
The Impact of Patient-Specific Positions on the Relationship between Iliac Blood Vessels and Lumbar Intervertebral Discs: Anatomical Significance and Clinical Implications

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
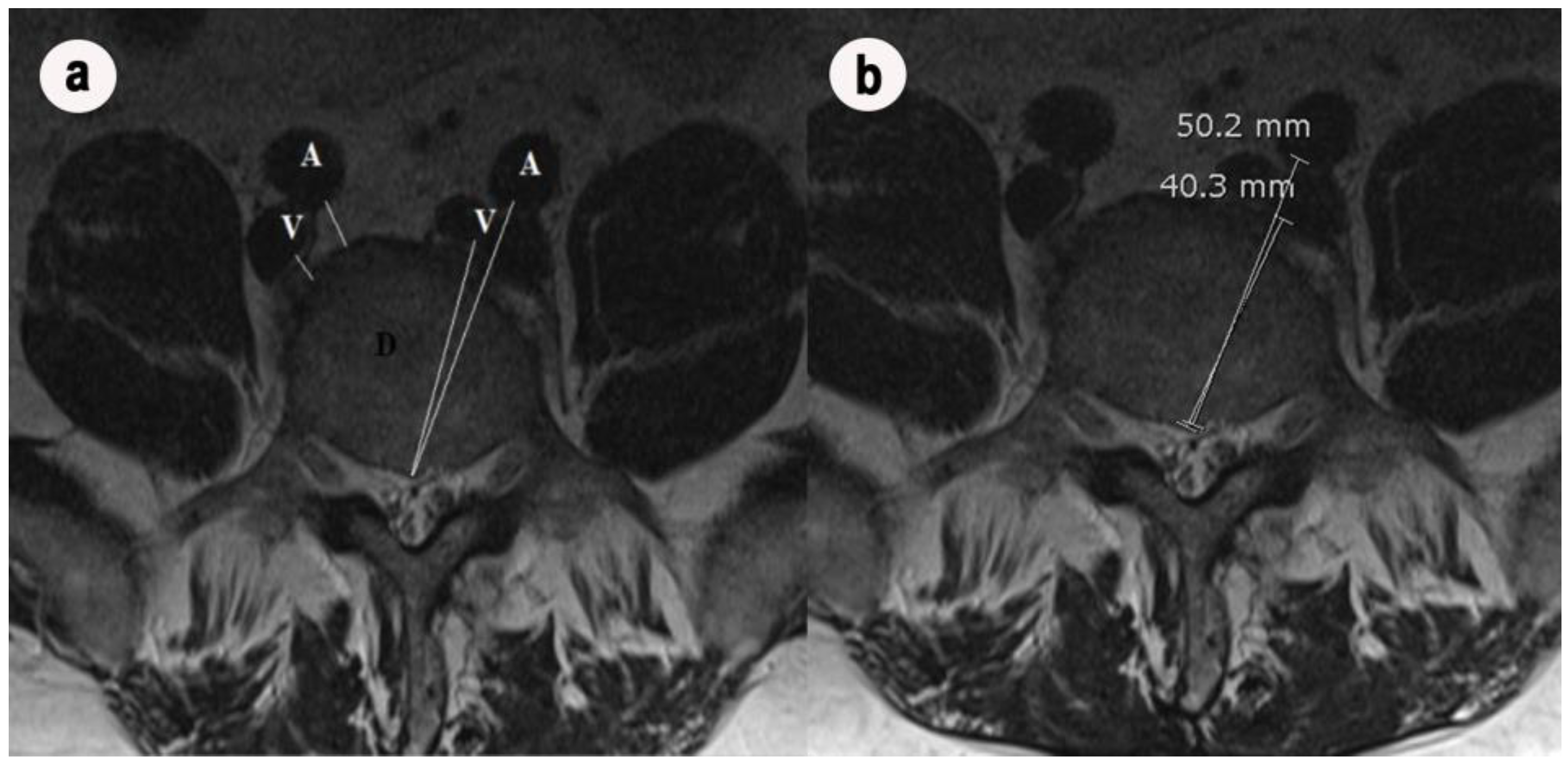
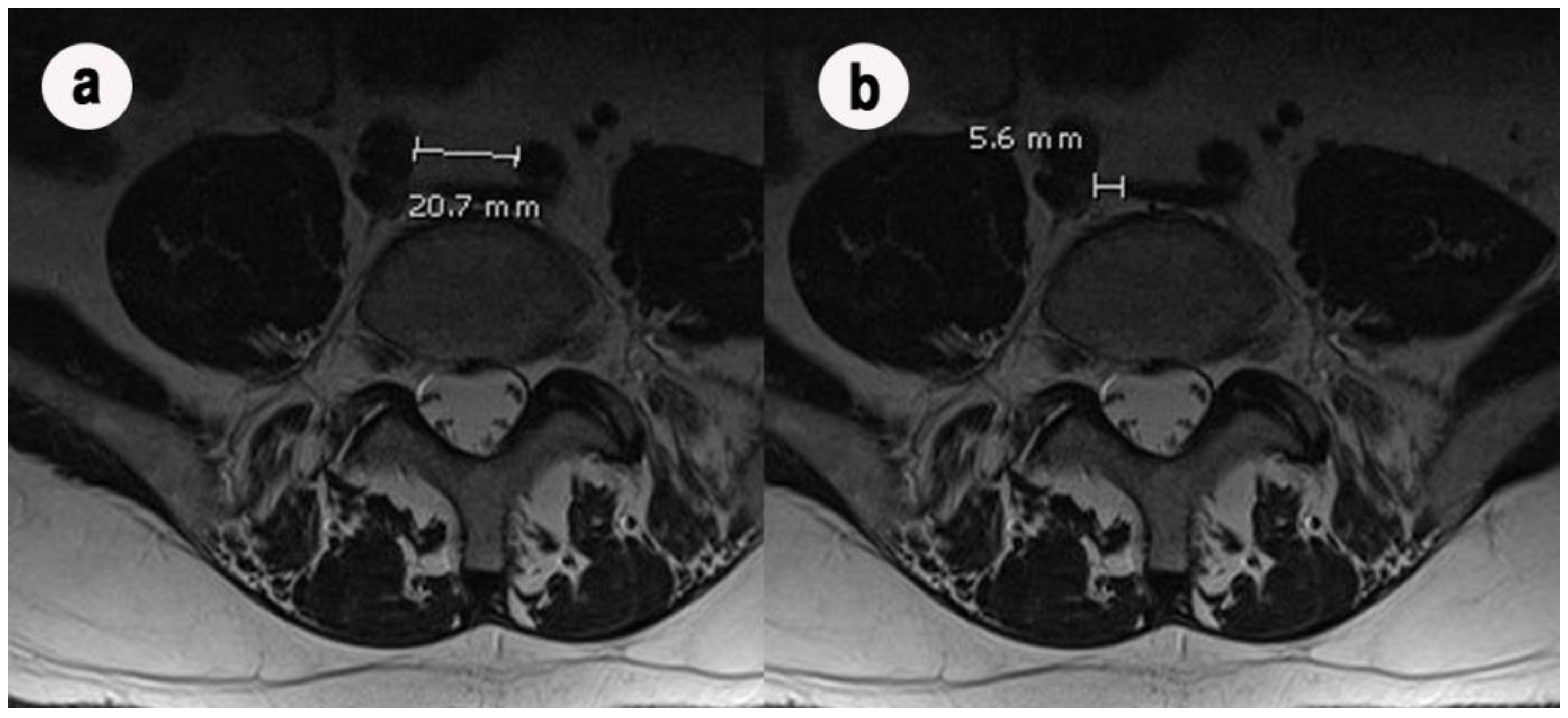
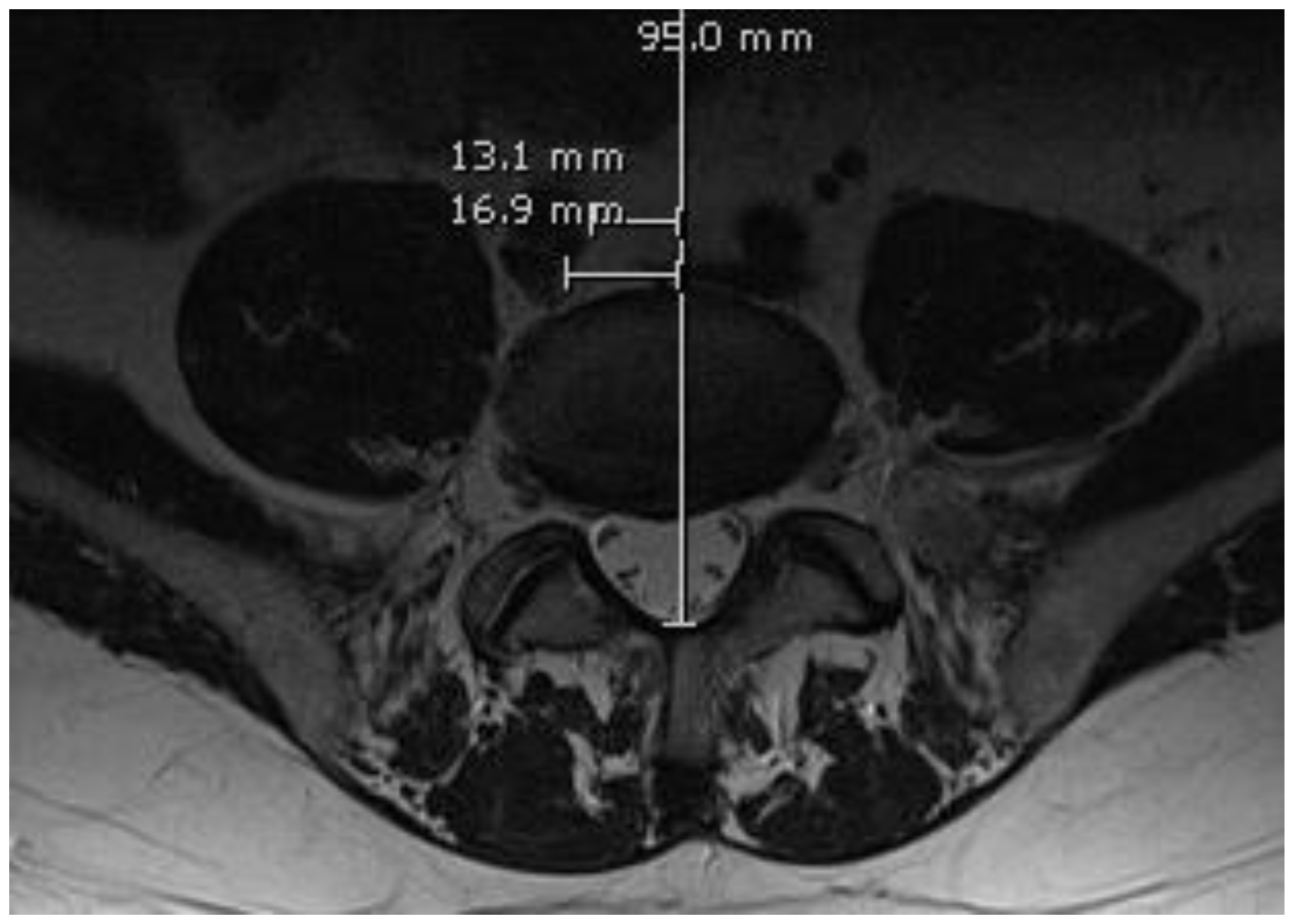
2.2. Methods
2.3. Statistical Analysis
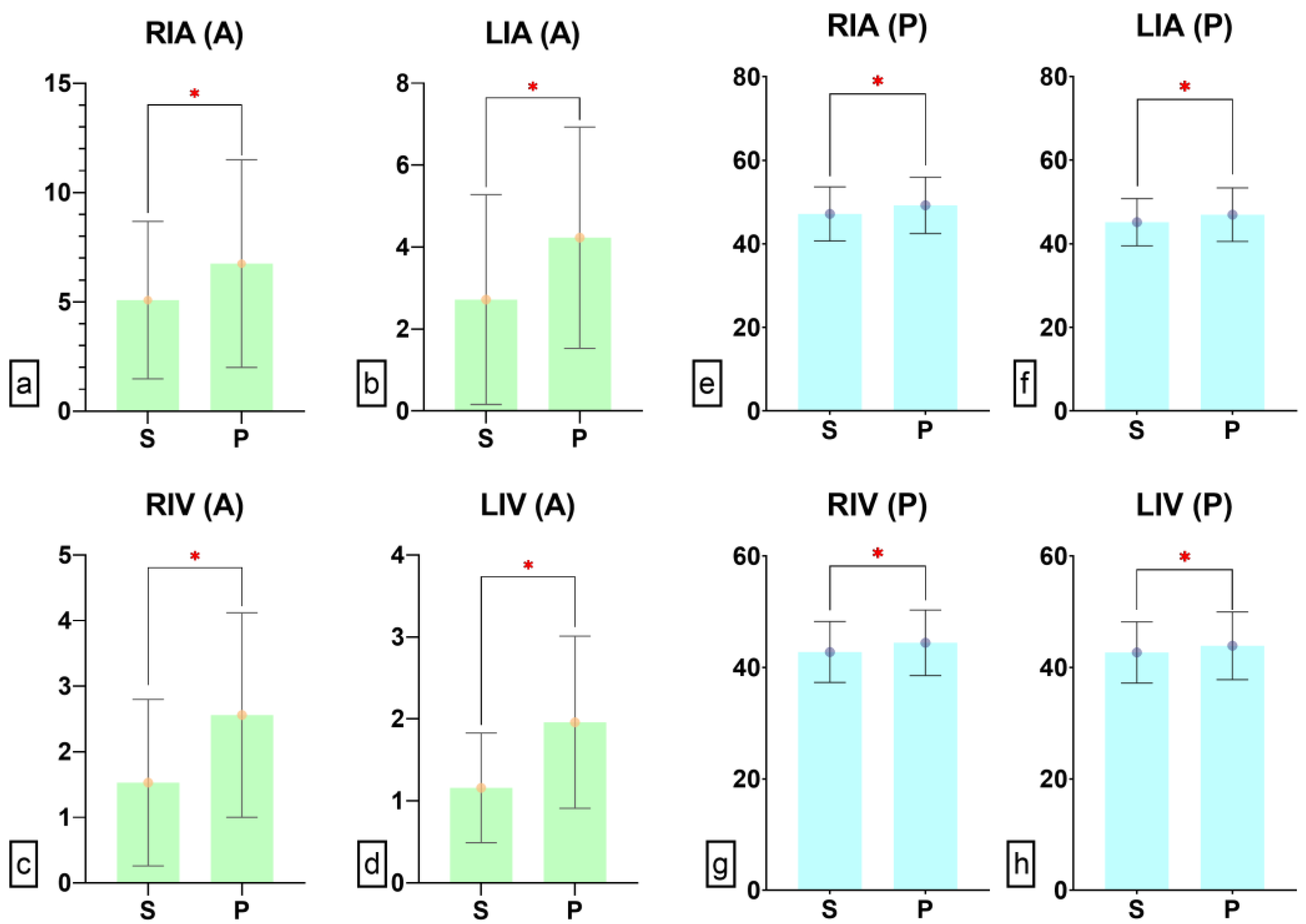
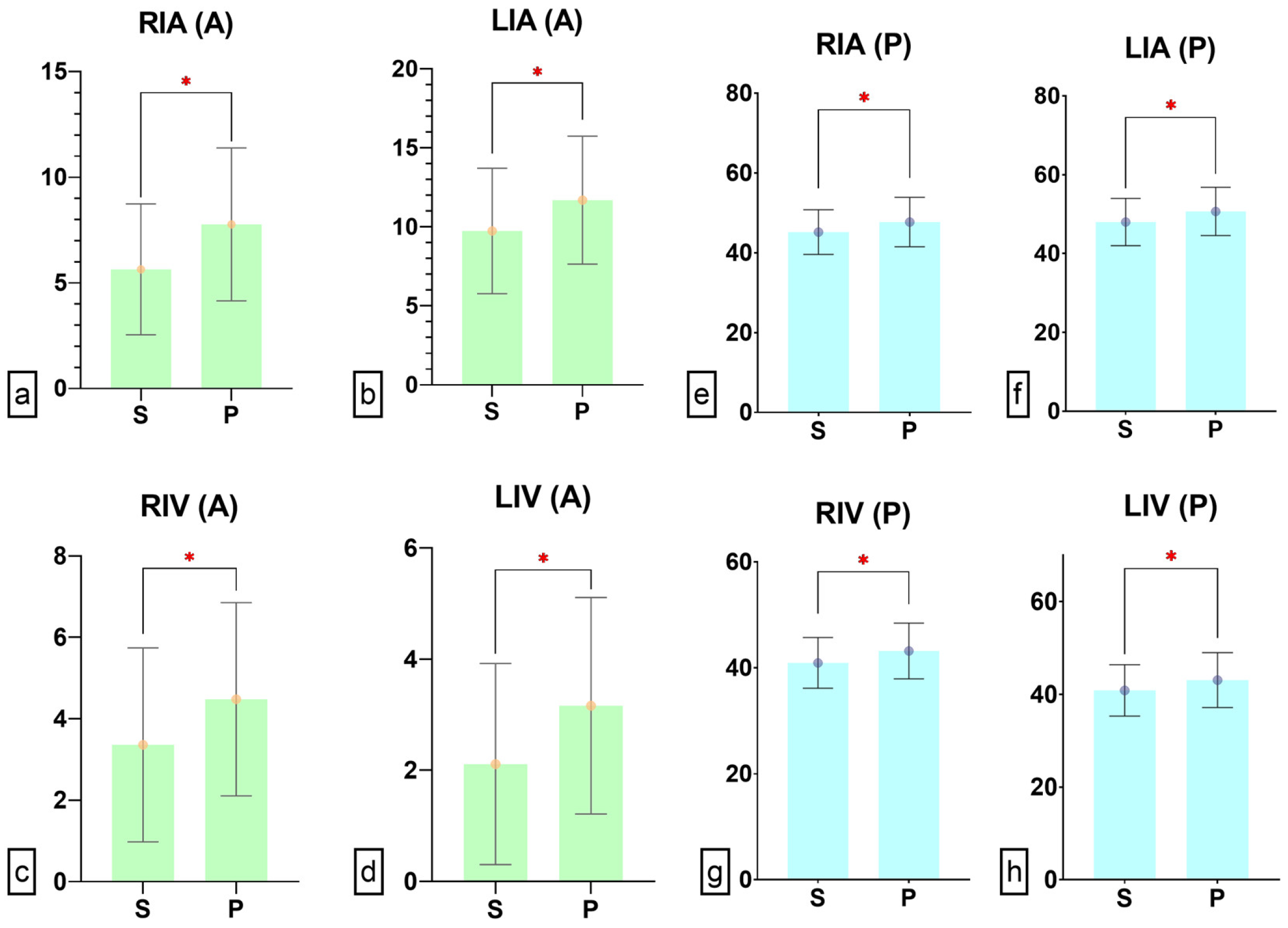
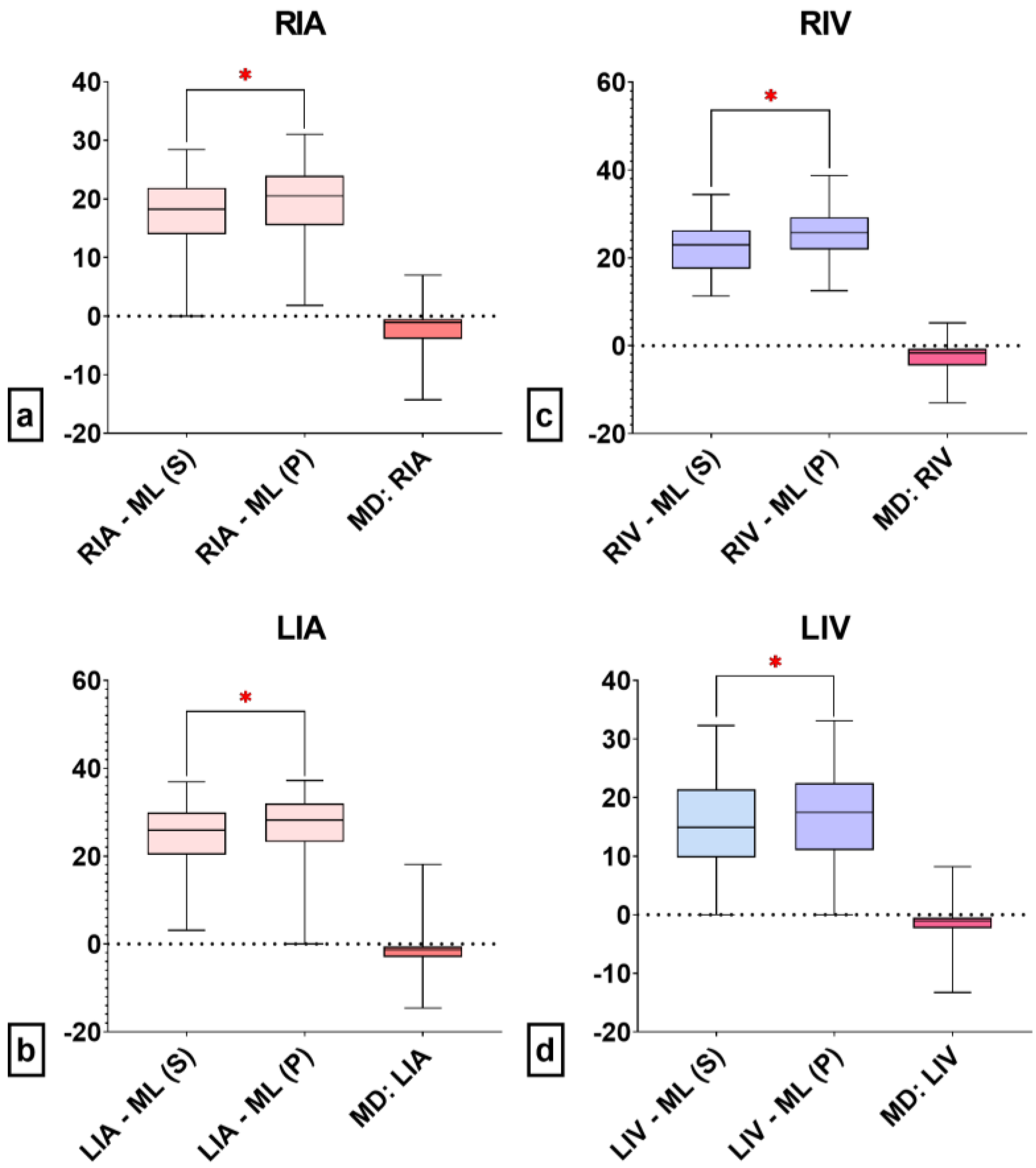
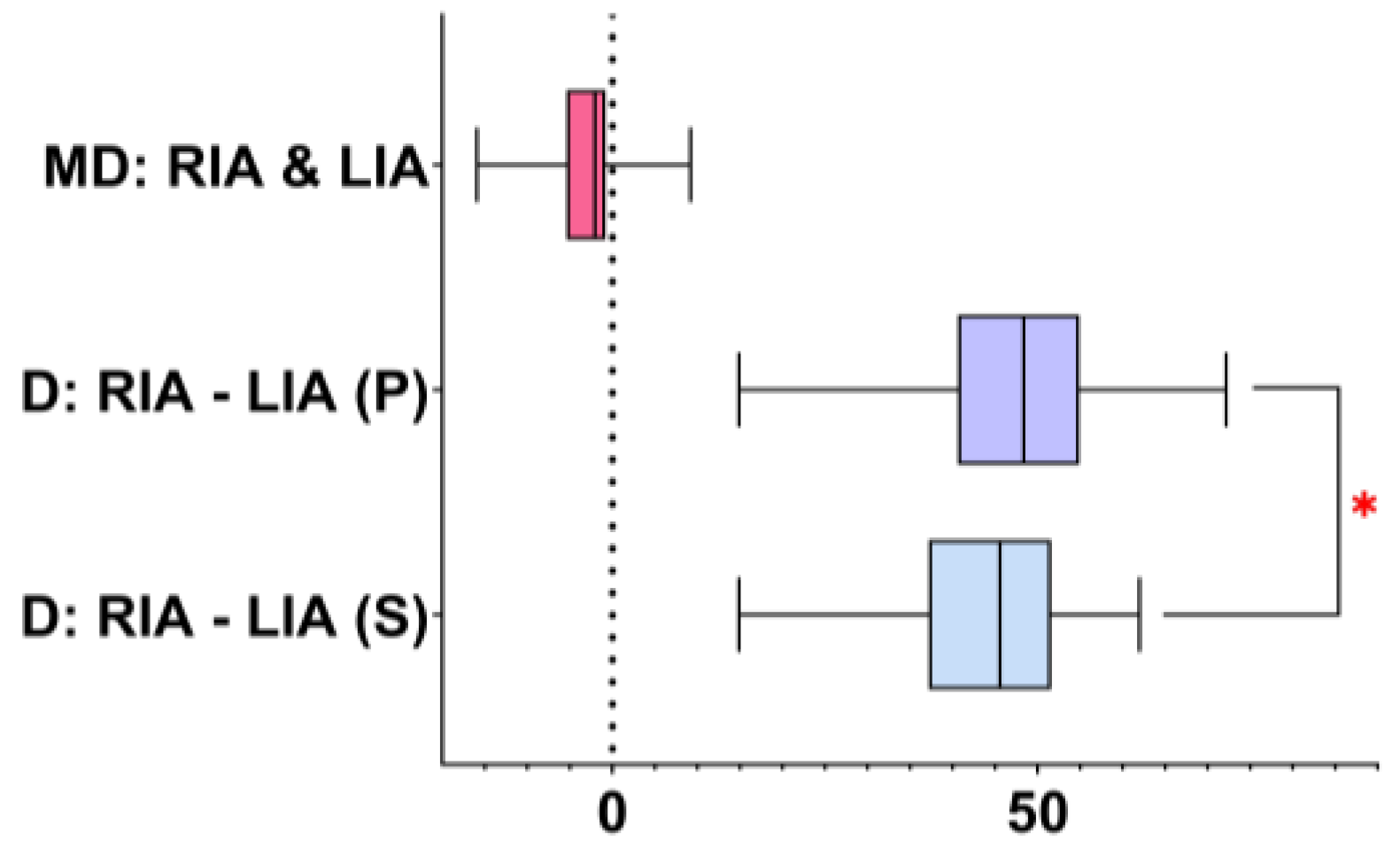
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bečulić, H. Degenerativne Bolesti Slabinske Kičme [Degenerative Diseases of Lumbar Spine]; Agfa Print: Zenica, Bosnia and Herzegovina, 2022; Available online: https://www.researchgate.net/publication/364112270_Degenerativne_bolesti_slabinske_kicme (accessed on 4 January 2024).
- Kot, A.; Polak, J.; Klepinowski, T.; Frączek, M.J.; Krzyżewski, R.M.; Grochowska, A.; Popiela, T.J.; Kwinta, B.M. Morphometric analysis of the lumbar vertebrae and intervertebral discs in relation to abdominal aorta: CT-based study. Surg. Radiol. Anat. 2022, 44, 431–441. [Google Scholar] [CrossRef]
- Hussain, S.; Mubeen, I.; Ullah, N.; Shah, S.; Khan, B.A.; Zahoor, M.; Ullah, R.; Khan, F.A.; Sultan, M.A. Modern Diagnostic Imaging Technique Applications and Risk Factors in the Medical Field: A Review. Biomed. Res. Int. 2022, 2022, 5164970. [Google Scholar] [CrossRef] [PubMed]
- Regev, G.J.; Chen, L.; Dhawan, M.; Lee, Y.P.; Garfin, S.R.; Kim, C.W. Morphometric analysis of the ventral nerve roots and retroperitoneal vessels with respect to the minimally invasive lateral approach in normal and deformed spines. Spine 2009, 34, 1330–1335. [Google Scholar] [CrossRef] [PubMed]
- Begagić, E.; Bečulić, H.; Skomorac, R.; Pojskić, M. Accessible Spinal Surgery: Transformation Through the Implementation of Exoscopes As Substitutes for Conventional Microsurgery in Low- and Middle-Income Settings. Cureus 2023, 15, e45350. [Google Scholar] [CrossRef] [PubMed]
- Waxenbaum, J.A.; Reddy, V.; Williams, C.; Futterman, B. Anatomy, Back, Lumbar Vertebrae; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Sassack, B.; Carrier, J.D. Anatomy, Back, Lumbar Spine; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Bečulić, H.; Begagić, E.; Skomorac, R.; Jusić, A.; Efendić, A.; Selimović, E.; Mašović, A.; Bečulić, L. A correlation of demographic characteristics, preoperative conservative therapy and timing with postoperative outcome in herniated disc-associated cauda equina syndrome: Do they really matter? Med. Glas. 2023, 20, 269–275. [Google Scholar] [CrossRef]
- DeSai, C.; Reddy, V.; Agarwal, A. Anatomy, Back, Vertebral Column; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Skomorac, R.; Delić, J.; Bečulić, H.; Jusić, A. Radiological evaluation of lumbosacral spine for post discectomy segmental instability. Med. Glas. 2016, 13, 142–147. [Google Scholar] [CrossRef]
- Skomorac, R.; Delić, J.; Jusić, A.; Beculić, H.; Bajtarević, A.; Hadzić, E. Morphometric changes of the lumbar intervertebral space following discectomy on one or two levels. Med. Glas. 2011, 8, 249–254. [Google Scholar]
- Zierle-Ghosh, A.; Jan, A. Physiology, Body Mass Index; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Skippage, P.; Raja, J.; McFarland, R.; Belli, A.M. Endovascular repair of iliac artery injury complicating lumbar disc surgery. Eur. Spine J. 2008, 17 (Suppl. 2), S228–S231. [Google Scholar] [CrossRef]
- Khamanarong, K.; Sae-Jung, S.; Supa-Adirek, C.; Teerakul, S.; Prachaney, P. Aortic bifurcation: A cadaveric study of its relationship to the spine. J. Med. Assoc. Thai 2009, 92, 47–49. [Google Scholar]
- Appaji, A.C.; Kulkarni, R.; Pai, S.B. Level of Bifurcation of Aorta and Iliocaval Confluence and Its Clinical Relevance. IOSR J. Dent. Med. Sci. 2014, 13, 56–60. [Google Scholar] [CrossRef]
- Deswal, A.; Tamang, B.K.; Bala, A. Study of aortic- common iliac bifurcation and its clinical significance. J. Clin. Diagn. Res. 2014, 8, Ac06–Ac08. [Google Scholar] [CrossRef] [PubMed]
- Chithriki, M.; Jaibaji, M.; Steele, R.D. The anatomical relationship of the aortic bifurcation to the lumbar vertebrae: A MRI study. Surg. Radiol. Anat. 2002, 24, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, A.R.; Kepler, C.K.; Rihn, J.A.; Suzuki, H.; Ratliff, J.K.; Harrop, J.S.; Morrison, W.B.; Limthongkul, W.; Albert, T.J. Anatomical relationships of the anterior blood vessels to the lower lumbar intervertebral discs: Analysis based on magnetic resonance imaging of patients in the prone position. J. Bone Jt. Surg. Am. 2012, 94, 1088–1094. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.D.; Barbosa, T.P.; Correia, G.; Silva, R.; Cruz Oliveira, N.; Varanda, P.; Direito-Santos, B. The ideal patient positioning in spine surgery: A preventive strategy. EFORT Open Rev. 2023, 8, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Garg, B.; Bansal, T.; Mehta, N.; Sharan, A.D. Patient Positioning in Spine Surgery: What Spine Surgeons Should Know? Asian Spine J. 2023, 17, 770–781. [Google Scholar] [CrossRef] [PubMed]
- Erkut, B.; Unlü, Y.; Kaygin, M.A.; Colak, A.; Erdem, A.F. Iatrogenic vascular injury during to lumbar disc surgery. Acta Neurochir. 2007, 149, 511–515; discussion 516. [Google Scholar] [CrossRef] [PubMed]
- Bečulić, H.; Sladojević, I.; Jusić, A.; Skomorac, R.; Imamović, M.; Efendić, A. Morphometric study of the anatomic relationship between large retroperitoneal blood vessels and intervertebral discs of the distal segment of the lumbar spine: A clinical significance. Med. Glas. 2019, 16, 1011–1019. [Google Scholar] [CrossRef]
- Behzadi, A.H.; Khilnani, N.M.; Zhang, W.; Bares, A.J.; Boddu, S.R.; Min, R.J.; Prince, M.R. Pelvic cardiovascular magnetic resonance venography: Venous changes with patient position and hydration status. J. Cardiovasc. Magn. Reson. 2019, 21, 3. [Google Scholar] [CrossRef]
- Kim, J.T.; Lee, N.J.; Na, H.S.; Jeon, Y.; Kim, H.S.; Kim, C.S.; Kim, S.D. Ultrasonographic investigation of the effect of inguinal compression on the cross-sectional area of the femoral vein. Acad. Emerg. Med. 2008, 15, 101–103. [Google Scholar] [CrossRef]
- Stone, M.B.; Price, D.D.; Anderson, B.S. Ultrasonographic investigation of the effect of reverse Trendelenburg on the cross-sectional area of the femoral vein. J. Emerg. Med. 2006, 30, 211–213. [Google Scholar] [CrossRef]
- Fronek, A.; Criqui, M.H.; Denenberg, J.; Langer, R.D. Common femoral vein dimensions and hemodynamics including Valsalva response as a function of sex, age, and ethnicity in a population study. J. Vasc. Surg. 2001, 33, 1050–1056. [Google Scholar] [CrossRef]
- Coxwell Matthewman, M.; Yanase, F.; Costa-Pinto, R.; Jones, D.; Karalapillai, D.; Modra, L.; Radford, S.; Ukor, I.F.; Warrillow, S.; Bellomo, R. Haemodynamic changes during prone versus supine position in patients with COVID-19 acute respiratory distress syndrome. Aust. Crit. Care 2023, in press. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef]
- Weiss, T.T.; Cerda, F.; Scott, J.B.; Kaur, R.; Sungurlu, S.; Mirza, S.H.; Alolaiwat, A.A.; Kaur, R.; Augustynovich, A.E.; Li, J. Prone positioning for patients intubated for severe acute respiratory distress syndrome (ARDS) secondary to COVID-19: A retrospective observational cohort study. Br. J. Anaesth. 2021, 126, 48–55. [Google Scholar] [CrossRef]
- Nair, M.N.; Ramakrishna, R.; Slimp, J.; Kinney, G.; Chesnut, R.M. Left iliac artery injury during anterior lumbar spine surgery diagnosed by intraoperative neurophysiological monitoring. Eur. Spine J. 2010, 19 (Suppl. 2), S203–S205. [Google Scholar] [CrossRef] [PubMed]
- Reilly, E.; Weger, N.; Stawicki, S. Vascular injury during spinal surgery. Int. J. Acad. Med. 2017, 3 (Suppl. 1), S39–S43. [Google Scholar] [CrossRef]
- Goodkin, R.; Laska, L.L. Vascular and visceral injuries associated with lumbar disc surgery: Medicolegal implications. Surg. Neurol. 1998, 49, 358–370; discussion 370–372. [Google Scholar] [CrossRef] [PubMed]
- Sadhasivam, S.; Kaynar, A.M. Iatrogenic arteriovenous fistula during lumbar microdiscectomy. Anesth. Analg. 2004, 99, 1815–1817. [Google Scholar] [CrossRef] [PubMed]
- Papadoulas, S.; Konstantinou, D.; Kourea, H.P.; Kritikos, N.; Haftouras, N.; Tsolakis, J.A. Vascular injury complicating lumbar disc surgery. A systematic review. Eur. J. Vasc. Endovasc. Surg. 2002, 24, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.P.; Hseu, S.S.; Sung, C.S.; Cheng, H.C.; Yien, H.W. Abdominal vascular injury during lumbar disc surgery. Zhonghua Yi Xue Za Zhi 2001, 64, 649–654. [Google Scholar] [PubMed]
- Quigley, T.M.; Stoney, R.J. Arteriovenous fistulas following lumbar laminectomy: The anatomy defined. J. Vasc. Surg. 1985, 2, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Antar, V.; Baran, O.; Kelten, B.; Atci, I.B.; Yilmaz, H.; Katar, S.; Yilmaz, A. Morphometric Analysis of Lumbar Disc Space in the Turkish Population and Safe Discectomy Distance in Lumbar Disc Surgery. Turk. Neurosurg. 2017, 27, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Jaganjac, B.; Džidić-Krivić, A.; Bečulić, H.; Šljivo, A.; Begagić, E.; Šišić, A. Magnetic resonance morphometry of the lumbar spinal canal in Zenica—Doboj Canton in Bosnia and Herzegovina. Med. Glas. 2023, 20, 263–268. [Google Scholar] [CrossRef]
- Ganesan, C.; Petrus, L.; Ross, I.B. Regarding the possibility of anterior vascular injury from the posterior approach to the lumbar disc space: An anatomical study. Spine 2012, 37, E1371–E1375. [Google Scholar] [CrossRef] [PubMed]
- Marchi, L.; Pimenta, L.; Oliveira, L.; Fortti, F.; Amaral, R.; Abdala, N. Distance between Great Vessels and the Lumbar Spine: MRI Study for Anterior Longitudinal Ligament Release Through a Lateral Approach. J. Neurol. Surg. Cent. Eur. Neurosurg. 2017, 78, 144–153. [Google Scholar] [CrossRef]
- Wildförster, U. Intraoperative complications in lumbar intervertebral disk operations. Cooperative study of the spinal study group of the German Society of Neurosurgery. Neurochirurgia 1991, 34, 53–56. [Google Scholar] [CrossRef]
- Döşoğlu, M.; Iş, M.; Pehlivan, M.; Yildiz, K.H. Nightmare of lumbar disc surgery: Iliac artery injury. Clin. Neurol. Neurosurg. 2006, 108, 174–177. [Google Scholar] [CrossRef]
- Turgut, M.; Akhaddar, A.; Turgut, A.T.; Hall, W.A. Iatrogenic Vascular Injury Associated with Cervical Spine Surgery: A Systematic Literature Review. World Neurosurg. 2022, 159, 83–106. [Google Scholar] [CrossRef]
- Holscher, E.C. Vascular and visceral injuries during lumbar-disc surgery. J. Bone Joint Surg. Am. 1968, 50, 383–393. [Google Scholar] [CrossRef]
- Nekhlopochyn, O.S.; Pylypenko, M.M.; Dubrov, S.O. Vascular injury during lumbar discectomy: Risk factors, diagnosis, methods of surgical correction, features of anaesthetic management and intensive care. Ukr. Neurosurg. J. 2023, 29, 3–18. [Google Scholar] [CrossRef]
- Keskin, M.; Serin, K.R.; Genc, F.A.; Aksoy, M.; Yanar, F.; Kurtoglu, M. Iatrogenic major vascular injury during lumbar discectomy: Report of three cases. Turk. Neurosurg. 2013, 23, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Anda, S.; Aakhus, S.; Skaanes, K.O.; Sande, E.; Schrader, H. Anterior perforations in lumbar discectomies. A report of four cases of vascular complications and a CT study of the prevertebral lumbar anatomy. Spine 1991, 16, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Sağdiç, K.; Ozer, Z.G.; Senkaya, I.; Türe, M. Vascular injury during lumbar disc surgery. Report of two cases; a review of the literature. Vasa 1996, 25, 378–381. [Google Scholar]
- Mirza, A.K.; Alvi, M.A.; Naylor, R.M.; Kerezoudis, P.; Krauss, W.E.; Clarke, M.J.; Shepherd, D.L.; Nassr, A.; DeMartino, R.R.; Bydon, M. Management of major vascular injury during pedicle screw instrumentation of thoracolumbar spine. Clin. Neurol. Neurosurg. 2017, 163, 53–59. [Google Scholar] [CrossRef]
- Kil, J.S.; Park, J.T. Simple New Screw Insertion Technique without Extraction for Broken Pedicle Screws. World Neurosurg. 2018, 113, 125–128. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No (%) or M ± SD (Min–Max) | p | |
|---|---|---|---|
| Sex | Male | 27 (45%) | 0.439 |
| Female | 33 (55%) | ||
| Age (years) | 56.07 ± 10.43 (30.0–73.0) | 0.921 | |
| Height (cm) | 174.02 ± 9.01 (155.0–194.0) | 0.282 | |
| Weight (kg) | 80.38 ± 13.48 (57.0–118.0) | 0.430 | |
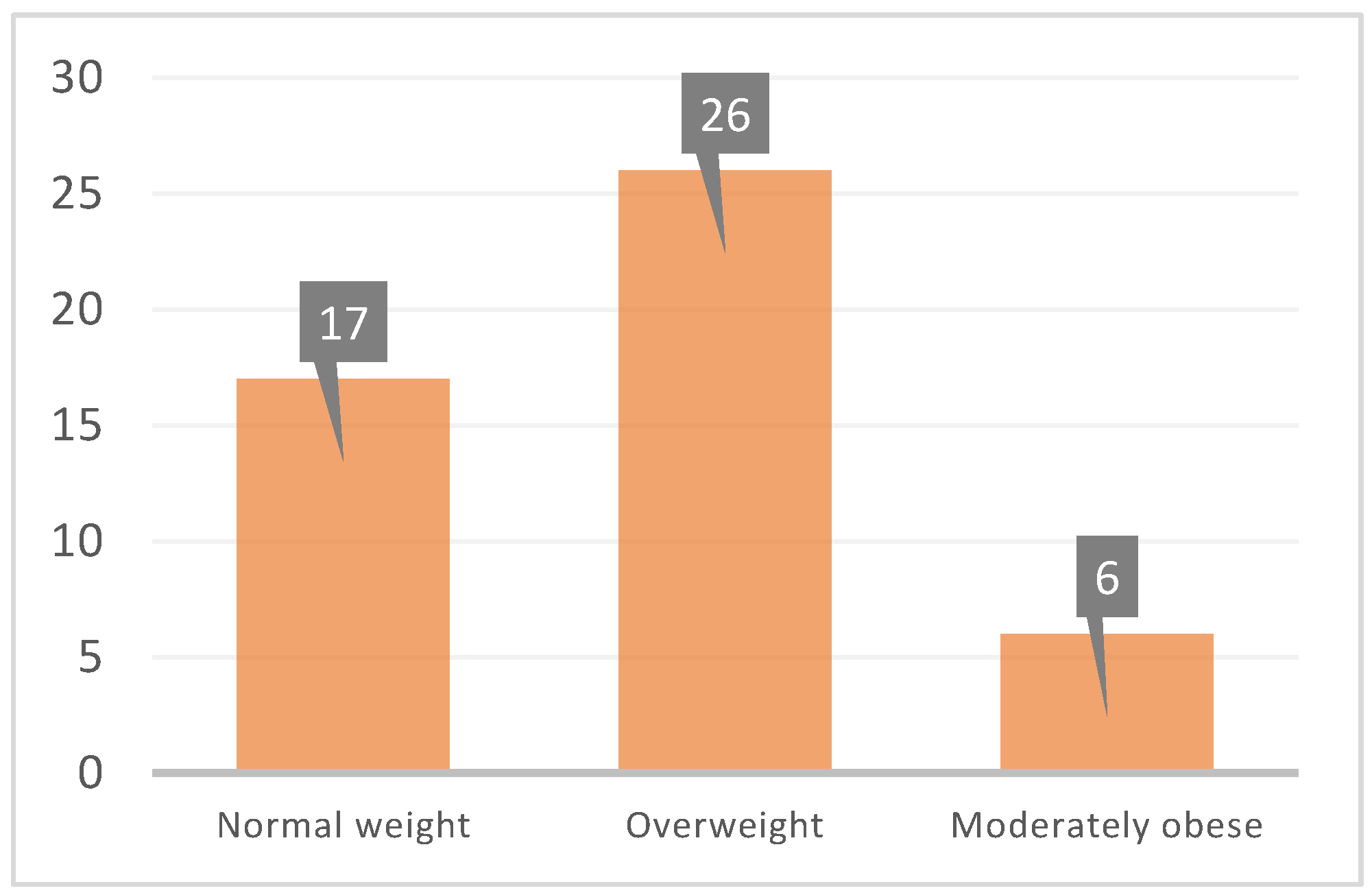
| BMI (kg/m2) | 26.53 ± 3.20 (19.3–31.7) | 0.002 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bečulić, H.; Begagić, E.; Džidić-Krivić, A.; Pugonja, R.; Jaganjac, B.; Imamović-Bošnjak, M.; Selimović, E.; Čeliković, A.; Skomorac, R.; Efendić, A.; et al. The Impact of Patient-Specific Positions on the Relationship between Iliac Blood Vessels and Lumbar Intervertebral Discs: Anatomical Significance and Clinical Implications. Anatomia 2024, 3, 16-28. https://doi.org/10.3390/anatomia3010003
Bečulić H, Begagić E, Džidić-Krivić A, Pugonja R, Jaganjac B, Imamović-Bošnjak M, Selimović E, Čeliković A, Skomorac R, Efendić A, et al. The Impact of Patient-Specific Positions on the Relationship between Iliac Blood Vessels and Lumbar Intervertebral Discs: Anatomical Significance and Clinical Implications. Anatomia. 2024; 3(1):16-28. https://doi.org/10.3390/anatomia3010003
Chicago/Turabian StyleBečulić, Hakija, Emir Begagić, Amina Džidić-Krivić, Ragib Pugonja, Belma Jaganjac, Melica Imamović-Bošnjak, Edin Selimović, Amila Čeliković, Rasim Skomorac, Alma Efendić, and et al. 2024. "The Impact of Patient-Specific Positions on the Relationship between Iliac Blood Vessels and Lumbar Intervertebral Discs: Anatomical Significance and Clinical Implications" Anatomia 3, no. 1: 16-28. https://doi.org/10.3390/anatomia3010003