
Antibody Titer Prediction from Serum Immunodiffusion Test of Patients with Paracoccidioidomycosis Using Infrared Spectroscopy and Chemometrics

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Serum Samples
2.2. FTIR-ATR Analysis
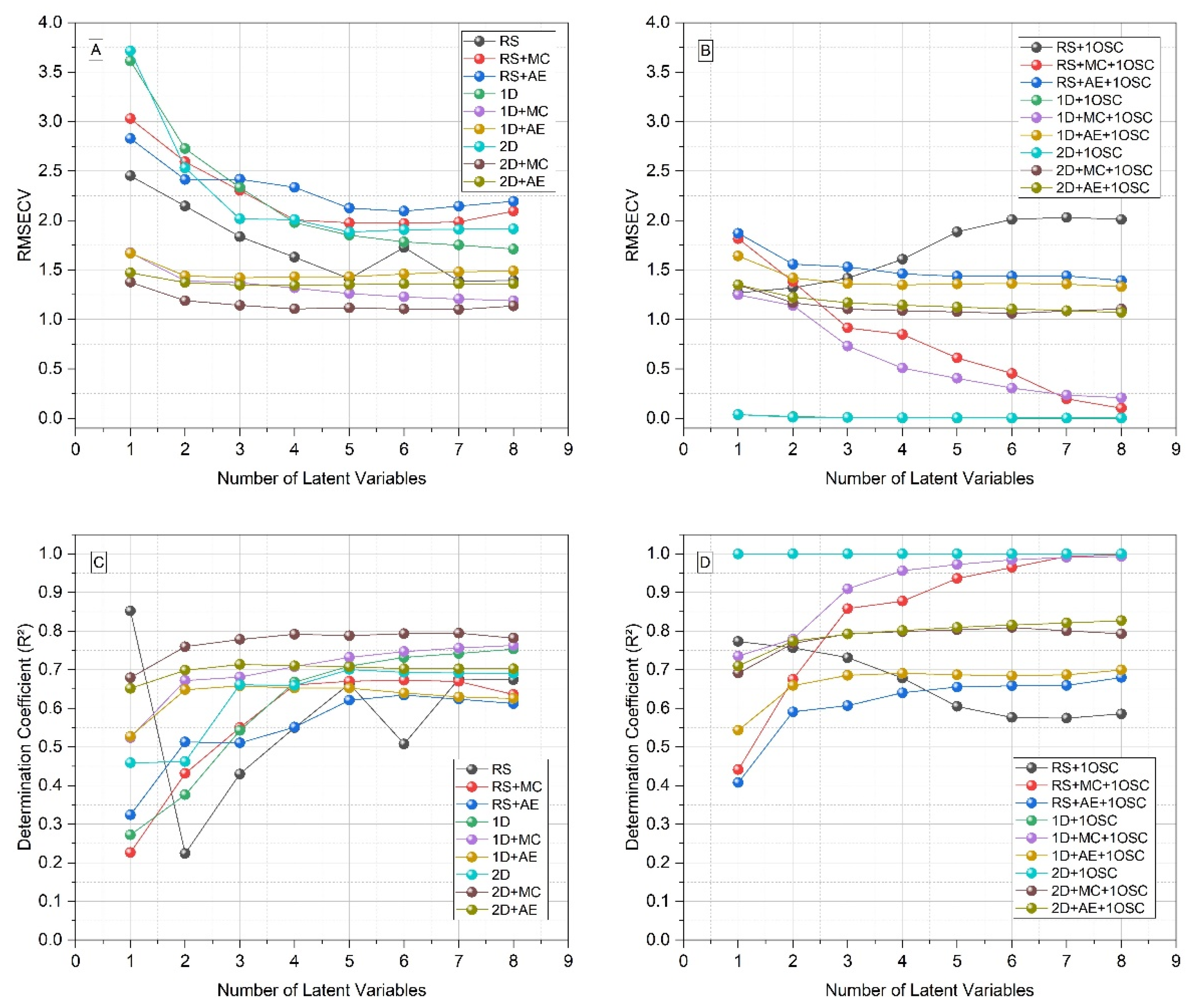
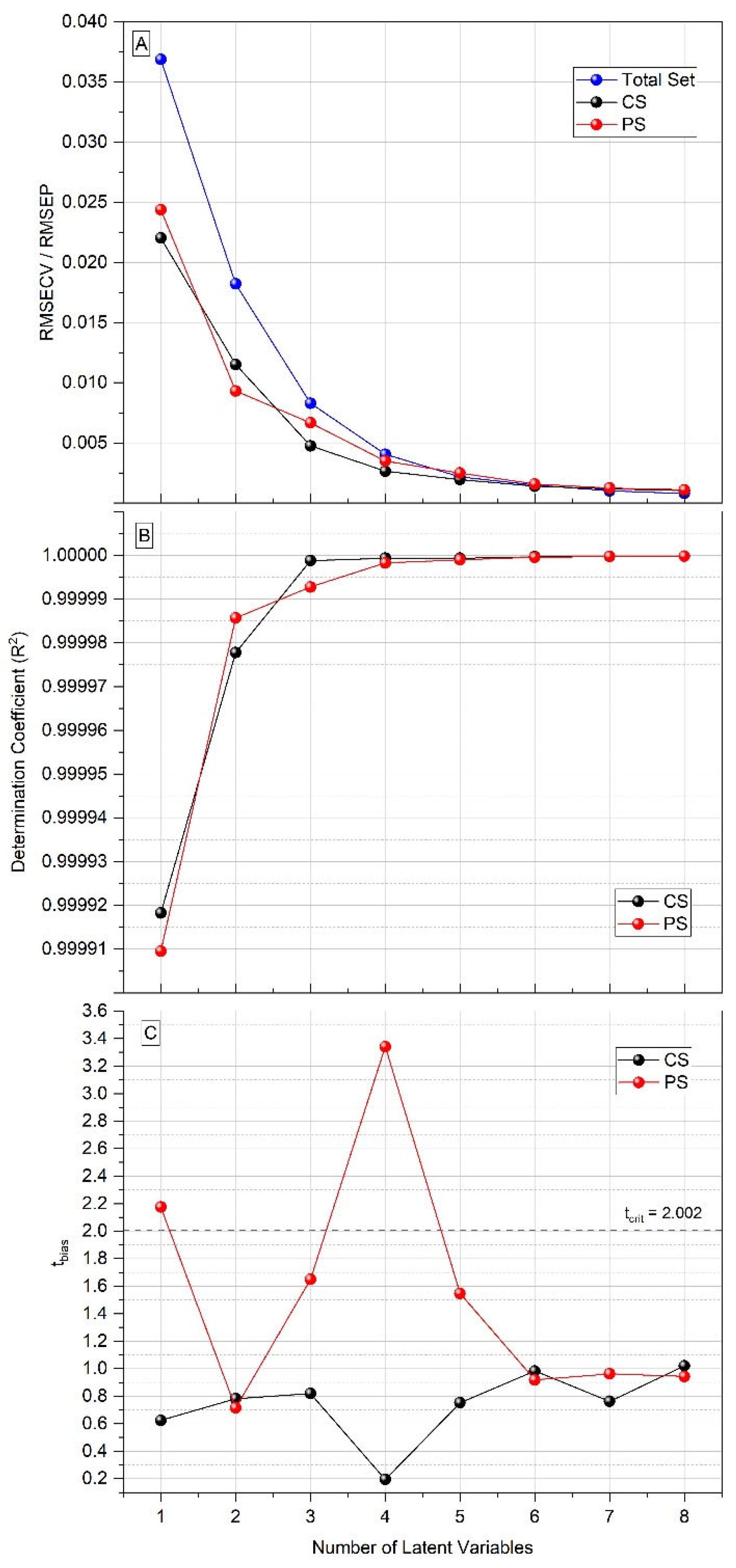
2.3. Chemometrics
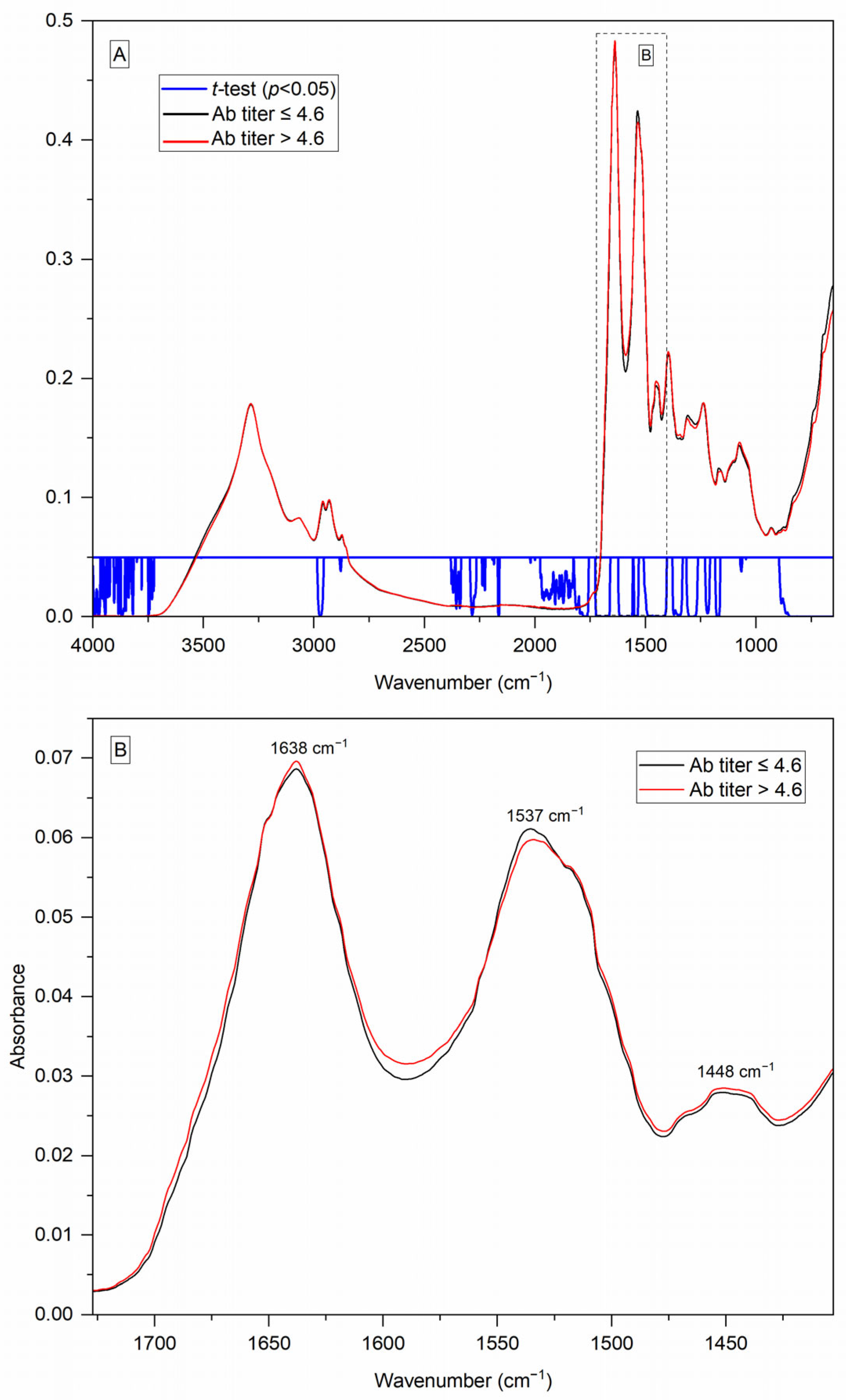
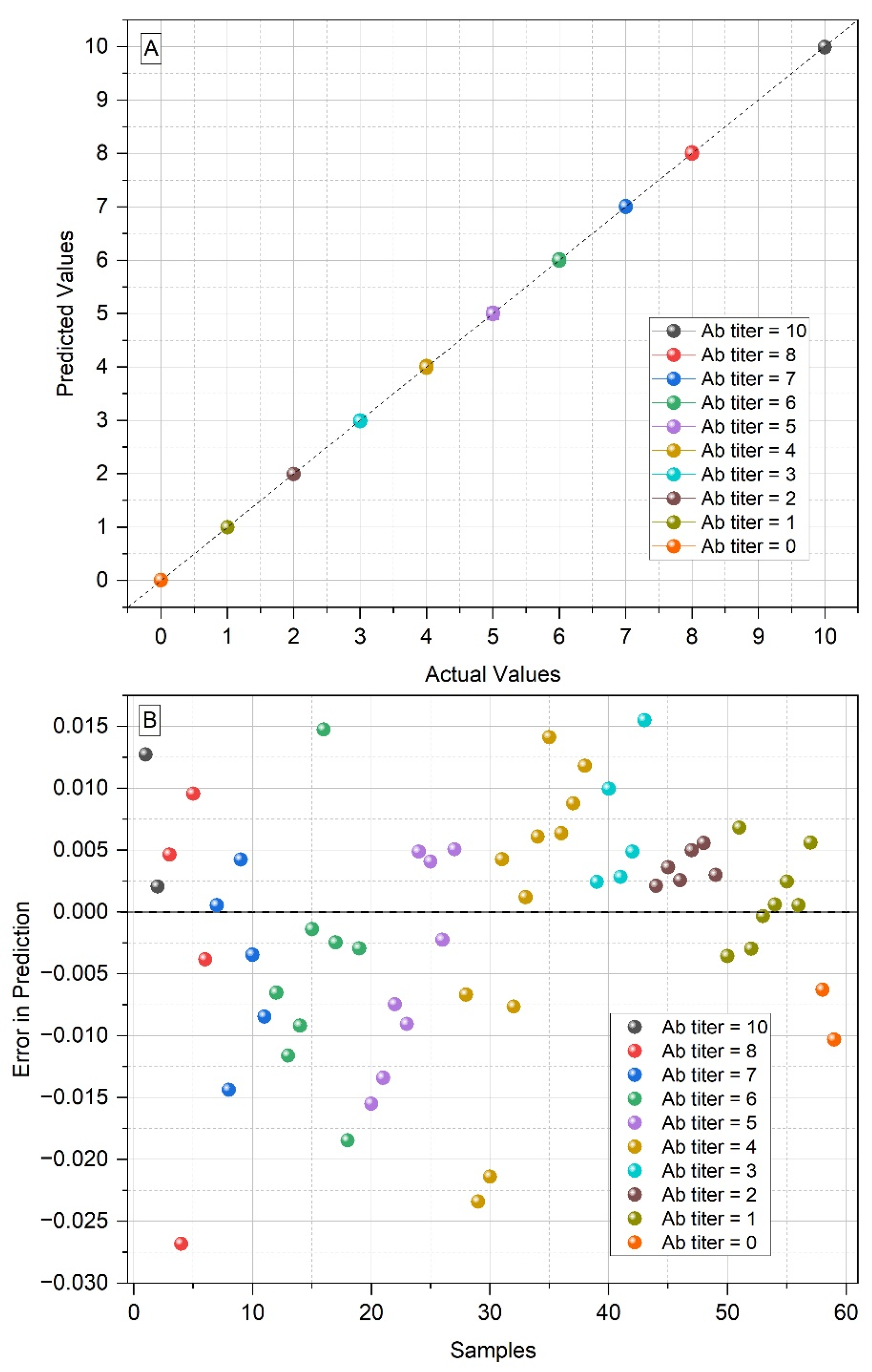
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Mendes, R.P.; Cavalcante, R.S.; Marques, S.A.; Marques, M.E.A.; Venturini, J.; Sylvestre, T.F.; Paniago, A.M.M.; Pereira, A.C.; Silva, J.F.; Fabro, A.T.; et al. Paracoccidioidomycosis: Current Perspectives from Brazil. Open Microbiol. J. 2017, 11, 224–282. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R. New trends in paracoccidioidomycosis epidemiology. J. Fungi 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Valle, A.C.F.; Macedo, P.M.; Almeida-Paes, R.; Romão, A.R.; Lazéra, M.S.; Wanke, B. Paracoccidioidomycosis after highway construction, Rio de Janeiro, Brazil. Emerg. Infect. Dis. 2017, 23, 1917–1919. [Google Scholar] [CrossRef]
- Krakhecke-Teixeira, A.G.; Yamauchi, D.H.; Rossi, A.; Sousa, H.R.; Garces, H.G.; Júnior, J.L.; Júnior, A.O.S.; Felipe, M.S.S.; Bagagli, E.; Andrade, H.F., Jr.; et al. Clinical and Eco-Epidemiological Aspects of a Novel Hyperendemic Area of Paracoccidioidomycosis in the Tocantins-Araguaia Basin (Northern Brazil), Caused by Paracoccidioides sp. J. Fungi 2022, 8, 502. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Fungal Priority Pathogens List to Guide Research, Development and Public Health Action; World Health Organization: Geneva, Switzerland, 2022.
- Griffiths, J.; Colombo, A.L.; Denning, D.W. The case for paracoccidioidomycosis to be accepted as a neglected tropical (fungal) disease. PLoS Negl. Trop. Dis. 2019, 13, e0007195. [Google Scholar] [CrossRef]
- Prado, M.; Silva, M.B.; Laurenti, R.; Travassos, L.R.; Taborda, C.P. Mortality due to systemic mycoses as a primary cause of death or in association with AIDS in Brazil: A review from 1996 to 2006. Mem. Inst. Oswaldo Cruz 2009, 104, 513–521. [Google Scholar] [CrossRef]
- Bittencourt, J.I.M.; Oliveira, R.M.; Coutinho, Z.F. Paracoccidioidomycosis mortality in the State of Paraná, Brazil, 1980/1998. Cad. Saúde Pública 2005, 21, 1856–1864. [Google Scholar] [CrossRef]
- Bagagli, E.; Matute, D.R.; Garces, G.; Tenório, B.G.; Garces, A.G.; Alves, L.G.B.; Yamauchi, D.H.; Hrycyk, M.F.; Barker, B.M.; Teixeira, M.M. Paracoccidioides brasiliensis Isolated from Nine-Banded Armadillos (Dasypus novemcinctus) Reveal Population Structure and Admixture in the Amazon Basin. J. Fungi 2021, 7, 54. [Google Scholar] [CrossRef]
- Peçanha, P.M.; Peçanha-Pietrobom, P.M.; Grão-Velloso, T.R.; Júnior, M.R.; Falqueto, A.; Gonçalves, S.S. Paracoccidioidomycosis: What We Know and What Is New in Epidemiology, Diagnosis, and Treatment. J. Fungi 2022, 8, 1098. [Google Scholar] [CrossRef]
- Hahn, R.C.; Hagen, F.; Mendes, R.P.; Burger, E.; Nery, A.F.; Siqueira, N.P.; Guevara, A.; Rodrigues, A.M.; Camargo, Z.P. Paracoccidioidomycosis: Current Status and Future Trends. Clin. Microbiol. Rev. 2022, 35, e00233-21. [Google Scholar] [CrossRef]
- Giacomazzi, J.; Baethgen, L.; Carneiro, L.C.; Millington, M.A.; Denning, D.W.; Colombo, A.L.; Pasqualotto, A.C. The burden of serious human fungal infections in Brazil. Mycoses 2016, 59, 145–150. [Google Scholar] [CrossRef] [PubMed]
- González, Á. The therapy of pulmonary fibrosis in paracoccidioidomycosis: What are the new experimental approaches? J. Fungi 2020, 6, 217. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.F.; Oliveira, H.C.; Marcos, C.M.; Assato, P.A.; Fusco-Almeida, A.M.; Mendes-Giannini, M.J.S. Advances and challenges in paracoccidioidomycosis serology caused by Paracoccidioides species complex: An update. Diag. Microbiol. Infect. Dis. 2016, 84, 87–94. [Google Scholar] [CrossRef]
- Shikanai-Yasuda, M.A.; Mendes, R.P.; Colombo, A.L.; Queiroz-Telles, F.; Kono, A.S.G.; Paniago, A.M.M.; Nathan, A.; Valle, A.C.F.; Bagagli, E.; Benard, G.; et al. Brazilian guidelines for the clinical management of paracoccidioidomycosis. Rev. Soc. Bras. Med. Trop. 2017, 50, 715–740. [Google Scholar] [CrossRef] [PubMed]
- Vidal, M.S.M.; Del Negro, G.M.B.; Vicentini, A.P.; Svidzinksi, T.I.E.; Mendes-Giannini, M.J.; Almeida, A.M.F.; Martinez, R.; Camargo, Z.P.; Taborda, C.P.; Benard, G. Serological Diagnosis of Paracoccidioidomycosis: High Rate of Inter-laboratorial Variability among Medical Mycology Reference Centers. PLoS Negl. Trop. Dis. 2014, 8, e3174. [Google Scholar] [CrossRef]
- Koehler, A.; Scroferneker, M.L.; Pereira, B.A.S.; Souza, N.M.P.; Cavalcante, R.S.; Mendes, R.P.; Corbellini, V.A. Using infrared spectroscopy of serum and chemometrics for diagnosis of paracoccidioidomycosis. J. Pharm. Biomed. Anal. 2022, 221, 115021. [Google Scholar] [CrossRef]
- Balan, V.; Mihai, C.T.; Cojocaru, F.D.; Uritu, C.M.; Dodi, G.; Botezat, D.; Gardikiotis, I. Vibrational Spectroscopy Fingerprinting in Medicine: From Molecular to Clinical Practice. Materials 2019, 12, 2884. [Google Scholar] [CrossRef]
- Camargo, Z.P.; Berzaghi, R.; Amaral, C.C.; Silva, S.H.M. Simplified method for producing Paracoccidioides brasiliensis exoantigens for use in immunodiffusion tests. Med. Mycol. 2003, 41, 539–542. [Google Scholar] [CrossRef]
- Trevisan, J.; Angelov, P.P.; Carmichael, P.L.; Scott, A.D.; Martin, F.L. Extracting biological information with computational analysis of Fourier transform infrared (FTIR) biospectroscopy datasets: Current practices to future perspectives. Analyst 2012, 137, 3202–3215. [Google Scholar] [CrossRef]
- ASTM—American Society for Testing and Materials. Standard Practices for Infrared Multivariate Quantitative Analysis, ASTM International E1655–17; West Conshohocken: Montgomery County, PA, USA, 2017. [Google Scholar]
- Barth, A. Infrared spectroscopy of proteins. Biochim. Biophys. Acta 2007, 1767, 1073–1101. [Google Scholar] [CrossRef]
- Petibois, C.; Cazorla, G.; Cassaigne, A.; Déléris, G. Plasma protein contents determined by Fourier-transform infrared spectroscopy. Clin. Chem. 2001, 47, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Butler, H.J.; Smith, B.R.; Fritzsch, R.; Radhakrishnan, P.; Palmer, D.S.; Baker, M.J. Optimised spectral pre-processing for discrimination of biofluids via ATR-FTIR spectroscopy. Analyst 2018, 143, 6121–6134. [Google Scholar] [CrossRef] [PubMed]
- Wold, S.; Antti, H.; Lindgren, F.; Öhman, J. Orthogonal signal correction of near-infrared spectra. Chemometr. Intell. Lab. Syst. 1998, 44, 175–185. [Google Scholar] [CrossRef]
- Heidrich, D.; Koehler, A.; Ramírez-Castrillón, M.; Pagani, D.M.; Ferrão, M.F.; Scroferneker, M.L.; Corbellini, V.A. Rapid classification of chromoblastomycosis agents genera by infrared spectroscopy and chemometrics supervised by sequencing of rDNA regions. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2021, 254, e119647. [Google Scholar] [CrossRef] [PubMed]
- Koehler, A.; Corbellini, V.A.; Heidrich, D.; Scroferneker, M.L. Prediction of itraconazol minium inhibitory concentration for Fonsecaea pedrosoi using Fourier Transform Infrared Spectroscopy (FTIR) and chemomectris. PLoS ONE 2020, 15, e0243231. [Google Scholar] [CrossRef] [PubMed]
- Camargo, Z.P.; Unterkircher, C.; Campoy, S.P.; Travassos, L.R. Production of Paracoccidioides brasiliensis Exoantigens for Immunodiffusion Tests. J. Clin. Microbiol. 1988, 26, 2147–2151. [Google Scholar] [CrossRef] [PubMed]
- Puccia, R.; Schenkman, S.; Gorin, P.A.J.; Travassos, L.R. Exocellular Components of Paracoccidioides brasiliensis: Identification of a Specific Antigen. Infec. Immun. 1986, 53, 199–206. [Google Scholar] [CrossRef]
- Camargo, Z.P. Serology of paracoccidioidomycosis. Mycopathologia 2008, 165, 289–302. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Hagen, F.; Puccia, R.; Hahn, R.C.; Camargo, Z.P. Paracoccidioides and Paracoccidioidomycosis in the 21st Century. Mycopathologia 2023, 188, 129–133. [Google Scholar] [CrossRef]
- Turissini, D.A.; Gomez, O.M.; Teixeira, M.M.; McEwen, J.G.; Matute, D.R. Species boundaries in the human pathogen Paracoccidioides. Fungal Genet. Biol. 2017, 106, 9–25. [Google Scholar] [CrossRef]
- Teixeira, M.M.; Theodoro, R.C.; Carvalho, M.J.A.; Fernandes, L.; Paes, H.C.; Hahn, R.C.; Mendoza, L.; Bagagli, E.; San-Blas, G.; Felipe, M.S.S. Phylogenetic analysis reveals a high level of speciation in the Paracoccidioides genus. Mol. Phylogenet. Evol. 2009, 52, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Vilela, R.; de Hoog, S.; Bensch, K.; Bagagli, E.; Mendoza, L. A taxonomic review of the genus Paracoccidioides, with focus on the uncultivable species. PLoS Negl. Trop. Dis. 2023, 17, e0011220. [Google Scholar] [CrossRef] [PubMed]
- Ricci, G.; Campanini, E.B.; Nishikaku, A.S.; Puccia, R.; Marques, M.; Bialek, R.; Rodrigues, A.M.; Batista, W.L. PbGP43 Genotyping Using Paraffin-Embedded Biopsies of Human Paracoccidioidomycosis Reveals a Genetically Distinct Lineage in the Paracoccidioides brasiliensis Complex. Mycopathologia 2022, 187, 157–168. [Google Scholar] [CrossRef] [PubMed]
- Júnior, L.P.Q.; Camargo, Z.P.; Tadano, T.; Rodrigues, A.M.; Takahara, D.T.; Gegembauer, G.; Araujo, L.M.; Hahn, R.C. Serological and antigenic profiles of clinical isolates of Paracoccidioides spp. from Central Western Brazil. Mycoses 2014, 57, 466–472. [Google Scholar] [CrossRef]
- Gegembauer, G.; Araujo, L.M.; Pereira, E.F.; Rodrigues, A.M.; Paniago, A.M.M.; Hahn, R.C.; Camargo, Z.P. Serology of Paracoccidioidomycosis Due to Paracoccidioides lutzii. PLoS Negl. Trop. Dis. 2014, e2986. [Google Scholar] [CrossRef]
- Cocio, T.A.; Martinez, R. Serological diagnosis of paracoccidioidomycosis using a Paracoccidioides spp. comercial antigen and the counterimmunoelectrophoresis method. Braz. J. Infect. Dis. 2021, 25, 101607. [Google Scholar] [CrossRef]
- Macedo, P.M.; Teixeira, M.M.; Barker, B.M.; Zancopé-Oliveira, R.M.; Almeida-Paes, R.; Valle, A.C.F. Clinical features and genetic background of the sympatric species Paracoccidioides brasiliensis and Paracoccidioides americana. PLoS Negl. Trop. Dis. 2019, 13, e0007309. [Google Scholar] [CrossRef]
- Rodrigues, A.M.; Kubitschek-Barreira, P.H.; Pinheiro, B.G.; Teixeira-Ferreira, R.; Hahn, R.C.; Camargo, Z.P. Immunoproteomic Analysis Reveals Novel Candidate Antigens for the Diagnosis of Paracoccidioidomycosis Due to Paracoccidioides lutzii. J. Fungi 2020, 6, 357. [Google Scholar] [CrossRef]
- Grossklaus, D.A.; Takahara, D.T.; Kruger, C.S.; Gonzaga, A.M.; Camargo, Z.P.; Nery, A.F.; Almeida, H.L.; Hahn, R.C. Profile of exoantigens from clinical isolates of Paracoccidioides lutzii in Mato Grosso, Brazil. Rev. Patol. Trop. 2016, 45, 265–272. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibody Titer * | Log2 (1/Antibody Titer) | Number of Samples (N = 118) | Percentage % |
|---|---|---|---|
| 1:1024 | 10 | 4 | 3.39 |
| 1:256 | 8 | 8 | 6.78 |
| 1:128 | 7 | 10 | 8.47 |
| 1:64 | 6 | 16 | 13.56 |
| 1:32 | 5 | 16 | 13.56 |
| 1:16 | 4 | 23 | 19.49 |
| 1:8 | 3 | 9 | 7.63 |
| 1:4 | 2 | 12 | 10.17 |
| 1:2 | 1 | 16 | 13.56 |
| 1:1 | 0 | 4 | 3.39 |
| Characteristics | n | Percentage % |
|---|---|---|
| Sex | ||
| Male | 90 | 76.27 |
| Female | 27 | 22.88 |
| Not informed | 1 | 0.85 |
| Clinical form and severity * | ||
| Moderate acute | 6 | 5.09 |
| Severe acute | 26 | 22.03 |
| Chronic mild | 2 | 1.69 |
| Chronic moderate | 63 | 53.39 |
| Chronic severe | 18 | 15.26 |
| Not informed | 3 | 2.54 |
| Set/Figures of Merit | Calibration Set (CS) n = 59 Samples | Prediction Set (PS) n = 59 Samples |
|---|---|---|
| R2 | 0.999978 | 0.999986 |
| RMSECV/RMSEP | 0.0115 | 0.0093 |
| tbias | 0.7830 | 0.7155 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koehler, A.; Scroferneker, M.L.; de Moraes, P.C.; Pereira, B.A.S.; Cavalcante, R.d.S.; Mendes, R.P.; Corbellini, V.A. Antibody Titer Prediction from Serum Immunodiffusion Test of Patients with Paracoccidioidomycosis Using Infrared Spectroscopy and Chemometrics. Analytica 2023, 4, 385-396. https://doi.org/10.3390/analytica4030028
Koehler A, Scroferneker ML, de Moraes PC, Pereira BAS, Cavalcante RdS, Mendes RP, Corbellini VA. Antibody Titer Prediction from Serum Immunodiffusion Test of Patients with Paracoccidioidomycosis Using Infrared Spectroscopy and Chemometrics. Analytica. 2023; 4(3):385-396. https://doi.org/10.3390/analytica4030028
Chicago/Turabian StyleKoehler, Alessandra, Maria Lúcia Scroferneker, Paulo Cezar de Moraes, Beatriz Aparecida Soares Pereira, Ricardo de Souza Cavalcante, Rinaldo Pôncio Mendes, and Valeriano Antonio Corbellini. 2023. "Antibody Titer Prediction from Serum Immunodiffusion Test of Patients with Paracoccidioidomycosis Using Infrared Spectroscopy and Chemometrics" Analytica 4, no. 3: 385-396. https://doi.org/10.3390/analytica4030028