
A Submucosal Tumor-like Lesion of the Cervical Esophagus Similar to the Tonsillar Structures of Waldeyer’s Ring: A Case Report

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
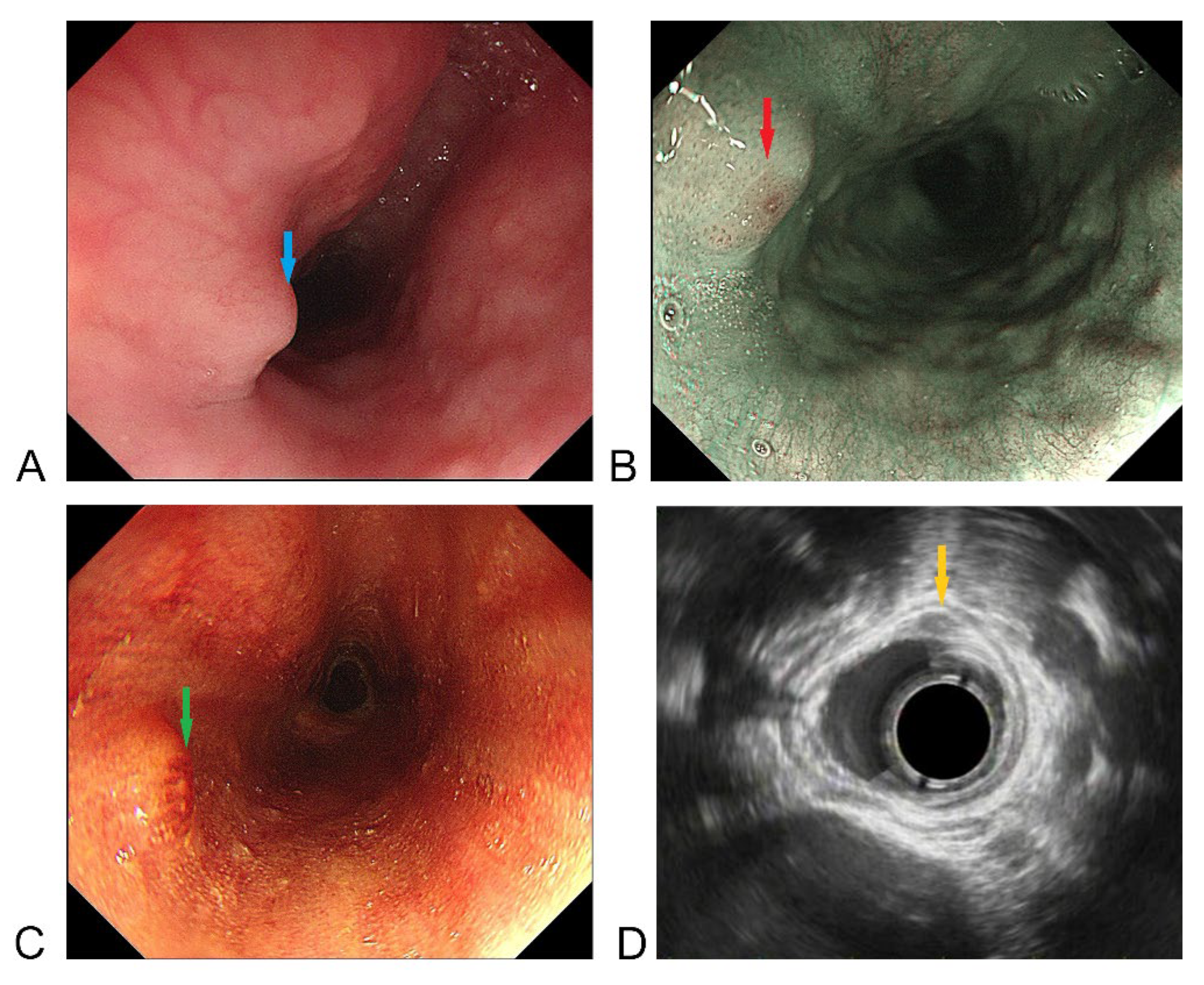
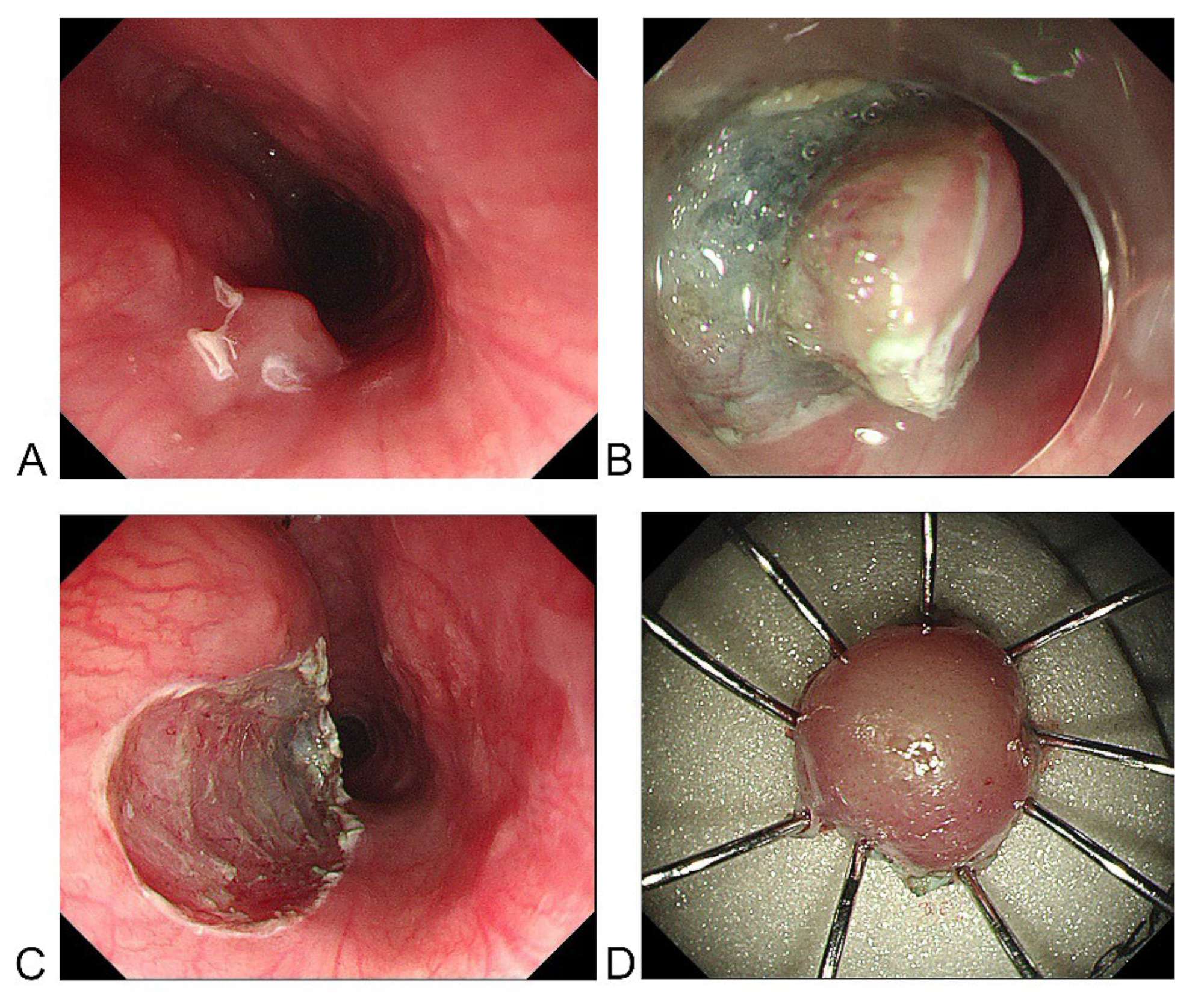
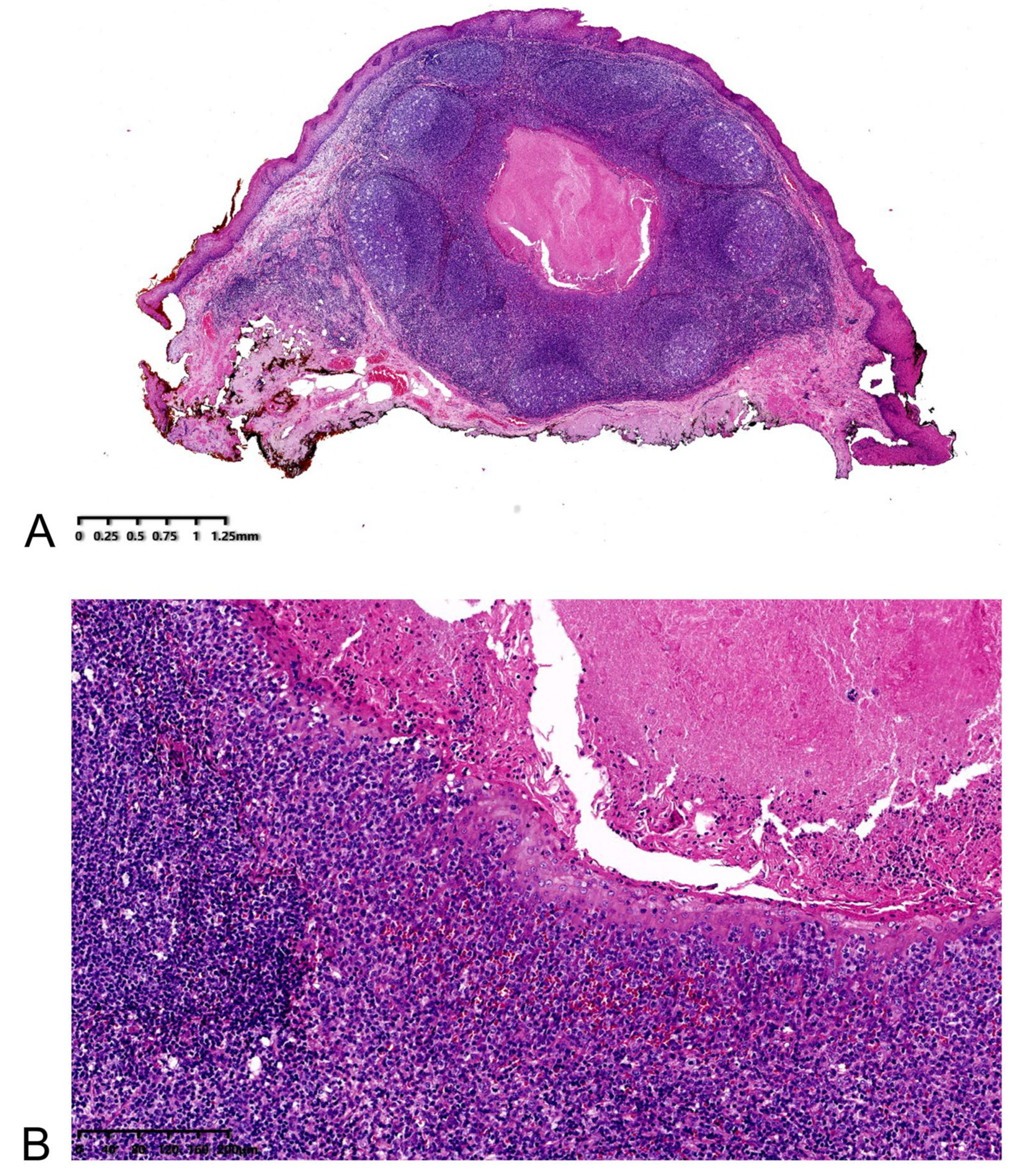
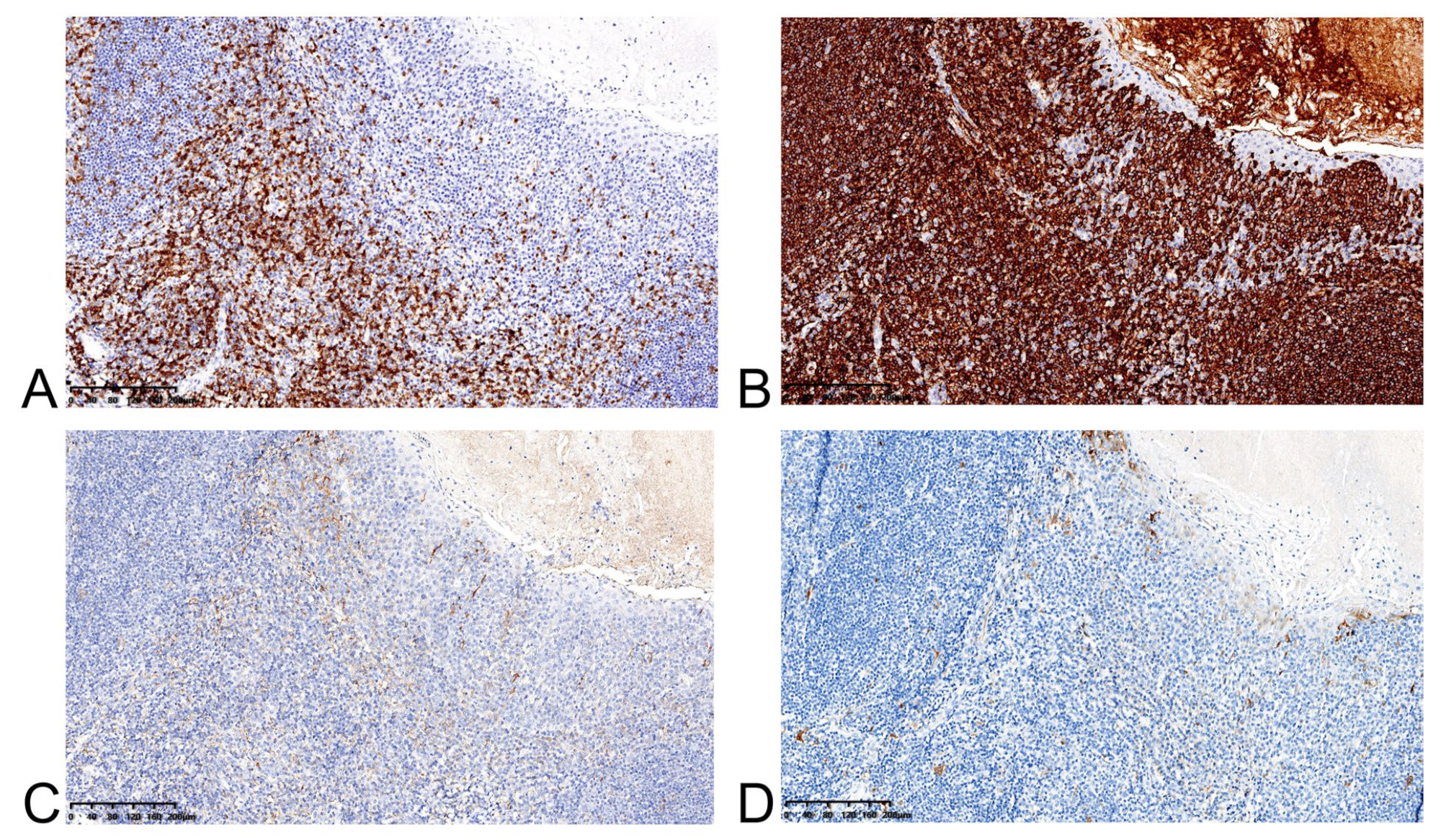
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Submucosal tumors | SMTs |
| Waldeyer’s ring | WR |
| Mucosa associated lymphoid tissue | MALT |
| Primary Waldeyer’s ring lymphoma | PWRL |
| non-Hodgkin lymphoma | NHL |
| Endoscopic ultrasonography | EUS |
| Endoscopic submucosal dissection | ESD |
References
- Ko, W.J.; Song, G.W.; Cho, J.Y. Evaluation and Endoscopic Management of Esophageal Submucosal Tumor. Clin. Endosc. 2017, 50, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, A.A.; Ibrahim, E.M.; El Weshi, A.N.; Khafaga, Y.M.; AlJurf, M.; Martin, J.M.; Ajarim, D.S.; Bazarbashi, S.N.; Stuart, R.K.; Zucca, E. Localized non-Hodgkin’s lymphoma of Waldeyer’s ring: Clinical features, management, and prognosis of 130 adult patients. Head Neck 2001, 23, 547–558. [Google Scholar] [CrossRef] [PubMed]
- Laskar, S.; Mohindra, P.; Gupta, S.; Shet, T.; Muckaden, M.A. Non-Hodgkin lymphoma of the Waldeyer’s ring: Clinicopathologic and therapeutic issues. Leuk. Lymphoma 2008, 49, 2263–2271. [Google Scholar] [CrossRef] [PubMed]
- Emory, T.S.; Sobin, L.H.; Lukes, L.; Lee, D.H.; O’Leary, T.J. Prognosis of gastrointestinal smooth-muscle (stromal) tumors: Dependence on anatomic site. Am. J. Surg. Pathol. 1999, 23, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Karch, H.W.; Gockel, I.; Goetz, M.; Kreft, A.; Lang, H. Granular-cell tumor (Abrikossoff’s tumor): Precise preoperative diagnosis is crucial when for minimally-invasive resection. Dtsch. Med. Wochenschr. 2011, 136, 1609–1612. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Zhou, X.; Xu, K.; Huang, Q. Esophageal lymphangioma: A case report and review of literature. BMC Gastroenterol. 2019, 19, 107. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Zhang, C.; Fang, S.; Zhong, P.; Zhu, X.; Lin, L.; Xiao, H. Primary esophageal mucosa-associated lymphoid tissue lymphoma: A case report and review of literature. Medicine 2017, 96, e6478. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.; Fei, D.; Jianguo, S.; Changping, W.; Juan, D.; Yin, Z.; Liwen, Z.; Jianping, C. Endoscopic submucosal dissection of coexisting early esophageal carcinoma and leiomyoma: A case report and review of the literature. J. Int. Med. Res. 2020, 48, 300060520961246. [Google Scholar] [CrossRef] [PubMed]
- Landi, B.; Palazzo, L. The role of endosonography in submucosal tumours. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 679–701. [Google Scholar] [CrossRef] [PubMed]
- Faulx, A.L.; Kothari, S.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Chandrasekhara, V.; Eloubeidi, M.A.; Fanelli, R.D.; Gurudu, S.R.; Khashab, M.A.; et al. The role of endoscopy in subepithelial lesions of the GI tract. Gastrointest. Endosc. 2017, 85, 1117–1132. [Google Scholar] [CrossRef] [PubMed]
- Aoki, T.; Nakamura, T.; Oshikiri, T.; Hasegawa, H.; Yamamoto, M.; Matsuda, Y.; Kanaji, S.; Yamashita, K.; Matsuda, T.; Sumi, Y.; et al. Strategy for esophageal non-epithelial tumors based on a retrospective analysis of a single facility. Esophagus Off. J. Jpn. Esophageal Soc. 2018, 15, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Quiñones-Avila Mdel, P.; Gonzalez-Longoria, A.A.; Admirand, J.H.; Medeiros, L.J. Hodgkin lymphoma involving Waldeyer ring: A clinicopathologic study of 22 cases. Am. J. Clin. Pathol. 2005, 123, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Rozwod, K.; Mauz-Körholz, C.; Heine, P.; Gattenlöhner, S.; Langer, C.; Steiner, D.; Krombach, G.; Georgi, T.W.; Kallenberg, K.; Sabri, O.; et al. Waldeyer’s ring involvement in a young patient with Hodgkin lymphoma: Challenges, interdisciplinary findings, and reliability check of the image-based algorithm for diagnosis and response assessment. Pediatric Blood Cancer 2022, 69, e29560. [Google Scholar] [CrossRef] [PubMed]
- He, G.; Wang, J.; Chen, B.; Xing, X.; Wang, J.; Chen, J.; He, Y.; Cui, Y.; Chen, M. Feasibility of endoscopic submucosal dissection for upper gastrointestinal submucosal tumors treatment and value of endoscopic ultrasonography in pre-operation assess and post-operation follow-up: A prospective study of 224 cases in a single medical center. Surg. Endosc. 2016, 30, 4206–4213. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, S.; Feng, X.; Liu, X.; Wang, G.; Xue, L. A Submucosal Tumor-like Lesion of the Cervical Esophagus Similar to the Tonsillar Structures of Waldeyer’s Ring: A Case Report. Medicina 2022, 58, 1804. https://doi.org/10.3390/medicina58121804
Song S, Feng X, Liu X, Wang G, Xue L. A Submucosal Tumor-like Lesion of the Cervical Esophagus Similar to the Tonsillar Structures of Waldeyer’s Ring: A Case Report. Medicina. 2022; 58(12):1804. https://doi.org/10.3390/medicina58121804
Chicago/Turabian StyleSong, Shibo, Xiaolong Feng, Xudong Liu, Guiqi Wang, and Liyan Xue. 2022. "A Submucosal Tumor-like Lesion of the Cervical Esophagus Similar to the Tonsillar Structures of Waldeyer’s Ring: A Case Report" Medicina 58, no. 12: 1804. https://doi.org/10.3390/medicina58121804