
An Independent C1 Nerve Root Variant of the Ansa Cervicalis: A Case Report

 , ,
, , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Disclaimer Regarding Use of Human Donor Patients
2.2. Anatomical Dissection
3. Results
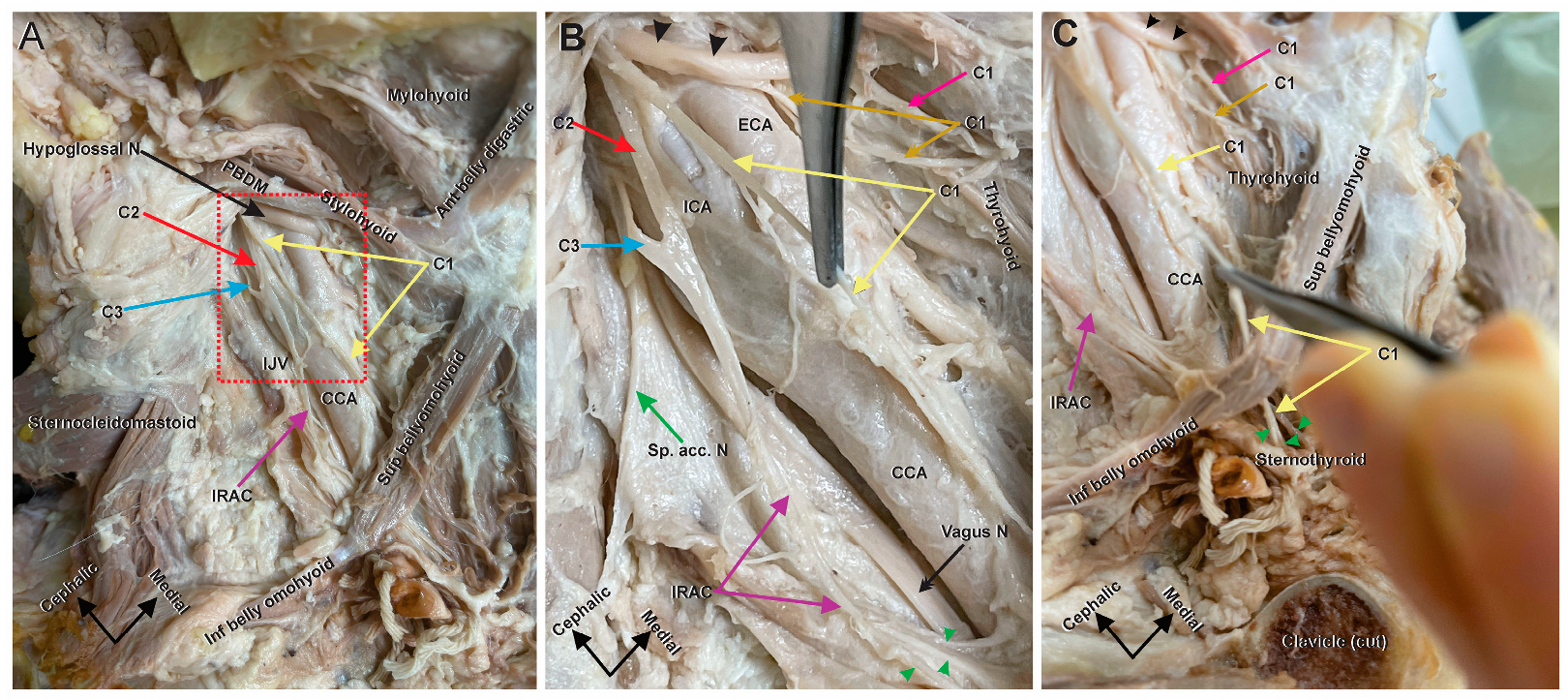
3.1. Anatomical Variant of the Right Ansa Cervicalis
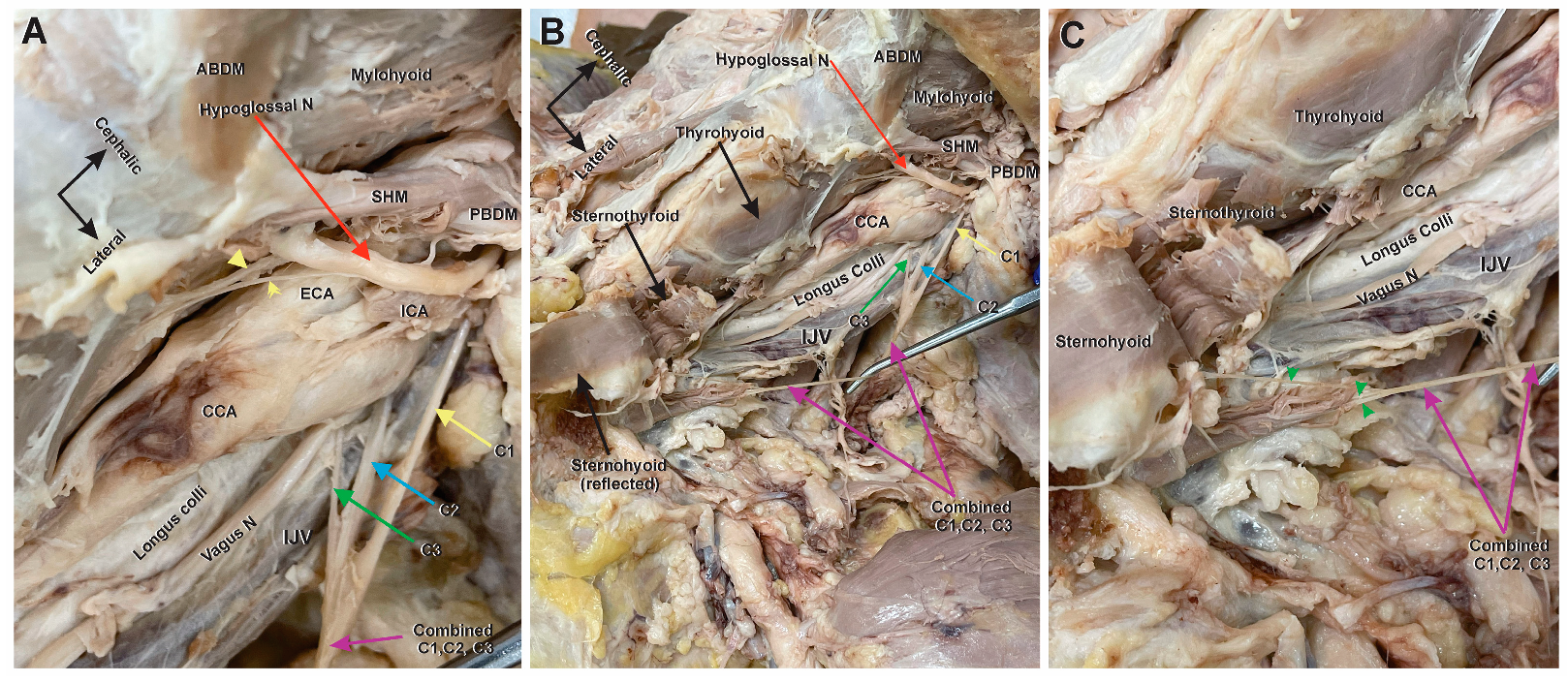
3.2. Bilateral Comparison of the Left Ansa Cervicalis
4. Discussion
5. Conclusions
- There is no ansa according to the true Latin derivative of the word (meaning “loop”);
- The root composed of C2 and C3, which would typically form the inferior root of the AC, descends independently to innervate the omohyoid and sternohyoid muscles;
- A C1 root exists that does not connect with the vagus nerve or C2/C3 branch, traveling independently to innervate the sternothyroid muscle.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kikuta, S.; Jenkins, S.; Kusukawa, J.; Iwanaga, J.; Loukas, M.; Tubbs, R.S. Ansa cervicalis: A comprehensive review of its anatomy, variations, pathology, and surgical applications. Anat. Cell Biol. 2019, 52, 221–225. [Google Scholar] [CrossRef]
- Mnatsakanian, A.; Al Khalili, Y. Anatomy, Head and Neck, Thyroid Muscles. In StatPearls; StatPearls Publishing LLC: Treasure Island, FL, USA, 2023. [Google Scholar]
- Quadros, L.S.; Prasanna, L.C.; D’Souza, A.S.; Singh, A.; Kalthur, S.G. Unilateral anatomical variation of the ansa cervicalis. Australas. Med. J. 2015, 8, 170–173. [Google Scholar] [CrossRef]
- Chhetri, D.K.; Blumin, J.H. Laryngeal reinnervation for unilateral vocal fold paralysis using ansa cervicalis nerve to recurrent laryngeal nerve anastomosis. Oper. Tech. Otolaryngol. Head Neck Surg. 2012, 23, 173–177. [Google Scholar] [CrossRef]
- Masuoka, H.; Miyauchi, A.; Yabuta, T.; Fukushima, M.; Miya, A. Innervation of the cricothyroid muscle by the recurrent laryngeal nerve. Head Neck 2016, 38 (Suppl. S1), E441–E445. [Google Scholar] [CrossRef]
- Lynch, J.; Parameswaran, R. Management of unilateral recurrent laryngeal nerve injury after thyroid surgery: A review. Head Neck 2017, 39, 1470–1478. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.T.; Scott, W.C.; Zealear, D.; Schwartz, A.R. Ansa cervicalis stimulation increases pharyngeal patency in patients with obstructive sleep apnea. J. Appl. Physiol. 2021, 131, 487–495. [Google Scholar] [CrossRef]
- Kent, D.T.; Zealear, D.; Schwartz, A.R. Ansa Cervicalis and Hypoglossal Nerve Stimulation in a Patient With Obstructive Sleep Apnea. Otolaryngol. Head Neck Surg. 2021, 165, 602–604. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Singh, V.; Ohtsuka, A.; Hwang, Y.; Kim, H.J.; Moryś, J.; Ravi, K.S.; Ribatti, D.; Trainor, P.A.; Sañudo, J.R.; et al. Acknowledging the use of human cadaveric tissues in research papers: Recommendations from anatomical journal editors. Clin. Anat. 2021, 34, 2–4. [Google Scholar] [CrossRef]
- Abu-Hijleh, M.F. Bilateral absence of ansa cervicalis replaced by vagocervical plexus: Case report and literature review. Ann. Anat. Anat. Anz. 2005, 187, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Chhetri, D.K.; Berke, G.S. Ansa Cervicalis Nerve: Review of the Topographic Anatomy and Morpholog. Laryngoscope 1997, 107, 1366–1372. [Google Scholar] [CrossRef]
- Caliot, P.; Dumont, D.; Bousquet, V.; Midy, D. A note on the anastomoses between the hypoglossal nerve and the cervical plexus. Surg. Radiol. Anat. 1986, 8, 75–79. [Google Scholar] [CrossRef]
- Ayyoubian, M.; Koruji, M. A rare anatomical variant of ansa cervicalis: Case report. Med. J. Islam. Repub. Iran 2011, 24, 238–240. [Google Scholar]
- D’Souza, A.S.; Ray, B. Study of the formation and distribution of the ansa cervicalis and its clinical significance. Eur. J. Anat. 2010, 14, 143–148. [Google Scholar]
- Rath, G.; Anand, C. Vagocervical complex replacing an absent ansa cervicalis. Surg. Radiol. Anat. 1994, 16, 441–443. [Google Scholar] [CrossRef]
- Manjunath, K.Y. Vagal origin of the ANSA cervicalis nerve—Report of two cases. Indian J. Otolaryngol. Head Neck Surg. 2000, 52, 257–258. [Google Scholar] [CrossRef]
- Kikuchi, T. A contribution to the morphology of the ansa cervicalis and the phrenic nerve. Kaibogaku Zasshi 1970, 45, 242–281. [Google Scholar]
- Jelev, L. Some unusual types of formation of the ansa cervicalis in humans and proposal of a new morphological classification. Clin. Anat. 2013, 26, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Blythe, J.N.; Matharu, J.; Reuther, W.J.; Brennan, P.A. Innervation of the lower third of the sternocleidomastoid muscle by the ansa cervicalis through the C1 descendens hypoglossal branch: A previously unreported anatomical variant. Br. J. Oral Maxillofac. Surg. 2015, 53, 470–471. [Google Scholar] [CrossRef]
- Anghel, A.; Anghel, I.; Dumitru, M.; Soreanu, C. Respiratory and phonatory impairment due to iatrogenic vocal fold paralysis and paresis. A retrospective study of 188 patients. Rom. J. Leg. Med. 2012, 20, 287–290. [Google Scholar] [CrossRef]
- Vrinceanu, D.; Dumitru, M.; Popa-Cherecheanu, M.; Marinescu, A.N.; Patrascu, O.-M.; Bobirca, F. Extracranial Facial Nerve Schwannoma—Histological Surprise or Therapeutic Planning? Medicina 2023, 59, 1167. [Google Scholar] [PubMed]
- Rath, S.; Sasmal, P.K.; Saha, K.; Deep, N.; Mishra, P.; Mishra, T.S.; Sharma, R. Ancient Schwannoma of Ansa Cervicalis: A Rare Clinical Entity and Review of the Literature. Case Rep. Surg. 2015, 2015, 578467. [Google Scholar] [CrossRef] [PubMed]
- Paniello, R.C. Laryngeal reinnervation. Otolaryngol. Clin. N. Am. 2004, 37, 161–181. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.; Mohan, S.; Richmon, J.D.; Jowett, N. An Anatomic Variant of the Ansa Cervicalis Precluding Its Use as a Donor Nerve. Ann. Otol. Rhinol. Laryngol. 2020, 129, 78–81. [Google Scholar] [CrossRef] [PubMed]
- Prades, J.M.; Gavid, M.; Dubois, M.D.; Dumollard, J.M.; Timoshenko, A.T.; Peoc’h, M. Surgical anatomy of the ansa cervicalis nerve: Which branch to use for laryngeal reinnervation in humans? Surg. Radiol. Anat. 2015, 37, 139–145. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lassiter, E.; Keating, J.M.; Tarter, K.; Saxton, K.; Yerubandi, S.; Habib, S.; Bailey, B.; Maklad, A. An Independent C1 Nerve Root Variant of the Ansa Cervicalis: A Case Report. Anatomia 2024, 3, 8-15. https://doi.org/10.3390/anatomia3010002
Lassiter E, Keating JM, Tarter K, Saxton K, Yerubandi S, Habib S, Bailey B, Maklad A. An Independent C1 Nerve Root Variant of the Ansa Cervicalis: A Case Report. Anatomia. 2024; 3(1):8-15. https://doi.org/10.3390/anatomia3010002
Chicago/Turabian StyleLassiter, Eric, Julia M Keating, Kristina Tarter, Kylie Saxton, Sanjana Yerubandi, Safa Habib, Brianna Bailey, and Adel Maklad. 2024. "An Independent C1 Nerve Root Variant of the Ansa Cervicalis: A Case Report" Anatomia 3, no. 1: 8-15. https://doi.org/10.3390/anatomia3010002