
Community Coping Strategies for COVID-19 in Bangladesh: A Nationwide Cross-Sectional Survey
 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
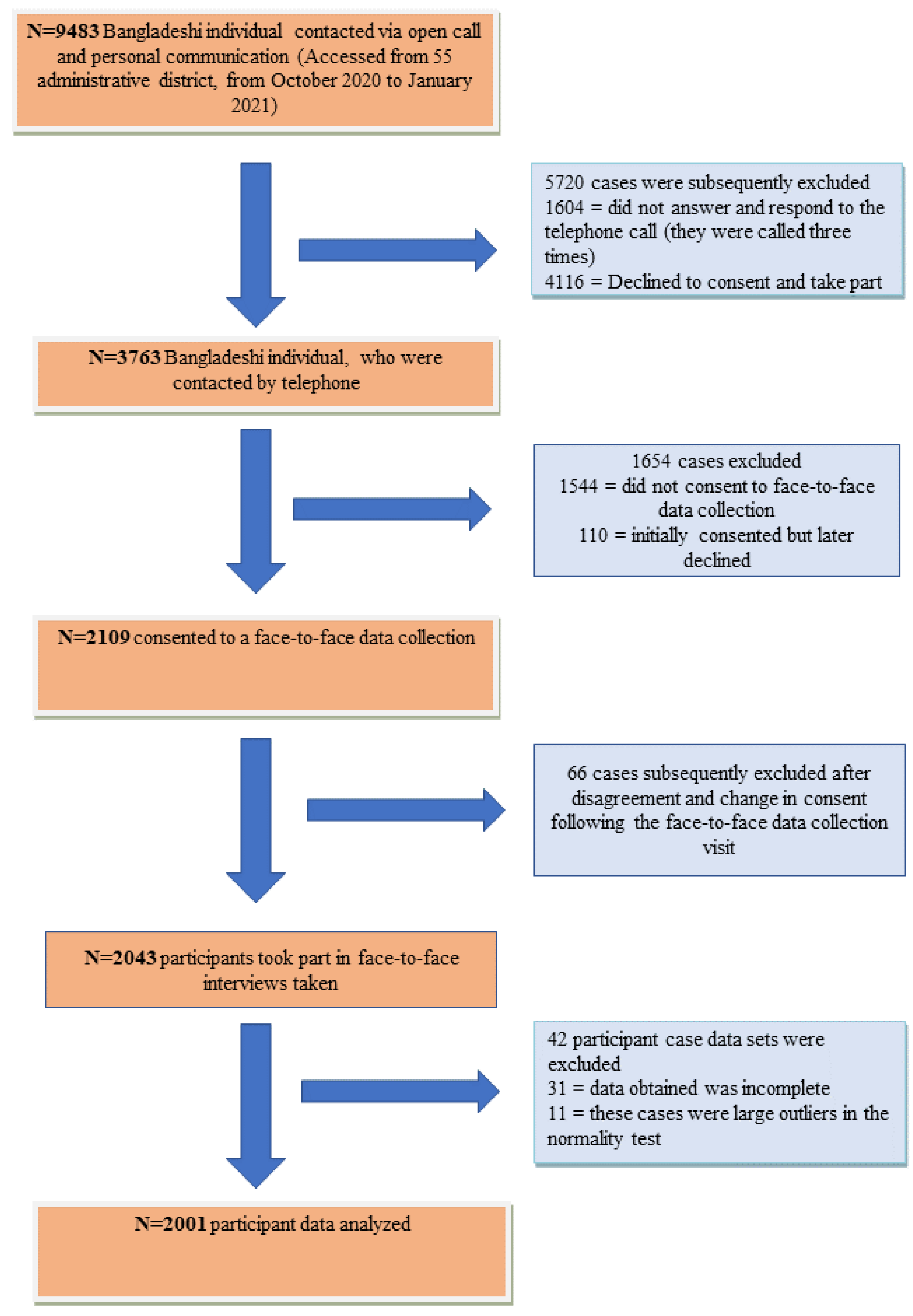
2.2. Participants
2.3. Ethical Permission
2.4. Study Procedure
2.5. Questionnaire
2.6. Reliability and Validity of the Brief-COPE
2.7. Statistical Testing
3. Results
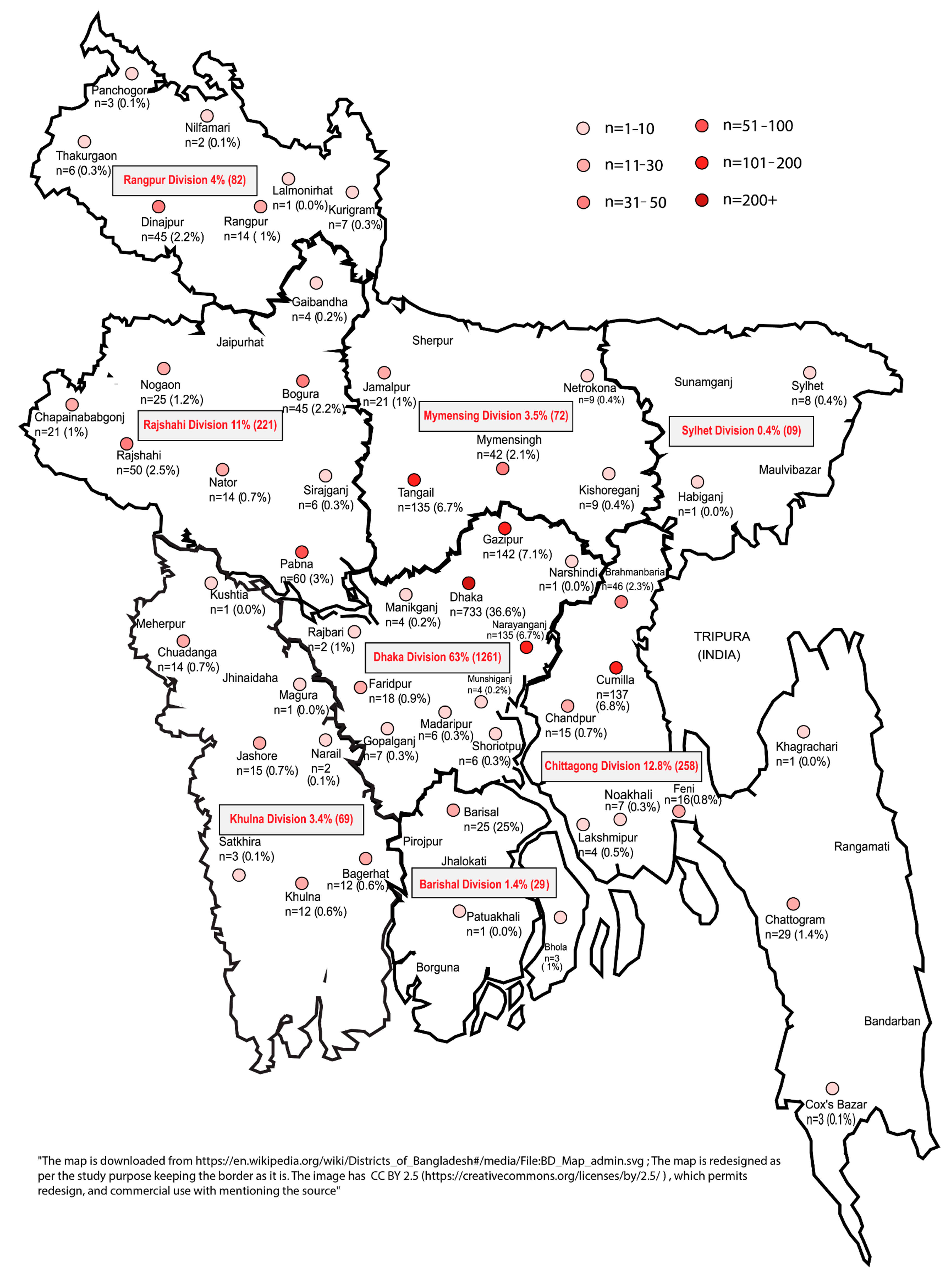
3.1. Distribution of Responses
3.2. Socio-Demography of Respondents Socio-Demographic Profile of the Respondents
3.3. Health-Related Information
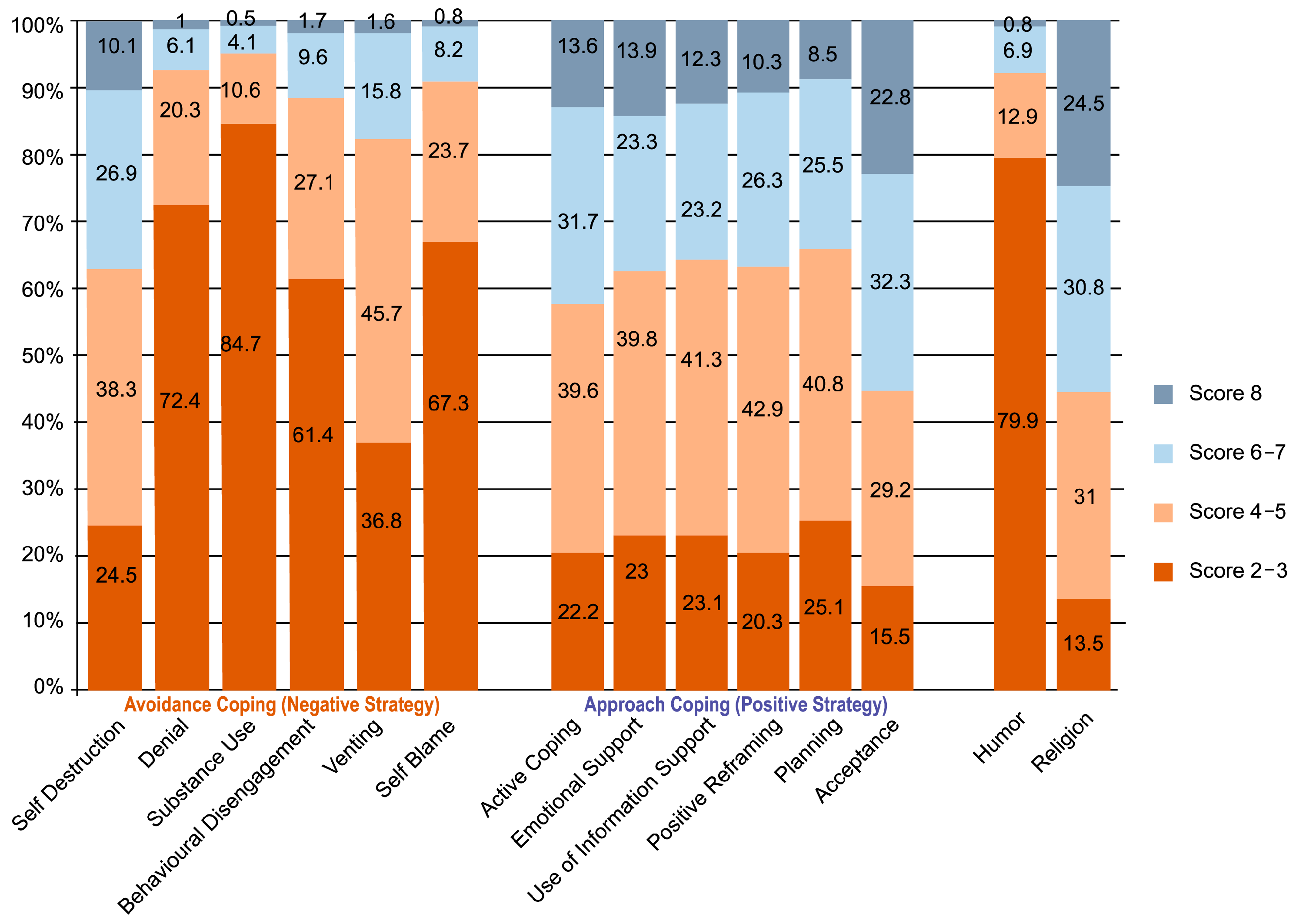
3.4. Coping Strategies
3.5. Relationship between Socio-Demographics and Coping Strategy
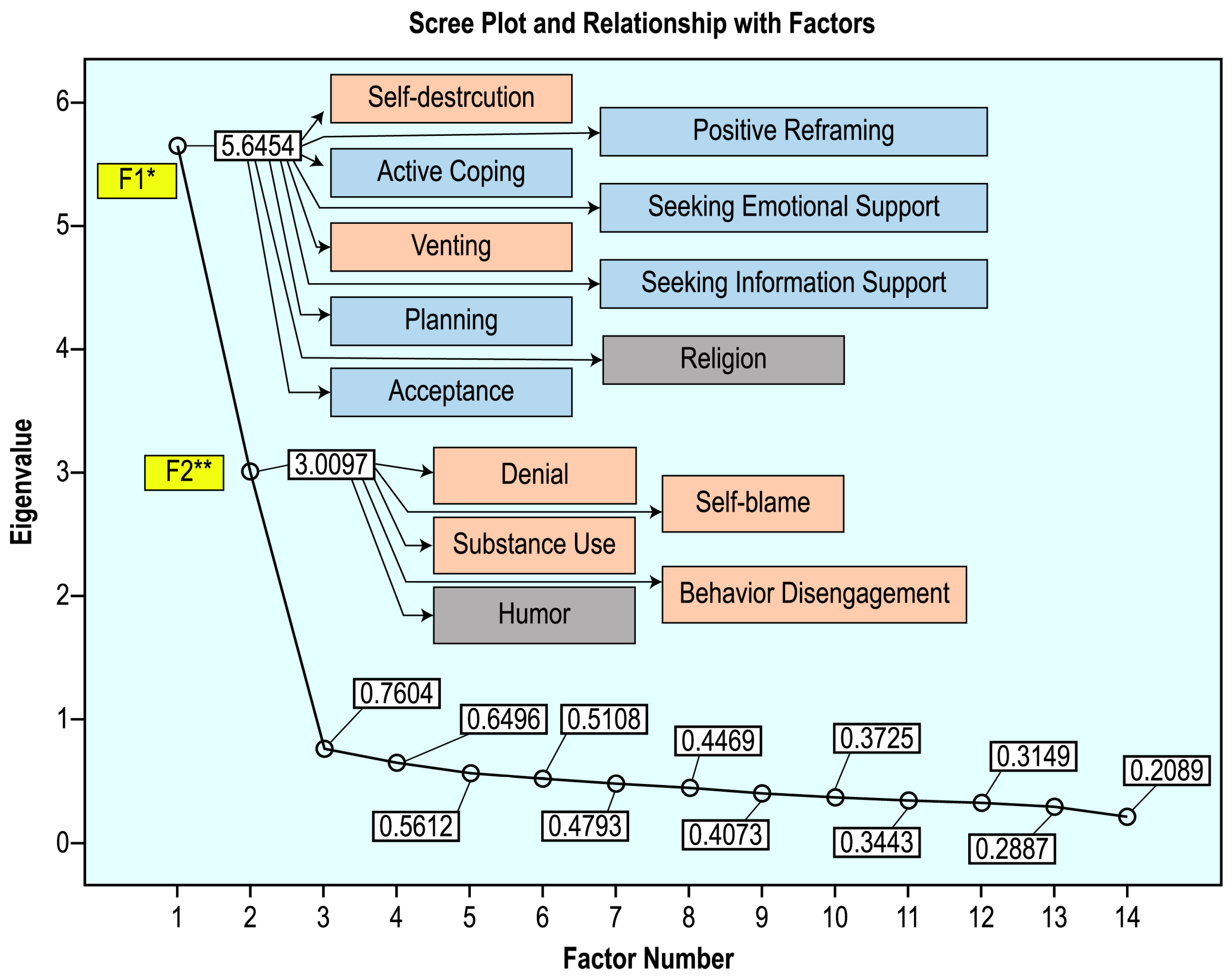
3.6. Exploratory Factor Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, A.; Sultana, M.; Hossain, S.; Hasan, M.; Ahmed, H.; Sikder, M. The impact of COVID-19 pandemic on mental health & wellbeing among home-quarantined Bangladeshi students: A cross-sectional pilot study. J. Affect. Disord. 2020, 277, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Bangladesh: WHO Coronavirus Disease (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/region/searo/country/bd/ (accessed on 21 March 2021).
- Ahmmed Sujan, M.; Islam, Z. Front Page. 2021. Available online: https://www.thedailystar.net/frontpage/news/number-critical-patients-surging-2059989 (accessed on 21 March 2021).
- Hossain, M.A.; Jahid, I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, O.; Kabir, F.; Arafat, S.M.Y.; Sakel, M.; Faruqui, R.; et al. Knowledge, attitudes, and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef] [PubMed]
- Hossain, K.; Roy, S.; Mosayed Ullah, M.; Kabir, R.; Arafat, S. COVID-19 and Mental Health Challenges in Bangladesh. Adv. Med. Dent. Health Sci. 2020, 3, 31–33. [Google Scholar] [CrossRef]
- Gurvich, C.; Thomas, N.; Thomas, E.H.; Hudaib, A.R.; Sood, L.; Fabiatos, K.; Sutton, K.; Isaacs, A.; Arunogiri, S.; Sharp, G.; et al. Coping styles and mental health in response to societal changes during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2021, 67, 540–549. [Google Scholar] [CrossRef]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Mamun, M.A.; Sakib, N.; Gozal, D.; Bhuiyan, A.I.; Hossain, S.; Doza, B.; Al Mamun, F.; Hosen, I.; Safiq, M.B.; Abdullah, A.H.; et al. The COVID-19 pandemic and serious psychological consequences in Bangladesh: A population-based nationwide study. J. Affect. Disord. 2020, 279, 462–472. [Google Scholar] [CrossRef]
- Xiang, Y.-T.; Yang, Y.; Li, W.; Zhang, L.; Zhang, Q.; Cheung, T.; Ng, C.H. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [Green Version]
- Jarus, O. 20 of the Worst Epidemics and Pandemics in History. 2021. Available online: https://www.livescience.com/worst-epidemics-and-pandemics-in-history.html (accessed on 21 March 2021).
- Ogueji, I.A.; Okoloba, M.M.; Demoko Ceccaldi, B.M. Coping strategies of individuals in the United Kingdom during the COVID-19 pandemic. Curr. Psychol. 2021, 41, 7493–7499. [Google Scholar] [CrossRef]
- Folkman, S. Stress: Appraisal and Coping. In Encyclopedia of Behavioral Medicine; Springer: Berlin/Heidelberg, Germany, 2013; pp. 1913–1915. [Google Scholar] [CrossRef]
- Brief-COPE—NovoPsych Psychometrics. 2021. Available online: https://novopsych.com.au/assessments/brief-cope/ (accessed on 21 March 2021).
- Protect Mental Health During COVID-19. 2021. Available online: https://www.who.int/bangladesh/emergencies/coronavirus-disease-(covid-19)-update/protect-mental-health-during-covid-19 (accessed on 21 March 2021).
- Shing, E.; Jayawickreme, E.; Waugh, C. Contextual Positive Coping as a Factor Contributing to Resilience After Disasters. J. Clin. Psychol. 2016, 72, 1287–1306. [Google Scholar] [CrossRef]
- Kehinde, T.; Eksin, E. How Fintech Can Help SMEs Rebuild after COVID-19. World Economic Forum. 2021. Available online: https://www.weforum.org/agenda/2020/05/fintech-can-help-smes-recover-covid-19/ (accessed on 21 March 2021).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Strobe Initiative. Strengthening the reporting of observational studies in Epidemiology (Strobe): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [Green Version]
- Carver, C. You want to measure coping but your protocol’ too long: Consider the brief cope. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- WMA—The World Medical Association-WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. 2021. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 21 March 2021).
- Live COVID Risk Test. 2021. Available online: https://livecoronatest.com/ (accessed on 21 March 2021).
- Carver, C.; Scheier, M.; Weintraub, J. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef] [PubMed]
- Laganà, L.; Zarankin, K. A cross-sectional study on health and physical functioning in relation to coping strategies among community-dwelling, ethnically diverse older women. BMC Women’s Health 2010, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Culver, J.; Arena, P.; Antoni, M.; Carver, C. Coping and distress among women under treatment for early stage breast cancer: Comparing african americans, hispanics and non-hispanic whites. Psycho-Oncology 2002, 11, 495–504. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.; Katona, C.; Orrell, M.; Livingston, G. Coping strategies, anxiety and depression in caregivers of people with Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2008, 23, 929–936. [Google Scholar] [CrossRef]
- Vosvick, M.; Koopman, C.; Gore-Felton, C.; Thoresen, C.; Krumboltz, J.; Spiegel, D. Relationship of Functional Quality of Life to Strategies for Coping With the Stress of Living With HIV/AIDS. Psychosomatics 2003, 44, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Mohanraj, R.; Jeyaseelan, V.; Kumar, S.; Mani, T.; Rao, D.; Murray, K.; Manhart, L.E. Cultural Adaptation of the Brief COPE for Persons Living with HIV/AIDS in Southern India. AIDS Behav. 2014, 19, 341–351. [Google Scholar] [CrossRef] [Green Version]
- Chodkiewicz, J.; Talarowska, M.; Miniszewska, J.; Nawrocka, N.; Bilinski, P. Alcohol Consumption Reported during the COVID-19 Pandemic: The Initial Stage. Int. J. Environ. Res. Public Health 2020, 17, 4677. [Google Scholar] [CrossRef]
- Bhui, K.; King, M.; Dein, S.; O’Connor, W. Ethnicity and religious coping with mental distress. J. Ment. Health 2008, 17, 141–151. [Google Scholar] [CrossRef]
- Grace, C.; Begum, R.; Subhani, S.; Kopelman, P.; Greenhalgh, T. Prevention of type 2 diabetes in British Bangladeshis: Qualitative study of community, religious, and professional perspectives. BMJ 2008, 337, a1931. [Google Scholar] [CrossRef] [Green Version]
- Haque, M.; Chowdhury, A.; Shahjahan, M.; Harun, M. Traditional healing practices in rural Bangladesh: A qualitative investigation. BMC Complement. Altern. Med. 2018, 18, 62. [Google Scholar] [CrossRef] [Green Version]
- Islam, J.Y.; Zaman, M.M.; Bhuiyan, M.R.; Hasan, M.; Ahsan, H.N.; Rahman, M.; Rahman, M.; Chowdhury, M.J. Alcohol consumption among adults in Bangladesh: Results from STEPS 2010. WHO South-East Asia J. Public Health 2017, 6, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Dewan, G.; Chowdhury, F.R. Alcohol use and alcohol use disorders in Bangladesh. Asia Pac. J. Med. Toxicol. 2015, 4, 83–90. [Google Scholar] [CrossRef]
- Myrick, J.; Nabi, R.; Eng, N. Consuming memes during the COVID pandemic: Effects of memes and meme type on COVID-related stress and coping efficacy. Psychol. Popul. Media 2021, 11, 316–323. [Google Scholar] [CrossRef]
- Kimemia, M.; Asner-Self, K.; Daire, A. An Exploratory Factor Analysis of the Brief COPE with a Sample of Kenyan Caregivers. Int. J. Adv. Couns. 2011, 33, 149–160. [Google Scholar] [CrossRef]
- Alam, S.; Arafat, S.; Hossain, K.; Sakel, M. COVID-19 impacts on Disability and Rehabilitation in Bangladesh. Bangladesh Physiother. J. 2020, 10, 2–5. [Google Scholar] [CrossRef]
- Hossain, K.M.A.; Walton, L.M.; Arafat, S.M.Y.; Maybee, N.; Sarker, R.H.; Ahmed, S.; Kabir, F. Expulsion from the Motherland: Association between Depression & Health-Related Quality of Life for Ethnic Rohingya Living with Refugee Status in Bangladesh. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 46–52. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Coping Domains | Coping Styles | Indicators |
|---|---|---|
| Avoidance coping (AVC) | Denial (D) | Question items 3 and 8 |
| Substance use (SU) | Question items 4 and 11 | |
| Venting (V) | Question items 9 and 21 | |
| Behavioral disengagement (BD) | Question items 6 and 16 | |
| Self-distraction (SD) | Question items 1 and 19 | |
| Self-blame (SB) | Question items 13 and 26 | |
| Approach coping (APC) | Active coping (AC) | Question items 2 and 7 |
| Positive reframing (PR) | Question items 12 and 17 | |
| Planning (P) | Question items 14 and 25 | |
| Acceptance (A) | Question items 20 and 24 | |
| Seeking emotional support (SES) | Question items 5 and 15 | |
| Seeking informational support (SIS) | Question items 10 and 23 | |
| Humor (H) | Humor (H) | Question items 18 and 28 |
| Religion (R) | Religion (R) | Question items 22 and 27 |
| Socio-Demographic Characteristics | Number of Participants, n (%) |
|---|---|
| Gender | |
| Male | 1068 (53.4) |
| Female | 933 (46.6) |
| Age | |
| Less than equal 25 years | 994 (49.7) |
| 26–37 years | 451 (22.5) |
| 38–49 years | 296 (14.8) |
| 50–61 years | 162 (8.1) |
| More than 61 years | 98 (4.9) |
| Marital status | |
| Unmarried | 1043 (52.1) |
| Married | 889(44.4) |
| Widowed and divorced | 69 (3.4) |
| Educational status | |
| No formal education | 81 (4) |
| Primary education | 190(9.5) |
| Secondary education | 325(16.2) |
| Higher secondary | 713 (35.6) |
| Bachelor’s degree | 508(25.4) |
| Master’s or above degree | 184 (9.2) |
| Occupation | |
| Government job | 117 (5.8) |
| Private job | 199 (9.9) |
| Farmer | 40 (2) |
| Business | 175 (8.7) |
| Student | 966(48.3) |
| Retired | 52(2.6) |
| Housewife | 359 (17.9) |
| Unemployed | 34 (1.7) |
| Others | 59 (2.9) |
| Living area | |
| Rural | 636 (31.8) |
| Urban | 1365 (68.2) |
| Tested COVID-19 | |
| Yes | 70 (3.5) |
| No | 1931 (96.5) |
| COVID-19-like symptoms | |
| Symptoms Present | 185 (9.2) |
| Symptoms Absent | 1816 (92.8) |
| COVID-19-positive among anyone around | |
| Yes | 387 (19.3) |
| No | 1614 (80.7) |
| Variables | Avoidance Mean ± SD | t/F | p-Value (2tailed) | Approach | t/Chi | p-Value (2tailed) | Humor | t/F | p-Value (2tailed) | Religion | t/F | p-Value (2tailed) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||||||
| Male Female | 21.39 ± 6.0 20.18 ± 5.9 | 4.80 a | 0.001 ** | 30.13 ± 8.7 29.49 ± 9.1 | 1.579 a | 0.114 | 2.82 ± 1.4 2.53 ± 1.9 | 4.7 a | 0.001 ** | 5.58 ± 1.9 5.70 ± 1.8 | −1.36 a | 0.174 |
| Age | ||||||||||||
| ≤25 26–37 38–49 50–61 >61 | 21.04 ± 6.42 0.52 ± 5.69 20.29 ± 5.61 21.00 ± 5.30 21.34 ± 5.80 | 1.397 b | 0.232 | 29.44 ± 8.99 29.77 ± 9.07 30.59 ± 9.15 31.10 ± 7.78 29.66 ± 8.99 | 1.835 b | 0.119 | 2.80 ± 1.49 2.57 ± 1.84 2.58 ± 1.22 2.59 ± 1.77 2.54 ± 1.24 | 3.41 b | 0.009 | 5.55 ± 1.91 5.51 ± 1.90 5.75 ± 1.88 5.92 ± 1.78 6.30 ± 1.76 | 5.21 b | 0.001 ** |
| Marital status | ||||||||||||
| Unmarried Married Widowed and divorced | 20.94 ± 6.3 20.51 ± 5.4 23.22 ± 8.1 | 6.83 b | 0.001 ** | 29.43 ± 8.9 30.34 ± 8.9 29.42 ± 8.2 | 2.531 b | 0.080 | 2.77 ± 1.4 2.54 ± 1.1 3.17 ± 1.8 | 11.89 b | 0.001 ** | 5.51 ± 1.9 5.76 ± 1.8 5.90 ± 1.6 | 5.00 b | 0.007 ** |
| Education | ||||||||||||
| No formal education Primary education Secondary education Higher secondary Bachelor’s degree Master’s and above degree | 22.02 ± 7.9 19.75 ± 5.7 20.56 ± 5.9 21.42 ± 6.3 20.29 ± 5.4 21.04 ± 5.76 | 4.22 b | 0.001 ** | 28.62 ± 10.9 28.45 ± 10.4 28.45 ± 8.7 30.19 ± 8.3 30.47 ± 9.1 31.07 ± 8.3 | 4.23 b | 0.001 ** | 3.25 ± 1.7 2.47 ± 1.0 2.58 ± 1.1 2.84 ± 1.5 2.50 ± 1.1 2.72 ± 1.4 | 8.07 b | 0.001 ** | 5.01 ± 2.2 5.26 ± 2.1 5.38 ± 1.8 5.75 ± 1.8 5.80 ± 1.8 5.88 ± 1.7 | 6.40 b | 0.001 ** |
| Occupation | ||||||||||||
| Government job Private job Farmer Business Student Retired Housewife Unemployed Others | 20.42 ± 5.7 20.31 ± 5.5 24.50 ± 6.3 20.90 ± 5.17 21.13 ± 6.3 21.85 ± 5.8 20.06 ± 5.74 20.62 ± 5.86 19.54 ± 5.8 | 3.67 b | 0.001 ** | 30.91 ± 9.1 30.65 ± 8.7 31.20 ± 9.3 30.07 ± 8.9 29.54 ± 8.8 31.15 ± 7.6 29.84 ± 9.2 28.88 ± 8.04 27.37 ± 9.6 | 1.42 b | 0.180 | 2.53 ± 1.2 2.50 ± 1.1 3.68 ± 1.6 2.58 ± 1.1 2.78 ± 1.4 2.50 ± 1.2 2.50 ± 1.2 2.74 ± 1.3 2.90 ± 1.7 | 5.21 b | 0.001 ** | 5.94 ± 1.8 5.80 ± 1.9 5.53 ± 1.8 5.45 ± 1.9 5.55 ± 1.9 6.29 ± 1.7 5.88 ± 1.8 5.24 ± 2.01 4.76 ± 1.8 | 4.40 b | 0.001 ** |
| Living area | ||||||||||||
| Rural Urban | 21.37 ± 6 20.57 ± 6 | 2.732 a | 0.006 ** | 30.98 ± 8.2 29.30 ± 9.2 | −3.944 a | 0.001 ** | 2.78 ± 1.43 2.64 ± 1.31 | −2.271 a | 0.023 * | 5.77 ± 1.85 5.58 ± 1.91 | −2.148 a | 0.032 * |
| Tested COVID | ||||||||||||
| Yes No | 21.93 ± 5.33 20.79 ± 6.07 | 1.562 a | 0.121 | 33.64 ± 7.13 29.72 ± 8.98 | 2.678 a | 0.007 ** | 2.76 ± 1.45 2.68 ± 1.35 | 0.461 a | 0.645 | 6.17 ± 1.45 5.62 ± 1.90 | 2.403 a | 0.016 * |
| COVID | ||||||||||||
| Symptoms Present No | 22.23 ± 4.52 20.68 ± 6.17 | 3.314 a | 0.001 ** | 34.15 ± 6.42 29.39 ± 9.05 | 6.962 a | 0.001 ** | 2.63 ± 1.23 2.69 ± 1.37 | −0.595 a | 0.552 | 6.23 ± 1.54 5.57 ± 1.91 | 5.168 a | 0.001 ** |
| COVID anyone around | ||||||||||||
| Yes No | 20.59 ± 4.20 20.88 ± 6.41 | −0.856 a | 0.392 | 22.97 ± 7.25 29.08 ± 9.15 | 7.796 a | 0.001 ** | 2.37 ± 0.96 2.76 ± 1.42 | −5.097 a | 0.001 ** | 6.12 ± 1.62 5.52 ± 1.93 | 5.669 a | 0.001 ** |
| Variables | Avoidance | Approach | Humor | Religion | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| χ2 | B | OR | p | χ2 | B | OR | p | χ2 | B | OR | p | χ2 | B | OR | p | |
| Male vs. Female | 67.93 | 0.135 | 0.874 | 0.003 ** | 31.9 | −0.135 | 0.874 | 0.003 ** | 25.49 | 0.135 | 0.874 | 0.003 ** | 3.335 | −0.135 | 0.874 | 0.003 ** |
| 18–35 vs. other age categories | 32.0 | −0.860 | 0.423 | 0.001 ** | 50.804 | 0.860 | 0.423 | 0.001 ** | 15.37 | −0.860 | 0.423 | 0.001 ** | 20.676 | −0.860 | 0.423 | 0.001 ** |
| Unmarried vs. others | 45.86 | −0.085 | 0.919 | 0.057 | 80.579 | −0.085 | 0.919 | 0.057 | 13.5 | −0.085 | 0.919 | 0.05 | 18.492 | −0.085 | 0.919 | 0.05 |
| Higher secondary and Bachelor vs. Other educational status | 61.0 | −0.448 | 0.639 | 0.001 ** | 67.403 | 0.448 | 0.639 | 0.001 ** | 13.47 | 0.448 | 0.639 | 0.001 ** | 5.62 | −0.448 | 0.639 | 0.001 ** |
| Student vs. Other occupation | 53.7 | 0.067 | 1.0 | 0.123 | 76.127 | 0.069 | 1.07 | 0.123 | 14.37 | 0.069 | 1.07 | 0.123 | 8.91 | 0.069 | 1.07 | 0.123 |
| Rural vs. Urban | 83.4 | −0.764 | 0.46 | 0.001 ** | 99.99 | −0.764 | 0.466 | 0.001 ** | 11.354 | −0.764 | 0.466 | 0.001 ** | 22.84 | −0.764 | 0.466 | 0.001 ** |
| Symptoms present vs. absent | 99.5 | 2.2 | 0.8 | 0.001 ** | 135.60 | 2.28 | 0.81 | 0.001 ** | 7.713 | 2.28 | 0.816 | 0.001 ** | 40.96 | 2.28 | 0.81 | 0.001 ** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hossain, K.M.A.; Shafin, R.; Yeasmin, M.H.; Jahid, I.K.; Hossain, M.A.; Rana, S.; Kabir, M.F.; Chokrovorty, S.K.; Faruqui, R. Community Coping Strategies for COVID-19 in Bangladesh: A Nationwide Cross-Sectional Survey. COVID 2023, 3, 320-335. https://doi.org/10.3390/covid3030024
Hossain KMA, Shafin R, Yeasmin MH, Jahid IK, Hossain MA, Rana S, Kabir MF, Chokrovorty SK, Faruqui R. Community Coping Strategies for COVID-19 in Bangladesh: A Nationwide Cross-Sectional Survey. COVID. 2023; 3(3):320-335. https://doi.org/10.3390/covid3030024
Chicago/Turabian StyleHossain, K. M. Amran, Rubayet Shafin, Mst. Hosneara Yeasmin, Iqbal Kabir Jahid, Mohammad Anwar Hossain, Shohag Rana, Mohammad Feroz Kabir, Sanjit Kumar Chokrovorty, and Rafey Faruqui. 2023. "Community Coping Strategies for COVID-19 in Bangladesh: A Nationwide Cross-Sectional Survey" COVID 3, no. 3: 320-335. https://doi.org/10.3390/covid3030024