
An Exploratory Study of Early Immune Response Markers for Pembrolizumab in Urothelial Tract Cancer
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients and Data Collection
2.3. TruCulture®
2.4. Statistics
3. Results
3.1. Patients
3.2. Tumor Responses
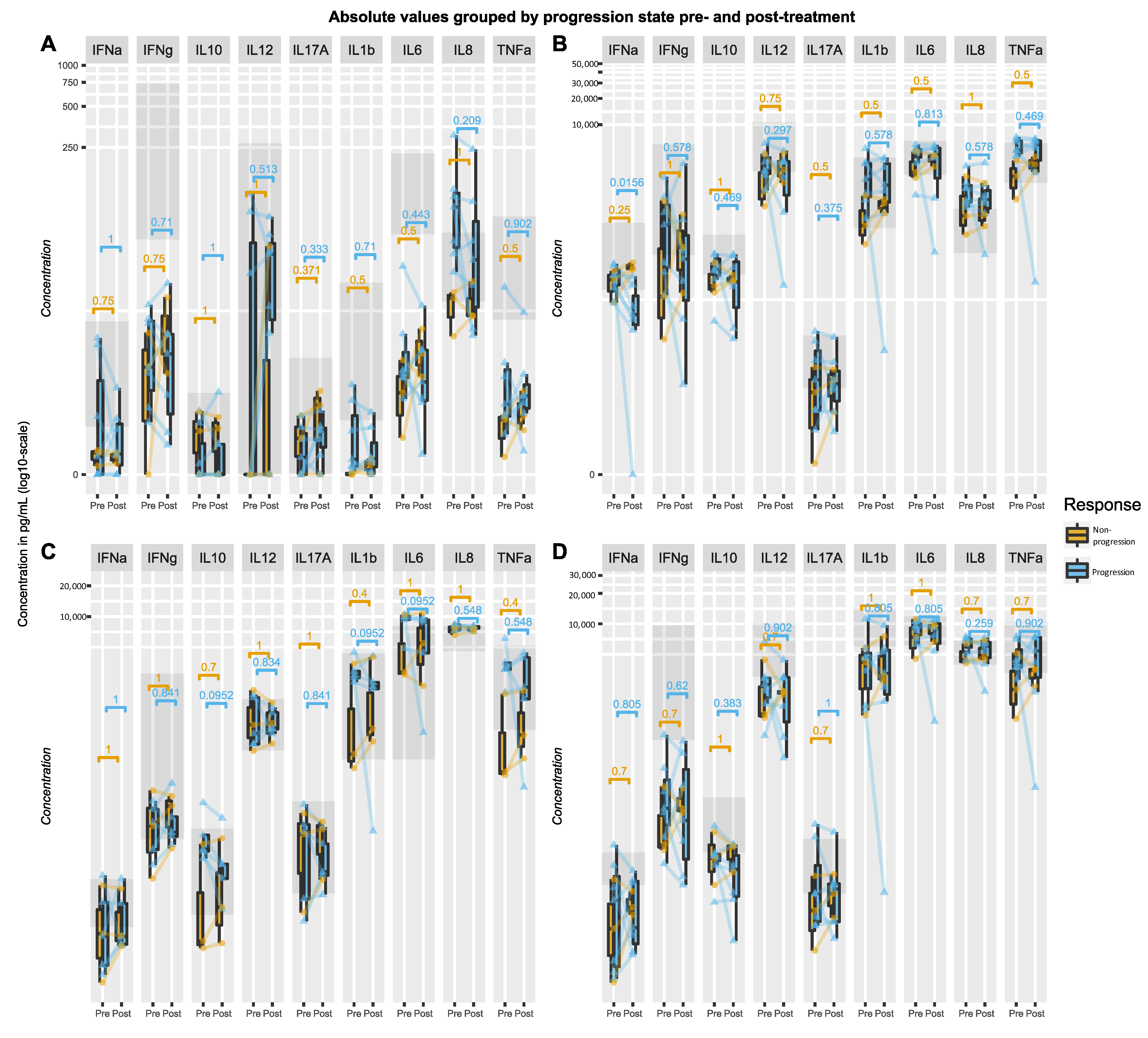
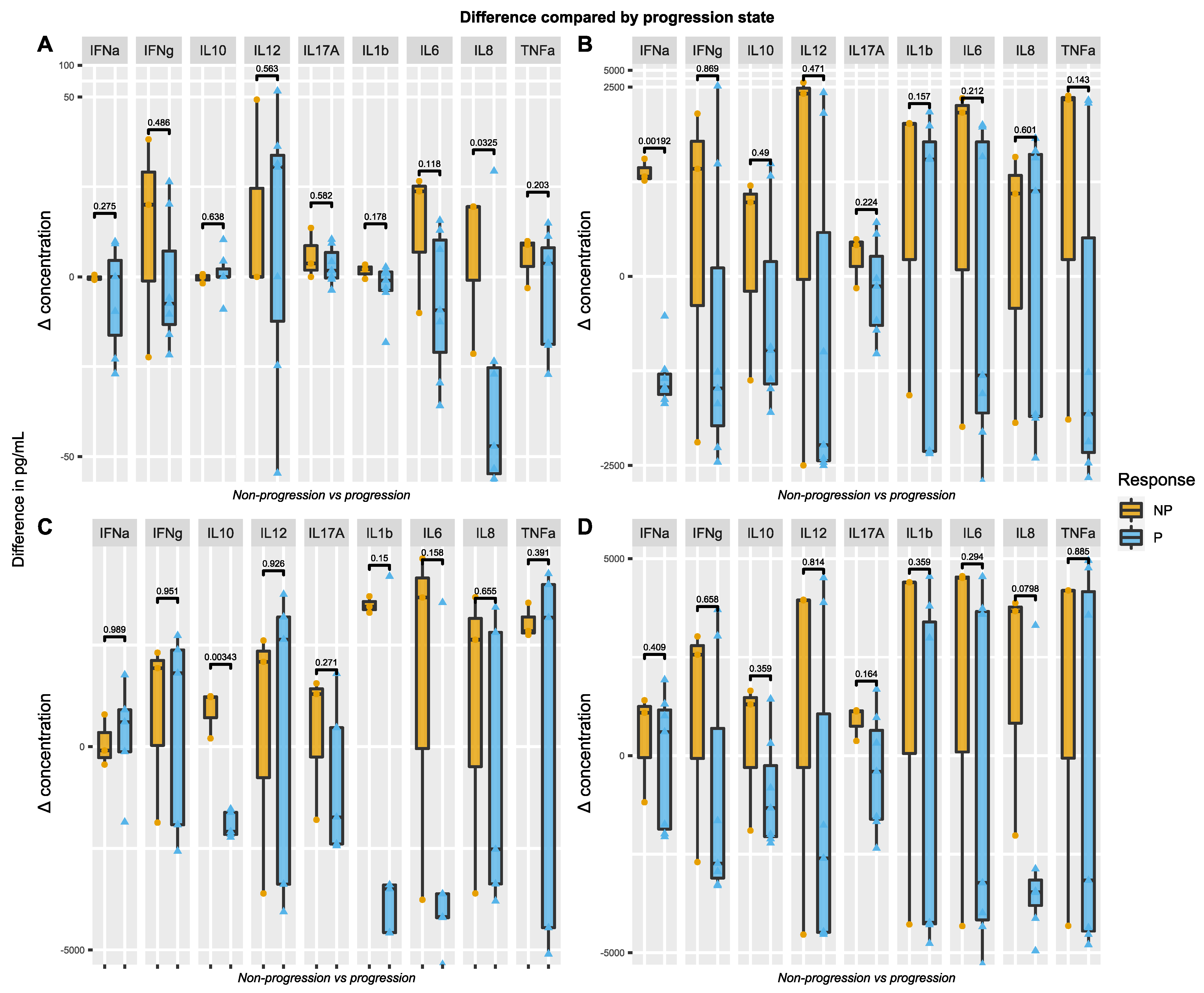
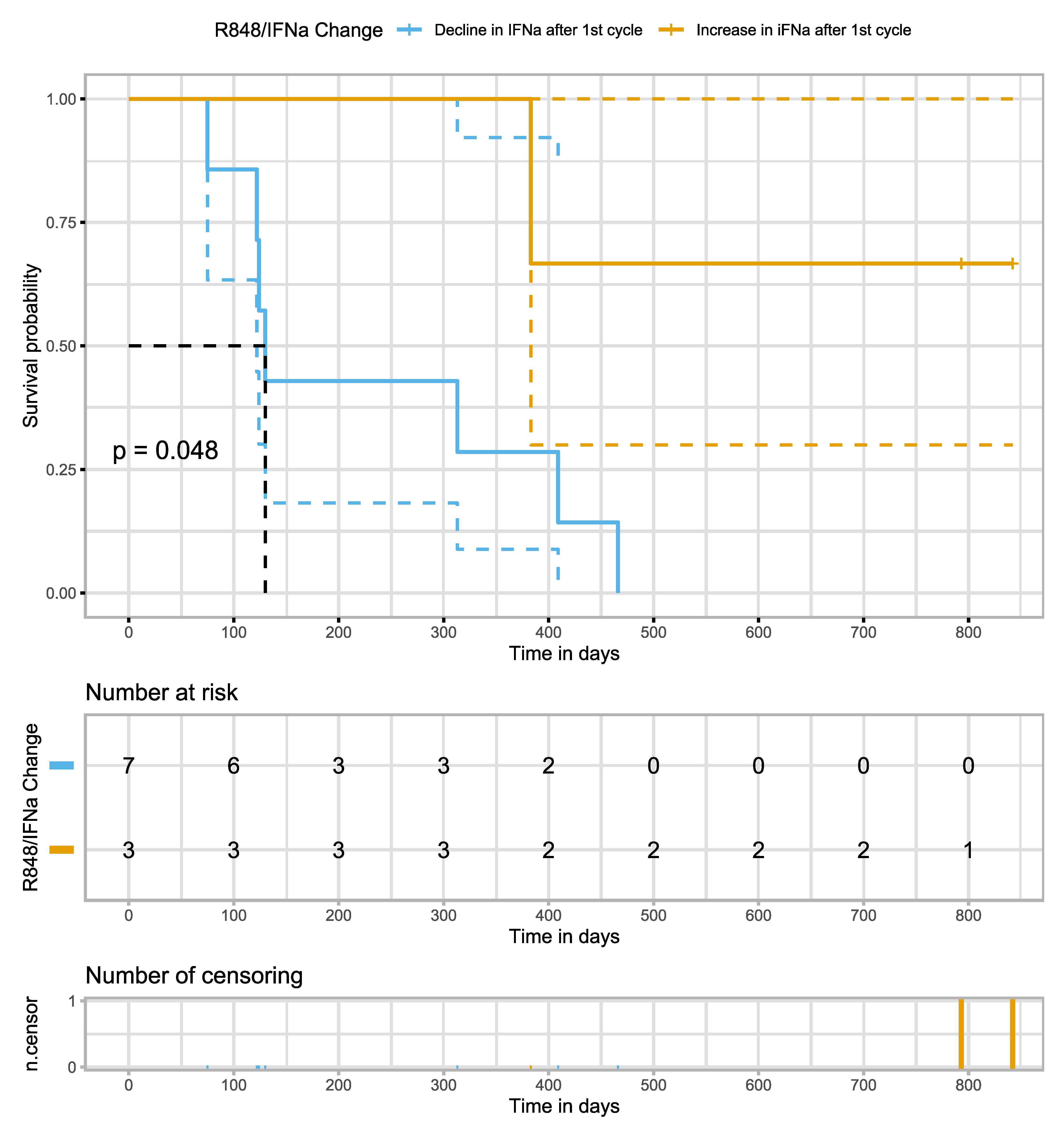
3.3. Stimulated Innate Immune Responses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Linares Espinós, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef] [PubMed]
- Hepp, Z.; Shah, S.N.; Smoyer, K.; Vadagam, P. Epidemiology and treatment patterns for locally advanced or metastatic urothelial carcinoma: A systematic literature review and gap analysis. J. Manag. Care Spec. Pharm. 2021, 27, 240–255. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Babjuk, M.; Bellmunt, J.; Bruins, H.M.; De Reijke, T.M.; De Santis, M.; Gillessen, S.; James, N.; Maclennan, S.; Palou, J.; et al. EAU-ESMO Consensus Statements on the Management of Advanced and Variant Bladder Cancer—An International Collaborative Multistakeholder Effort†. Eur. Urol. 2020, 77, 223–250. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Castellano, D.; O’Donnell, P.H.; Grivas, P.; Vuky, J.; Powles, T.; Plimack, E.R.; Hahn, N.M.; de Wit, R.; Pang, L.; et al. First-line pembrolizumab in cisplatin-ineligible patients with locally advanced and unresectable or metastatic urothelial cancer (KEYNOTE-052): A multicentre, single-arm, phase 2 study. Lancet Oncol. 2017, 18, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Balar, A.V.; Galsky, M.D.; Rosenberg, J.E.; Powles, T.; Petrylak, D.P.; Bellmunt, J.; Loriot, Y.; Necchi, A.; Hoffman-Censits, J.; Perez-Gracia, J.L.; et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: A single-arm, multicentre, phase 2 trial. Lancet 2017, 389, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; de Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef]
- Parikh, M.; Powles, T. Immune Checkpoint Inhibition in Advanced Bladder and Kidney Cancer: Responses and Further Management. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, e182–e189. [Google Scholar] [CrossRef]
- Jun, T.; Anker, J.; Galsky, M.D. Biomarkers for therapy selection in metastatic urothelial cancer. J. Cancer Metastasis Treat. 2022, 8, 1. [Google Scholar] [CrossRef]
- Szabados, B.; Prendergast, A.; Jackson-Spence, F.; Choy, J.; Powles, T. Immune Checkpoint Inhibitors in Front-line Therapy for Urothelial Cancer. Eur. Urol. Oncol. 2021, 4, 943–947. [Google Scholar] [CrossRef]
- Schulz, G.B.; Todorova, R.; Braunschweig, T.; Rodler, S.; Volz, Y.; Eismann, L.; Pfitzinger, P.; Jokisch, F.; Buchner, A.; Stief, C.; et al. PD-L1 expression in bladder cancer: Which scoring algorithm in what tissue? Urol. Oncol. Semin. Orig. Investig. 2021, 39, 734.e1–734.e10. [Google Scholar] [CrossRef]
- EMA Restricts Use of Keytruda and Tecentriq in Bladder Cancer. Available online: https://www.ema.europa.eu/en/news/ema-restricts-use-keytruda-tecentriq-bladder-cancer (accessed on 15 November 2023).
- Rouanne, M.; Radulescu, C.; Adam, J.; Allory, Y. PD-L1 testing in urothelial bladder cancer: Essentials of clinical practice. World J. Urol. 2021, 39, 1345–1355. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 24, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Rosenberg, J.E.; Sonpavde, G.P.; Loriot, Y.; Durán, I.; Lee, J.L.; Matsubara, N.; Vulsteke, C.; Castellano, D.; Wu, C.; et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Loriot, Y.; Necchi, A.; Park, S.H.; Garcia-Donas, J.; Huddart, R.; Burgess, E.; Fleming, M.; Rezazadeh, A.; Mellado, B.; Varlamov, S.; et al. Erdafitinib in Locally Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2019, 381, 338–348. [Google Scholar] [CrossRef]
- Powles, T.; Bellmunt, J.; Comperat, E.; De Santis, M.; Huddart, R.; Loriot, Y.; Necchi, A.; Valderrama, B.P.; Ravaud, A.; Shariat, S.F.; et al. Bladder cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2021, 33, S0923753421048274. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Albacker, L.A.; Hopkins, A.C.; Montesion, M.; Murugesan, K.; Vithayathil, T.T.; Zaidi, N.; Azad, N.S.; Laheru, D.A.; Frampton, G.M.; et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight 2019, 4, e126908. [Google Scholar] [CrossRef]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.J.R.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.-L.; et al. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar] [CrossRef]
- Galsky, M.D.; Banchereau, R.; Hamidi, H.R.; Leng, N.; Harris, W.; O’Donnell, P.H.; Kadel, E.E.; Yuen, K.C.Y.; Jin, D.; Koeppen, H.; et al. Tumor, immune, and stromal characteristics associated with clinical outcomes with atezolizumab (atezo) + platinum-based chemotherapy (PBC) or atezo monotherapy (mono) versus PBC in metastatic urothelial cancer (mUC) from the phase III IMvigor130 study. J. Clin. Oncol. 2020, 38, 5011. [Google Scholar] [CrossRef]
- Litchfield, K.; Reading, J.L.; Puttick, C.; Thakkar, K.; Abbosh, C.; Bentham, R.; Watkins, T.B.K.; Rosenthal, R.; Biswas, D.; Rowan, A.; et al. Meta-analysis of tumor- and T cell-intrinsic mechanisms of sensitization to checkpoint inhibition. Cell 2021, 184, 596–614.e14. [Google Scholar] [CrossRef]
- Boutsikou, E.; Domvri, K.; Hardavella, G.; Tsiouda, D.; Zarogoulidis, K.; Kontakiotis, T. Tumour necrosis factor, interferon-gamma and interleukins as predictive markers of antiprogrammed cell-death protein-1 treatment in advanced non-small cell lung cancer: A pragmatic approach in clinical practice. Ther. Adv. Med. Oncol. 2018, 10, 175883591876823. [Google Scholar] [CrossRef]
- Davoodzadeh Gholami, M.; Kardar, G.A.; Saeedi, Y.; Heydari, S.; Garssen, J.; Falak, R. Exhaustion of T lymphocytes in the tumor microenvironment: Significance and effective mechanisms. Cell. Immunol. 2017, 322, 1–14. [Google Scholar] [CrossRef]
- Wherry, E.J. T cell exhaustion. Nat. Immunol. 2011, 12, 492–499. [Google Scholar] [CrossRef] [PubMed]
- McLane, L.M.; Abdel-Hakeem, M.S.; Wherry, E.J. CD8 T Cell Exhaustion During Chronic Viral Infection and Cancer. Annu. Rev. Immunol. 2019, 37, 457–495. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.K.; Chevalier, M.F.; Derré, L. The multifaceted immune regulation of bladder cancer. Nat. Rev. Urol. 2019, 16, 613–630. [Google Scholar] [CrossRef] [PubMed]
- Iwahori, K.; Shintani, Y.; Funaki, S.; Yamamoto, Y.; Matsumoto, M.; Yoshida, T.; Morimoto-Okazawa, A.; Kawashima, A.; Sato, E.; Gottschalk, S.; et al. Peripheral T cell cytotoxicity predicts T cell function in the tumor microenvironment. Sci. Rep. 2019, 9, 2636. [Google Scholar] [CrossRef] [PubMed]
- McNamara, M.J.; Hilgart-Martiszus, I.; Barragan Echenique, D.M.; Linch, S.N.; Kasiewicz, M.J.; Redmond, W.L. Interferon-γ Production by Peripheral Lymphocytes Predicts Survival of Tumor-Bearing Mice Receiving Dual PD-1/CTLA-4 Blockade. Cancer Immunol. Res. 2016, 4, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Duffy, D.; Rouilly, V.; Libri, V.; Hasan, M.; Beitz, B.; David, M.; Urrutia, A.; Bisiaux, A.; LaBrie, S.T.; Dubois, A.; et al. Functional Analysis via Standardized Whole-Blood Stimulation Systems Defines the Boundaries of a Healthy Immune Response to Complex Stimuli. Immunity 2014, 40, 436–450. [Google Scholar] [CrossRef]
- Duffy, D.; Rouilly, V.; Braudeau, C.; Corbière, V.; Djebali, R.; Ungeheuer, M.-N.; Josien, R.; LaBrie, S.T.; Lantz, O.; Louis, D.; et al. Standardized whole blood stimulation improves immunomonitoring of induced immune responses in multi-center study. Clin. Immunol. 2017, 183, 325–335. [Google Scholar] [CrossRef]
- Herberth, M.; Rahmoune, H.; Schwarz, E.; Koethe, D.; Harris, L.W.; Kranaster, L.; Witt, S.H.; Spain, M.; Barnes, A.; Schmolz, M.; et al. Identification of a Molecular Profile Associated with Immune Status in First-Onset Schizophrenia Patients. Clin. Schizophr. Relat. Psychoses 2014, 7, 207–215. [Google Scholar] [CrossRef]
- Rodrigues, K.B.; Dufort, M.J.; Llibre, A.; Speake, C.; Rahman, M.J.; Bondet, V.; Quiel, J.; Linsley, P.S.; Greenbaum, C.J.; Duffy, D.; et al. Innate immune stimulation of whole blood reveals IFN-1 hyper-responsiveness in type 1 diabetes. Diabetologia 2020, 63, 1576–1587. [Google Scholar] [CrossRef] [PubMed]
- Duffy, D.; Nemes, E.; Llibre, A.; Rouilly, V.; Musvosvi, M.; Smith, N.; Filander, E.; Africa, H.; Mabwe, S.; Jaxa, L.; et al. Immune Profiling Enables Stratification of Patients with Active Tuberculosis Disease or Mycobacteriu m tuberculosis Infection. Clin. Infect. Dis. 2021, 73, e3398–e3408. [Google Scholar] [CrossRef] [PubMed]
- Aasvang, E.K.; Pitter, S.; Hansen, C.P.; Storkholm, J.H.; Krohn, P.S.; Burgdorf, S.K.; Von Stemann, J.H.; Lundgren, J.D.; Nielsen, S.D.; Kehlet, H.; et al. Preoperative TruCulture® whole blood cytokine response predicts post-operative inflammation in pancreaticoduodenectomy patients—A pilot cohort study. Scand. J. Immunol. 2020, 92, e12930. [Google Scholar] [CrossRef]
- Gjærde, L.K.; Brooks, P.T.; Andersen, N.S.; Friis, L.S.; Kornblit, B.; Petersen, S.L.; Schjødt, I.; Nielsen, S.D.; Ostrowski, S.R.; Sengeløv, H. Functional immune reconstitution early after allogeneic haematopoietic cell transplantation: A comparison of pre- and post-transplantation cytokine responses in stimulated whole blood. Scand. J. Immunol. 2021, 94, e13042. [Google Scholar] [CrossRef]
- Ørbæk, M.; Gynthersen, R.M.M.; Mens, H.; Stenør, C.; Wiese, L.; Brandt, C.; Ostrowski, S.R.; Nielsen, S.D.; Lebech, A.-M. Stimulated Immune Response by TruCulture® Whole Blood Assay in Patients With European Lyme Neuroborreliosis: A Prospective Cohort Study. Front. Cell. Infect. Microbiol. 2021, 11, 666037. [Google Scholar] [CrossRef] [PubMed]
- Todberg, T.; Loft, N.; Møller, D.L.; Ostrowski, S.R.; Nielsen, S.D.; Skov, L. Impact of methotrexate and adalimumab on immune function of patients with psoriasis. Dermatol. Ther. 2022, 35, e15284. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Wang, S.; Wornow, M.; Altman, R.B. Construction of disease-specific cytokine profiles by associating disease genes with immune responses. PLoS Comput. Biol. 2022, 18, e1009497. [Google Scholar] [CrossRef]
- Dockrell, D.H. Imiquimod and resiquimod as novel immunomodulators. J. Antimicrob. Chemother. 2001, 48, 751–755. [Google Scholar] [CrossRef]
- Bishop, G.A.; Hsing, Y.; Hostager, B.S.; Jalukar, S.V.; Ramirez, L.M.; Tomai, M.A. Molecular Mechanisms of B Lymphocyte Activation by the Immune Response Modifier R-848. J. Immunol. 2000, 165, 5552–5557. [Google Scholar] [CrossRef]
- Chi, H.; Li, C.; Zhao, F.S.; Zhang, L.; Ng, T.B.; Jin, G.; Sha, O. Anti-tumor Activity of Toll-Like Receptor 7 Agonists. Front. Pharmacol. 2017, 8, 304. [Google Scholar] [CrossRef]
- Javaid, N.; Choi, S. Toll-like Receptors from the Perspective of Cancer Treatment. Cancers 2020, 12, 297. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zeng, G. Cancer and Innate Immune System Interactions: Translational Potentials for Cancer Immunotherapy. J. Immunother. 2012, 35, 299–308. [Google Scholar] [CrossRef]
- Brown, G.D.; Herre, J.; Williams, D.L.; Willment, J.A.; Marshall, A.S.J.; Gordon, S. Dectin-1 Mediates the Biological Effects of β-Glucans. J. Exp. Med. 2003, 197, 1119–1124. [Google Scholar] [CrossRef]
- Gantner, B.N.; Simmons, R.M.; Canavera, S.J.; Akira, S.; Underhill, D.M. Collaborative Induction of Inflammatory Responses by Dectin-1 and Toll-like Receptor 2. J. Exp. Med. 2003, 197, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhai, X.; Li, J.; Guan, J.; Xu, S.; Li, Y.; Zhu, H. The Role of Cytokines in Predicting the Response and Adverse Events Related to Immune Checkpoint Inhibitors. Front. Immunol. 2021, 12, 670391. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, N.; Kiyohara, Y.; Uhara, H.; Iizuka, H.; Uehara, J.; Otsuka, F.; Fujisawa, Y.; Takenouchi, T.; Isei, T.; Iwatsuki, K.; et al. Cytokine biomarkers to predict antitumor responses to nivolumab suggested in a phase 2 study for advanced melanoma. Cancer Sci. 2017, 108, 1022–1031. [Google Scholar] [CrossRef] [PubMed]
- Hirashima, T.; Kanai, T.; Suzuki, H.; Yoshida, H.; Matsushita, A.; Kawasumi, H.; Samejima, Y.; Noda, Y.; Nasu, S.; Tanaka, A.; et al. The Levels of Interferon-gamma Release as a Biomarker for Non-small-cell Lung Cancer Patients Receiving Immune Checkpoint Inhibitors. Anticancer Res. 2019, 39, 6231–6240. [Google Scholar] [CrossRef]
- Costantini, A.; Julie, C.; Dumenil, C.; Hélias-Rodzewicz, Z.; Tisserand, J.; Dumoulin, J.; Giraud, V.; Labrune, S.; Chinet, T.; Emile, J.-F.; et al. Predictive role of plasmatic biomarkers in advanced non-small cell lung cancer treated by nivolumab. OncoImmunology 2018, 7, e1452581. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pt. ID | Age | Gender | PS at Baseline | Post Pembro Treatment | Disease Burden | Cycles before CT Scan | Response at 1st CT Scan | Number of Cycles | Reason for EOT | Treatment Line | Histology | Days between Measurements | PD-L1 Status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | male | 1 | None | LbD,Car,Adr | PD | 2 | Decline in PS | UC | <10 | ||||
| 2 | male | NA | Vinflunine | St | PR | 9 | PD | UC | <10 | ||||
| 3 | male | 1 | None | LbD, Pen | PD | 3 | PD | UC | NA | ||||
| 4 | male | 1 | EV,Vinflunine | LbD | PD | 3 | PD | UC | NA | ||||
| 5 | female | 0 | None | LbD | SD | 24 | EOT (2 years) | SCC | >10 | ||||
| 6 | male | 1 | None | LbD | PD | 3 | PD | UC | NA | ||||
| 7 | male | 1 | None | Adr | PD | 2 | PD | UC | >10 | ||||
| 8 | male | 0 | None | St, Lu | PD | 3 | PD | UC | >10 | ||||
| 9 | male | 1 | None | LbD | PR | 8 | Decline in PS | UC | NA | ||||
| 10 | male | 0 | None | Lu, Bo | PD | 3 | PD | UC | >10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stormoen, D.R.; Omland, L.H.; Mouw, K.W.; Szallasi, Z.; Ostrowski, S.R.; Nielsen, S.D.; Pappot, H. An Exploratory Study of Early Immune Response Markers for Pembrolizumab in Urothelial Tract Cancer. Uro 2024, 4, 1-11. https://doi.org/10.3390/uro4010001
Stormoen DR, Omland LH, Mouw KW, Szallasi Z, Ostrowski SR, Nielsen SD, Pappot H. An Exploratory Study of Early Immune Response Markers for Pembrolizumab in Urothelial Tract Cancer. Uro. 2024; 4(1):1-11. https://doi.org/10.3390/uro4010001
Chicago/Turabian StyleStormoen, Dag Rune, Lise Høj Omland, Kent William Mouw, Zoltan Szallasi, Sisse Rye Ostrowski, Susanne Dam Nielsen, and Helle Pappot. 2024. "An Exploratory Study of Early Immune Response Markers for Pembrolizumab in Urothelial Tract Cancer" Uro 4, no. 1: 1-11. https://doi.org/10.3390/uro4010001