


Infection Prevention and Control in Public Hospitals and COVID-19 Temporary Treatment and Monitoring Facilities in the Philippines: Results of a Baseline Survey
 ,
,
Abstract
:1. Introduction
1.1. Challenges in IPC Implementation
1.2. Rapid IPC Assessment
2. Methods
2.1. Study Population and Period
2.2. Data Collection
2.3. Data Processing and Analysis
2.4. Public Participation and Involvement
3. Results
3.1. Characteristics of Surveyed Facilities
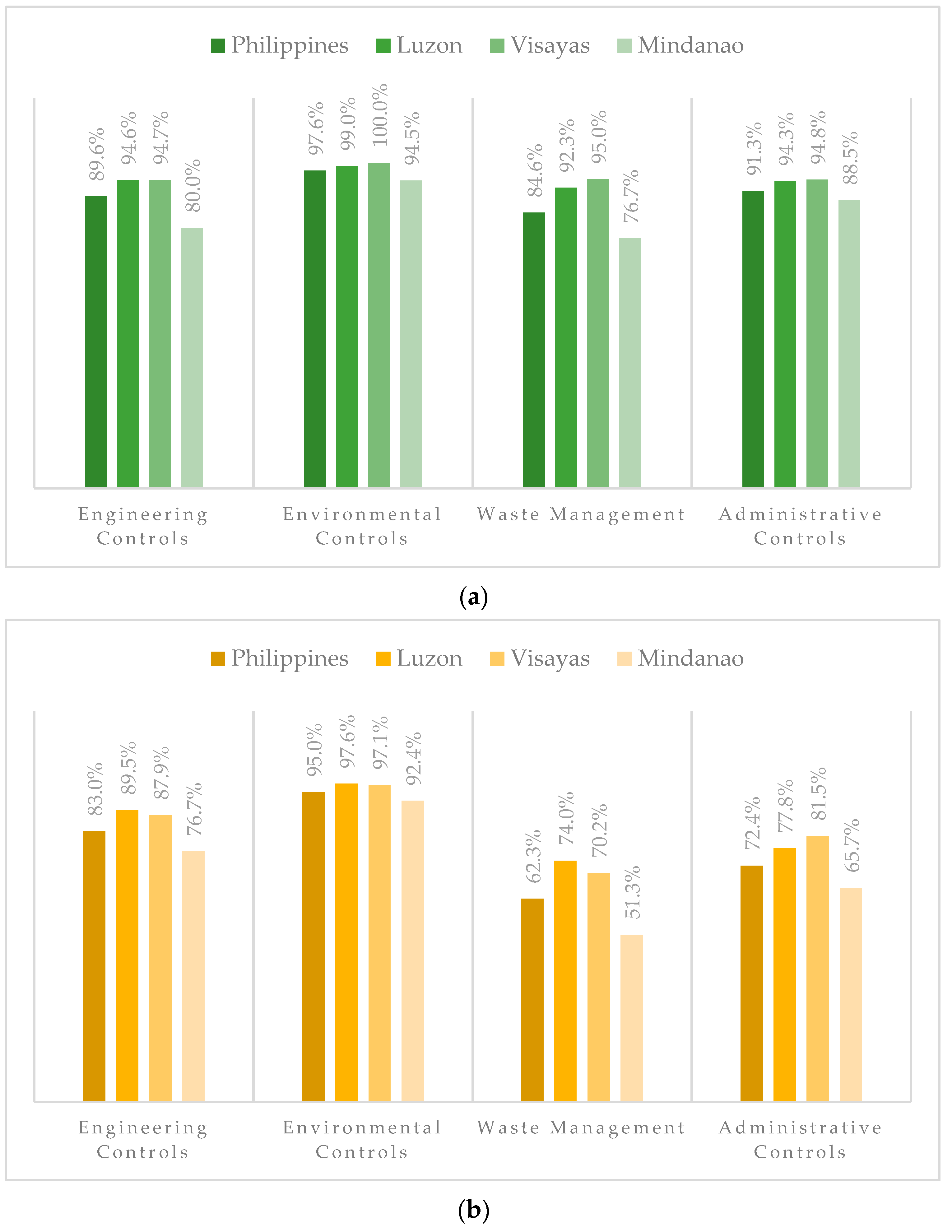
3.2. Compliance with COVID-19 IPC Standards
3.2.1. Engineering and Environmental Controls
3.2.2. Waste Management
3.2.3. Administrative Controls
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.; Lau, E.H.; Wong, J.Y.; et al. Early transmission dynamics in Wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 2 February 2023).
- Chu, D.T.; Vu Ngoc, S.M.; Vu Thi, H.; Nguyen Thi, Y.V.; Ho, T.T.; Hoang, V.T.; Singh, V.; Al-Tawfiq, J.A. COVID-19 in Southeast Asia: Current status and perspectives. Bioengineered 2022, 13, 3797–3809. [Google Scholar] [CrossRef] [PubMed]
- Edrada, E.M.; Lopez, E.B.; Villarama, J.B.; Salva-Villarama, E.P.; Dagoc, B.F.; Smith, C.; Sayo, A.R.; Verona, J.A.; Trifalgar-Arches, J.; Lazaro, J.; et al. First COVID-19 infections in the Philippines: A case report. Trop. Med. Health 2020, 48, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health. Philippines COVID-19 Tracker. Available online: https://doh.gov.ph/covid19tracker (accessed on 31 December 2021).
- Lai, X.; Wang, M.; Qin, C.; Tan, L.; Ran, L.; Chen, D.; Zhang, H.; Shang, K.; Xia, C.; Wang, S.; et al. Coronavirus disease 2019 (COVID-2019) infection among health care workers and implications for prevention measures in a tertiary hospital in Wuhan, China. JAMA Netw. Open 2020, 3, e209666. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Workers: A Global Profile. 2020. Available online: https://www.who.int/whr/2006/06_chap1_en.pdf (accessed on 31 December 2021).
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, A.M.; Lazaro, J.; Sayo, A.R.; Han, S.M.; Ukawa, T.; Suzuki, S.; Takaya, S.; Telan, E.; Solante, R.; Ariyoshi, K.; et al. COVID-19 screening for healthcare workers in a tertiary infectious diseases referral hospital in Manila, the Philippines. Am. J. Trop. Med. Hyg. 2020, 103, 1211. [Google Scholar] [CrossRef]
- Agrupis, K.A.; Smith, C.; Suzuki, S.; Villanueva, A.M.; Ariyoshi, K.; Solante, R.; Telan, E.F.; Estrada, K.A.; Uichanco, A.C.; Sagurit, J.; et al. Epidemiological and clinical characteristics of the first 500 confirmed COVID-19 inpatients in a tertiary infectious disease referral hospital in Manila, Philippines. Trop. Med. Health 2021, 49, 48. [Google Scholar] [CrossRef]
- Morales, N.J.; Lema, K. Philippine Medical Workers under Strain as COVID-19 Cases Jump. Reuters, 13 August 2021. Available online: https://www.reuters.com/world/asia-pacific/philippines-extends-travel-ban-10-countries-over-delta-concerns-2021-08-13/(accessed on 31 December 2021).
- World Health Organization. Guidelines on Core Components of Infection Prevention and Control Programmes at the National and Acute Health Care Facility Level; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Zhang, L.; Welsch, R.E.; Cao, Z. The transmission, infection prevention, and control during the COVID-19 Pandemic in China: A retrospective study. Int. J. Environ. Res. Public Health 2022, 19, 3074. [Google Scholar] [CrossRef]
- World Health Organization. Improving Infection Prevention and Control at the HEALTH Facility: Interim Practical Manual Supporting the Implementation of the WHO Guidelines on Core Components of Infection Prevention and Control Programmes; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Pradhan, D.; Biswasroy, P.; Naik, P.K.; Ghosh, G.; Rath, G. A review of current interventions for COVID-19 prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef]
- Shbaklo, N.; Lupia, T.; De Rosa, F.G.; Corcione, S. Infection Control in the Era of COVID-19: A Narrative Review. Antibiotics 2021, 10, 1244. [Google Scholar] [CrossRef]
- Maina, M.; Tosas-Auguet, O.; English, M.; Schultsz, C.; McKnight, J. Infection prevention and control during the COVID-19 pandemic: Challenges and opportunities for Kenyan public hospitals. Wellcome Open Res. 2020, 5, 211. [Google Scholar] [CrossRef] [PubMed]
- Tartari, E.; Hopman, J.; Allegranzi, B.; Gao, B.; Widmer, A.; Cheng, V.C.; Wong, S.C.; Marimuthu, K.; Ogunsola, F.; Voss, A. Perceived challenges of COVID-19 infection prevention and control preparedness: A multinational survey. J. Glob. Antimicrob. Resist. 2020, 22, 779. [Google Scholar] [CrossRef] [PubMed]
- Harun, M.G.; Anwar, M.M.; Sumon, S.A.; Hassan, M.Z.; Haque, T.; Mah-E-Muneer, S.; Rahman, A.; Abdullah, S.A.; Islam, M.S.; Styczynski, A.R.; et al. Infection prevention and control in tertiary care hospitals of Bangladesh: Results from WHO infection prevention and control assessment framework (IPCAF). Antimicrob. Resist. Infect. Control 2022, 11, 125. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. National Standards in Infection Control for Healthcare Facilities. Available online: https://doh.gov.ph/sites/default/files/publications/NATIONAL_STANDARDS_IN_INFECTION_CONTROL_FOR_HEALTH.pdf (accessed on 31 December 2021).
- Department of Health. Department Memorandum No. 2020-0208: Interim Guidelines on Enhancing the Infection Prevention and Control Measures through Engineering and Environmental Controls in all Health Facilities and Temporary Treatment and Monitoring Facilities during the COVID-19 Pandemic. Available online: https://doh.gov.ph/sites/default/files/health-update/dm2020-0208.pdf (accessed on 31 December 2021).
- Department of Health. Department Circular No. 2020-0225: Advisory on the Use of the Infection Prevention and Control Checklist for Temporary Treatment and Monitoring Facilities (TTMF). Available online: https://dmas.doh.gov.ph:8083/Rest/GetFile?id=654432 (accessed on 31 December 2021).
- Department of Health. Department Memorandum No. 2020-0170: Interim Guidelines on the Management of Health Care Waste in Health Facilities, Community Quarantine Units, and Temporary Treatment and Monitoring Facilities with Cases of Coronavirus Disease 2019 (COVID-19). Available online: https://doh.gov.ph/sites/default/files/health-update/dm2020-0170.pdf (accessed on 31 December 2021).
- World Health Organization. Infection Prevention and Control during Health Care when Coronavirus Disease (COVID-19) is Suspected or Confirmed: Interim Guidance, 12 July 2021. WHO. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-IPC-2021.1 (accessed on 31 December 2021).
- Storr, J.; Twyman, A.; Zingg, W.; Damani, N.; Kilpatrick, C.; Reilly, J.; Price, L.; Egger, M.; Grayson, M.L.; Kelley, E.; et al. Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrob. Resist. Infect. Control 2017, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.H.; Lee, G.A.; Lee, S.H.; Park, Y.H. Effectiveness and core components of infection prevention and control programmes in long-term care facilities: A systematic review. J. Hosp. Infect. 2019, 102, 377–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health. Department Memorandum No. 2020-0123: Interim Guidelines on the Management of Surge Capacity through Conversion of Public Spaces to Operate as Temporary Treatment and Monitoring Facilities for the Management of Persons under Investigation and Mild Cases of COVID-19. Available online: https://doh.gov.ph/sites/default/files/health-update/dm2020-0123.pdf (accessed on 31 December 2021).
- Department of Health. Department Memorandum No. 2020-0186: Interim Guidelines on the Operations of Converted Public and Private Spaces into Temporary Treatment and Monitoring Facilities for COVID-19. Available online: https://doh.gov.ph/sites/default/files/health-update/dm2020-0186.pdf (accessed on 31 December 2021).
- Ogawa, F.; Kato, H.; Sakai, K.; Nakamura, K.; Ogawa, M.; Uchiyama, M.; Nakajima, K.; Ohyama, Y.; Abe, T.; Takeuchi, I. Environmental maintenance with effective and useful zoning to protect patients and medical staff from COVID-19 infection. Acute Med. Surg. 2020, 7, e536. [Google Scholar] [CrossRef]
- Gullapalli, N.; Lim, Z.J.; Ramanathan, K.; Bihari, S.; Haji, J.; Shekar, K.; Wong, W.T.; Rajamani, A.; Subramaniam, A. Personal protective equipment preparedness in intensive care units during the coronavirus disease 2019 pandemic: An Asia-Pacific follow-up survey. Aust. Crit. Care 2022, 35, 5–12. [Google Scholar] [CrossRef]
- Emmanuel, U.; Osondu, E.D.; Kalu, K.C. Architectural design strategies for infection prevention and control (IPC) in health-care facilities: Towards curbing the spread of Covid-19. J. Environ. Health Sci. Eng. 2020, 18, 1699–1707. [Google Scholar] [CrossRef]
- Das, A.K.; Islam, M.N.; Billah, M.M.; Sarker, A. COVID-19 pandemic and healthcare solid waste management strategy–A mini-review. Sci. Total Environ. 2021, 778, 146220. [Google Scholar] [CrossRef]
- Sangkham, S. Face mask and medical waste disposal during the novel COVID-19 pandemic in Asia. Case Studies Chem. Environ. Eng. 2020, 2, 100052. [Google Scholar] [CrossRef]
- Hantoko, D.; Li, X.; Pariatamby, A.; Yoshikawa, K.; Horttanainen, M.; Yan, M. Challenges and practices on waste management and disposal during COVID-19 pandemic. J. Environ. Manag. 2021, 286, 112140. [Google Scholar] [CrossRef]
- Houghton, C.; Meskell, P.; Delaney, H.; Smalle, M.; Glenton, C.; Booth, A.; Chan, X.H.; Devane, D.; Biesty, L.M. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: A rapid qualitative evidence synthesis. Cochrane Database Syst. Rev. 2020, 4, CD013582. [Google Scholar]
- Mae, S.A.; Angelo, T.A. Factors affecting compliance to COVID-19 infection prevention and control measures and its effects on the risk of COVID-19 infection among physicians in a tertiary government hospital. Respirology 2021, 26 (Suppl 3), 15–16. [Google Scholar]
- Flores, J.M.; Borbe, M.M. Knowledge, attitude, and practices toward COVID-19 and infection prevention and control among tertiary level hospital labor and delivery room healthcare workers in time of pandemic: A cross-sectional survey. Philipp. J. Obstet. Gynecol. 2022, 46, 1–11. [Google Scholar] [CrossRef]
- Sastry, S.; Masroor, N.; Bearman, G.; Hajjeh, R.; Holmes, A.; Memish, Z.; Lassmann, B.; Pittet, D.; Macnab, F.; Kamau, R.; et al. The 17th International Congress on Infectious Diseases workshop on developing infection prevention and control resources for low-and middle-income countries. Int. J. Infect. Dis. 2017, 57, 138–143. [Google Scholar] [CrossRef] [Green Version]
- Qureshi, M.O.; Chughtai, A.A.; Seale, H. Recommendations related to occupational infection prevention and control training to protect healthcare workers from infectious diseases: A scoping review of infection prevention and control guidelines. BMC Health Serv. Res. 2022, 22, 272. [Google Scholar] [CrossRef]
- Antommaria, A.H.M. Conflicting duties and reciprocal obligations during a pandemic. J. Hosp. Med. 2020, 15, 285. [Google Scholar] [CrossRef] [Green Version]
- Risko, N.; Werner, K.; Offorjebe, O.A.; Vecino-Ortiz, A.I.; Wallis, L.A.; Razzak, J. Cost-effectiveness and return on investment of protecting health workers in low-and middle-income countries during the COVID-19 pandemic. PLoS ONE 2020, 15, e0240503. [Google Scholar] [CrossRef]
- Angrup, A.; Kanaujia, R.; Ray, P.; Biswal, M. Healthcare facilities in low-and middle-income countries affected by COVID-19: Time to upgrade basic infection control and prevention practices. Indian J. Med. Microbiol. 2020, 38, 139–143. [Google Scholar] [CrossRef]
- Cooper, S.; Wiyeh, A.; Schmidt, B.M.; Wiysonge, C.S. Cochrane corner: Factors that influence compliance by healthcare workers with infection prevention and control guidelines for COVID-19 and other respiratory infections. Pan Afr. Med. J. 2020, 35, 23. [Google Scholar] [CrossRef]
- Gilmore, B.; Ndejjo, R.; Tchetchia, A.; De Claro, V.; Mago, E.; Lopes, C.; Bhattacharyya, S. Community engagement for COVID-19 prevention and control: A rapid evidence synthesis. BMJ Glob. Health 2020, 5, e003188. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | No. of Respondents n (%) | Comparison between Island Groups | ||
|---|---|---|---|---|
| Luzon | Visayas | Mindanao | ||
| Public hospitals | 83 (100.0) | 39 (47.0) | 15 (18.1) | 29 (34.9) |
| Respondents by profession: | ||||
| Chief of hospital | 9 (10.8) | 2 (5.1) | 3 (20.0) | 4 (13.8) |
| IPC physician | 3 (3.6) | 2 (5.1) | 1 (6.7) | - |
| IPC nurse | 53 (63.9) | 26 (66.7) | 6 (40.0) | 23 (79.3) |
| IPC officer | 7 (8.4) | 4 (10.3) | 3 (20.0) | - |
| Other professionals | 11 (13.3) | 5 (12.8) | 2 (13.3) | 2 (6.9) |
| Facility certification | ||||
| DOH licensed | 83 (100.0) | 39 (100.0) | 15 (100.0) | 29 (100.0) |
| PhilHealth accredited | 78 (94.0) | 39 (100.0) | 14 (93.3) | 25 (86.2) |
| TTMFs | 139 (100.0) | 50 (36.0) | 21 (15.1) | 68 (48.9) |
| Respondents by profession: | ||||
| Facility manager | 32 (23.0) | 6 (12.0) | 4 (19.0) | 22 (32.4) |
| IPC physician | 25 (18.0) | 9 (18.0) | 5 (23.8) | 11 (16.2) |
| IPC nurse | 49 (35.3) | 18 (36.0) | 10 (47.6) | 21 (30.9) |
| Other professionals | 33 (23.7) | 17 (34.0) | 2 (9.5) | 14 (20.6) |
| Facility certification | ||||
| DOH licensed | 76 (54.7) | 24 (48.0) | 13 (61.9) | 38 (55.9) |
| PhilHealth accredited | 27 (19.4) | 7 (14.0) | 13 (61.9) | 7 (10.3) |
| Domain/Standards | No. of Respondents n (%) | Comparison between Island Groups | |||
|---|---|---|---|---|---|
| Luzon | Visayas | Mindanao | p-Value | ||
| Engineering Controls | |||||
| Triage area has hand hygiene area | 81 (97.6) | 39 (100.0) | 15 (100.0) | 26 (89.7) | 0.005 |
| Triage area has directional signage | 66 (79.5) | 35 (89.7) | 14 (93.3) | 17 (58.6) | 0.003 |
| HCWs wearing proper PPE | 80 (96.4) | 39 (100.0) | 15 (100.0) | 26 (89.7) | 0.005 |
| Cleaners are wearing proper PPE | 79 (95.2) | 37 (94.9) | 15 (100.0) | 27 (93.1) | 0.010 |
| Emergency room isolation has contaminated zone | 76 (91.6) | 37 (94.9) | 14 (93.3) | 25 (86.2) | 0.005 |
| Emergency room isolation has buffer zone | 76 (91.6) | 37 (94.9) | 15 (100.0) | 24 (82.8) | 0.008 |
| Emergency room isolation has sterile zone | 74 (89.2) | 37 (94.9) | 13 (86.7) | 24 (82.8) | 0.003 |
| COVID-19 isolation ward has contaminated zone | 71 (85.5) | 36 (92.3) | 14 (93.3) | 21 (72.4) | 0.005 |
| COVID-19 isolation ward has buffer zone | 71 (85.5) | 36 (92.3) | 14 (93.3) | 21 (72.4) | 0.005 |
| COVID-19 isolation ward has sterile zone | 70 (84.3) | 36 (92.3) | 13 (86.7) | 21 (72.4) | 0.003 |
| Environmental Controls | |||||
| Cleaning and disinfection of surface areas once a day | 82 (98.8) | 38 (97.4) | 15 (100.0) | 29 (100.0) | 0.007 |
| Cleaning and disinfection upon discharge of patient | 82 (98.8) | 39 (100.0) | 15 (100.0) | 28 (96.6) | 0.005 |
| Use of 70% ethyl alcohol or 0.1% sodium hypochlorite to disinfect surfaces | 81 (97.6) | 39 (100.0) | 15 (100.0) | 27 (93.1) | 0.005 |
| Use of 0.5% sodium hypochlorite to clean bodily fluids | 78 (93.9) | 38 (97.4) | 15 (100.0) | 25 (86.2) | 0.006 |
| Compliance with ≥30 min standard waiting time for disinfection | 82 (98.8) | 39 (100.0) | 15 (100.0) | 28 (96.6) | 0.005 |
| Waste Management | |||||
| Appropriate labeling of waste bins | 79 (95.2) | 39 (100.0) | 15 (100.0) | 27 (93.1) | 0.005 |
| Use of color-coded bags | 58 (69.9) | 27 (69.2) | 15 (100.0) | 16 (55.2) | 0.101 |
| Presence of posters/printed instructions for disposal | 69 (83.1) | 36 (92.3) | 14 (93.3) | 19 (65.5) | 0.003 |
| Designated temporary collection point for infectious waste | 76 (91.6) | 37 (94.9) | 13 (86.7) | 28 (96.6) | 0.004 |
| Temporary collection point is covered/sealed | 74 (89.2) | 37 (94.9) | 13 (86.7) | 26 (89.7) | 0.003 |
| Temporary collection point is far from public access | 79 (95.2) | 39 (100.0) | 15 (100.0) | 27 (93.1) | 0.002 |
| Central storage for infectious waste | 58 (69.9) | 27 (69.2) | 15 (100.0) | 16 (55.2) | 0.005 |
| Central storage is proximate to exit gate/garbage pick-up | 69 (83.1) | 36 (92.3) | 14 (93.3) | 19 (65.5) | 0.004 |
| Administrative Controls | |||||
| Written policy on IPC | 74 (89.2) | 37 (94.9) | 13 (86.7) | 26 (89.7) | 0.005 |
| Dedicated IPC Officer | 75 (90.4) | 37 (94.9) | 12 (80.0) | 28 (96.6) | 0.007 |
| HCWs trained in IPC | 81 (97.6) | 39 (100.0) | 15 (100.0) | 29 (100.0) | 0.007 |
| Familiarity with the steps to proper handwashing | 78 (94.0) | 38 (97.4) | 14 (93.3) | 28 (96.6) | 0.007 |
| Familiarity with the steps to proper donning of PPE | 81 (97.6) | 38 (97.4) | 15 (100.0) | 28 (96.6) | 0.007 |
| Familiarity with the steps to proper doffing of PPE | 81 (97.6) | 38 (97.4) | 15 (100.0) | 28 (96.6) | 0.007 |
| Promotional materials on proper handwashing | 74 (89.2) | 39 (100.0) | 15 (100.0) | 20 (86.9) | 0.002 |
| Promotional materials on respiratory etiquette and physical distancing | 72 (86.7) | 32 (82.1) | 15 (100.0) | 25 (86.2) | 0.048 |
| Promotional materials on use of PPE per zone | 66 (79.5) | 33 (84.6) | 14 (93.3) | 19 (65.5) | 0.012 |
| Domain/Standards | No. of Respondents n (%) | Comparison between Island Groups | |||
|---|---|---|---|---|---|
| Luzon | Visayas | Mindanao | p-Value | ||
| Engineering Controls | |||||
| Entrance and exit for HCWs are connected to clean/sterile area | 116 (83.5) | 47 (94.0) | 20 (95.2) | 49 (72.1) | <0.001 |
| Entrance and exit for HCWs have directional signage | 68 (48.9) | 29 (58.0) | 14 (66.7) | 25 (36.8) | 0.069 |
| Entrance and exit for patients are connected to contaminated area | 115 (82.7) | 45 (90.0) | 19 (90.5) | 51 (75.0) | <0.001 |
| Entrance and exit for patients have directional signage | 68 (48.9) | 30 (60.0) | 14 (66.7) | 24 (35.3) | 0.056 |
| Use of the following PPE by HCWs: | |||||
| Face mask | 128 (92.1) | 48 (96.0) | 20 (95.2) | 60 (88.2) | <0.001 |
| Eye protection | 134 (96.4) | 50 (100.0) | 20 (95.2) | 64 (94.1) | <0.001 |
| Gloves | 133 (95.7) | 50 (100.0) | 20 (95.2) | 63 (92.6) | <0.001 |
| Gown | 127 (91.4) | 49 (98.0) | 18 (85.7) | 60 (88.2) | <0.001 |
| Has a designated contaminated zone | 129 (92.8) | 48 (96.0) | 20 (95.2) | 61 (89.7) | <0.001 |
| Has a designated buffer zone | 127 (91.4) | 49 (98.0) | 19 (90.5) | 59 (86.8) | <0.001 |
| Has a designated sterile zone | 124 (89.2) | 47 (94.0) | 19 (90.5) | 58 (85.3) | <0.001 |
| Environmental Controls | |||||
| Cleaning and disinfection of surface areas daily | 134 (96.4) | 49 (98.0) | 19 (90.5) | 66 (97.1) | <0.001 |
| Cleaning and disinfection upon discharge of patient | 139 (100.0) | 50 (100.0) | 21 (100.0) | 68 (100.0) | <0.001 |
| Use of 70% ethyl alcohol or 0.1% sodium hypochlorite to disinfect surfaces | 135 (97.1) | 50 (100.0) | 20 (95.2) | 65 (95.6) | <0.001 |
| Use of 0.5% sodium hypochlorite to clean bodily fluids | 122 (87.8) | 47 (94.0) | 21 (100.0) | 54 (79.4) | <0.001 |
| Compliance with ≥30 min standard waiting time for disinfection | 130 (93.5) | 48 (96.0) | 21 (100.0) | 61 (89.7) | <0.001 |
| Waste Management | |||||
| Appropriate labeling of waste bins | 87 (62.2) | 39 (78.0) | 16 (76.2) | 32 (47.1) | 0.008 |
| Use of color-coded bags | 46 (33.1) | 20 (40.0) | 12 (57.1) | 14 (20.6) | 0.323 |
| Presence of posters/printed instructions for disposal | 47 (33.8) | 27 (54.0) | 7 (33.3) | 13 (19.1) | <0.001 |
| Designated temporary collection point for infectious waste | 114 (82.0) | 46 (92.0) | 18 (85.7) | 50 (73.5) | <0.001 |
| Temporary collection point is covered/sealed | 98 (70.5) | 39 (78.0) | 16 (76.2) | 43 (63.2) | 0.002 |
| Temporary collection point is far from public access | 102 (73.4) | 41 (82.0) | 17 (81.0) | 44 (64.7) | 0.002 |
| Central storage for infectious waste | 97 (69.8) | 42 (84.0) | 15 (71.4) | 40 (58.8) | <0.001 |
| Central storage is proximate to exit gate/garbage pick-up | 102 (73.4) | 42 (84.0) | 17 (81.0) | 43 (63.2) | 0.002 |
| Administrative Controls | |||||
| Written policy on IPC | 82 (58.9) | 25 (50.0) | 10 (47.6) | 47 (69.1) | <0.001 |
| Dedicated IPC Officer | 114 (82.0) | 48 (96.0) | 19 (90.5) | 47 (69.1) | <0.001 |
| HCWs trained in IPC | 114 (82.0) | 42 (84.0) | 17 (80.9) | 55 (80.9) | <0.001 |
| Familiarity with the steps to proper handwashing | 133 (95.7) | 50 (100.0) | 21 (100.0) | 62 (91.2) | <0.001 |
| Familiarity with the steps to proper donning of PPE | 132 (94.9) | 48 (96.0) | 21 (100.0) | 63 (92.6) | <0.001 |
| Familiarity with the steps to proper doffing of PPE | 133 (95.7) | 49 (98.0) | 21 (100.0) | 63 (92.6) | <0.001 |
| Promotional materials on proper handwashing | 78 (56.1) | 35 (70.0) | 18 (85.7) | 25 (36.8) | 0.060 |
| Promotional materials on respiratory etiquette and physical distancing | 58 (41.7) | 27 (54.0) | 14 (66.7) | 17 (25.0) | 0.091 |
| Promotional/educational materials on use of PPE per zone | 62 (44.6) | 26 (52.0) | 13 (61.9) | 23 (33.8) | 0.106 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Claro, V.; Bautista, N.; Torralba, M.R.; Castro, V.V.; Lucero, M.A.; Molleno, L.J.; Stan, L. Infection Prevention and Control in Public Hospitals and COVID-19 Temporary Treatment and Monitoring Facilities in the Philippines: Results of a Baseline Survey. COVID 2023, 3, 336-347. https://doi.org/10.3390/covid3030025
de Claro V, Bautista N, Torralba MR, Castro VV, Lucero MA, Molleno LJ, Stan L. Infection Prevention and Control in Public Hospitals and COVID-19 Temporary Treatment and Monitoring Facilities in the Philippines: Results of a Baseline Survey. COVID. 2023; 3(3):336-347. https://doi.org/10.3390/covid3030025
Chicago/Turabian Stylede Claro, Vergil, Noemi Bautista, Ma. Rosario Torralba, Vina Vanessa Castro, Miguel Angelo Lucero, Lady Jedfeliz Molleno, and Laurentiu Stan. 2023. "Infection Prevention and Control in Public Hospitals and COVID-19 Temporary Treatment and Monitoring Facilities in the Philippines: Results of a Baseline Survey" COVID 3, no. 3: 336-347. https://doi.org/10.3390/covid3030025