo, L.A.G.; Valencia, M.R.L.; Doria, P.M.; Nole, V.M.; Escalante, F.P.; Saenz, C.R.; Borda-Luque, G. Emergency Abdominal Laparoscopic Surgery During the Coronavirus Disease 2019 Pandemic: Experience in a Private Center in Peru. J. Laparoendosc. Adv. Surg. Tech. 2021, 31, 261–265. [Google Scholar] [CrossRef]
- Nishida, Y.; Otagiri, N.; Tauchi, K. Emergency abdominal surgeries remain unchanged in the COVID-19 affected environment: A single-center experience at a community hospital in Japan. Acute Med. Surg. 2021, 8, e623. [Google Scholar] [CrossRef]
- Salgaonkar, H.; Aladeojebi, A.; Murcott, D.; Nnaji, M.; Tsiamis, A.; Cheruvu, C.V. Emergency appendicectomy during COVID-19 pandemic—A single UK centre experience. Pol. J. Surg. 2021, 93, 33–39. [Google Scholar] [CrossRef]
- D’Urbano, F.; Fabbri, N.; Radica, M.K.; Rossin, E.; Carcoforo, P. Emergency surgery in COVID-19 outbreak: Has anything changed? Single center experience. World J. Clin. Cases 2020, 8, 3691–3696. [Google Scholar] [CrossRef]
- Hossain, N.; Naidu, V.; Hosny, S.; Khalifa, M.; Mathur, P.; Al Whouhayb, M. Hospital Presentations of Acute Diverticulitis During COVID-19 Pandemic may be More Likely to Require Surgery due to Increased Severity: A Single-Centre Experience. Am. Surg. 2020, 81, 133–139. [Google Scholar] [CrossRef]
- Fonseca, M.K.; Trindade, E.N.; Filho, O.P.C.; Nácul, M.P.; Seabra, A.P. Impact of COVID-19 Outbreak on the Emergency Presentation of Acute Appendicitis. Am. Surg. 2020, 86, 1508–1512. [Google Scholar] [CrossRef] [PubMed]
- Madrazo, Z.; Osorio, J.; Videla, S.; Sainz, B.; Rodríguez-González, A.; Campos, A.; Santamaría, M.; Pelegrina, A.; González-Serrano, C.; Aldeano, A.; et al. P-POSSUM as mortality predictor in COVID-19-infected patients submitted to emergency digestive surgery. A retrospective cohort study. Int. J. Surg. 2021, 96, 106171. [Google Scholar] [CrossRef] [PubMed]
- Fallani, G.; Lombardi, R.; Masetti, M.; Chisari, M.; Zanini, N.; Cattaneo, G.M.; Filosa, M.; Zanzi, F.; Guerra, E.; Bonilauri, S.; et al. Urgent and emergency surgery for secondary peritonitis during the COVID-19 outbreak: An unseen burden of a healthcare crisis. Updat. Surg. 2021, 73, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Rashdan, M.; Al-Taher, R.; Al-Qaisi, M.; Khrais, I.; Salameh, M.; Obaidat, I.; Abbad, M.; Alsaadi, T.; Hani, A.B. The impact of the Covid-19 pandemic on emergency surgery in a tertiary hospital in Jordan. A cross sectional study. Ann. Med. Surg. 2021, 66, 102339. [Google Scholar] [CrossRef] [PubMed]
- Kamil, A.M.; Davey, M.G.; Marzouk, F.; Sehgal, R.; Fowler, A.L.; Corless, K.; O’Neill, M.; Collins, C.G. The impact of COVID-19 on emergency surgical presentations in a university teaching hospital. Ir. J. Med. Sci. 2021, 191, 1059–1065. [Google Scholar] [CrossRef]
- Surgical management protocol during the COVID-19 pandemic in an Italian non-referral center. Minerva Surg. 2021, 76, 281–285. [CrossRef]
- Malik, A.; Zohdy, M.; Ahmad, A.; Seretis, C. Single-centre experience of emergency hernia surgery during COVID-19 pandemic: A comparative study of the operative activity and outcomes before and after the outbreak. Med. Glas. Off. Publ. Med. Assoc. Zenica-Doboj Canton Bosnia Herzeg. 2021, 18, 462–467. [Google Scholar] [CrossRef]
- Moreland, A.; Herlihy, C.; Tynan, M.A.; Sunshine, G.; Mccord, R.F.; Hilton, C.; Poovey, J.; Werner, A.K.; Jones, C.D.; Fulmer, E.B.; et al. Timing of State and Territorial COVID-19 Stay-at-Home Orders and Changes in Population Movement—United States, March 1–May 31, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 1198–1203. [Google Scholar] [CrossRef]
- Koutserimpas, C.; Agouridakis, P.; Velimezis, G.; Papagiannakis, G.; Keramidis, I.; Ioannidis, A.; Samonis, G. The burden on public emergency departments during the economic crisis years in Greece: A two-center comparative study. Public Health 2019, 167, 16–20. [Google Scholar] [CrossRef]
- Gkentzi, D.; Katsoula, V.; Fouzas, S.; Mentis, M.; Karatza, A.; Dimitriou, G. Economic Recession and Attendances in the Pediatric Emergency Department. BioMed Res. Int. 2019, 2019, 4186486. [Google Scholar] [CrossRef] [Green Version]
- Petrovici, I.; Ionica, M.; Neagoe, O. Economic Crisis: A Factor for the Delayed Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 3998. [Google Scholar] [CrossRef] [PubMed]
- Karavokyros, I.G.; Kirkilessis, G.I.; Schizas, D.; Chelidonis, G.; Pikoulis, E.; Griniatsos, J. Emergency inguinal hernioplasties in a tertiary public Hospital in Athens Greece, during the economic crisis. BMC Surg. 2019, 19, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karlafti, E.; Kotzakioulafi, E.; Peroglou, D.-C.; Gklaveri, S.; Malliou, P.; Ioannidis, A.; Panidis, S.; Netta, S.; Savopoulos, C.; Michalopoulos, A.; et al. Emergency General Surgery and COVID-19 Pandemic: Are There Any Changes? A Scoping Review. Medicina 2022, 58, 1197. https://doi.org/10.3390/medicina58091197
Karlafti E, Kotzakioulafi E, Peroglou D-C, Gklaveri S, Malliou P, Ioannidis A, Panidis S, Netta S, Savopoulos C, Michalopoulos A, et al. Emergency General Surgery and COVID-19 Pandemic: Are There Any Changes? A Scoping Review. Medicina. 2022; 58(9):1197. https://doi.org/10.3390/medicina58091197
Chicago/Turabian StyleKarlafti, Eleni, Evangelia Kotzakioulafi, Dimitrios-Christos Peroglou, Styliani Gklaveri, Petra Malliou, Aristeidis Ioannidis, Stavros Panidis, Smaro Netta, Christos Savopoulos, Antonios Michalopoulos, and et al. 2022. "Emergency General Surgery and COVID-19 Pandemic: Are There Any Changes? A Scoping Review" Medicina 58, no. 9: 1197. https://doi.org/10.3390/medicina58091197