
Prophylactic Lymphadenectomy in Patients with Penile Cancer: Is Sooner Better?
 , , ,
, , ,
Abstract
:1. Introduction
Research Questions
2. Materials and Methods
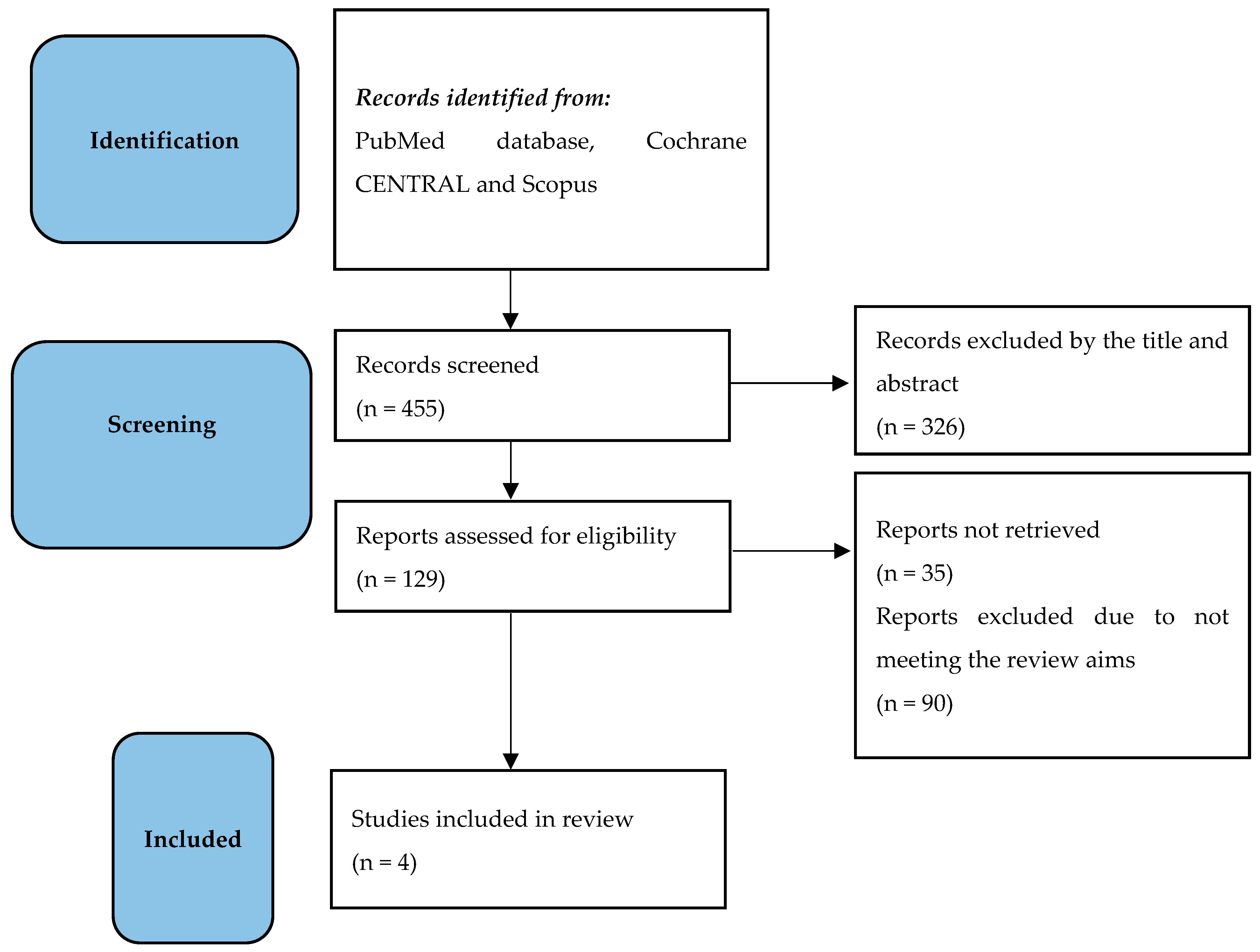
Research Strategy
3. Research Evidence
3.1. Indication for Inguinal Lymph Node Dissection
- -
- Palpable lymph nodes (cN1-cN2);
- -
- pT2 or higher penile cancer stage, even in the case of non-palpable lymph nodes;
- -
- Presence of lymphovascular invasion;
- -
- Poorly differentiated histology.
3.1.1. Timing of Inguinal Lymph Node Dissection
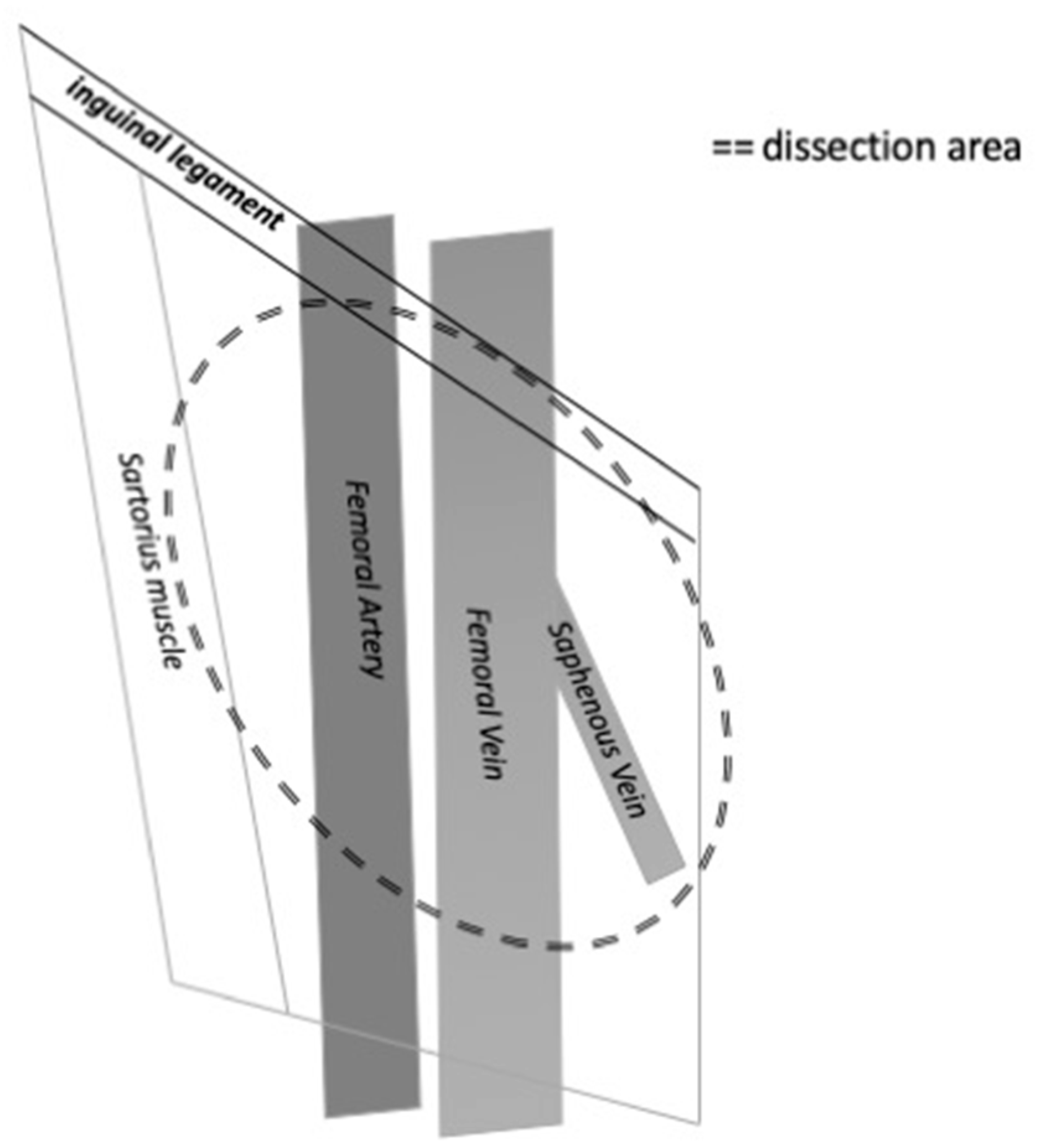
3.1.2. Anatomical Considerations of Inguinal Lymph Node Dissection
3.2. Indications for Pelvic Lymph Node Dissection
3.2.1. Timing of Pelvic Lymph Node Dissection
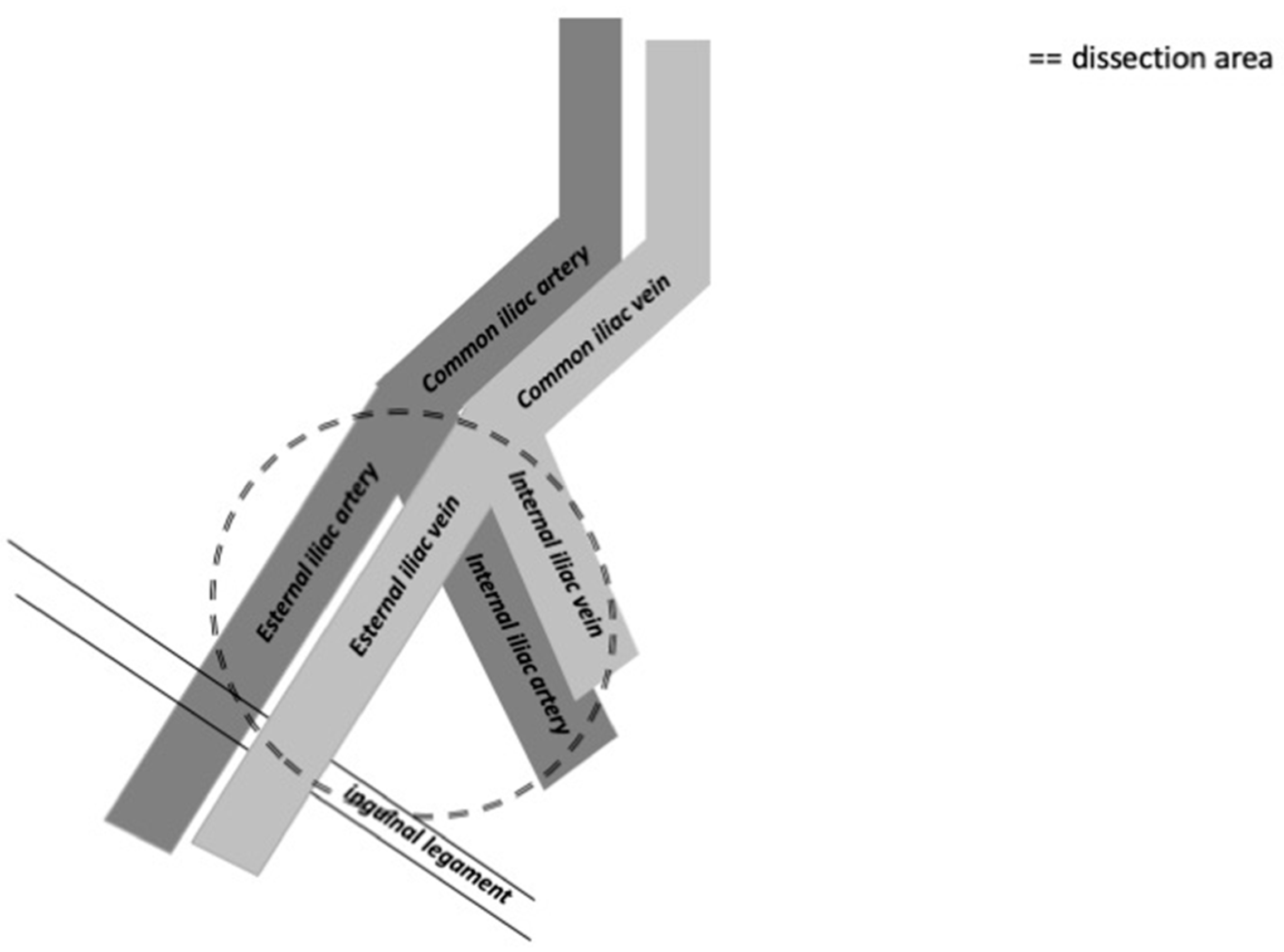
3.2.2. Anatomical Considerations of Pelvic Lymph Node Dissection
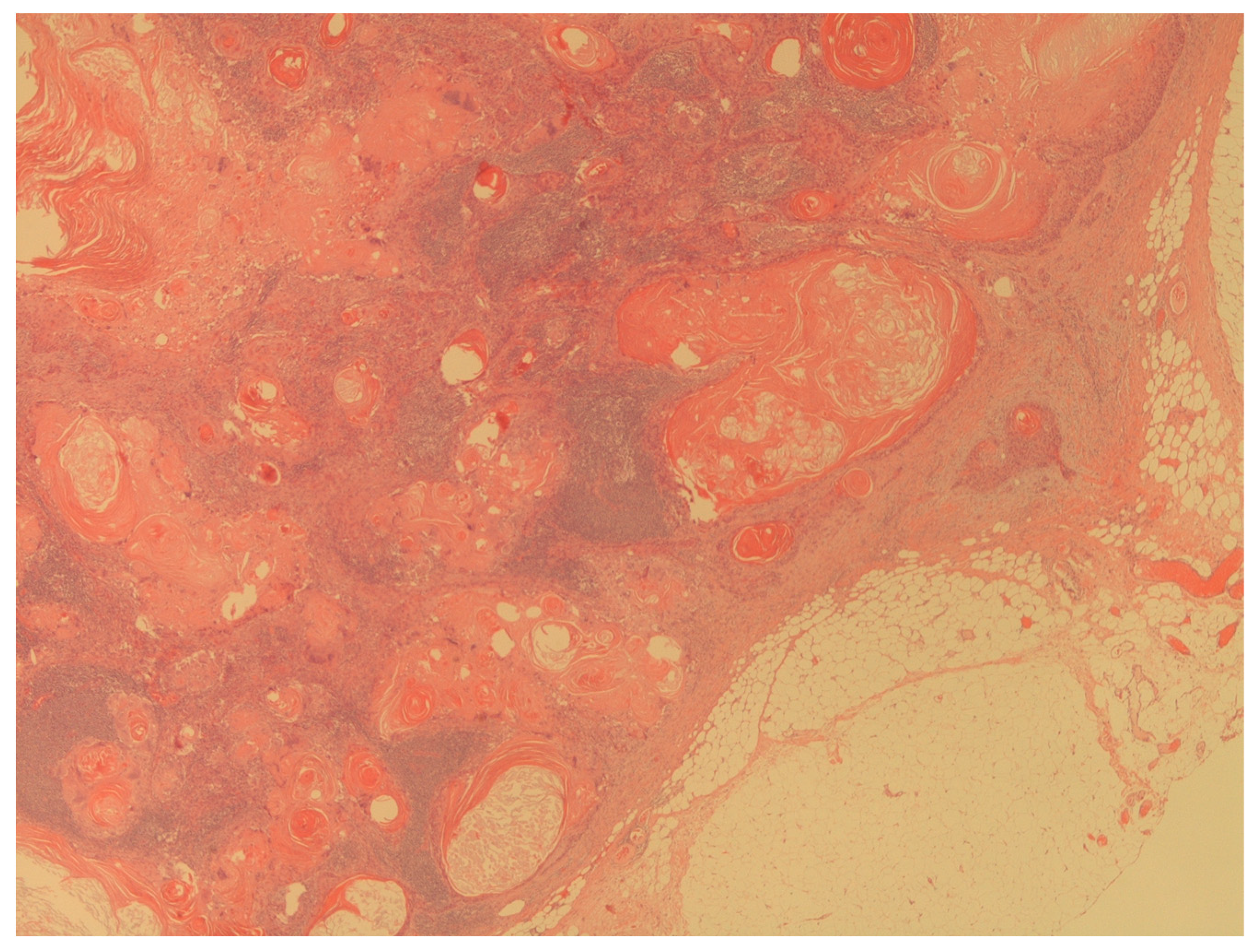
3.3. Pathological Considerations on Lymph Node Analysis
3.4. Systematic Review Findings on the Timing of Lymph Node Dissection
4. Limitations
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salvioni, R.; Necchi, A.; Piva, L.; Colecchia, M.; Nicolai, N. Penile cancer. Urol. Oncol. 2009, 27, 677–685. [Google Scholar] [CrossRef]
- Ma, S.; Zhao, J.; Liu, Z.; Wu, T.; Wang, S.; Wu, C.; Pan, L.; Jiang, X.; Guan, Z.; Wang, Y.; et al. Prophylactic inguinal lymphadenectomy for high-risk cN0 penile cancer: The optimal surgical timing. Front. Oncol. 2023, 13, 1069284. [Google Scholar] [CrossRef]
- Pow-Sang, M.R.; Ferreira, U.; Pow-Sang, J.M.; Nardi, A.C.; Destefano, V. Epidemiology and natural history of penile cancer. Urology 2010, 76 (Suppl. S1), S2–S6. [Google Scholar] [CrossRef]
- Kroon, B.K.; Horenblas, S.; Lont, A.P.; Tanis, P.J.; Gallee, M.P.; Nieweg, O.E. Patients with penile carcinoma benefit from immediate resection of clinically occult lymph node metastases. J. Urol. 2005, 173, 816–819. [Google Scholar] [CrossRef]
- Available online: https://d56bochluxqnz.cloudfront.net/documents/full-guideline/EAU-ASCO-Guidelines-on-Penile-Cancer-2023_2023-03-08-131333_piyo.pdf (accessed on 3 September 2023).
- Johnson, D.E.; Lo, R.K. Management of regional lymph nodes in penile carcinoma. Five-year results following therapeutic groin dissections. Urology 1984, 24, 308–311. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- The, J.; Duncan, C.; Qu, L.; Guerra, G.; Narasimhan, V.; Pham, T.; Lawrentschuk, N. Inguinal lymph node dissection for penile cancer: A contemporary review. Transl. Androl. Urol. 2020, 9, 3210–3218. [Google Scholar] [CrossRef]
- Saisorn, I.; Lawrentschuk, N.; Leewansangtong, S.; Bolton, D.M. Fine-needle aspiration cytology predicts inguinal lymph node metastasis without antibiotic pretreatment in penile carcinoma. BJU Int. 2006, 97, 1225–1228. [Google Scholar] [CrossRef] [PubMed]
- Clark, P.E.; Spiess, P.E.; Agarwal, N.; Biagioli, M.C.; Eisenberger, M.A.; Greenberg, R.E.; Herr, H.W.; Inman, B.A.; Kuban, D.A.; Kuzel, T.M.; et al. Penile cancer: Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2013, 11, 594–615. [Google Scholar] [CrossRef]
- Ren, S.; Shao, Y.; Bao, Y.; Li, X. Prediction of survival in patients with penile cancer after lymph node dissection. Asian J. Surg. 2022, 45, 1700–1702. [Google Scholar] [CrossRef]
- Chipollini, J.; Tang, D.H.; Gilbert, S.M.; Poch, M.A.; Pow-Sang, J.M.; Sexton, W.J.; Spiess, P.E. Delay to Inguinal Lymph Node Dissection Greater than 3 Months Predicts Poorer Recurrence-Free Survival for Patients with Penile Cancer. J. Urol. 2017, 198, 1346–1352. [Google Scholar] [CrossRef] [PubMed]
- Gulia, A.K.; Mandhani, A.; Muruganandham, K.; Kapoor, R.; Ansari, M.S.; Srivastava, A. Impact of delay in inguinal lymph node dissection in patients with carcinoma of penis. Indian J. Cancer 2009, 46, 214–218. [Google Scholar] [CrossRef]
- Catalona, W.J. Modified inguinal lymphadenectomy for carcinoma of the penis with preservation of saphenous veins: Technique and preliminary results. J. Urol. 1988, 140, 306–310. [Google Scholar] [CrossRef]
- Spiess, P.E.; Hernandez, M.S.; Pettaway, C.A. Contemporary inguinal lymph node dissection: Minimizing complications. World J. Urol. 2009, 27, 205–212. [Google Scholar] [CrossRef]
- Bevan-Thomas, R.; Slaton, J.W.; Pettaway, C.A. Contemporary morbidity from lymphadenectomy for penile squamous cell carcinoma: The M.D. Anderson Cancer Center Experience. J. Urol. 2002, 167, 1638–1642. [Google Scholar] [CrossRef]
- Sadeghi, R.; Gholami, H.; Zakavi, S.R.; Kakhki, V.R.; Horenblas, S. Accuracy of 18F-FDG PET/CT for diagnosing inguinal lymph node involvement in penile squamous cell carcinoma: Systematic review and meta-analysis of the literature. Clin. Nucl. Med. 2012, 37, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kim, S.J. Diagnostic Performance of 18F-FDG PET/CT for Lymph Node Staging in Penile Cancer. Clin. Nucl. Med. 2022, 47, 402–408. [Google Scholar] [CrossRef]
- Jakobsen, J.K.; Frahm Nielsen, T.; Ipsen, P.; Albrecht-Beste, E.; Cardoso Costa, J.; Alslev, L.; Predbjørn Krarup, K.; Grønkaer Toft, B.; Høyer, S.; Bouchelouche, K.; et al. DaPeCa-7: Comparative assessment of fluorodeoxyglucose positron emission tomography/computed tomography (CT) and conventional diagnostic CT in diagnosis of lymph node metastases, distant metastases and incidental findings in patients with invasive penile cancer. BJU Int. 2021, 127, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www2.tri-kobe.org/nccn/guideline/urological/english/penile.pdf (accessed on 3 September 2023).
- Yao, K.; Chen, Y.; Ye, Y.; Wu, Z.; Chen, D.; Han, H.; Li, Z.; Liu, Z.; Wang, Y.; Qin, Z.; et al. Lymph Node Mapping in Patients with Penile Cancer Undergoing Pelvic Lymph Node Dissection. J. Urol. 2021, 205, 145. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, S.L.; Ye, D.W.; Yao, X.D.; Dai, B.; Zhang, H.L.; Shen, Y.J.; Zhu, Y.P.; Shi, G.H.; Ma, C.G. Prospectively packaged ilioinguinal lymphadenectomy for penile cancer: The disseminative pattern of lymph node metastasis. J. Urol. 2009, 181, 2103. [Google Scholar] [CrossRef] [PubMed]
- Perera, M.; McGrath, S.; Sengupta, S.; Crozier, J.; Bolton, D.; Lawrentschuk, N. Pelvic lymph node dissection during radical cystectomy for muscle-invasive bladder cancer. Nat. Rev. Urol. 2018, 15, 686–692. [Google Scholar] [CrossRef] [PubMed]
- Ficarra, V.; Martignoni, G.; Maffei, N.; Cerruto, M.A.; Novara, G.; Cavalleri, S.; Artibani, W. Predictive pathological factors of lymph nodes involvement in the squamous cell carcinoma of the penis. Int. Urol. Nephrol. 2002, 34, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Kamat, A.M.; Carpenter, S.M.; Czerniak, B.A.; Pisters, L.L. Metastatic penile cancer in a young Caucasian male: Impact of delayed diagnosis. Urol. Oncol. 2005, 23, 130–131. [Google Scholar] [CrossRef] [PubMed]
- Reyes, A.J.; Ramcharan, K.; Goetz, L.; Aboh, S. Penectomy for self-neglected opportunistic carcinoma: A large primary urogenital squamous cell carcinoma as initial manifestation of HIV-AIDS. BMJ Case Rep. 2016, 2016, bcr2016217040. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Ibarrola, R.; Basulto-Martinez, M.; Sigle, A.; Abufaraj, M.; Gratzke, C.; Miernik, A. Is There an Oncological Benefit of Performing Bilateral Pelvic Lymph Node Dissection in Patients with Penile Cancer and Inguinal Lymph Node Metastasis? J. Clin. Med. 2021, 10, 754. [Google Scholar] [CrossRef] [PubMed]
- Cai, T.; Verze, P.; Bjerklund Johansen, T.E. The Quality of Life Definition: Where Are We Going? Uro 2021, 1, 14–22. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Type of Study | Aim | Description of Findings |
|---|---|---|---|---|
| Chipollini J [12] | 2017 | Retrospective cohort study | To determine the optimal time to perform inguinal lymph node dissection. | Inguinal lymph node dissection should be undertaken within 3 months after penile cancer diagnosis. |
| Gulia AK [13] | 2009 | Retrospective case-control study | To evaluate the impact of delay in inguinal lymph node dissection. | Inguinal lymph node dissection should be undertaken during the same hospital admission as for treating the penile lesion or within 2 months after penile cancer diagnosis. |
| Johnson DE [6] | 1984 | Retrospective case-control study | To compare early therapeutic dissection with late therapeutic dissection. | Early therapeutic dissection should be preferred in order to improve the patients’ survival. |
| Kroon BK [4] | 2005 | Retrospective cohort study | To compare the outcome of early vs. delayed lymph node dissection. | Early lymph node dissection in patients with penile cancer improves survival. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, T.; Capece, M.; Zorzi, M.G.; Palmieri, A.; Nesi, G.; Barbareschi, M.; Bjerklund Johansen, T.E. Prophylactic Lymphadenectomy in Patients with Penile Cancer: Is Sooner Better? Uro 2023, 3, 251-261. https://doi.org/10.3390/uro3040025
Cai T, Capece M, Zorzi MG, Palmieri A, Nesi G, Barbareschi M, Bjerklund Johansen TE. Prophylactic Lymphadenectomy in Patients with Penile Cancer: Is Sooner Better? Uro. 2023; 3(4):251-261. https://doi.org/10.3390/uro3040025
Chicago/Turabian StyleCai, Tommaso, Marco Capece, Maria Grazia Zorzi, Alessandro Palmieri, Gabriella Nesi, Mattia Barbareschi, and Truls E. Bjerklund Johansen. 2023. "Prophylactic Lymphadenectomy in Patients with Penile Cancer: Is Sooner Better?" Uro 3, no. 4: 251-261. https://doi.org/10.3390/uro3040025