
Efficacy of Fosfomycin against Extended Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Patient Urinary Cultures in the General Reference Hospital of Niamey, Niger
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site, Period, and Data Gathering
2.2. Identification and Antimicrobial Susceptibility Testing
2.3. Data Analysis and Processing
3. Results
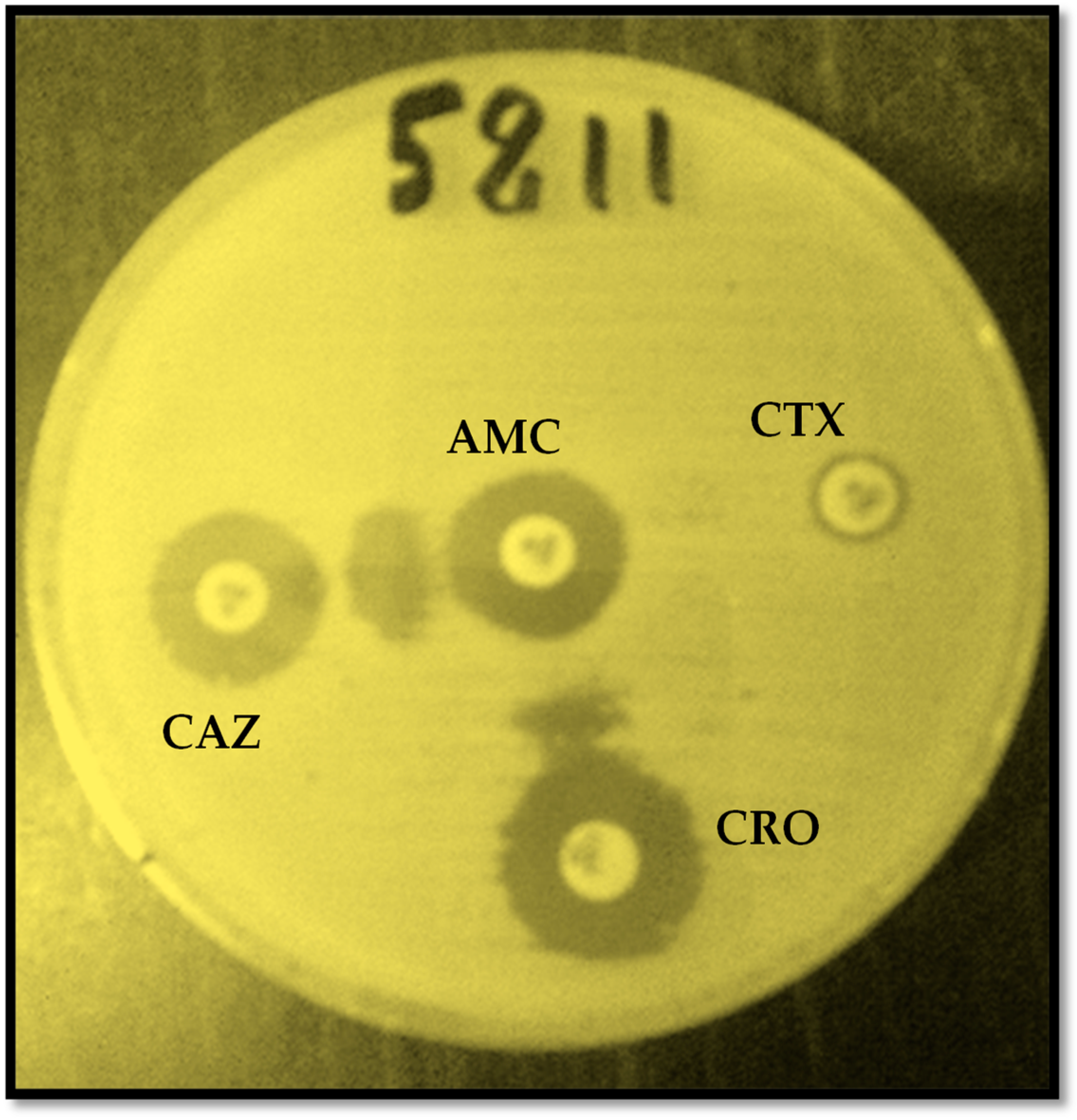
3.1. Prevalence of ESBL-Producing E. coli Isolates
3.2. Susceptibility of ESBL-Producing E. coli to Fosfomycin
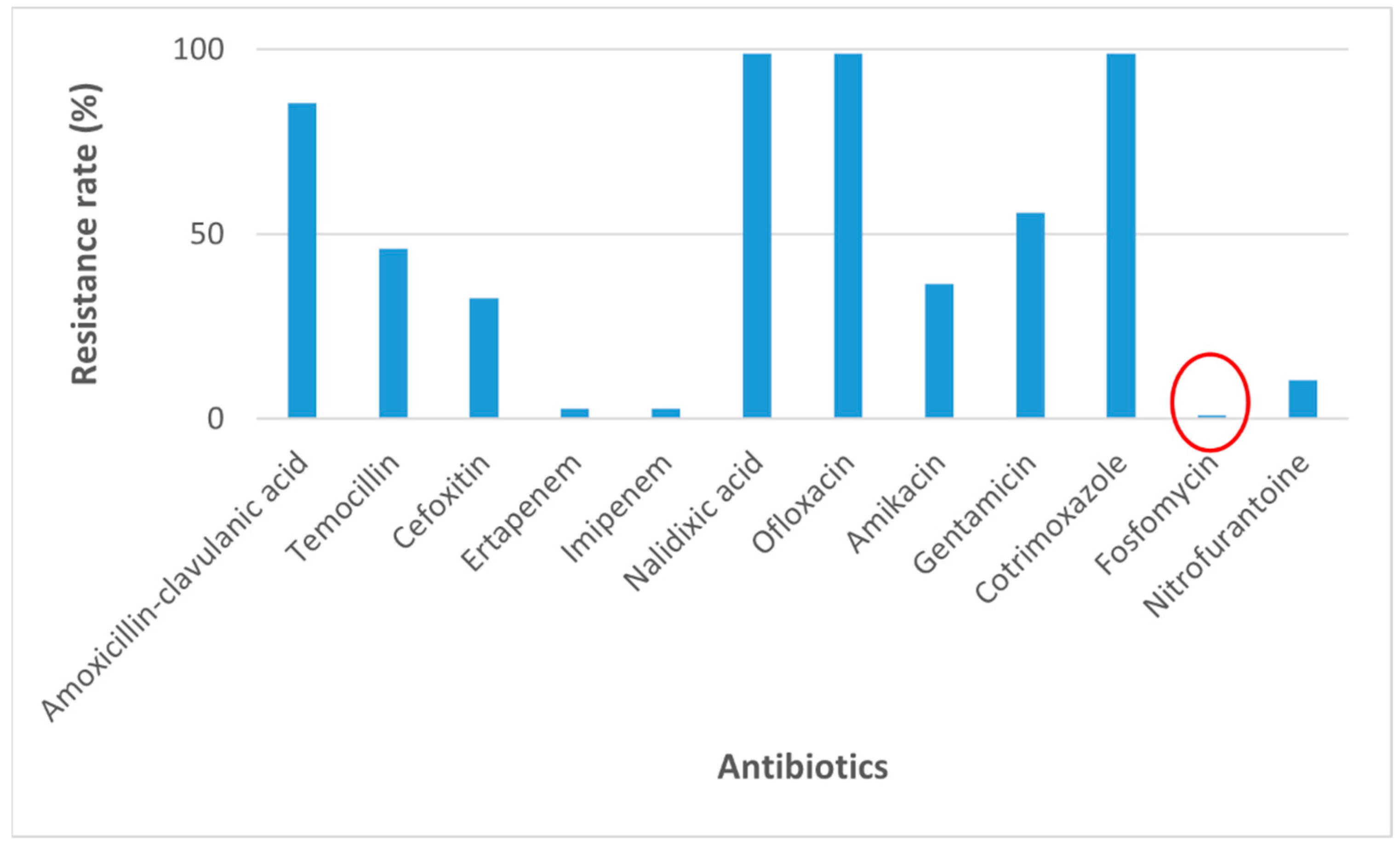
3.3. Antibiotic Resistance Profile of ESBL-Producing Escherichia coli
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fody, A.M.; Bagré, T.S.; Traoré, A.; Yacouba, A.; Dembelé, R.; Boubou, L.; Inoussa, A.; Sidikou, R.; Traoré, A.S.; Gassama-Sow, A.; et al. Molecular characterization of extended spectrum beta-lactamase among clinical multidrug resistant Escherichia coli in two hospitals of Niamey, Niger. Afr. J. Clin. Exp. Microbiol. 2018, 19, 1–8. [Google Scholar] [CrossRef]
- Gohar, H.; Afridi, F.I.; Fatima, M.; Fatima, A.; Afzal, N.; Fasih, F. Effectiveness of Fosfomycin against Extended Spectrum Beta-Lactamase Producing Escherichia coli in Urinary Cultures. Pak. J. Med. Dent. 2021, 10, 44–50. [Google Scholar]
- Wilson, D.T.; May, D.B. Potential Role of Fosfomycin in the Treatment of Community-Acquired Lower Urinary Tract Infections Caused by Extended-Spectrum β-Lactamase-Producing Escherichia coli. Am. J. Ther. 2013, 20, 685–690. [Google Scholar] [CrossRef]
- Liu, H.Y.; Lin, H.C.; Lin, Y.C.; Yu, S.H.; Wu, W.H.; Lee, Y.J. Antimicrobial susceptibilities of urinary extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae to fosfomycin and nitrofurantoin in a teaching hospital in Taiwan. J. Microbiol. Immunol. Infect. 2011, 44, 364–368. [Google Scholar] [CrossRef]
- Djim-Adjim-Ngana, K.; Oumar, L.A.; Mbiakop, B.W.; Njifon, H.L.M.; Crucitti, T.; Nchiwan, E.N.; Yanou, N.N.; Deweerdt, L. Prevalence of extended-spectrum beta-lactamase-producing enterobacterial urinary infections and associated risk factors in small children of Garoua, Northern Cameroon. Pan Afr. Med. J. 2020, 36, 157. [Google Scholar] [CrossRef]
- de Cueto, M.; Aliaga, L.; Alós, J.I.; Canut, A.; Los-Arcos, I.; Martínez, J.A.; Mensa, J.; Pintado, V.; Rodriguez-Pardo, D.; Yuste, J.R. Executive summary of the diagnosis and treatment of urinary tract infection: Guidelines of the Spanish Society of Clinical Microbiology and Infectious Diseases (SEIMC). Enfermedades Infecc. Microbiol. Clin. 2017, 35, 314–320. [Google Scholar] [CrossRef]
- Klein, R.D.; Hultgren, S.J. Urinary tract infections: Microbial pathogenesis, host-pathogen interactions and new treatment strategies. Nat. Rev. Microbiol. 2020, 18, 211–226. [Google Scholar] [CrossRef]
- Rodríguez-Baño, J.; Gutiérrez-Gutiérrez, B.; Machuca, I.; Pascual, A. Treatment of Infections Caused by Extended-Spectrum-Beta-Lactamase-, AmpC-, and Carbapenemase-Producing Enterobacteriaceae. Clin. Microbiol. Rev. 2018, 31, e00079-17. [Google Scholar] [CrossRef]
- Rodriguez-Avial, C.; Rodriguez-Avial, I.; Hernandez, E.; Picazo, J.J. Increasing prevalence of fosfomycin resistance in extended-spectrum-beta-lactamase-producing Escherichia coli urinary isolates (2005–2009–2011). Rev. Espanola Quimioter. 2013, 26, 43–46. [Google Scholar]
- Sagna, T.; Somda, W.D.N.; Koné, A.C.; Sagna, Y.; Tialla, D. Antibiotic Susceptibility of Escherichia coli and Klebsiella pneumoniae Strains, Urinary Tract Infections Cases in Bobo-Dioulasso, Burkina Faso. EC Microbiol. 2019, 15, 172–178. [Google Scholar]
- Falagas, M.E.; Vouloumanou, E.K.; Samonis, G.; Vardakas, K.Z. Fosfomycin. Clin. Microbiol. Rev. 2016, 29, 321–347. [Google Scholar] [CrossRef] [PubMed]
- Dinh, A.; Salomon, J.; Bru, J.P.; Bernard, L. Fosfomycin: Efficacy against infections caused by multidrug-resistant bacteria. Scand. J. Infect. Dis. 2012, 44, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Díez-Aguilar, M.; Cantón, R. New microbiological aspects of fosfomycin. Rev. Española Quimioter. 2019, 32, 8. [Google Scholar]
- Keating, G.M. Fosfomycin trometamol: A review of its use as a single-dose oral treatment for patients with acute lower urinary tract infections and pregnant women with asymptomatic bacteriuria. Drugs 2013, 73, 1951–1966. [Google Scholar] [CrossRef] [PubMed]
- Kahan, F.M.; Kahan, J.S.; Cassidy, P.J.; Kropp, H. The mechanism of action of fosfomycin (phosphonomycin). Ann. N. Y. Acad. Sci. 1974, 235, 364–386. [Google Scholar] [CrossRef] [PubMed]
- Matthews, P.C.; Barrett, L.K.; Warren, S.; Stoesser, N.; Snelling, M.; Scarborough, M.; Jones, N. Oral fosfomycin for treatment of urinary tract infection: A retrospective cohort study. BMC Infect. Dis. 2016, 16, 556. [Google Scholar] [CrossRef] [PubMed]
- Pullukcu, H.; Tasbakan, M.; Sipahi, O.R.; Yamazhan, T.; Aydemir, S.; Ulusoy, S. Fosfomycin in the treatment of extended spectrum beta-lactamase-producing Escherichia coli-related lower urinary tract infections. Int. J. Antimicrob. Agents 2007, 29, 62–65. [Google Scholar] [CrossRef]
- Margulieux, K.R.; Srijan, A.; Ruekit, S.; Nobthai, P.; Poramathikul, K.; Pandey, P.; Serichantalergs, O.; Shrestha, S.K.; Bodhidatta, L.; Swierczewski, B.E. Extended-spectrum β-lactamase prevalence and virulence factor characterization of enterotoxigenic Escherichia coli responsible for acute diarrhea in Nepal from 2001 to 2016. Antimicrob. Resist. Infect. Control. 2018, 7, 87. [Google Scholar] [CrossRef]
- Mohamed, A.H.; Dembélé, R.; Salaou, C.; Kagambèga, A.B.; Coulibaly, H.; Bado, F.F.; Fody, A.M.; Boubou, L.; Ibrahim, I.; Omar, E.A.; et al. Antibiotic Resistance in the Uropathogenic Enterobacteria Isolated from Patients Attending General Reference Hospital (GRH) of Niamey, Niger. Open J. Med. Microbiol. 2023, 13, 78–90. [Google Scholar] [CrossRef]
- Angaali, N.; Vemu, L.; Padmasri, C.; Mamidi, N.; Teja, V.D. Direct identification and susceptibility testing of Gram-negative bacilli from turbid urine samples using VITEK2. J. Lab. Physicians 2018, 10, 299–303. [Google Scholar] [CrossRef]
- CA-SFM/EUCAST 2019. Available online: https://www.bing.com/search?q=CA-SFM+%2F+EUCAST+2019&cvid=876c1b1bccb044a2adb894132c95eac7&aqs=edge..69i57j69i60.4058j0j1&pglt=43&FORM=ANNTA1&PC=U531 (accessed on 30 August 2023).
- Anand, M.; Sahu, C.; Negi, A.; Singh, A. In vitro assessment of fosfomycin: A beacon of hope in drug resistant organisms causing urinary tract infections. J. Adv. Med. Med. Res. 2019, 30, 1–9. [Google Scholar] [CrossRef]
- Hareendranath, G.; Mukundan, A.; Kunjappan, S.P. Fosfomycin Susceptibility in Multidrug Resistant Urinary Escherichia coli Isolates. J. Evol. Med. Dent. Sci. 2021, 10, 414–419. [Google Scholar] [CrossRef]
- Bader, M.S.; Loeb, M.; Leto, D.; Brooks, A.A. Treatment of urinary tract infections in the era of antimicrobial resistance and new antimicrobial agents. Postgrad. Med. 2020, 132, 234–250. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Chatterjee, K.; Deka, S.; Shankar, R.; Kalita, D. Increased isolation of extended-spectrum beta-lactamase-producing Escherichia coli from community-onset urinary tract infection cases in Uttarakhand, India. Cureus 2021, 13, e13837. [Google Scholar] [CrossRef] [PubMed]
- Kettani Halabi, M.; Lahlou, F.A.; Diawara, I.; El Adouzi, Y.; Marnaoui, R.; Benmessaoud, R.; Smyej, I. Antibiotic resistance pattern of extended spectrum beta lactamase producing Escherichia coli isolated from patients with urinary tract infection in Morocco. Front. Cell. Infect. Microbiol. 2021, 11, 720701. [Google Scholar] [CrossRef] [PubMed]
- Jia, P.; Zhu, Y.; Li, X.; Kudinha, T.; Yang, Y.; Zhang, G.; Zhang, J.; Xu, Y.; Yang, Q. High prevalence of extended-spectrum beta-lactamases in Escherichia coli strains collected from strictly defined community-acquired urinary tract infections in adults in China: A multicenter prospective clinical microbiological and molecular study. Front. Microbiol. 2021, 12, 663033. [Google Scholar] [CrossRef] [PubMed]
- Padmini, N.; Ajilda, A.A.K.; Sivakumar, N.; Selvakumar, G. Extended spectrum β-lactamase producing Escherichia coli and Klebsiella pneumoniae: Critical tools for antibiotic resistance pattern. J. Basic Microbiol. 2017, 57, 460–470. [Google Scholar] [CrossRef] [PubMed]
- Abayneh, M.; Tesfaw, G.; Abdissa, A. Isolation of extended-spectrum β-lactamase-(ESBL-) producing Escherichia coli and Klebsiella pneumoniae from patients with community-onset urinary tract infections in Jimma University Specialized Hospital, Southwest Ethiopia. Can. J. Infect. Dis. Med. Microbiol. 2018, 2018, 4846159. [Google Scholar] [CrossRef]
- Priyadharshana, U.; Piyasiri, L.B.; Wijesinghe, C. Prevalence, antibiotic sensitivity pattern and genetic analysis of extended spectrum beta lactamase producing Escherichia coli and Klebsiella spp. among patients with community acquired urinary tract infection in Galle district, Sri Lanka. Ceylon Med. J. 2019, 64, 140–145. [Google Scholar] [CrossRef]
- Mahajan, K.D.; Joshi, R. Evaluation of clinical Spectrum, antibiotic Sensitivity, and clinical Outcome in pediatric Age Group (0–18 Years) with Extended-spectrum Beta-lactamase-producing Escherichia coli-associated Urinary Tract Infection in Tertiary Care Hospital in India. Pediatr. Infect. Dis. 2022, 4, 133–137. [Google Scholar] [CrossRef]
- Aris, P.; Boroumand, M.A.; Rahbar, M.; Douraghi, M. The activity of fosfomycin against extended-spectrum beta-lactamase-producing isolates of Enterobacteriaceae recovered from urinary tract infections: A single-center study over a period of 12 years. Microb. Drug Resist. 2018, 24, 607–612. [Google Scholar] [CrossRef]
- Dijkmans, A.C.; Ortiz Zacarías, N.V.; Burggraaf, J.; Mouton, J.W.; Wilms, E.B.; Van Nieuwkoop, C.; Touw, D.J.; Stevens, J.; Kamerling, I.M. Fosfomycin: Pharmacological, clinical and future perspectives. Antibiotics 2017, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Falagas, M.E.; Kastoris, A.C.; Kapaskelis, A.M.; Karageorgopoulos, D.E. Fosfomycin for the treatment of multidrug-resistant, including extended-spectrum β-lactamase producing, Enterobacteriaceae infections: A systematic review. Lancet Infect. Dis. 2010, 10, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Neuner, E.A.; Sekeres, J.; Hall, G.S.; van Duin, D. Experience with fosfomycin for treatment of urinary tract infections due to multidrug-resistant organisms. Antimicrob. Agents Chemother. 2012, 56, 5744–5748. [Google Scholar] [CrossRef]
- Cai, T.; Palagin, I.; Brunelli, R.; Cipelli, R.; Pellini, E.; Truzzi, J.C.; Van Bruwaene, S. Office-based approach to urinary tract infections in 50 000 patients: Results from the REWIND study. Int. J. Antimicrob. Agents 2020, 56, 105966. [Google Scholar] [CrossRef]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [PubMed]
- Bonkat, G.; Bartoletti, R.; Bruyere, F.; Cai, T.; Geerlings, S.; Köves, B.; Schubert, S.; Wagenlehner, F.; Mezei, T.; Pilatz, A. EAU guidelines on urological infections. Eur. Assoc. Urol. 2017, 18, 22–26. [Google Scholar]
- Bonkat, G.; Bartoletti, R.; Bruyere, F.; Cai, T.; Geerlings, S.; Köves, B.; Schubert, S.; Wagenlehner, F. EAU Guideline of Urological Infections. Eur. Assoc. Urol. 2022, 78. Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-Guidelines-on-Urological-Infections-2022.pdf (accessed on 30 August 2023).
- Bouiller, K.; Zayet, S.; Lalloz, P.E.; Potron, A.; Gendrin, V.; Chirouze, C.; Klopfenstein, T. Efficacy and Safety of Oral Fosfomycin-Trometamol in Male Urinary Tract Infections with Multidrug-Resistant Enterobacterales. Antibiotics 2022, 11, 198. [Google Scholar] [CrossRef]
- Sardar, A.; Basireddy, S.R.; Navaz, A.; Singh, M.; Kabra, V. Comparative evaluation of fosfomycin activity with other antimicrobial agents against E. coli isolates from urinary tract infections. J. Clin. Diagn. Res. JCDR 2017, 11, DC26. [Google Scholar]
- Tutone, M.; Johansen, T.E.B.; Cai, T.; Mushtaq, S.; Livermore, D.M. Susceptibility and Resistance to fosfomycin and other antimicrobial agents among pathogens causing lower urinary tract infections: Findings of the SURF study. Int. J. Antimicrob. Agents 2022, 59, 106574. [Google Scholar] [CrossRef]
- Kot, B. Antibiotic resistance among uropathogenic. Pol. J. Microbiol. 2019, 68, 403–415. [Google Scholar] [CrossRef] [PubMed]
- Hashemian, S.M.R.; Farhadi, Z.; Farhadi, T. Fosfomycin: The characteristics, activity, and use in critical care. Ther. Clin. Risk Manag. 2019, 15, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.G.; Walkty, A.J.; Karlowsky, J.A. Fosfomycin: A first-line oral therapy for acute uncomplicated cystitis. Can. J. Infect. Dis. Med. Microbiol. 2016, 2016, 2082693. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age (Years) | ≤5 N (%) | 6–25 N (%) | 26–45 N (%) | 46–65 N (%) | ≥66 N (%) | Total N (%) | |
|---|---|---|---|---|---|---|---|
| Sexe | Male | 0 (0) | 0 (0) | 6 (42.86) | 28 (45.90) | 16 (72.73) | 50 (48.10) |
| Female | 1 (100) | 6 (100) | 8 (57.14) | 33 (54.10) | 6 (27.27) | 54 (51.90) | |
| Status | Inpatients | 0 (0) | 1 (16.67) | 2 (14.30) | 18 (29.51) | 4 (18.19) | 25 (24.04) |
| Outpatients | 1 (100) | 5 (83.33) | 12 (85.70) | 43 (70.49) | 18 (81.81) | 79 (75.96) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohamed, A.H.; Dembélé, R.; Fody, A.M.; Kagambèga, A.B.; Coulibaly, H.; Bado, F.F.; Salaou, C.; Boubou, L.; Ibrahim, A.; Omar, E.A.; et al. Efficacy of Fosfomycin against Extended Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Patient Urinary Cultures in the General Reference Hospital of Niamey, Niger. Uro 2023, 3, 262-270. https://doi.org/10.3390/uro3040026
Mohamed AH, Dembélé R, Fody AM, Kagambèga AB, Coulibaly H, Bado FF, Salaou C, Boubou L, Ibrahim A, Omar EA, et al. Efficacy of Fosfomycin against Extended Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Patient Urinary Cultures in the General Reference Hospital of Niamey, Niger. Uro. 2023; 3(4):262-270. https://doi.org/10.3390/uro3040026
Chicago/Turabian StyleMohamed, Alassane Halawen, René Dembélé, Alio Mahamadou Fody, Alix Bénédicte Kagambèga, Hiliassa Coulibaly, Frédéric François Bado, Chaibou Salaou, Laouali Boubou, Alkassoum Ibrahim, Eric Adehossi Omar, and et al. 2023. "Efficacy of Fosfomycin against Extended Spectrum Beta-Lactamase-Producing Escherichia coli Isolated from Patient Urinary Cultures in the General Reference Hospital of Niamey, Niger" Uro 3, no. 4: 262-270. https://doi.org/10.3390/uro3040026