
Brain Abscess Secondary to an Apparently Benign Transorbital Injury: An Infrequent Case Report with Literature Review
 ,
,  , ,
, , 
Abstract
:1. Introduction
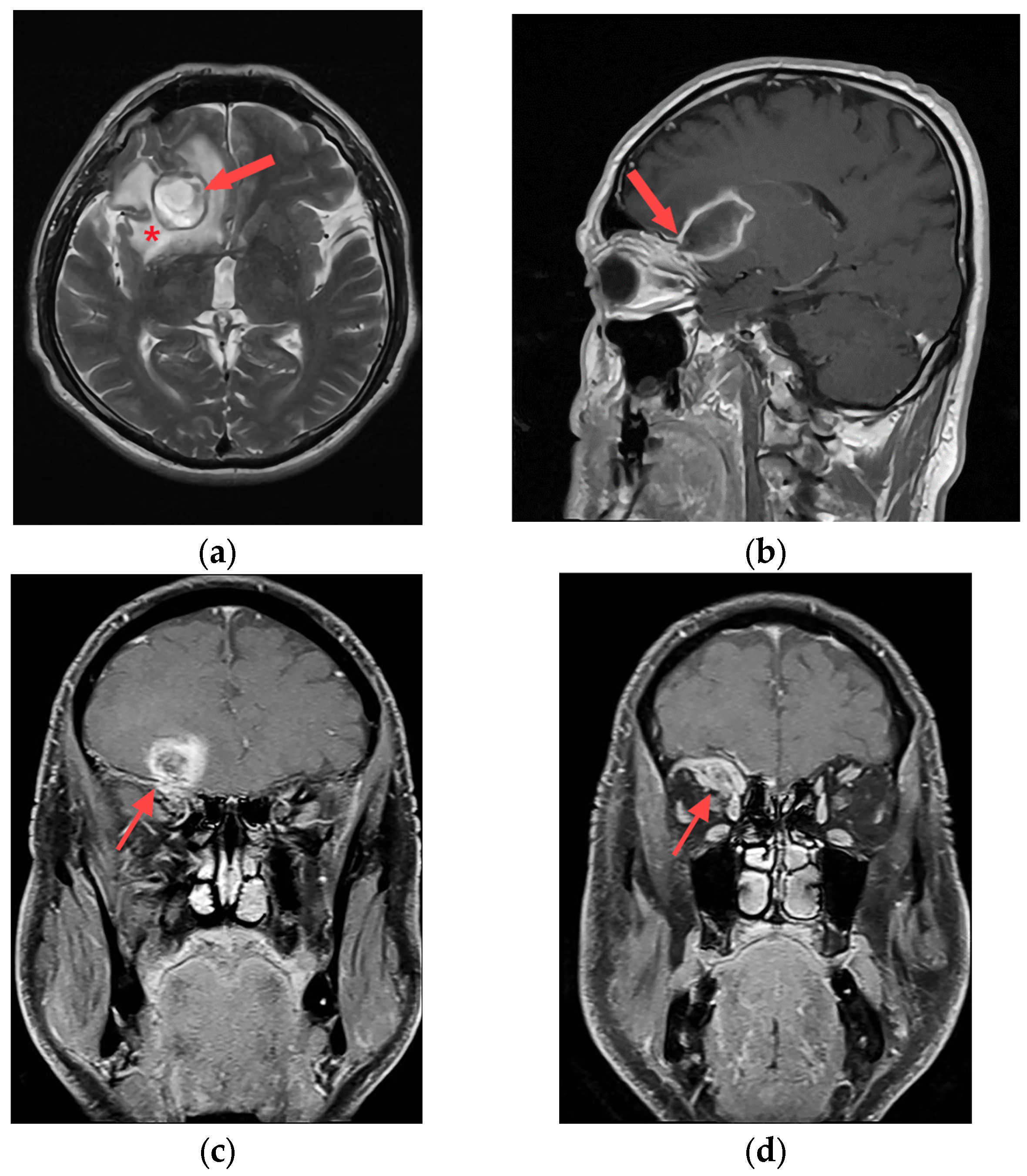
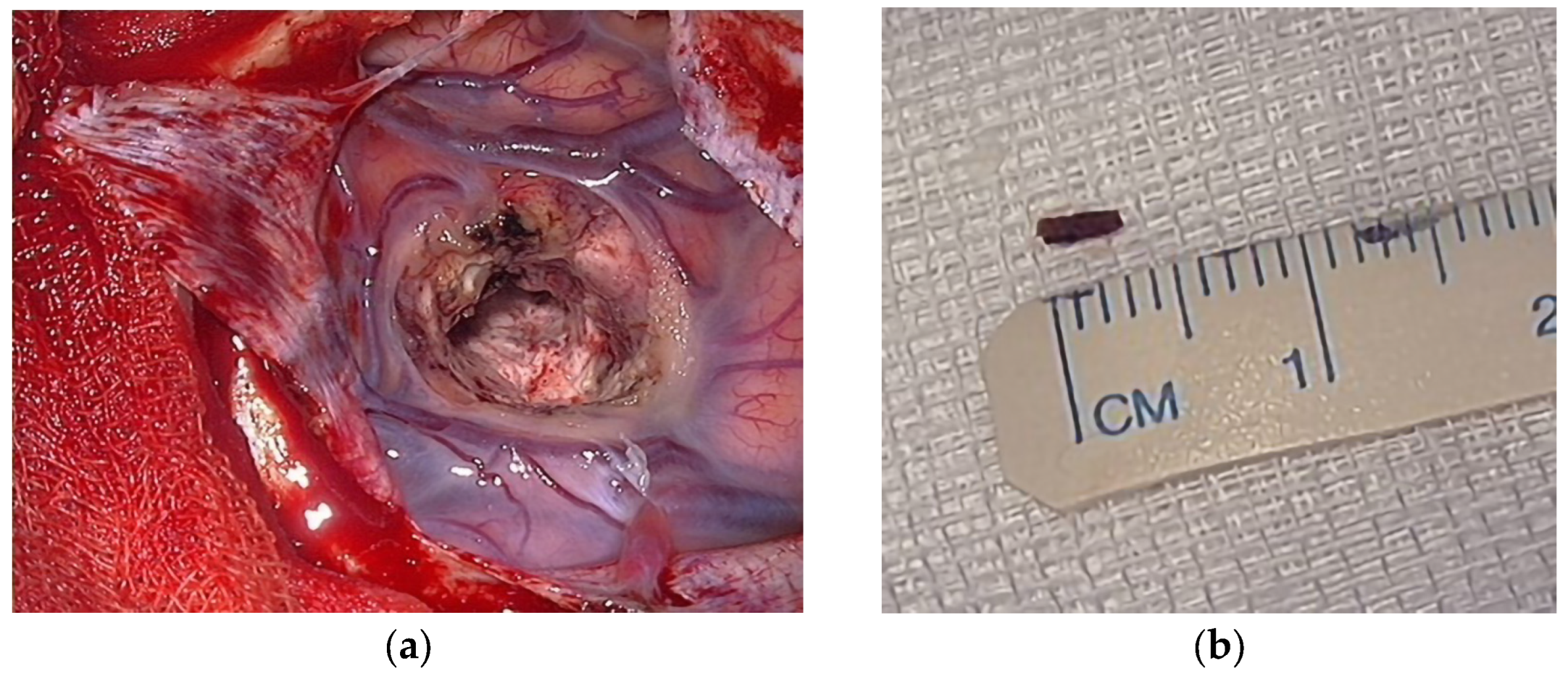
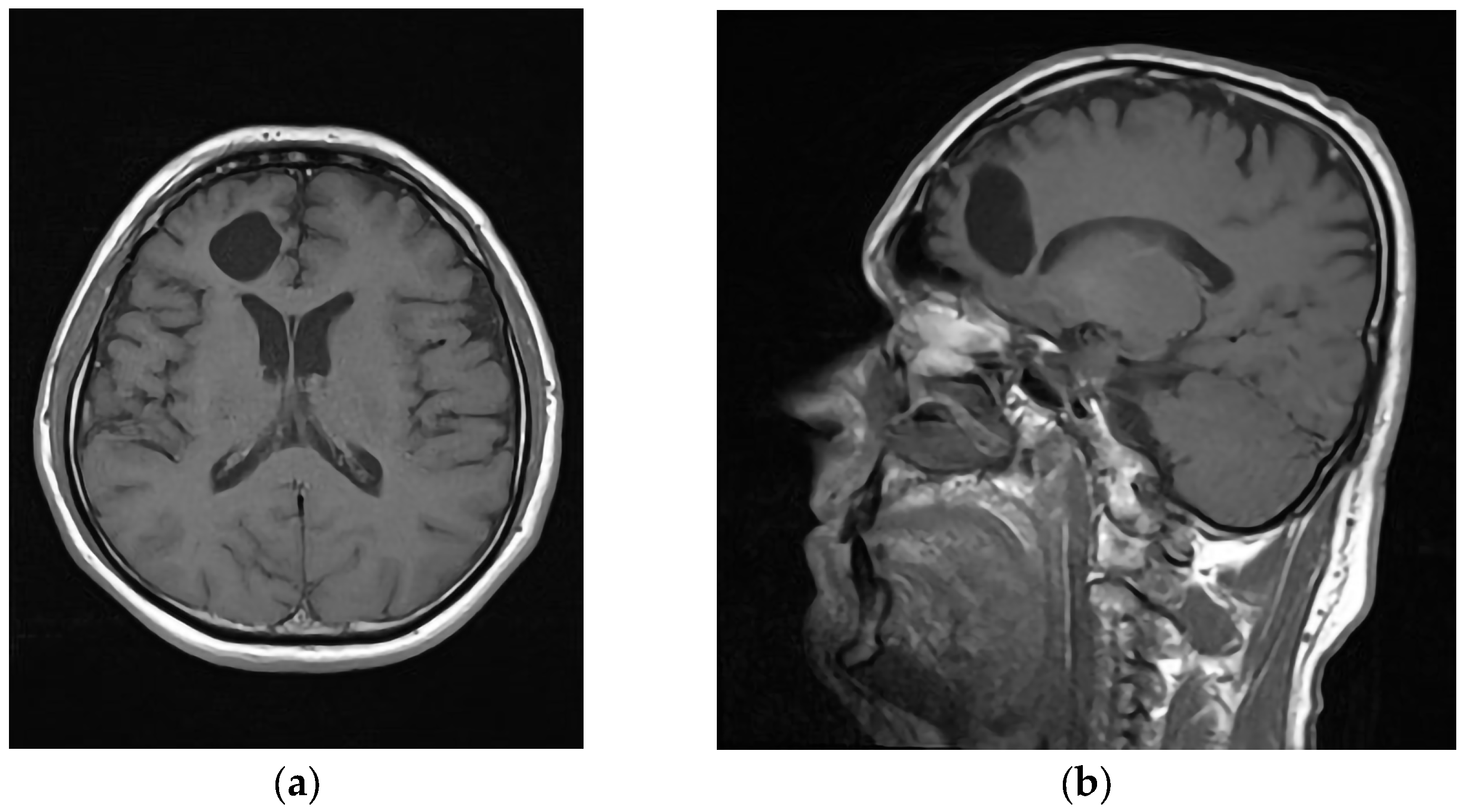
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baiden, F.; Anto-Ocrah, M.; Adjei, G.; Gyaase, S.; Abebrese, J.; Punguyire, D.; Owusu-Agyei, S.; Moresky, R.T. Head Injury Prevalence in a Population of Injured Patients Seeking Care in Ghana, West Africa. Front. Neurol. 2022, 13, 917294. [Google Scholar] [CrossRef] [PubMed]
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maruya, J.; Yamamoto, K.; Wakai, M.; Kaneko, U. Brain abscess following transorbital penetrating injury due to bamboo fragments—Case report. Neurol. Med. Chir. 2002, 42, 143–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koenen, L.; Waseem, M. Orbital Floor Fracture. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Lethaus, B.; Weigl, S.; Kloss-Brandstätter, A.; Kloss, F.R.; Kessler, P.; Hölzle, F.; Bangard, C. Looking for landmarks in medial orbital trauma surgery. Int. J. Oral Maxillofac. Surg. 2013, 42, 209–213. [Google Scholar] [CrossRef]
- Ghosh, S.K.; Narayan, R.K. Fractures involving bony orbit: A comprehensive review of relevant clinical anatomy. Transl. Res. Anat. 2021, 24, 100125. [Google Scholar] [CrossRef]
- Xu, L.; Xu, F.; Li, L.; Liu, W.; Kit Leung, G.K.; Liu, B. The Surgical Strategies and Techniques of Transorbital Nonmissile Brain Injury. World Neurosurg. 2020, 144, e856–e865. [Google Scholar] [CrossRef]
- Reinshagen, K.L.; Massoud, T.F.; Cunnane, M.B. Anatomy of the Orbit. Neuroimaging Clin. N. Am. 2022, 32, 699–711. [Google Scholar] [CrossRef]
- Liu, S.; Yan, W.; Wang, G.; Zhao, R.; Qiu, H.; Cao, L.; Wang, H. Topographic Anatomy of the Zygomatico-Orbital Artery: Implications for Improving the Safety of Temporal Augmentation. Plast. Reconstr. Surg. 2021, 148, 19e–27e. [Google Scholar] [CrossRef]
- Apaydin, N.; Kendir, S.; Karahan, S.T. The Anatomical Relationships of the Ocular Motor Nerves with an Emphasis on Surgical Anatomy of the Orbit. Anat. Rec. 2019, 302, 568–574. [Google Scholar] [CrossRef]
- Alvis Miranda, H.; Castellar-Leones, S.M.; Elzain, M.A.; Moscote-Salazar, L.R. Brain abscess: Current management. J. Neurosci. Rural Pract. 2013, 4, S67–S81. [Google Scholar] [CrossRef]
- Prasetyo, E.; Oley, M.C.; Sumual, V.; Faruk, M. Transorbital-penetrating intracranial injury due to a homemade metal arrow: A case report. Ann. Med. Surg. 2020, 57, 183–189. [Google Scholar] [CrossRef]
- Kuromi, Y.; Sato, T.; Ando, H.; Matsumoto, Y.; Oda, K.; Ito, E.; Ichikawa, M.; Watanabe, T.; Sakuma, J.; Saito, K. Removal of bamboo fragments transorbitally penetrated into the cerebellum and temporal lobe 30 years after the injury. Neurol. Surg. 2012, 40, 979–983. [Google Scholar]
- Amano, K.; Kamano, S. Cerebellar abscess due to penetrating orbital wound. J. Comput. Assist. Tomogr. 1982, 6, 1163–1166. [Google Scholar] [CrossRef] [PubMed]
- Abdulbaki, A.; Al-Otaibi, F.; Almalki, A.; Alohaly, N.; Baeesa, S. Transorbital Craniocerebral Occult Penetrating Injury with Cerebral Abscess Complication. Case Rep. Ophthalmol. Med. 2012, 2012, 742186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdulrazeq, H.; Walek, K.; Sampath, S.; Shaaya, E.; Beqiri, D.; Woo, A.; Sampath, P. Development of posttraumatic frontal brain abscess in association with an orbital roof fracture and odontogenic abscess: A case report. Surg. Neurol. Int. 2022, 13, 539. [Google Scholar] [CrossRef] [PubMed]
- Seider, N.; Gilboa, M.; Lautman, E.; Miller, B. Delayed presentation of orbito-cerebral abscess caused by pencil-tip injury. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 316–317. [Google Scholar] [CrossRef]
- Di Roio, C.; Jourdan, C.; Mottolese, C.; Convert, J.; Artru, F. Craniocerebral injury resulting from transorbital stick penetration in children. Childs Nerv. Syst. 2000, 16, 503–506; discussion 507. [Google Scholar] [CrossRef]
- Aulino, J.M.; Gyure, K.A.; Morton, A.; Cole, J.W. Temporal lobe intraparenchymal retained foreign body from remote orbital trauma. AJNR Am. J. Neuroradiol. 2005, 26, 1855–1857. [Google Scholar]
- Santoreneos, S.; Hanieh, A.; Moore, L. ‘Splinter in the mind’: A case of penetrating periorbital injury. J. Clin. Neurosci. 1997, 4, 255–257. [Google Scholar] [CrossRef]
- De Andres Crespo, M.; McKinnon, C.; Halliday, J. What you need to know about brain abscesses. Br. J. Hosp. Med. 2020, 81, 1–7. [Google Scholar] [CrossRef]
- Brouwer, M.C.; van de Beek, D. Epidemiology, diagnosis, and treatment of brain abscesses. Curr. Opin. Infect. Dis. 2017, 30, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Seydoux, C.; Francioli, P. Bacterial brain abscesses: Factors influencing mortality and sequelae. Clin. Infect. Dis. 1992, 15, 394–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadgil, N.; Patel, A.J.; Gopinath, S.P. Open craniotomy for brain abscess: A forgotten experience? Surg. Neurol. Int. 2013, 4, 34. [Google Scholar] [CrossRef]
- Mampalam, T.J.; Rosenblum, M.L. Trends in the management of bacterial brain abscesses: A review of 102 cases over 17 years. Neurosurgery 1988, 23, 451–458. [Google Scholar] [CrossRef]
- Ratnaike, T.E.; Das, S.; Gregson, B.A.; Mendelow, A.D. A review of brain abscess surgical treatment—78 years: Aspiration versus excision. World Neurosurg. 2011, 76, 431–436. [Google Scholar] [CrossRef]
- Cavuşoglu, H.; Kaya, R.A.; Türkmenoglu, O.N.; Colak, I.; Aydin, Y. Brain abscess: Analysis of results in a series of 51 patients with a combined surgical and medical approach during an 11-year period. Neurosurg. Focus 2008, 24, E9. [Google Scholar] [CrossRef] [Green Version]
- Elmallawany, M.; Ashry, A.; Alsawy, M.F. Endoscopic treatment of brain abscess. Surg. Neurol. Int. 2021, 12, 36. [Google Scholar] [CrossRef]
- Feraco, P.; Donner, D.; Gagliardo, C.; Leonardi, I.; Piccinini, S.; Del Poggio, A.; Franciosi, R.; Petralia, B.; van den Hauwe, L. Cerebral abscesses imaging: A practical approach. J. Popul. Ther. Clin. Pharmacol. 2020, 27, e11–e24. [Google Scholar] [CrossRef]
- Beculić, H.; Begagić, E.; Skomorac, R.; Jusic, A.; Čejvan, L. Seemingly innocuous trauma on the neurosurgical table: A rare case of brain abscess. In Proceedings of the 8th Annual Meeting of Serbian Neurosurgery Society, Beograd, Serbia, 8–10 December 2022. [Google Scholar]
- Hiraishi, T.; Tomikawa, M.; Kobayashi, T.; Kawaguchi, T. Delayed brain abscess after penetrating transorbital injury. Neurol. Surg. 2007, 35, 481–486. [Google Scholar]
- Rahman, N.U.; Jamjoom, A.; Jamjoom, Z.A.; Abu el-Asrar, A. Orbito-cranial injury caused by penetrating metallic foreign bodies: Report of two cases. Int. Ophthalmol. 1997, 21, 13–17. [Google Scholar] [CrossRef]
- Potapov, A.A.; Eropkin, S.V.; Kornienko, V.N.; Arutyunov, N.V.; Yeolchiyan, S.A.; Serova, N.K.; Kravtchuk, A.D.; Shahinian, G.G. Late diagnosis and removal of a large wooden foreign body in the cranio-orbital region. J. Craniofac. Surg. 1996, 7, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Rupa, R.; Vladimirov, T.; Pojskic, M.; Nimsky, C.; Voellger, B. Dynamics in the Neurotrauma Catchment Area of a German University Hospital during the COVID-19 Pandemic. Healthcare 2022, 10, 1376. [Google Scholar] [CrossRef] [PubMed]
- Efendić, A.; Bečulić, H.; Skomorac, R.; Jusić, A.; Selimović, E.; Begagić, E.; Juković-Bihorac, F. Infrequent case of cavum septi pellucidi empyema and principles of neurosurgical management: Case report and literature review. Medica Jadertina 2023, 53, 55–60. [Google Scholar] [CrossRef]
- Alic, F.; Jusic, A.; Beculic, H.; Barucija, N.; Ibrahimagic-Suljic, E. Successful management of subdural intracranial empyema linked with cerebral abscess as a consequence of pansinusitis. Medeniyet Med. J. 2018, 33, 140–143. [Google Scholar] [CrossRef] [Green Version]
- Martin-Canal, G.; Saavedra, A.; Asensi, J.M.; Suarez-Zarracina, T.; Rodriguez-Guardado, A.; Bustillo, E.; Fierer, J.; Carton, J.A.; Collazos, J.; Asensi, V. Meropenem monotherapy is as effective as and safer than imipenem to treat brain abscesses. Int. J. Antimicrob. Agents 2010, 35, 301–304. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Reference | Patient Information | Foreign Body and Its Path | Abscess Occur | ||
|---|---|---|---|---|---|
| Y | G | Anamnestic Data | |||
| Maruya et al. [3] | 56 | F | TOPI while hiking on mountain | Bamboo grove (left upper eyelid) | 2 weeks a.i. |
| Hiraishi et al. [31] | 14 | F | TOPI |
Plastic chopstick (left upper eyelid) | 9 years a.i. |
| Kuromi et al. [13] | 37 | M | TOPI |
Bamboo fragments (trough cavernous sinus to FCP) | 30 years a.i. |
| Abdulrazeq et al. [16] | 40 | TF |
Superior, lateral, medial, and inferior orbital due vehicle accident | None detected | 2 months a.i. |
| Abdulbaki et al. [15] | 5 | M | TOPI due to fall | Pen (right upper eyelid to orbital roof) | 4 or 5 days |
| Seider et al. [17] | 1 | M | Stabbed in right upper eyelid | Pen with graphite tip (right upper eyelid) | 3 weeks a.i. |
| Aulino et al. [19] | 35 | M | A blow to the left orbit with a billiard cue stick 16 years previous | Fiberglass or wood | 16 days a.i. |
| Santoreneos et al. [20] | 12 | M | Orbito-cranial injury while riding a motorbike | Branch of tree (right lower eyelid) | 10 days a.i. postop |
| Rahman et al. [32] | 30 | M | TOPI due nail hammering | Nail (superior orbital fissure) | meningitis a.i. |
| Potapov et al. [33] | 26 | M | TOPI after motocycle crashed into tree | Branch of tree (medial orbital wall) | 2 months a.i. |
| Di Roio et al. [18] | 6 | M | TOPI and closure of interventricular anastomosis 6 years before; Down syndrome | Chopstick (orbital roof) | 10 days a.i. |
| Amano et al. [14] | 7 | M | TOPI after jumping from garage (2 m) | Bamboo grove (eyelid) | 10 months a.i. |
| Bečulić et al. [This study] | 57 | M | TOPI | Wooden twig | 1 month a.i. |
| Reference | Bacterial Cause | Laboratory | Radiological findings | ||
| Maruya et al. [3] | none isolated | WBC and CRP increased | CT: cerebral contusion and free bone fragments in temporal lobe) | ||
| Hiraishi et al. [31] | unknown a | Unknown a | CT: two ring-enhancing masses in right temporal lobe | ||
| Kuromi et al. [13] | unknown a | Unknown a | MRI: two ring-enhanced lesions in cerebellum | ||
| Abdulrazeq et al. [16] | Streptococcus intermedius | CRP and erythrocyte sedimentation rate elevated | MRI: right frontal heterogeneous collection | ||
| Abdulbaki et al. [15] | none isolated | w/o leukocytosis | CT: a bordered formation around metal tip of pen | ||
| Seider et al. [17] | Alpha-hemolytic streptococci | Nothing reported | CT: large extraconal multiloculated orbito-cerebral abscess | ||
| Aulino et al. [19] | nothing reported | Unremarkable | MR: multilocular intraparenchymal abscesses in left temporal lobe | ||
| Santoreneos et al. [20] | Enterobacter agglomerans (2 biotypes) | Nothing reported | Initial CT: fracture of medial orbital wall 2nd CT: a ring enhancing lesion of the right temporal lobe 3rd CT: slight decrease in size of the abscess | ||
| Rahman et al. [32] | nothing reported | Nothing reported | X-ray: bent nail in the orbit and middle cranial fossa CT: nail lodged in orbital cavity and temporal lobe | ||
| Potapov et al. [33] | nothing reported | Nothing reported | CT: a bordered formation in right temporal lobe | ||
| Di Roio et al. [18] | nothing reported | WBC increased in blood and CSF with glycorrhachia | CT: hypodense mass occupying the left frontal lobe | ||
| Amano et al. [14] | Escherihia coli | Nothing reported | CT: cerebellar abscess | ||
| Bečulić et al. [This study] | none isolated | Unremarkable | MRI: expansive intracerebral process in the right frontal lobe | ||
| Reference | Treatment | Outcome | |||
| Antibiotics | Surgical | ||||
| Maruya et al. [3] | 5 days of oral antibiotics (unknown), 3 days of antibiotic (unknown) solution irrigation | Stereotaxic aspiration with drainage tube for antibiotic solution irrigation | Abscess reduction; left eye had a slight lateral gaze limitation | ||
| Hiraishi et al. [31] | 4-week course of antibiotics (unknown a) |
Fronto-temporal decompressive craniectomy and stereotactic aspiration; removal of foreign body | Discharged with slight hyposmia | ||
| Kuromi et al. [13] | Unknown a | Endoscopic aproach, drainage | Left blindness, oculomotor palsy, trigeminal nerve anesthesia, and ataxia | ||
| Abdulrazeq et al. [16] | Ceftriaxone for 6 weeks | Open surgery due multiple fractures | 3 months after: oedema and abscess resolution | ||
| Abdulbaki et al. [15] | Vancomycin, ceftazidime, and metronidazole for 3 weeks | Transcutaneous upper eyelid surgery | 2 months after: CT showed abscess resolution. Mild right eyelid ptosis. | ||
| Seider et al. [17] | Ceftriaxone and metronidazole for 6 weeks | Drainage through a frontal burr hole for 1 week | 1 mm of right upper eyelid ptosis after 10 months | ||
| Aulino et al. [19] | Nothing reported | Surgical excision | Full recovery | ||
| Santoreneos et al. [20] | Gentamicin (replaced by cefotaxime due to toxicity), penicillin and metronidazole | Elective extirpation of abscess cavity after 3rd CT | Full recovery | ||
| Rahman et al. [32] | Ceftriaxone and metronidazole | Craniotomy and early meningitis noticed | Right side blindness due eyeball penetration | ||
| Potapov et al. [33] | Cefotaxime, metronidazole and amikacin | Craniotomy, sphenoid bone resection, pus aspiration and irrigation (antiseptic solution) | Mucocele in frontal sinus 6 months later | ||
| Di Roio et al. [18] | Initially amoxicillin, then josamycin and cefaclor (10 days), due to worsening ceftriaxone, fosfomycin and metronidazole administred (4 weeks). At home: oral amoxicillin and clindamycin (4 weeks) | Abscess puncture | Abscess resolution 2 months after surgery | ||
| Amano et al. [14] | Systematic antibiotics administred (unknown) | None | Reduction in abscess | ||
| Bečulić et al. [This study] | Meropenem for 5 weeks | Abscess drainage | Full recovery | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bečulić, H.; Begagić, E.; Skomorac, R.; Jusić, A.; Selimović, E.; Čejvan, L.; Pojskić, M. Brain Abscess Secondary to an Apparently Benign Transorbital Injury: An Infrequent Case Report with Literature Review. Anatomia 2023, 2, 243-252. https://doi.org/10.3390/anatomia2030022
Bečulić H, Begagić E, Skomorac R, Jusić A, Selimović E, Čejvan L, Pojskić M. Brain Abscess Secondary to an Apparently Benign Transorbital Injury: An Infrequent Case Report with Literature Review. Anatomia. 2023; 2(3):243-252. https://doi.org/10.3390/anatomia2030022
Chicago/Turabian StyleBečulić, Hakija, Emir Begagić, Rasim Skomorac, Aldin Jusić, Edin Selimović, Lejla Čejvan, and Mirza Pojskić. 2023. "Brain Abscess Secondary to an Apparently Benign Transorbital Injury: An Infrequent Case Report with Literature Review" Anatomia 2, no. 3: 243-252. https://doi.org/10.3390/anatomia2030022