1. Introduction
Renal failure, a debilitating condition characterized by the loss of kidney function, has long been recognized as a significant health challenge worldwide. Over the years, extensive research has advanced our understanding of the pathology, etiology, and treatment options for renal failure. This research paper aims to analyze the mortality rates of renal failure in the United States from 1999 to 2020, exploring temporal trends, demographic disparities, and the impact of advancements in renal failure management. By delving into the history, pathology, etiology, and treatment landscape of this disease, this study aims to provide valuable insights into the dynamics of renal failure and the factors influencing mortality rates, informing efforts to improve patient outcomes and healthcare delivery.
The history of renal failure dates back centuries, with notable advancements in our understanding of its pathology and treatment. Renal failure encompasses a spectrum of conditions, including acute kidney injury (AKI) and chronic kidney disease (CKD), each characterized by distinct underlying mechanisms and clinical features [
1,
2]. Rapid identification and intervention in AKI are critical for mitigating its potentially dire consequences and facilitating recovery relating to renal failure. Additionally, given its insidious onset, CKD poses challenges for early detection and intervention, necessitating a comprehensive understanding of its pathophysiology and risk factors.
The etiology of renal failure is multifactorial, with both intrinsic and extrinsic factors contributing to its development. Intrinsic causes include diseases that directly affect the kidneys, such as glomerulonephritis, diabetic nephropathy, and polycystic kidney disease [
3]. Extrinsic causes encompass conditions that affect renal function indirectly, including hypertension, diabetes mellitus, autoimmune disorders, and certain medications including antibiotics [
3,
4]. Understanding the diverse etiological factors is crucial for targeted prevention, early detection, and appropriate management strategies to mitigate the progression of renal failure and reduce associated mortality rates.
Treatment options for renal failure have evolved significantly over the past two decades. From 1999 to 2020, advancements in medical therapies, dialysis techniques, kidney transplantation, and immunosuppression have revolutionized the management of this condition. Pharmacological interventions aimed at controlling blood pressure, managing underlying comorbidities, and slowing the progression of CKD have improved patient outcomes and extended survival rates [
5,
6]. Therapeutic dialysis, including both hemodialysis and peritoneal dialysis, have provided life-sustaining renal replacement therapy for individuals with end-stage renal disease (ESRD) [
7,
8]. Kidney transplantation, a definitive treatment modality, offers the best long-term outcomes, enhancing quality of life and reducing mortality rates for suitable candidates [
9]. The disparities that exist among measurable variables of renal failure highlight the diverse ways disease affects different patient populations. Furthermore, the significance of studying the mortality rates of renal failure lies in its substantial impact on individuals and healthcare systems. The burden of renal failure extends beyond the affected individuals, impacting families, caregivers, and the broader society. Renal failure places a significant strain on healthcare resources due to the chronic and complex nature of the disease, the need for specialized care, and the excessive cost of treatment [
10]. Analyzing mortality rates provides valuable insights into the efficacy of interventions, advancements in treatments, and changes in healthcare policies over time. It enables us to assess the progress made in improving patient outcomes, identify areas of concern, and inform evidence-based interventions to reduce mortality rates associated with renal failure. By conducting a comprehensive analysis of renal failure mortality rates in the United States from 1999 to 2020, this research paper aims to contribute to the existing body of knowledge.
2. Methods
The public Center for Disease Control and Prevention’s Wide-ranging ONline Data for Epidemiologic Research (CDC WONDER) was used to access multiple cause of death mortality data with ICD-10 Codes: N17–N19 (Acute renal failure, Chronic Renal failure, Unspecified renal failure) from 1999 to 2020. The CDC WONDER uses death certificates to gather data on cause of death, place of death, as well as demographic information. The dataset was queried to gather mortality information due to renal failure of various demographic groups from 1999 to 2020. The age-adjusted mortality rates (AAMRs), with renal failure as a multiple cause of death, were collected and separated by sex and race. For purpose of this study, the categories for race include the following: Native American or Alaskan Native (AI/AN), Asian or Pacific Islander (AAPI), African American, and White. Ethnicity status is defined as Hispanic/LatinX and non-Hispanic/LatinX. The data collection, analysis, and reporting in this manuscript follow Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. Institutional review board (IRB) approval was not required as CDC WONDER uses public deidentified information.
The CDC WONDER database calculates the age-adjusted mortality rate per 100,000 and associated standard error values for mortality due to renal failure in the 1999–2020 time period. AAMRs are calculated by (mortality number/total population) and standardizing the value to the 2000 U.S. Standard Population [
11]. Using the Joinpoint Regression Program (Joinpoint V 4.9.0.0, National Cancer Institute), significant trends in mortality rates for each group were calculated by determining the annual percent change (APC) for each year between 1999 and 2020 [
12]. Additionally, a significant average annual percent change (AAPC) from 1999 to 2020 was calculated. The program analyzed APC trends for significance using log-linear regression models [
13]. APCs (Annual Percent Changes) and corresponding 95% confidence intervals were calculated using the Grid Search Method, permutation, and parametric test. Significant differences in trends between groups were calculated using a parallel pairwise comparison, which compares segmented line regression models [
14]. Previous literature has used this program to assess trends in mortality rates [
15,
16,
17]. Significance for all tests is set at
p < 0.05.
4. Discussion
The observed significant declines in renal failure mortality rates for both sexes during the late 2000s can be attributed to numerous factors, including the implementation of the Affordable Care Act (ACA) and advancements in renal care practices. The ACA, enacted in 2010, aimed to improve healthcare access and affordability for individuals across the United States. Its provisions, such as expanded insurance coverage, Medicaid expansion, and the elimination of pre-existing condition exclusions, contributed to improved access to healthcare services, including early detection and management of renal failure [
18,
19].
Beyond its overarching impact on healthcare, the implementation of the ACA heralded a paradigm shift in addressing renal failure mortality, aligning with the Triple Aim of care articulated by the former director for Centers for Medicare and Medicaid Services, Donald Berwick [
17]. This threefold focus emphasized enhancing the health of populations, improving the overall patient care experience, and concurrently reducing healthcare costs. Specifically, the ACA played a pivotal role in expanding public insurance, notably by broadening eligibility for Medicaid enrollment from 44% to 138% of the federal poverty line [
16].
The substantial increase in healthcare coverage facilitated by the ACA has likely yielded multifaceted benefits in the context of renal failure. By extending coverage to a larger segment of the population, the ACA may have contributed to earlier diagnoses and interventions for individuals at risk of renal failure [
16,
17]. Timely access to preventive care, routine health screenings, and participation in disease management programs could have collectively facilitated the identification and management of renal dysfunction at its nascent stages. This timely intervention has the potential not only to ameliorate patient outcomes but also to curtail mortality rates associated with renal failure [
16,
17]. From an economic perspective, the ACA’s emphasis on reducing healthcare costs aligns with the imperative to manage the economic burden associated with renal failure [
17]. The increased availability of healthcare coverage could lead to a shift in the economics of renal failure management, as early interventions and preventive measures are generally more cost effective than addressing advanced-stage complications. Furthermore, by enhancing access to regular healthcare services, the ACA may have contributed to a reduction in the reliance on costly emergency and acute care services for individuals with renal failure.
Additionally, the decline in mortality rates in the late 2000s can be attributed in part to notable advancements in renal care practices during that period. Progress in renal replacement therapies, particularly innovations in hemodialysis and peritoneal dialysis techniques, has played a pivotal role in improving patient outcomes [
18]. The refinement of these dialysis modalities has likely resulted in more efficient and tailored approaches, contributing to enhanced survival rates. Advancements in the management of comorbidities and complications associated with renal failure have been integral to the overall improvement in patient outcomes [
18]. Comprehensive care strategies that address not only the primary renal condition but also the concurrent health issues have become increasingly sophisticated, leading to better control of complications and a reduction in the overall burden of renal failure on patients.
The synergy of advancements in medical technologies and pharmaceuticals has further elevated the standard of care in renal medicine. Continuous innovations in diagnostic tools, treatment modalities, and pharmaceutical interventions have likely translated into more effective and personalized treatments for individuals with renal failure. These advancements may have not only reduced the occurrence of complications but also contributed to the overall improvement in the quality of life for patients undergoing renal care. Ongoing research and development in the field of renal medicine continue to yield new insights and innovations. These may include emerging therapies, advancements in transplantation techniques, and the exploration of regenerative medicine approaches for renal conditions [
18]. The dynamic nature of medical research underscores the potential for continuous improvement in renal care practices, further refining patient outcomes and mortality rates over time.
In addition, increased awareness of risk factors, such as hypertension and diabetes, and targeted interventions to address these conditions may have positively influenced renal failure mortality rates [
20,
21]. Public health initiatives focusing on lifestyle modifications, early detection, and disease management have contributed to better control of these underlying risk factors, potentially reducing the incidence and progression of renal failure [
20,
21,
22]. Public health initiatives may also contribute to cost savings by reducing the overall burden of renal failure on the healthcare system. The early detection and management of risk factors can potentially avert the need for more intensive and costly interventions associated with advanced renal failure stages [
17,
19,
20,
21]. Consequently, investing in public health programs that address modifiable risk factors aligns with a preventive healthcare approach, offering both clinical and economic benefits.
While the ACA and advancements in renal care practices likely played significant roles, it is essential to consider other contributing factors that could have influenced the decline in renal failure mortality rates during the late 2000s. These may include improved public health campaigns promoting healthier lifestyles, increased awareness of kidney disease, better adherence to prescribed treatments, and improved overall healthcare quality [
22,
23,
24].
It is worth noting that additional research and data analysis beyond the scope of this study would be required to delve deeper into the specific contributions of each factor and to assess their individual impacts on the observed decline in renal failure mortality rates. Nevertheless, the findings suggest a positive trend and underscore the importance of continued efforts to enhance healthcare access, advance medical interventions, and improve preventive care strategies for renal failure management.
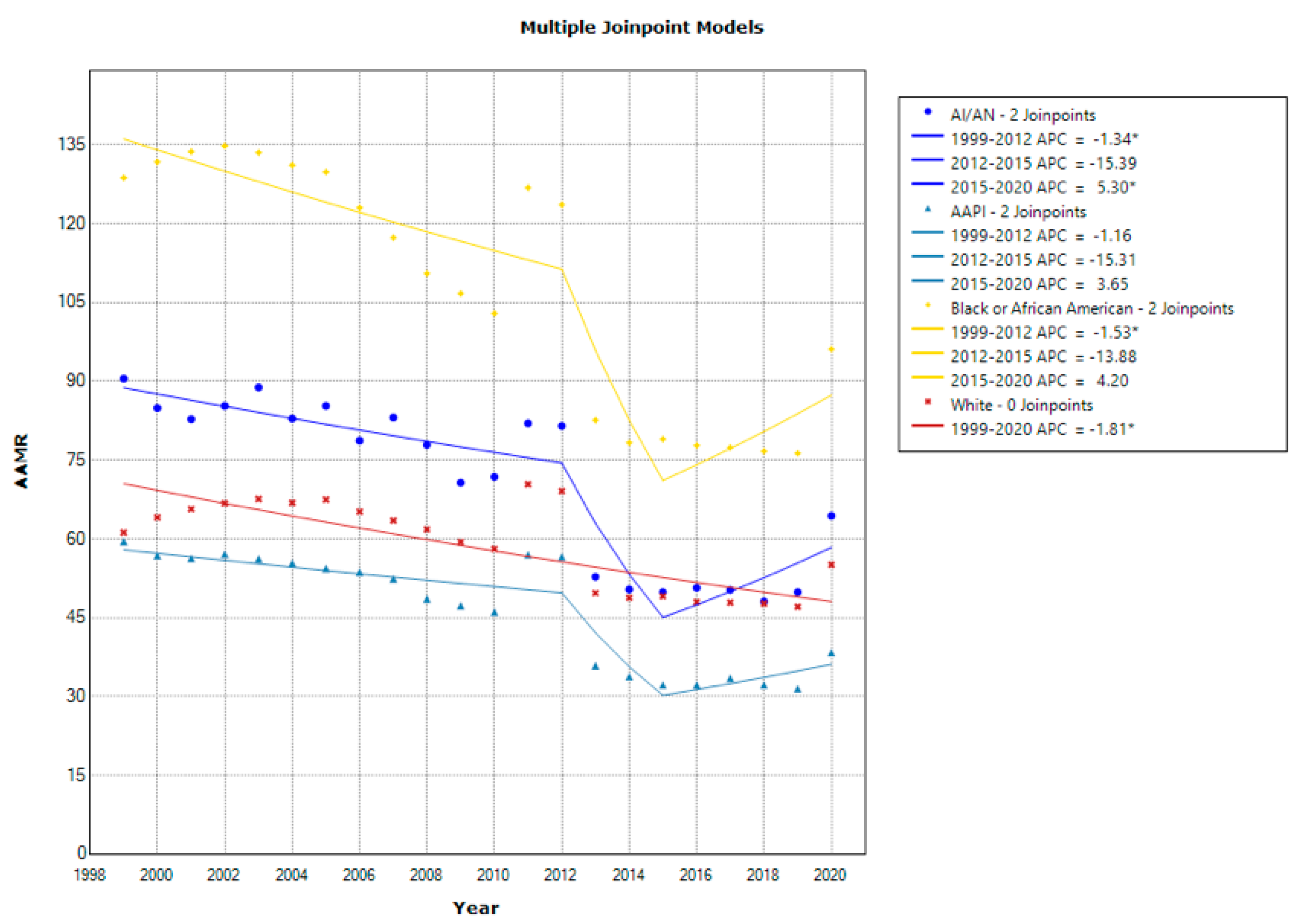
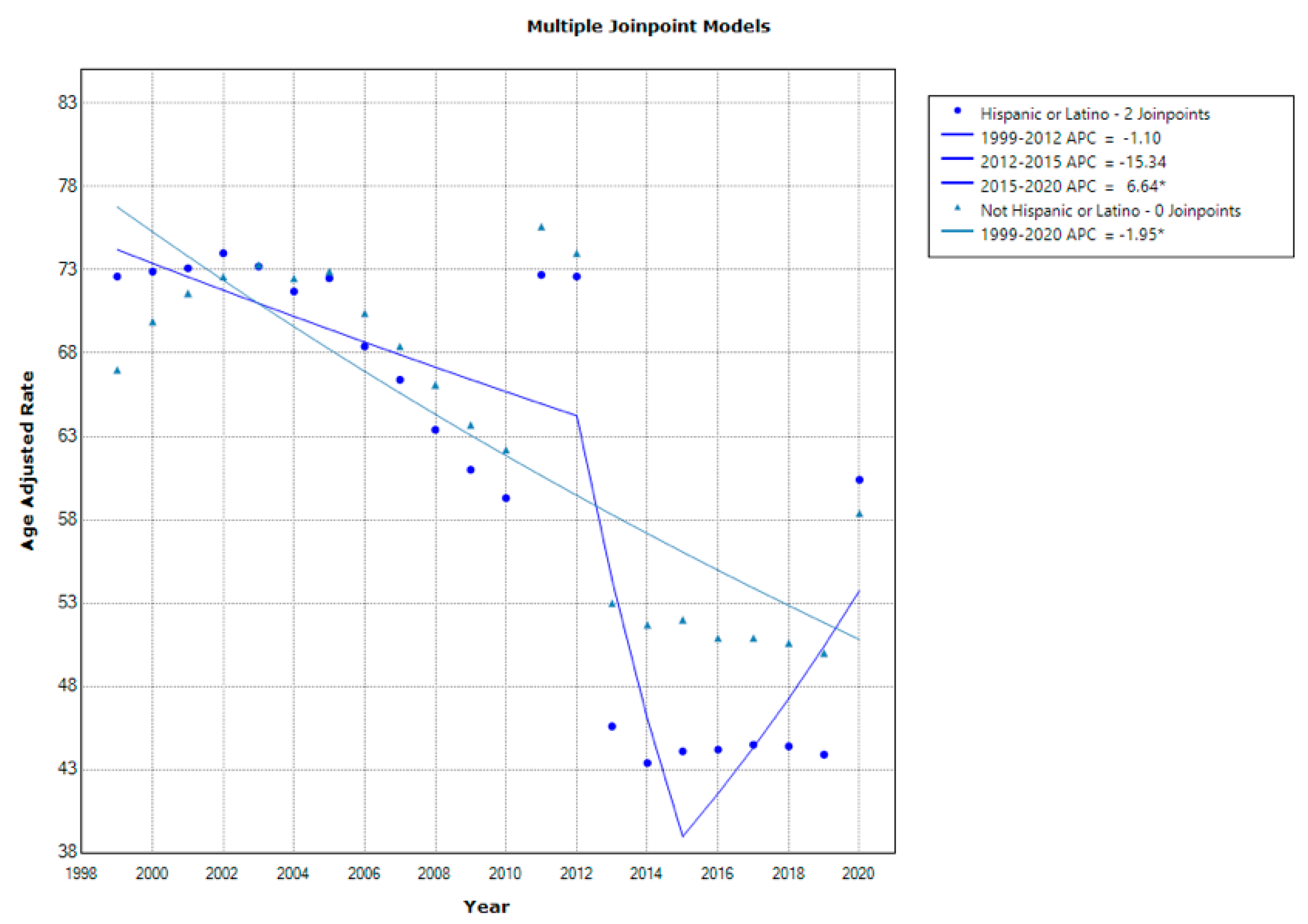
Persistent disparities in renal failure mortality rates have been observed among different racial and ethnic groups in the United States. African Americans and Hispanics especially have consistently exhibited higher mortality rates compared to non-Hispanic Whites [
25]. Higher serum creatinine levels have previously been associated with African Americans, which could potentially contribute to these discrepancies [
26,
27,
28]. These disparities can also be attributed to multiple factors, including socioeconomic disparities, limited access to healthcare services, higher rates of comorbidities such as diabetes and hypertension, and genetic predispositions [
20,
21,
29,
30]. Efforts to address these disparities should involve targeted interventions, such as improving access to quality healthcare, reducing socioeconomic barriers, enhancing health education programs, and promoting the early detection and management of risk factors among vulnerable populations.
Renal failure mortality rates vary significantly across states and regions within the United States. Variations can be attributed to diverse factors such as population density, healthcare infrastructure, socioeconomic conditions, and the availability of specialized care facilities. Regions with higher poverty rates and limited access to healthcare facilities often experience higher mortality rates [
31,
32,
33]. To mitigate these disparities, state-level initiatives should focus on strengthening healthcare infrastructure, increasing the availability of dialysis centers and renal care facilities, implementing preventative measures, and improving access to healthcare services, particularly in underserved areas.
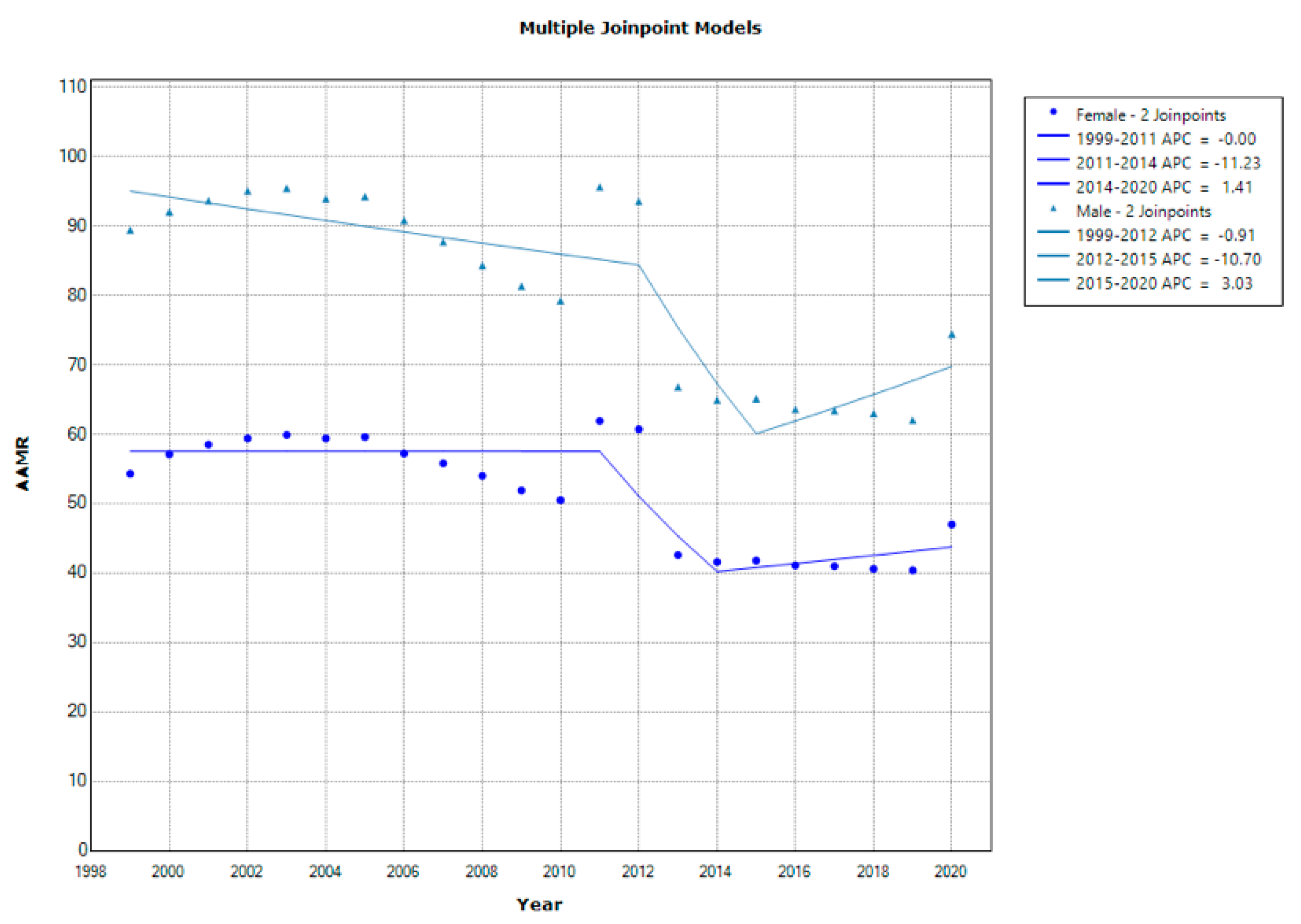
Sex and gender differences play a role in renal failure mortality rates. Historically, men have exhibited higher mortality rates compared to women. This disparity can be attributed to differences in risk factors, including a higher prevalence of hypertension and diabetes among men [
34,
35]. Hormonal factors such as the protective effects of estrogens in women may also contribute to the observed differences [
36]. Recognizing and addressing these disparities is crucial for developing targeted prevention and treatment strategies. Tailored interventions should consider the specific risk profiles and healthcare needs of both men and women to effectively reduce mortality rates associated with renal failure.
Multiple risk factors influence renal failure mortality rates, including hypertension, diabetes, obesity, smoking, and cardiovascular diseases [
20,
21]. Age is also a significant factor, as the prevalence of renal failure and mortality rates increase with advancing age [
35,
37]. The aging population in the United States underscores the importance of proactive measures to manage risk factors and implement early detection and intervention strategies [
38]. Encouraging healthy lifestyles, regular screenings for hypertension and diabetes, comprehensive management of comorbidities, and optimizing cardiovascular health are essential for reducing mortality rates associated with renal failure.
Advancements in diagnosing and treating renal failure have contributed to improved outcomes and reduced mortality rates. Early detection through routine screenings, imaging such as ultrasound of the kidneys, and improved understanding of risk factors have enabled timely intervention and management [
24]. Additionally, calcineurin inhibitor (CNI) minimization strategies and newer immunosuppressive agents may have improved patient survival rates [
23]. Dialysis also remains a reliable option to treat this disease as well [
8,
39]. The ongoing research and development of novel therapies, including regenerative medicine and precision medicine approaches, hold promise for further advancements in renal failure management. Collaboration between healthcare providers and researchers and participation in clinical trials are critical for enhancing diagnosing and treatment strategies.
Despite notable advancements, several drawbacks need to be addressed regarding renal failure mortality rates. Limited access to healthcare services, especially in underserved communities and rural areas, remains a significant challenge. Health disparities, including racial and ethnic disparities, contribute to unequal outcomes and higher mortality rates [
35]. The excessive cost of renal replacement therapies, such as dialysis and transplantation, poses a barrier to optimal care for many individuals. Long wait lists to receive a donated kidney stand as an issue as well [
23]. In addressing the multifaceted challenges of renal failure management, it is imperative to underscore the significance of activities directed at increasing the pool of living donors. Encouraging and facilitating living kidney donation not only holds the potential to significantly reduce the protracted wait times associated with receiving a donated kidney but also enables patients in the pre-emptive stage to circumvent the need for renal replacement therapy, thereby optimizing overall patient outcomes [
23].
Regrettably, the healthcare systems in the United States are confronted with several challenges that impede the progress of renal failure care. Nephrologists operate within a compensation framework known as Fee-for-Service (FFS), where their remuneration is contingent on the frequency of patient visits, forming an incremental monthly payment structure. The success of a nephrology practice is intricately tied to the patient volume under their care and the efficiency with which that care is administered. However, the predominant FFS model currently in place tends to incentivize the expansion of patient volumes suffering from end-stage renal disease (ESRD) rather than prioritizing the delivery of value-based care in the upstream stages, which could potentially contribute to a reduction in ESRD incident rates [
16,
17].
Consequently, the provision of ESRD care, along with fees associated with medical directorship responsibilities, collectively constitutes a substantial portion, ranging from 50% to 60% of a nephrologist’s overall income [
17]. Notably, outpatient CKD care, which is centered on patients referred by primary care providers, remains embedded within an FFS payment structure that experiences annual erosion in real inflation-adjusted dollars [
18,
19]. This trend has become increasingly apparent between the years 2011 and 2020 [
17]. Despite the existence of defined FFS payment models for outpatient care, the reimbursement falls short of covering the actual costs associated with providing such care. This financial dynamic creates incentives that prompt the cross-subsidization of office-based CKD care using income generated from hospital and ESRD care, underscoring a misalignment in physician incentives [
17].
Efforts should focus on developing cost-effective interventions, improving access to care for all populations, enhancing health literacy, and implementing policies that promote equitable healthcare delivery. Further research is needed to identify and address the specific barriers and challenges associated with renal failure management in different populations.
5. Limitations
While this research project has strived for comprehensive and accurate analysis of renal failure mortality rates in the United States from 1999 to 2020, it is important to acknowledge several limitations that may impact the interpretation of our findings. The study relies on data obtained from CDC WONDER, which, while a valuable resource, is subject to potential inaccuracies in death certificates and variations in reporting practices across different states and time periods. These variations could introduce minor discrepancies in the data.
As an observational study using publicly available, de-identified data, our research is inherently limited by the lack of direct access to individual medical records or the ability to conduct prospective assessments. This limitation precludes a more detailed examination of specific clinical factors, comorbidities, or treatment modalities that could provide deeper insights into the observed trends.
Additionally, while we have taken great care to account for demographic factors, including age, sex, race, and ethnicity, as well as the impact of the Affordable Care Act (ACA) and advancements in renal care practices, there may be other unmeasured or confounding variables that could influence renal failure mortality rates. Socioeconomic factors, lifestyle variables, regional disparities, and cultural differences, among others, are potential variables that could play a role but were not included in this analysis.
Our research also provides a retrospective view of renal failure mortality rates over a 21-year period. Changes in healthcare policies, healthcare delivery, and treatment practices may have continued to evolve beyond 2020, potentially affecting mortality rates. Future research may be needed to assess the long-term impact of these evolving factors on renal failure outcomes.
In summary, while this research project offers valuable insights into renal failure mortality rates and associated factors, it is imperative to consider these limitations when interpreting the findings. These limitations underscore the complexity of the topic and emphasize the need for ongoing research and data analysis to further enhance our understanding of renal failure and inform strategies for its prevention and management.


{kind=link}
{kind=link}
{kind=link}


