
Immersive Virtual Reality during Robot-Assisted Gait Training: Validation of a New Device in Stroke Rehabilitation

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
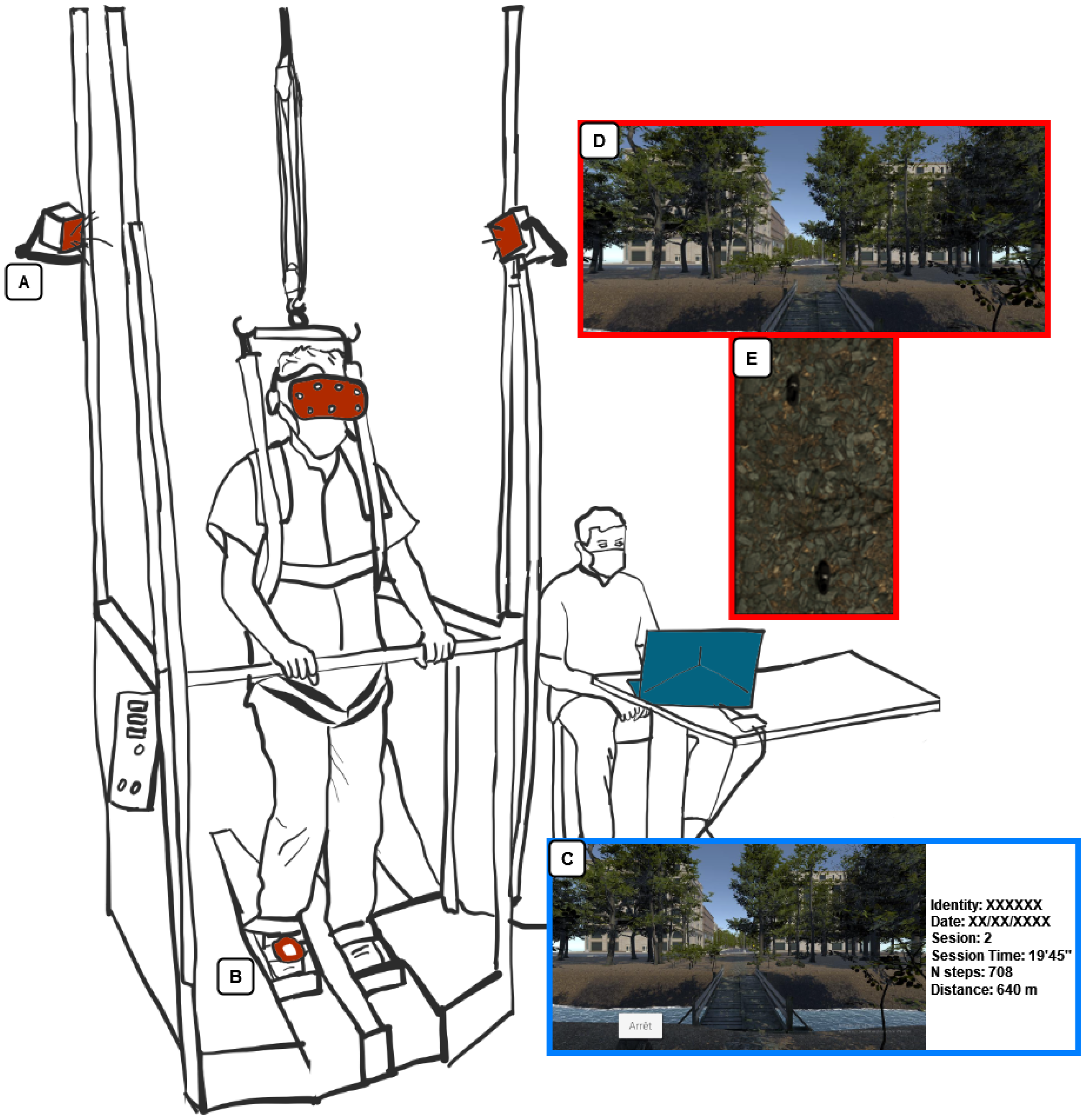
2.1. Robot-Assisted Gait Training and VR-Device
2.2. VR Environment
2.3. Procedure
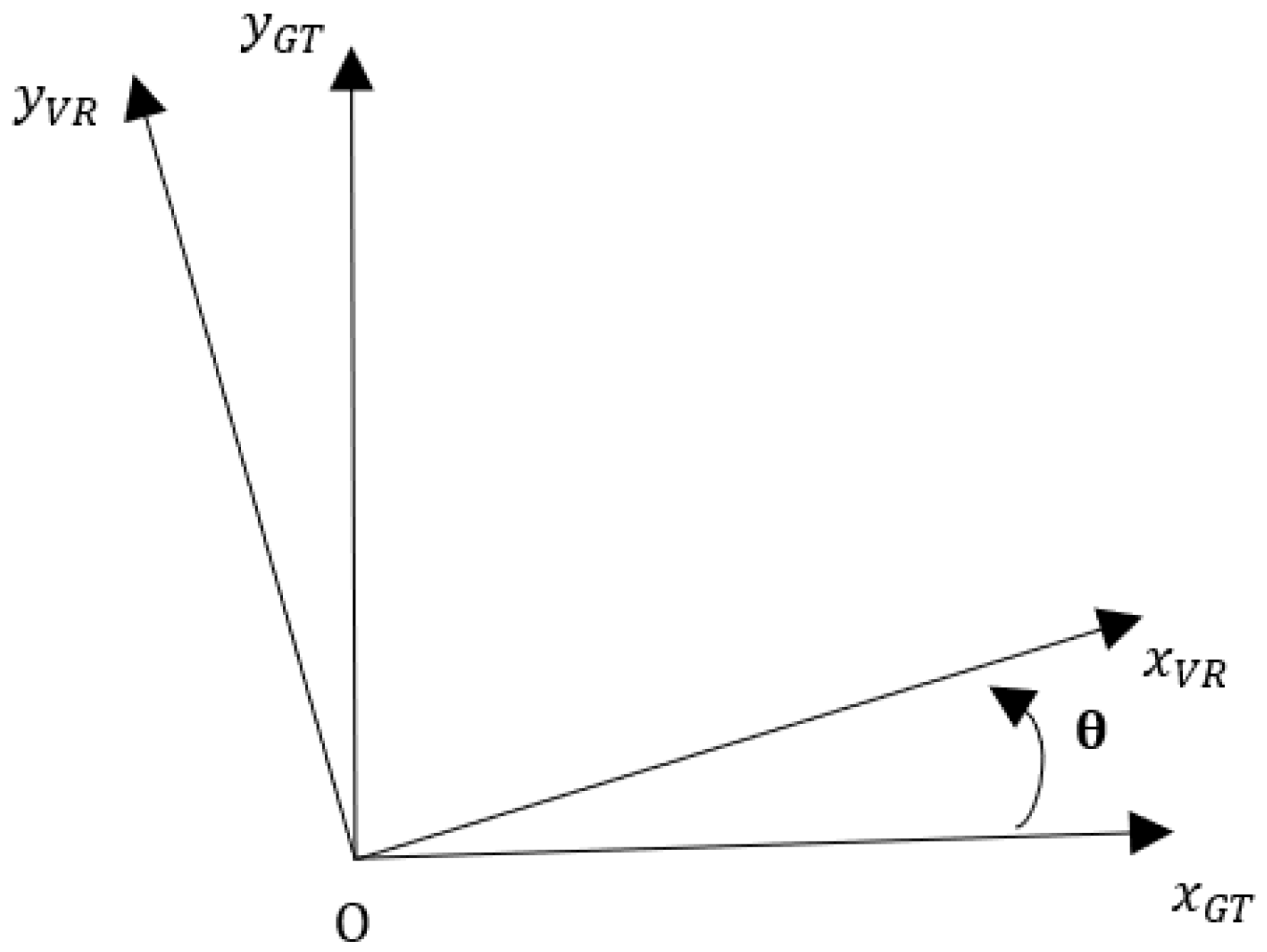
2.4. Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. The Future of Our Application
4.2. Future Research with Stroke Patients
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Recovery of walking function in stroke patients: The copenhagen stroke study. Arch. Phys. Med. Rehabil. 1995, 76, 27–32. [Google Scholar] [CrossRef]
- Beyaert, C.; Vasa, R.; Frykberg, G.E. Gait post-stroke: Pathophysiology and rehabilitation strategies. Neurophysiol. Clin. Clin. Neurophysiol. 2015, 45, 335–355. [Google Scholar] [CrossRef]
- Mohan, D.M.; Khandoker, A.H.; Wasti, S.A.; Ismail Ibrahim Ismail Alali, S.; Jelinek, H.F.; Khalaf, K. Assessment Methods of Post-stroke Gait: A Scoping Review of Technology-Driven Approaches to Gait Characterization and Analysis. Front. Neurol. 2021, 12, 650024. [Google Scholar] [CrossRef]
- Price, R.; Choy, N.L. Investigating the Relationship of the Functional Gait Assessment to Spatiotemporal Parameters of Gait and Quality of Life in Individuals with Stroke. J. Geriatr. Phys. Ther. 2019, 42, 256–264. [Google Scholar] [CrossRef]
- Coleman, E.R.; Moudgal, R.; Lang, K.; Hyacinth, H.I.; Awosika, O.O.; Kissela, B.M.; Feng, W. Early Rehabilitation After Stroke: A Narrative Review. Curr. Atheroscler. Rep. 2017, 19, 59. [Google Scholar] [CrossRef] [Green Version]
- Mehrholz, J.; Thomas, S.; Kugler, J.; Pohl, M.; Elsner, B. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst. Rev. 2020, 10, 1–23. [Google Scholar] [CrossRef]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual reality to augment robot-assisted gait training in non-ambulatory patients with a subacute stroke: A pilot randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 397–407. [Google Scholar] [CrossRef]
- Kayabinar, B.; Alemdaroğlu-Gürbüz, İ.; Yilmaz, Ö. The effects of virtual reality augmented robot-assisted gait training on dual-task performance and functional measures in chronic stroke: A randomized controlled single-blind trial. Eur. J. Phys. Rehabil. Med. 2021, 57, 227–237. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; De Luca, R.; Balletta, T.; Buda, A.; la Rosa, G.; Bramanti, A.; Bramanti, P. The role of virtual reality in improving motor performance as revealed by EEG: A randomized clinical trial. J. Neuroeng. Rehabil. 2017, 14, 53. [Google Scholar] [CrossRef]
- Winter, C.; Kern, F.; Gall, D.; Latoschik, M.E.; Pauli, P.; Käthner, I. Immersive virtual reality during gait rehabilitation increases walking speed and motivation: A usability evaluation with healthy participants and patients with multiple sclerosis and stroke. J. Neuroeng. Rehabil. 2021, 18, 68. [Google Scholar] [CrossRef]
- Cummings, J.J.; Bailenson, J.N. How Immersive Is Enough? A Meta-Analysis of the Effect of Immersive Technology on User Presence. Media Psychol. 2016, 19, 272–309. [Google Scholar] [CrossRef]
- Huygelier, H.; Mattheus, E.; Vanden Abeele, V.; Van Ee, R.; Gillebert, C.R. The Use of the Term Virtual Reality in Post-Stroke Rehabilitation: A Scoping Review and Commentary. Psychol. Belg. 2021, 61, 145. [Google Scholar] [CrossRef]
- Weiss, P.L.; Kizony, R.; Feintuch, U.; Katz, N. Virtual Reality in Neurorehabilitation. In Textbook of Neural Repair and Rehabilitation; Selzer, M., Clarke, S., Cohen, L., Duncan, P., Gage, F., Eds.; Cambridge University Press: Cambridge, UK, 2006; pp. 182–197. [Google Scholar] [CrossRef]
- Tieri, G.; Morone, G.; Paolucci, S.; Iosa, M. Virtual reality in cognitive and motor rehabilitation: Facts, fiction and fallacies. Expert Rev. Med. Devices 2018, 15, 107–117. [Google Scholar] [CrossRef]
- Slater, M.; Wilbur, S. A Framework for Immersive Virtual Environments (FIVE): Speculations on the Role of Presence in Virtual Environments. Presence Teleoperators Virtual Environ. 1997, 6, 603–616. [Google Scholar] [CrossRef]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [Green Version]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Dużmańska, N.; Strojny, P.; Strojny, A. Can Simulator Sickness Be Avoided? A Review on Temporal Aspects of Simulator Sickness. Front. Psychol. 2018, 9, 2132. [Google Scholar] [CrossRef]
- Caserman, P.; Garcia-Agundez, A.; Gámez Zerban, A.; Göbel, S. Cybersickness in current-generation virtual reality head-mounted displays: Systematic review and outlook. Virtual Real. 2021, 25, 1153–1170. [Google Scholar] [CrossRef]
- Gallagher, M.; Ferrè, E.R. Cybersickness: A Multisensory Integration Perspective. Multisens. Res. 2018, 31, 645–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saredakis, D.; Szpak, A.; Birckhead, B.; Keage, H.A.D.; Rizzo, A.; Loetscher, T. Factors Associated with Virtual Reality Sickness in Head-Mounted Displays: A Systematic Review and Meta-Analysis. Front. Hum. Neurosci. 2020, 14, 96. [Google Scholar] [CrossRef] [Green Version]
- Golding, J.F. Motion sickness susceptibility questionnaire revised and its relationship to other forms of sickness. Brain Res. Bull. 1998, 47, 507–516. [Google Scholar] [CrossRef]
- Weber, L.M.; Nilsen, D.M.; Gillen, G.; Yoon, J.; Stein, J. Immersive Virtual Reality Mirror Therapy for Upper Limb Recovery After Stroke: A Pilot Study. Am. J. Phys. Med. Rehabil. 2019, 98, 783–788. [Google Scholar] [CrossRef]
- Hesse, S.; Werner, C.; Uhlenbrock, D.; Frankenberg, S.V.; Bardeleben, A.; Brandl-Hesse, B. An Electromechanical Gait Trainer for Restoration of Gait in Hemiparetic Stroke Patients: Preliminary Results. Neurorehabil. Neural Repair. 2001, 15, 39–50. [Google Scholar] [CrossRef]
- Freivogel, S.; Schmalohr, D.; Mehrholz, J. Improved walking ability and reduced therapeutic stress with an electromechanical gait device. J. Rehabil. Med. 2009, 41, 734–739. [Google Scholar] [CrossRef] [Green Version]
- Lwowski, J.; Majumdar, A.; Benavidez, P.; Prevost, J.J.; Jamshidi, M. HTC Vive Tracker: Accuracy for Indoor Localization. IEEE Syst. Man Cybern. Mag. 2020, 6, 15–22. [Google Scholar] [CrossRef]
- Niehorster, D.C.; Li, L.; Lappe, M. The Accuracy and Precision of Position and Orientation Tracking in the HTC Vive Virtual Reality System for Scientific Research. i-Perception 2017, 8, 204166951770820. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Brooke, J. SUS: A retrospective. J. Usability Stud. 2013, 8, 29–40. [Google Scholar]
- Witmer, B.G.; Jerome, C.; Singer, M.J. The factor structure of the presence questionnaire. Presence Teleoperators Virtual Environ. 2005, 14, 298–312. [Google Scholar] [CrossRef]
- Bimberg, P.; Weissker, T.; Kulik, A. On the Usage of the Simulator Sickness Questionnaire for Virtual Reality Research. In Proceedings of the 2020 IEEE Conference on Virtual Reality and 3D User Interfaces Abstracts and Workshops (VRW), Atlanta, GA, USA, 22–26 March 2020; pp. 464–467. [Google Scholar] [CrossRef]
- Stanney, K.; Fidopiastis, C.; Foster, L. Virtual Reality Is Sexist: But It Does Not Have to Be. Front. Robot. AI 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruck, S.; Watters, P.A. The factor structure of cybersickness. Displays 2011, 32, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Hamzeheinejad, N.; Straka, S.; Gall, D.; Weilbach, F.; Erich Latoschik, M. Immersive Robot-Assisted Virtual Reality Therapy for Neurologically-Caused Gait Impairments. In Proceedings of the 2018 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Reutlingen, Germany, 18–22 March 2018; pp. 565–566. [Google Scholar] [CrossRef]
- Borrego, A.; Latorre, J.; Alcañiz, M.; Llorens, R. Comparison of Oculus Rift and HTC Vive: Feasibility for Virtual Reality-Based Exploration, Navigation, Exergaming, and Rehabilitation. Games Health J. 2018, 7, 151–156. [Google Scholar] [CrossRef]
- Borrego, A.; Latorre, J.; Alcañiz, M.; Llorens, R. Embodiment and Presence in Virtual Reality After Stroke. A Comparative Study with Healthy Subjects. Front. Neurol. 2019, 10, 1061. [Google Scholar] [CrossRef]
- Moyle, W.; Jones, C.; Dwan, T.; Petrovich, T. Effectiveness of a Virtual Reality Forest on People with Dementia: A Mixed Methods Pilot Study. Gerontologist 2018, 58, 478–487. [Google Scholar] [CrossRef] [Green Version]
- Appel, L.; Appel, E.; Bogler, O.; Wiseman, M.; Cohen, L.; Ein, N.; Abrams, H.B.; Campos, J.L. Older Adults with Cognitive and/or Physical Impairments Can Benefit from Immersive Virtual Reality Experiences: A Feasibility Study. Front. Med. 2020, 6, 329. [Google Scholar] [CrossRef] [Green Version]
- Deblock-Bellamy, A.; Lamontagne, A.; McFadyen, B.J.; Ouellet, M.C.; Blanchette, A.K. Dual-Task Abilities During Activities Representative of Daily Life in Community-Dwelling Stroke Survivors: A Pilot Study. Front. Neurol. 2022, 13, 855226. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| SSQ > 5 | SSQ > 10 | SSQ > 15 | |
|---|---|---|---|
| Individual Characteristics | |||
| n (M/F) | 8 (3/5) | 7 (2/5) | 3 (0/3) |
| Age (mean ± sd) | 23.88 ± 3.87 | 24.14 ± 4.10 | 22 ± 1.73 |
| MSSQ (mean ± sd) | 14.63 ± 8.50 | 14.61 ± 9.18 | 17.25 ± 7.12 |
| Occurrence of adverse effects (Session 1/Session 2) | |||
| Eyestrain (n) | 5 (62.5%)/3 (37.5%) | 4 (57.14%)/2 (28.57%) | 2 (66%)/0 |
| Fullness of head (n) | 3 (37.5%)/1 (12.5%) | 3 (42.86)/1 (14.28%) | 3 (100%)/1 (33%) |
| Headache (n) | 3 (37.5%)/3 (37.5%) | 3 (42.86)/2 (28.57%) | 2 (66%)/0 |
| Nausea (n) | 3 (37.5%)/2 (25%) | 3 (42.86)/2 (28.57%) | 2 (66%)/1 (33%) |
| Vertigo (n) | 3 (37.5%)/1 (12.5%) | 3 (42.86)/1 (14.28%) | 2 (66%)/0 |
| Difficulty focusing (n) | 2 (25%)/2 (25%) | 2 (28.57%)/2 (28.57%) | 2 (66%)/0 |
| SSQ Total | Pre-session | Post-session | p-value |
| Session 1 | 1.31 ± 2.53 | 3.33 ± 6.98 | 0.203 |
| Session 2 | 0.80 ± 2.00 | 2.32 ± 5.53 | 0.032 * |
| Parameters | Session 1 | Session 2 | p-Value |
|---|---|---|---|
| PQ | 104.11 ± 9.37 | 108.73 ± 9.10 | <0.001 |
| SUS | 86.08 ± 7.54 | / | |
| nGT (n) | 704.03 ± 3.09 | 703.32 ± 2.33 | / |
| nVR (n) | 728.03 ± 49.26 * | 727.24 ± 39.83 * | / |
| Distance in GT (meter) | 675.87 ± 2.96 | 675.19 ± 2.24 | / |
| Distance in VR (meter) | 699.03 ± 47.32 * | 698.03 ± 38.27 * | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morizio, C.; Compagnat, M.; Boujut, A.; Labbani-Igbida, O.; Billot, M.; Perrochon, A. Immersive Virtual Reality during Robot-Assisted Gait Training: Validation of a New Device in Stroke Rehabilitation. Medicina 2022, 58, 1805. https://doi.org/10.3390/medicina58121805
Morizio C, Compagnat M, Boujut A, Labbani-Igbida O, Billot M, Perrochon A. Immersive Virtual Reality during Robot-Assisted Gait Training: Validation of a New Device in Stroke Rehabilitation. Medicina. 2022; 58(12):1805. https://doi.org/10.3390/medicina58121805
Chicago/Turabian StyleMorizio, Charles, Maxence Compagnat, Arnaud Boujut, Ouiddad Labbani-Igbida, Maxime Billot, and Anaick Perrochon. 2022. "Immersive Virtual Reality during Robot-Assisted Gait Training: Validation of a New Device in Stroke Rehabilitation" Medicina 58, no. 12: 1805. https://doi.org/10.3390/medicina58121805